REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
Publicação Oficial da Sociedade Brasileira de Anestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Remifentanil
does
not
increase
urine
output
during
oral
surgery,
contrary
to
its
effect
during
other
surgeries
---
a
cohort
study
Kentaro
Ouchi
∗,
Kazuna
Sugiyama
KagoshimaUniversityGraduateSchoolofMedicalandDentalSciences,FieldofOralandMaxillofacialRehabilitation, DepartmentofDentalAnesthesiology,Kagoshima,Japan
Received25November2015;accepted16December2015 Availableonline29April2016
KEYWORDS
Remifentanil;
Urineoutput;
Generalanesthesia
Abstract
Background: Anincreaseinurineoutputbyremifentanilinjectionduringlaparoscopic proce-duresandsurgeriessuchascardiacandgynecologicalprocedures,duetosuppressionofthe stressresponsetosurgery,hasbeenreported.Theaimofourprospective,observational,cohort studywastoassesstheeffectofremifentanilanalgesiaonurineoutputduringdentalandminor oralsurgerybycomparingintraoperativeurineoutputunderdefinedinfusionvolumeswithand withouttheuseofremifentanil.
Methods:Dentalpatientsaged16yearsorolder,AmericanSocietyofAnesthesiologistsphysical status1,withnorenaldiseasesorabnormalbloodvaluesofserumcreatinineandBUN,noton treatmentwithdiureticdrugs,andundergoingminororo-maxillofacialsurgeryordental treat-mentunderinhalationgeneralanesthesiawereincludedinthisstudy.Urethralcatheterization wasperformedafteranesthesiainduction,andurineoutputwasmeasuredevery30minutes. Wemeasuredurinevolume(mL)andrateofurineoutput(mL.kg−1.h−1)intraoperatively,and comparedtheseparametersbetweenpatientswhodidanddidnotreceiveremifentanilduring theintraoperativeperiod.
Results:Eighty-sevenpatientswerecategorizedintotheremifentanilgroup(n=43)or remifen-tanilnon-usegroup(n=44).Bothvolumeofurine(mL)andrateofurineoutput(mL.kg−1.h−1) werenotsignificantlydifferentbetweenthetwogroups(remifentanilgroup,372.3±273.5mL, 1.8±1.1mL.kg−1.h−1; remifentanilnon-use group, 343.3±283.3mL,1.9±1.2mL.kg−1.h−1; p=0.63;0.57).
∗Correspondingauthor.
E-mail:[email protected](K.Ouchi).
http://dx.doi.org/10.1016/j.bjane.2015.12.004
Conclusion: Ourresultsshowthatuseofremifentanilduringdental andminororalsurgeries doesnotincreaseurineoutput.
©2016SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE
Remifentanil; Diurese;
Anestesiageral
Remifentanilnãoaumentaadiuresedurantecirurgiaoral,contrariamenteaoseu efeitoduranteoutrascirurgias---estudodecoorte
Resumo
Justificativa: Foirelatadoumaumentonadiureseapósainjec¸ãoderemifentanildurante pro-cedimentoslaparoscópicosecirurgiascardíacaseginecológicas,devidoàsupressãodaresposta aoestressedacirurgia.Oobjetivodenossoestudoprospectivo,observacionaledecoortefoi avaliaroefeitodaanalgesiacomremifentanilsobreadiuresedurantecirurgiaodontológicae oraldepequenoporteecompararadiuresenointraoperatóriosobinfusãodevolumesdefinidos, comesemousoderemifentanil.
Métodos: Pacientesodontológicos≥16anos,estadofísicoASAI,semdoenc¸asrenaisouvalores sanguíneosanormaisdecreatininaséricaeureia,semtratamentocomdiuréticose submeti-dosàcirurgia bucomaxilofacialdepequenoporteoutratamentoodontológicosobanestesia geralinalatóriaforamincluídosnesteestudo.Cateterismouretralfoifeitoapósainduc¸ãoda anestesiaeadiuresefoimedidaacada30min.Medimosovolumedeurina(mL)eataxade diurese(mL.kg−1.h−1)nointraoperatórioecomparamosessesparâmetrosentreospacientes quereceberamequenãoreceberamremifentanilduranteoperíodointraoperatório.
Resultados: Foramdesignados87pacientesparaosgruposcomremifentanil(n=43)ougrupo semremifentanil(n=44).Ovolumedeurina(mL)eataxadediurese(mL.kg−1.h−1)nãoforam significativamentediferentesentreosdoisgrupos(grupocomremifentanil:372,3±273,5mL, 1,8±1,1mL.kg−1.h−1;gruposemremifentanil:343,3±283,3mL,1,9±1,2mL.kg−1.h−1;p= 0,63;0,57).
Conclusão:Nossos resultadosmostramqueouso deremifentanilduranteascirurgias odon-tológicasedepequenoportenãoaumentaadiurese.
©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigo OpenAccess sobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Reportedly, remifentanil increases urine output during surgery, probably by preventing the stress response to surgery.1---5Previousstudiesonincreasesinurineoutputdue toremifentanil were performed duringlaparoscopic, car-diac,or gynecological surgeries,but itseffectduringoral andmaxillofacialtreatmenthasnotbeenreported.
Theaimofourobservationalstudywastocompareurine outputduringuseofremifentanilversusnon-useof remifen-tanil in patients undergoing minor oral surgery or dental procedures,bymeasuringurineoutputunderdefined infu-sionvolumesintheintraoperativeperiod.
Methods
Dental patients aged 16 years or older, undergoing minor oro-maxillofacial surgery and dental treatment under inhalationalgeneralanesthesiaattheClinicalDepartment
ofDentalAnesthesia,KagoshimaUniversityMedicalDental HospitalfromApril2011toMarch2014werestudied.Tobe includedinthestudy,patientshadtobeAmericanSociety ofAnesthesiologistsphysicalstatus1.Patientswithknown renaldisease,laboratorydataindicativeofabnormalblood valuesofserumcreatinineandBloodUreaNitrogen(BUN), andthoseontreatmentwithdiureticdrugswereexcluded. Informed consentfor oral surgeryand for participationin thisstudyundergeneralanesthesiawasobtainedfromeach patient.The institutionalreview board of Kagoshima Uni-versityMedicalDentalHospitalapprovedthestudyprotocol, whichwasconductedinaccordancewiththeDeclarationof Helsinki.
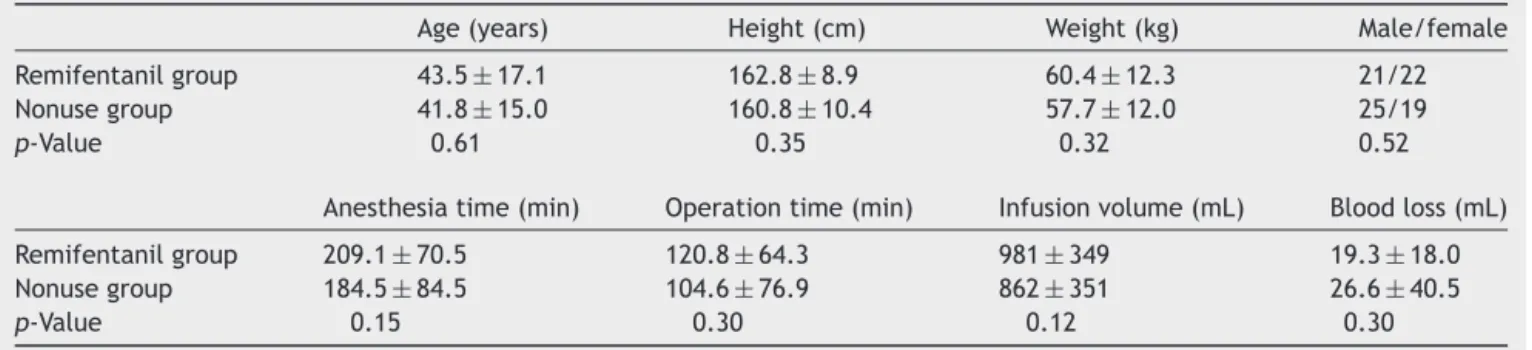
Table1 Demographicsofpatientsintheremifentaniluseandnon-usegroups.
Age(years) Height(cm) Weight(kg) Male/female
Remifentanilgroup 43.5±17.1 162.8±8.9 60.4±12.3 21/22
Nonusegroup 41.8±15.0 160.8±10.4 57.7±12.0 25/19
p-Value 0.61 0.35 0.32 0.52
Anesthesiatime(min) Operationtime(min) Infusionvolume(mL) Bloodloss(mL)
Remifentanilgroup 209.1±70.5 120.8±64.3 981±349 19.3±18.0
Nonusegroup 184.5±84.5 104.6±76.9 862±351 26.6±40.5
p-Value 0.15 0.30 0.12 0.30
Anesthesiaprotocol
According to current recommendations, patients were
allowed solid foods for up to the night before surgery,
and clear fluids for up to 2.5h before general
anes-thesia induction. An intravenous line was secured for
administration of the isotonic fluid (140mEq.L−1 sodium
with 1% glucose; Physio140, Otsuka Pharmaceutical, Co.,
Ltd.,Tokyo,Japan).Furthermore,allpatientscontinuously
underwentnon-invasiveblood pressureand
electrocardio-graphicmonitoringusingastandardautomatedmonitoring
device(Marquette Solar8000M,GE Medical Systems,UK).
Anesthesia was induced with propofol 1.5mg.kg−1 IV,
and intubation was facilitated with the IV administration
of rocuronium 0.9mg.kg−1. In remifentanil-use cases, it
was administered at the rate of 0.25g.kg−1.min−1
dur-inganesthesia induction. Anesthesia wasmaintained with
sevoflurane (1.5%), nitrous oxide (4L.min−1) and oxygen
(2L.min−1). Remifentanil-use cases additionally received
a continuous infusion of remifentanil at the rate of
0.05---0.15g.kg−1.min−1.Remifentanilnon-usepatientsdid
notreceiveanyopioids. Remifentanil-usepatientsdidnot
receiveotheropioids.Localanesthesiawasusedbythe
sur-geons,asappropriate.Thesurgeonswereunawareoftheuse
or non-use of remifentanil.Rocuronium wasadministered
forintubation,withnoadditionaldosesbeingadministered
intraoperatively. All patients received 4.5mL.kg−1.h−1 of
thecrystalloid fluidwithan infusion pump fromthe time
of securing the intravenous line. Urethral catheterization
wasperformedafteranesthesiainductionandurineoutput
wasmeasured every 30min during anesthesia. If patients
developedhypotensionintraoperatively,withafallin
sys-tolicBPtolessthan80mm.Hg−1,remifentanilinfusionwas
temporarilydiscontinued,andtheyweregivenephedrine.
Thesepatientswerethenexcludedfromthestudy.All
anes-theticswerestoppedattheendofsurgery.
Measurementofparameters
Wemeasuredthetotalvolumeofurine(mL)andvolumeof
urineperkilogrambodyweightperunittime(mL.kg−1.h−1)
in all patients. We then compared these values between
remifentaniluseandnon-usegroups.
Statisticalanalyses
Continuousdemographicandlaboratoryvariableswere
com-paredusingtheunpairedt-test,andtheChi-squaretestwas
usedforcategoricalvariables.JMPsoftware(version10,SAS
InstituteInc.,Japan)wasusedforstatisticalanalysis,and
p<0.05wasregardedasbeingstatisticallysignificant.The
resultsarepresentedasmean±SD.
Results
Eighty-sevenpatientswereincludedinthisstudyandwere
categorizedintotheremifentanilgroup(n=43)or
remifen-tanil non-use group (n=44). Table 1 shows the patients’
demographicdataandTable2liststhesurgicalprocedures performed.Useofremifentanilwasattheattending anes-thesiologist’sdiscretion.Thestudysubjectswereattended tobyoneofthefouranesthesiologists.AnesthesiologistsA and B routinely administer remifentanil, and anesthesiol-ogistsCandDdonotroutinelyadministerremifentanil.In casesinwhichitwasused,remifentanilwasgiveninthedose rangeof0.05---0.15g.kg−1.min−1.Bloodpressureduringthe
intraoperativeperioddecreasedbymorethan15---25% com-paredwithpre-anesthesiavaluesinbothgroups.
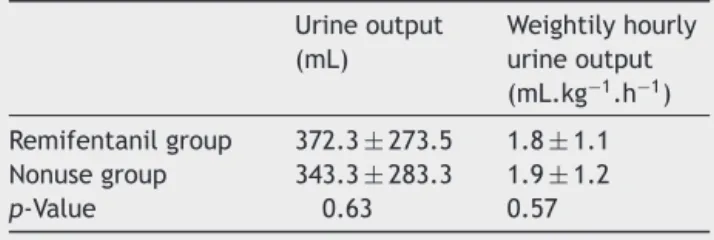
Volume of urine (mL) and volume of urine per kilo-gram body weight per unit time (mL.kg−1.h−1) were not
significantlydifferentbetweenthetwogroups(remifentanil group, 372.3±273.5mL, 1.8±1.1mL.kg−1.h−1; non-use
group, 343.3±283.3mL, 1.9±1.2mL.kg−1.h−1; p=0.63;
0.57,respectively)(Table3).
Table2 Surgeriesperformedinthestudysubjects. Remifentanil
group
Nonusegroup
Toothextraction 15 19
Cystextirpation 15 16
Platesexclusion 4 2
Dentaltreatment 2 2
Cleftlipnasaldeformity 1 2
Dentalimplant 1 0
Incisionaldrainage 1 0
Sialolithextirpation 1 0
Bonetransplantation 0 1
Osteoplasty 2 1
Leukoplakiaexcision 1 1
Table3 Urineoutputwithandwithouttheuseof remifen-tanilduringdental/minororalsurgery.
Urineoutput (mL)
Weightilyhourly urineoutput (mL.kg−1.h−1)
Remifentanilgroup 372.3±273.5 1.8±1.1
Nonusegroup 343.3±283.3 1.9±1.2
p-Value 0.63 0.57
Discussion
The purpose of this study was to evaluate the effect of
remifentanilonurineoutputin patientsundergoingminor
oralandmaxillofacialsurgeryundergeneralanesthesiawith
nitrous oxide and sevoflurane. The authors hypothesized
that remifentanilwould increase urine outputduring oral
surgeries,similartothatduringlaparoscopic surgeries,as
well ascardiac and gynecological procedures. We found,
however, that remifentanil does not increase urine
out-putduring dentaland oralsurgery. The mechanismof the
previously reported increase in urine volumeby
remifen-tanilisbelieved tobeasfollows.Adequateanalgesiawith
remifentanilreducesthesecretionofantidiuretichormone,
resulting in an increase in urine output. One of the
pre-vious reports states that the increase in urine volume
induced by remifentanil is accompanied by a decreasein
catecholamine secretionand a highly significant decrease
in cortisol excretion.1 In other reports, although the
lev-els of antidiuretic hormone, catecholamine and cortisol were not measured, their values were believed to have decreased.1,3---5 In all of these previous reports, the sur-geries performed were those in which local anesthesia alonewouldnotprovideadequateanalgesia.Inlaparoscopic surgeryfor example,becausea widerangeofanalgesiais requiredforincisionoftheperitoneum,epiduralanesthesia doesnotprovideadequateanalgesia.1Moreover,in laparo-scopicsurgery,acomparativelyhigherdoseofremifentanil isrequiredtodecreasethecatecholaminesecretioninduced bysurgicalstimulation.6Remifentanilinfluencestherelease of stressresponse markers,such asantidiuretichormone, ACTH, cortisol, noradrenaline and adrenaline.7,8 In this study,inboththegroups,irrespectiveoftheuseornon-use ofremifentanil,anesthesiawasmaintainedwithsevoflurane 1.5%,nitrousoxide66.6%andoxygen33.3%.Consequently, patients received 1.51 MAC of inhalational anesthetics, because1MACofsevofluraneis 1.71%andthatof nitrous oxideis 105%.Thus,the concentrationofanesthetics was sufficient for minor surgery. The procedures evaluatedin this study included minor oral surgeries, such as tooth extractionandcystextirpation.Minororalsurgeryisusually performed under local anesthesiaor localanesthesia and intravenousanesthesia/sedation(non-useofopioids).Even cleftlipdeformitycanberepairedunderlocalanesthesia.9 Thus,inoperationsinthisstudy,localanesthesiaand inhala-tionanestheticsprovidedadequateanalgesiainallsubjects, even those who did not receive remifentanil. We postu-latethattheabsenceofanincreaseinurineoutputunder remifentanilanalgesiaduringminororalanddentalsurgery,
asseen inthis study,is duetothefact thatinthese pro-cedures,anesthesiawithout remifentanil providesenough analgesiathatthe stress response,andhence, stress hor-monesreleaseis blunted,which results in minimal effect of remifentanil on these hormones and hence, on urine output.
Therehasbeennostudyinvestigatingthedirecteffect ofremifentanilonrenalfunction.However,previousstudies onthepreconditioningeffectofremifentanilhavereported thatalthoughremifentanilisa-receptoragonist,its car-dioprotective effect is mediated through and ␦ opioid receptors.Reportedly,receptoractionmayincreaseurine output,because agonists have been reported toinduce diuresisinanimalstudies.10,11However,urineoutputwasnot greaterintheremifentanilgroupinthisstudy.Thissuggests thatreceptoractionisnotresponsiblefortheincreasein urineoutput induced by remifentanil.Further studies are neededtoelucidatethemechanismofthediuresisinduced byremifentanil.
The type of fluid administered intraoperatively may affect urine output. It is reported that during use of 0.9%saline,increasedafferentarteriolarresistancereduces renalflowandglomerularfiltrationrate,leadingtoreduced urineoutput.12 Consequently,differenttypesoffluidsmay havedifferenteffectsonurineoutput.Thus,fluidinfusion inthisstudywasrestrictedtoasingletypeoffluid.Inthis study,fluidwasinfusedattherateof4.5mL.kg−1.h−1.For
a60kgpatient,whichwasthemeanweightofsubjectsin this study, this amounted to 270mL.h−1. If fluid
require-mentis calculatedbasedonthe 4-2-1rule(4mL.kg−1.h−1
for the first 10kg body weight, 2mL.kg−1.h−1 from11 to
20kg and 1mL.kg−1.h−1 for every kg above 20kg), this
would have amounted to 100mL.h−1 for a 60kg patient.
Thus,theamountofmaintenancefluidadministeredduring anesthesiawasan over dose,although thereasonfor this over-infusionwastocompensateforpreoperative dehydra-tionoverthe shorttimeperiodofthe operation(planned for0.5---2h).
In thisstudy, use of remifentanilwasat theattending anesthesiologist’sdiscretion.While the decision touse or notuse remifentanil differs according to the anesthesiol-ogist, the number of patients in the two groups in this study wasalmost identical.Further, sincethe rest of the anesthesiaprotocol,otherthanuseornon-useof remifen-tanil, was prescribed, the likelihood of operator bias, in terms of the attending anesthesiologist, in this study is minimal.
Conclusions
Inconclusion,our resultssuggest thatuse of remifentanil does not increase urine output during general anesthesia withnitrousoxideandsevofluranefordentalandminororal surgery.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
ThisworkwassupportedbytheDepartmentalResearchFund ofKagoshimaUniversity.Thisworkwaspresented,inpart, on October 10---12, 2014, at the 42th Annual Meeting of theJapaneseDentalSocietyofAnesthesiology(Chairperson: Prof.KimitoSano),Niigata.
References
1.IshikawaK, SakaiA, NagataH, et al.Remifentanil increases urine outputin patients undergoing laparoscopic colectomy. Masui.2012;61:526---30.
2.MylesPS,HuntJO,FletcherH,etal.Remifentanil,fentanyl,and cardiacsurgery:adouble-blinded,randomized,controlledtrial ofcostsandoutcomes.AnesthAnalg.2002;95:805---12[tableof contents].
3.OnakaM,YamamotoH.Remifentanilmaybebeneficialto uri-nary outputunderepidural-basedgeneral anesthesia.Masui. 2010;59:1391---5.
4.Yago Y, Tajiri O, Ito H, et al. Effect of remifentanil on urineoutputduringgynecologicallaparoscopicsurgery.Masui. 2009;58:613---5.
5.Kawai M, Nakata J, Kawaguchi M, et al. Comparison of urinary output during general anesthesia, between patients administeredwithremifentanilandthosewithoutremifentanil administration.Masui.2010;59:179---82.
6.MyreK, Raeder J, Rostrup M, et al. Catecholamine release duringlaparoscopicfundoplicationwithhighandlowdosesof remifentanil.ActaAnaesthesiolScand.2003;47:267---73. 7.MaranaE,ScambiaG,ColicciS,etal.Leptinandperioperative
neuroendocrinestressresponsewithtwodifferentanaesthetic techniques.ActaAnaesthesiolScand.2008;52:541---6.
8.WinterhalterM,BrandlK,Rahe-MeyerN,etal.Endocrinestress responseandinflammatoryactivationduringCABGsurgery.A randomizedtrialcomparingremifentanilinfusionto intermit-tentfentanyl.EurJAnaesthesiol.2008;25:326---35.
9.LalondeDH,PriceC,WongAL, etal.Minimally painfullocal anestheticinjectionforcleftlip/nasalrepairingrownpatients. PlastReconstrSurgGlobOpen.2014;2:e171.
10.KimJE,LeeJS,KimMK,etal.Nicardipineinfusionfor hypoten-sive anesthesia during orthognathic surgery has protective effect on renal function. J Oral Maxillofac Surg. 2014;72: 41---6.
11.Ashton N, Balment RJ, Blackburn TP. Kappa-opioid-induced changes in renal water and electrolyte management and endocrinesecretion.BrJPharmacol.1989;97:769---76. 12.SantiM, Lava SA, CamozziP, et al. The greatfluid debate:
salineor so-called ‘‘balanced’’salt solutions? ItalJ Pediatr. 2015;41:47.