jcoloproctol(rioj).2015;35(3):178–181
w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Case
Report
Late
diagnosis
of
Hirschsprung’s
disease
Marielle
Rodrigues
Martins
a,b,∗,
Carlos
Henrique
Marques
dos
Santos
a,b,c,
Gustavo
Ribeiro
Falcão
a,baUniversidadeFederaldeMatoGrossodoSul(UFMS),CampoGrande,MS,Brazil bHospitalUniversitárioMariaAparecidaPedrossian,CampoGrande,MS,Brazil cHospitalRegionaldeMatoGrossodoSul(HRMS),CampoGrande,MS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received11December2014 Accepted20February2015 Availableonline27May2015
Keywords:
Hirschsprung’sdisease Congenitalmegacolon Fecalincontinence
a
b
s
t
r
a
c
t
Hirschsprung’sdiseaseisaconditioncharacterizedbytheabsenceofganglioncellsina variablesegmentofthelargeintestine,mainlyproducingthesymptomofconstipationand beingusuallydiagnosedinthefirstyearoflife.Withdiagnosticmethodsalreadyestablished intheliterature,thesoletreatmentissurgery.Theobjectiveofthisstudyistoreportacaseof latediagnosisofthediseaseatage13,withsymptomsoffecalincontinenceinitsevolution. ©2015SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
Diagnóstico
tardio
da
doenc¸a
de
Hirschsprung
Palavras-chave:
Doenc¸adeHirschsprung Megacolocongênito Incontinênciafecal
r
e
s
u
m
o
ADoenc¸adeHirschsprungéumapatologiacaracterizadapelaausênciadecélulas gan-glionares em um segmento variáveldo intestino grosso, produzindo principalmenteo sintomadeconstipac¸ão,sendonormalmentediagnosticadaatéoprimeiroanodevida.Com métodosdiagnósticosjáconsagradosnaliteratura,otratamentoéexclusivamentecirúrgico. Oobjetivodestetrabalhoérelatarumcasodediagnósticotardiodadoenc¸a,aos13anos, comsintomatologiadeincontinênciafecalnaevoluc¸ãodoquadro.
©2015SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Introduction
Hirschsprung’sDisease(HD),alsoknownascongenital agan-glionicmegacolon,isananomalycharacterizedbyanabsence
∗ Correspondingauthor.
E-mail:[email protected](M.R.Martins).
ofganglioncellsinthemyentericandsubmucosalplexusesin avariablebowelsegment.1,2
Theabsenceofganglioncellsresultsinpermanent con-traction of the affected segment, preventing the passage offecalcontentthrough thatregion.3 Thedistalfunctional
http://dx.doi.org/10.1016/j.jcol.2015.02.009
jcoloproctol(rioj).2015;35(3):178–181
179
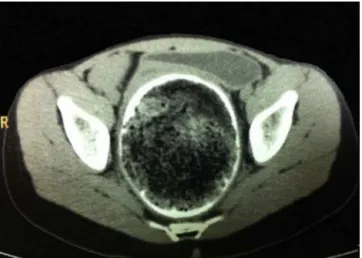
Fig.1–Computedtomography(axialplane)showingrectal fecalimpactionwithmegarectum.
obstruction leads to inefficient peristaltic contractions, withconsequentdilatationofproximalintestine,producing megacolon.1
HDpresentsitselfbysymptomsofconstipation,suchasa greaterthan48-hdelayineliminationofmeconium, abdom-inaldistentionandvomiting.In80%ofcases,thisdiseaseis diagnosedinthefirstyearoflife,beinguncommonin adoles-cenceandadulthood;suchcasesusuallyappearintheform ofanultrashortsegmentdisease.4
TheobjectiveofthispaperistoreportacaseofHDina 13-oldpatient,withtreatmentandoutpatientfollow-upatthe HospitalRegionaldeMatoGrossodoSulRosaPedrossian– HRMS.Theinfrequencyofthisdiagnosisinthisageandthe clinicalcourseofthispatientunderscoretheuniquenessof thiscase.
Clinical
case
Femalepatient,13yearsold,comingfromCampoGrande–MS, reportsthatsincebirthhadintestinalconstipation,withmean bowel movements at every 3–5 days with hardened feces, beingfollowed-upbyapediatricianandintreatmentfor func-tionalconstipation.Thegirlrefersonsetoffecalincontinence attheageof12.
Testsordered:giventheunavailabilityofbariumenema,a computedtomography(CT)studywasobtained,revealingthe presenceofrectalfecaloma(Figs.1and2).
A hypothesis of HD was proposed; thus an anorectal manometrywasasked,butitsresultwasinconclusivedueto patient’slackofcooperation.
Thenarectalbiopsywasperformed;thepathologistreport confirmedtheabsenceofganglioncellswithneurotizationof myentericandsubmucosalplexusesinashortrectalsegment (Fig.3),confirminganultra-shortformofaganglionosis.
Serology for Chagas’ disease was carried out in order toexcludeadiagnosis ofChagas’ Diseasemegacolon, with negativeresult. Thus, the diagnosis of HD was confirmed. Surgicaltreatmentwas performedlaparoscopically, accord-ingtoDuhamel-Haddadtechniquemodifiedwithprotective
Fig.2–Computedtomography(coronalplane)showing rectalfecalimpactionwithmegarectum.
loop ileostomy,withgoodclinicalprogression.Thegirlwas dischargedonthe5thdayaftersurgery.
Discussion
HDisacongenitalanomalythatoccursduetoa discontin-uationofthecranial–caudalmigrationofneuralcrestcells, whichareresponsibleforinnervationofthecolon,orwhen theganglioncellsundergoprematuredeathbetween5thand 12thweeksofpregnancy.1–3Itwasalsosuggestedthatchanges intheextracellularmatrixinthehumanembryogutcan inter-rupt the migration ofneural crest-derived cells,producing aganglionosis.2
Accordingtotheextentofcoloninvolvement,HDis clas-sified into short-segment disease (80% ofcases),when the aganglionic segmentdoesnotexceedthe sigmoidcolon; or intolong-segmentdisease,whenitoutrunsthesigmoidcolon. Inthislattercase,HDmayaffecttheentirecolonandeventhe smallintestine.5HDisstillclassifiedintoultrashort-segment diseasewhenitinvolvesonlythedistalpartoftherectum, occurringin2–3%(insomereports,withestimatesofupto 8%)ofthecases.2,6
180
jcoloproctol(rioj).2015;35(3):178–181Fig.3–Histopathology–(AandB)absenceofganglioncells.(C)Surgicalmarginwithganglioncells.
abnormalities;10%ofallcasesoccurinchildrenwithDown syndrome.1
Mostcasesof HD are sporadic,but 10%have afamilial origin.Halfoffamilialcasesand15% ofsporadiccasesare associatedwithgenemutationsinactivatingtheRETreceptor fortyrosinekinaseonchromosome10q.Somecasesinvolve genemutationsforendothelin-Breceptor.3Asthisisan auto-somaldominant disorder with incomplete penetrance, the modificationofgenesorenvironmentalfactorsmustalsobe important.1
Inaddition, it isestablishedthatfactors relatedto gen-der playa role,since menare preferentially affected,at a frequencyof4:1.5 However,incaseswherethediagnosis is madeinamoreadvancedage,thefrequencyishigheramong females(3:1),7,8asisthecaseforourpatient.
ThesymptomsthatleadtoanearlysuspicionofHDare bowelconstipation,definedinthenewbornasagreaterthan 48-hdelayintheeliminationofmeconiumassociatedwith abdominaldistensionandvomiting.In80%ofcasesHDis diag-nosedwithinthefirstyearoflife.Thisdisorderisuncommon inadolescenceandinadulthoodandwhenpresentinthisage group,itshowsupasanultrashort-segmentdisease.4
Intheliterature,in50–60%ofcasesthediagnosisis estab-lishedinthefirstmonthoflife.9However,mildcasesofHD caneludeanearlydiagnosis,eitherbylackofsymptoms,or becauseitssymptomsaremisinterpreted.Insuchcases,itis commonacertaindegreeofconstipationoffluctuating inten-sity, with fecaloma characterizing the clinical progression, ofteninassociationtochangesinnutritionandtogrowth.10
Some patients reach adulthood without adiagnosis for thisdisease.Typically,patientsgotothedoctorwitha long-standinghistoryofconstipationrequiringfrequentlaxative use.11 The current frequency of the disease in adults is unknown,especiallysinceHDisanoverlookedand misdiag-noseddiseaseinthisagegroup.
Ourpatienthadahistoryoflong-standingbowel consti-pation, progressing to fecal incontinence.This finding can beexplained by apermanent distention ofthe anal canal duetothe presenceofafecaloma, withconstant pressure ontheinternalsphincterandkeepingitopen.Therefore,the mostliquidstoolsupstreampassaroundthefecalimpaction andproducethereportedsymptom,knownasfecal inconti-nence(soiling).Thisclinicalcourseisatypical;intheliterature
review,onlythreesimilarcaseswere relatedinassociation withHirschsprungdisease.12,13
Complaintsoffecalincontinenceareoftenreportedinthe literatureincasesoffunctionalconstipationandofidiopathic megacolon.11,14 This problem is also reported in patients withacquiredmegacolon,beingmoreuncommonin congen-ital casesduetothe permanenceofaclosedinternal anal sphincter.11Fecalincontinenceisacommonpost-operative complicationofcongenitalmegacolon.2
Forourpatient,fecalincontinenceisamorelimiting symp-tomthantheconstipationitself,becausethegirlwaslivingin constantfearofoccurrenceofsuchfactinenvironmentslike herschool,whichwouldcausegreatembarrassmentbefore otherpeople.Inaddition,thereportedsymptomscausedthe girl’sparentstobegintojustifysuchafactasaresultofsome psychological,ratherthanorganic,disorder.Thisfactor con-tributedtothedelayinherdiagnosis,drivingthepediatrician out of a HD hypothesis. Therefore, fecal incontinence can cause emotionaldisturbancestopatients, withsubsequent relationshipproblemsatschoolandwiththeirownfamilies.15 ThediagnosisofHDissupportedbybariumenemastudies, anorectalmanometryandrectalbiopsy.4
Thetechniqueconsideredasthegoldenstandardforthe diagnosis of HD is the absence ofganglion cells ina rec-tal biopsyspecimen. Inaddition,theremay beanincrease innon-myelinatedcholinergicnervefibersinthesubmucosa andamongmusclelayers(neuralhyperplasia),whichhelpsin diagnosticconfirmation,2aswasthecaseofourpatient.
Imagingstudiessuchascomputedtomography(CT)and bariumenemasareusuallyacceptedforevaluationofchronic constipation, whichis acommon disorder inadults.16 Our patientunderwentCTduetotheunavailabilityofabarium enemastudy,butCTisamoreexpensivemethod.
Theanorectalmanometry,eventhoughnotcontributingin thepresentcase,isanancillarytestoftheutmostimportance, sincethepresenceoftherectum-analreflexinthisexam usu-allyruleoutthediagnosisofHD.14
jcoloproctol(rioj).2015;35(3):178–181
181
Nevertheless, the literature considers as the procedure of choicethe Duhamel technique inonly one surgical time,2 whichreducesthehospitalizationtime.
This surgery is considered curative. However, post-operative bowel functioning is not always satisfactory. Enterocolitis,constipationand fecalincontinencerepresent themainpostoperativecomplicationsinchildren.5 Todate, theprogressionforadolescentoradultpatientsisnotfully clarifiedyet,duetothesmallnumberofreportedcases.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. RobbinsSL,CotranRS,KumarV.Patologia:basespatológicas dasdoenc¸as.8thed.RiodeJaneiro:Elsevier;2010.
2. PazAM,GonzaloA,GloriaRC.Revisión:Enfermedadde Hirschsprung.RevPedElec.2008;5(1).Availableat: http://www.revistapediatria.cl/vol5num1/6.html[cited 04.03.14].
3. RubinE.Rubinpatologia:basesclinicopatológicasda medicina.4thed.RiodeJaneiro:GuanabaraKoogan;2010. 4. IcazaChávezME,TakahashiMonroyT,UribeUribeN,
HernándezOrtizJ,ValdovinosMA.Enfermedadde Hirschsprungeneladulto.Informedeumcaso.Rev GastroenterolMéx.2000;65:171–4.
5. VillarMAM,JungMDP,CardosoLCDA,CardosoMHCDA, LlerenaJuniorJC.Doenc¸adeHirschsprung:experiênciacom umasériede55casos.RevBrasSaúdeMaternInfant. 2009;3:285–91.
6.BakariAA,GaliBM,IbrahimAG,NggadaHA,AliN,DogoD, etal.Casereport:congenitalaganglionicmegacolonin Nigerianadults:twocasereportsandreviewoftheliterature. NigerJClinPract.2011;14:249–52.
7.BurlandoE,BernhardtR,StegerH,StoletniyE.Enfermedadde Hirschsprungdeladulto:correcciónquirúrgica.RevArgent ResidCir.2009;13:79–81.
8.LombanaLJ,DomínguezLC.Cirugíaenlaenfermedadde Hirschsprungdeladulto.RevColombGastroenterol. 2007;22:231–7.
9.BigélliRH,FernandesMI,GalvãoLC,SawamuraR.Estudo retrospectivode53crianc¸ascomdoenc¸adeHirschsprung: achadosclínicoselaboratoriais.Medicina(RibeiraoPreto). 2002;35:78–84.Availableat:
http://www.revistas.usp.br/rmrp/article/view/798[cited 04.03.14].
10.JonesFA,GoddingEW.Tratamentodaconstipacao.SãoPaulo: Manole;1975.
11.GordonPH,NivatvongsS.Principlesandpracticeofsurgery forthecolon,rectumandanus.2thed.St.Louis:Quality Medical;1992.
12.BarnesPR,Lennard-JonesJE,HawleyPR,ToddIP.
Hirschsprung’sdiseaseandidiopathicmegacoloninadults andadolescents.Gut.1986;27:534–41.
13.SotoD.EnfermedaddeHirschsprungenadultos.VerCirChil. 2001;53:346.
14.Costa-PintoEAL,Bustorff-SilvaJM,FukushimaE.Papelda manometriaanorretalnodiagnósticodiferencialda constipac¸ãoemcrianc¸as.JPediatr(RiodeJ).2000;76: 227–32.
15.DeMoraisMB,MaffeiHVL.Constipac¸ãointestinal.JPediatr. 2000;76:S147.