www.revportcardiol.org
Revista
Portuguesa
de
Cardiologia
Portuguese
Journal
of
Cardiology
ORIGINAL
ARTICLE
Transradial
left
ventricular
endomyocardial
biopsy
feasibility,
safety
and
clinical
usefulness:
Initial
experience
of
a
tertiary
university
center
Miguel
Nobre
Menezes
a,b,∗,
Eduardo
Infante
Oliveira
a,b,
Artur
Costa
e
Silva
c,
Dulce
Brito
a,b,
Maria
da
Conceic
¸ão
Azevedo
Coutinho
a,b,
Pedro
Canas
da
Silva
a,b,
Fausto
J.
Pinto
a,baServic¸odeCardiologia,CentroHospitalarUniversitárioLisboaNorte,Lisboa,Portugal bCAML,CCUL,FaculdadedeMedicinadeLisboa,UniversidadedeLisboa,Portugal
cServic¸odeAnatomiaPatológica,CentroHospitalarUniversitárioLisboaNorte,Lisboa,Portugal
Received5July2019;accepted10November2019 Availableonline1August2020
KEYWORDS Leftendomyocardial biopsy; Transradial; Myocarditis; Cardiomyopathy Abstract
Introductionandobjectives:Over thelastdecade, severalstudies havesuggested thatleft ventricularendomyocardialbiopsyissaferandhasahigherdiagnosticyieldthantransvenous rightventricularbiopsy.Inaddition,recentpublicationsindicatethatthetransradialapproachis afeasibleandsafealternativetothetransfemoralapproachforsamplingtheleftventricle.We reportourinitialexperiencewithtransradialendomyocardialbiopsywithregardstofeasibility, safetyandusefulness.
Methods:Single-center registryofconsecutivepatients undergoingintendedtransradial left endomyocardialbiopsy.Clinicalandtechnicaldatawerecollectedprospectively,witha partic-ularfocusonsuccessrateandcomplications.
Results:Twenty-seven patients were screened for left ventricle biopsy. Twenty (25) were selectedforanintendedtransradialapproach(meanage51±18yearsold,22male).Success ratewas100%withnocrossovertofemoralapproach.Therewerenomajorcomplications.Two patientsexperiencedmildradialspasm.Oneofthemalsohadarunofnon-sustainedventricular tachycardia.
Indicationfor biopsywas either myocarditisor cardiomyopathyofunknown etiology.The finaldiagnosiswasacutelymphocyticmyocarditisinfivepatients,chronicmyocarditisinone patient,amyloidlight-chainamyloidosisinfourpatientsandtransthyretinamyloidosis insix patients.Myocarditiswasruledoutineightpatientsandamyloidosisinonepatient.
∗Correspondingauthor.
E-mailaddress:[email protected](M.NobreMenezes).
https://doi.org/10.1016/j.repc.2019.11.004
0870-2551/©2020SociedadePortuguesadeCardiologia.PublishedbyElsevierEspa˜na,S.L.U.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Conclusions:Transradialleftventricleendomyocardialbiopsyisaverysafeandfeasiblemethod ofsamplingthemyocardiumfor histopathologicalanalysis,withagooddiagnosticyieldand clinicallymeaningfulresultsinproperlyselectedpatients.
©2020SociedadePortuguesadeCardiologia.PublishedbyElsevierEspa˜na,S.L.U.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/). PALAVRAS-CHAVE Biópsia endomiocárdica esquerda; Transradial; Miocardite; Miocardiopatia
Exequibilidade,seguranc¸aeutilidadedabiópsiaendomiocárdicaventricular
esquerdaporacessotransradial:experiênciainicialdeumcentrouniversitário
terciário
Resumo
Introduc¸ãoeobjetivos: Duranteaúltimadécada, váriosestudos têmsugeridoqueabiópsia endomiocárdicaventricularesquerdaémaisseguraedesuperiorrentabilidadediagnósticado quea doventrículo direito.Adicionalmente, váriaspublicac¸õesrecentes têm introduzidoa abordagemtransradialcomoumaalternativaexequíveleseguraàtransfemoral,paraamostrar oventrículoesquerdo.Oobjetivodesteestudoéreportaraexperiênciainicialdeumcentro embiópsiaendomiocárdicaventricularesquerdatransradial,relativamenteaexequibilidade, seguranc¸aeutilidade.
Métodos: Registounicêntrico dedoentesconsecutivos submetidosabiópsia endomiocárdica ventricularesquerda,comacessodeprimeiraintenc¸ãoradial.Registaram-seosdadosclínicos etécnicos,comparticularfoconataxadesucessoecomplicac¸ões.
Resultados: Foramsubmetidosabiópsiaendomiocárdicaventricularesquerda27doentes,25 dosquaispré-selecionadosparaacessotransradial (idademédia51±18,22homens).Ataxa desucessofoide100%. Nãoocorreramcomplicac¸õesmajor,apenasespasmoradialemdois doentes, num dos quais se observou uma salva de taquicardia ventricular não mantida. A indicac¸ãofoi miocarditeoumiocardiopatia deetiologiaaesclarecer.Odiagnóstico finalfoi demiocarditeagudaemcincodoentes,miocarditecrónicaemumdoente,amiloidoseALem quatrodoenteseATTRem seisdoentes.Excluiu-semiocarditeemoitodoenteseamiloidose emumdoente.
Conclusão:Abiópsiaendomiocárdicaventricularesquerdatransradialdemonstrousersegura, exequível e de boa rentabilidade diagnóstica, com resultados clinicamente relevantes em doentesselecionados.
©2020SociedadePortuguesadeCardiologia.PublicadoporElsevierEspa˜na,S.L.U.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
The development of endomyocardial biopsy in the 1960s facilitatedpercutaneoussamplingofthemyocardium with-out the need for a grossly invasive procedure.1 However,
in recent decades, significant advances in both invasive and non-invasive cardiac imaginghave enabled the study of a wide array of cardiac diseases, without the need for a histopathological analysis of the heart. As a result, enthusiasmfor myocardial biopsy haswaned. Indeed,the most recent recommendations regarding endomyocardial biopsydate back to2007,and a highlevel of recommen-dation applies in only a handful of settings.2 However,
these guidelines base their recommendations on efficacy and safety data in existence at that time. Since then, twomain changes have occurred: Firstly, several authors havepublishedextensivedataonan approachvia theleft ventricleratherthan justthe rightventricle,allowing for more extended myocardial sampling.3,4 Secondly, several
operators started performing left ventricular (LV) biopsy usingtheradialapproach, widelypopularinthe interven-tionalcommunityfor itssimplicity, comfortandincreased safety.5 As a result, more recent documents call for a
wideruse ofthistechnique,particularlyin myocarditis,6,7
dilated cardiomyopathy8 and myocardial infarction with
non-obstructivecoronaryarterydisease.9
Inthispaper,wereportourinitialexperienceofthe fea-sibility,safetyandusefulnessoftransradialendomyocardial biopsy.
Methods
Generalfeatures
This studyinvolved asingle-centerregistryof consecutive patients undergoing intended transradial endomyocardial biopsy.Patientswereselectedforendomyocardialbiopsyof
theleftventricleandscreenedfor thefeasibilityofradial access individually,based on theoperator’s clinical judg-ment.
Clinical data included demographics, clinical setting, imaging,complications,andfinal biopsyresults.Technical dataincludedaccesssite,sheath/cathetersizeandshape, biopsymodelandsize,proceduraltime,fluoroscopytime, successrateandcross-overratetofemoralapproach.
Statisticalanalysis
This is a descriptiveregistry; complex statistical analysis wasnotperformed.Qualitativevariablesareexpressedboth numerically and in percentages. Continuous variables are depictedasmean ± standarddeviation andrange,where appropriate.SPSSStatistics24wasusedforanalysis.
Procedureoverview
Detailed information on technique has been published in recentpapers.10---13However,becauseminorvariationoccurs
acrosscentersandoperators,anoverviewofthetechnique asitwasperformedisprovided.
The procedure was always undertaken by the same operator, who had been previously trained in transradial interventionandinperformingleftmyocardialbiopsies. Dur-ingtheprocedure,thepatientwascontinuouslymonitored asinaroutinecoronaryangiography(i.e.withcontinuous 12-leadelectrocardiogramandinvasivebloodpressure mea-surement).
Routine transthoracicechocardiographywasperformed before,during andafter the procedure. Particular atten-tionwasgiventodocumentingandquantifyingpericardial effusionandmitralregurgitation,aswell asexcluding the presenceofLVthrombusormasseswhichmight contraindi-catetheprocedure.
Spasmprophylaxiswithintra-arterial0.5-1mgof isosor-bidedinitrateand/or2.5mgofverapamiland5000unitsof unfractionatedheparinwereadministered.
If the patient required a coronary angiogram, a stan-dard transradial coronaryangiogram was performed using aTerumo5/6Frslendersheath(externaldiameter5Fr)and standardJudkins5Frcoronarydiagnosticcatheters.
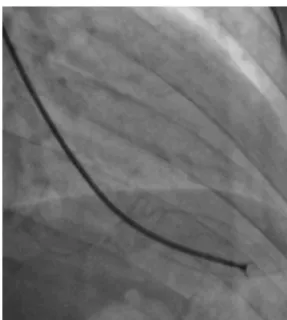
Afterwards, a 7.5 Fr (external diameter 6 Fr) Asahi Eaucathsheathlessguidecatheterwasadvancedovera stan-dard0.035’’J wiretotheascendingaorta.An MP1orJR 3.5/4 curve was used according to operator choice. The dilator wasremoved anda 5Fr pigtail catheterwasthen used inside the 7.5 Fr for crossing the aortic valve and safely’’landing’’ in the leftventricle. The guide catheter wasadvancedoverthepigtail,whichwasthenremoved,and placedinthemid-cavityoftheleftventricle.Thecatheter wasconnectedto thepressure system, initialLV pressure wasrecordedandaminimalamountofcontrastwasinjected (Figure1).A5.5 Fr Cordis104 cmor 5.4Fr Maslanka120 cm bioptome was advanced and the myocardial wall was sampled (Figure2). Back-bleedfrom the catheterand, if necessary, aspiration, were then performed to ensure no air bubbles were in the system. These steps were then repeatedseveraltimesuntilthedesirednumberofsamples
Figure1 Contrastinjectionintotheleftventricleafterguide catheterplacement.
Figure2 Bioptomedeploymentwithopenforceps, immedi-atelybeforesampling.
wasobtained---aminimumoffive---ofwhichatleastone wasfrozenforfurtheranalysis,ifnecessary.
Allmid-apical segmentsofallthewallsoftheleft ven-tricleweresampledbygentlydirectingthecatheterduring the procedure, guided by fluoroscopy and echocardiogra-phy.Firsttheguideispositionedusingfluoroscopyandthen confirmedbytransthoracicechocardiographybyanassisting physician.This enablesdetailed guideandbioptome posi-tioningand early identification of possible complications. Theprocesswasrepeatedforallsamples.
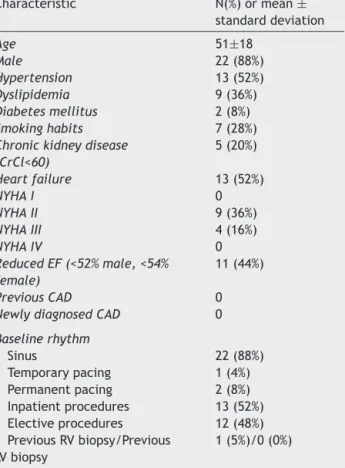
Table1 Baselineclinicalcharacteristics. Characteristic N(%)ormean± standarddeviation Age 51±18 Male 22(88%) Hypertension 13(52%) Dyslipidemia 9(36%) Diabetesmellitus 2(8%) Smokinghabits 7(28%)
Chronickidneydisease (CrCl<60) 5(20%) Heartfailure 13(52%) NYHAI 0 NYHAII 9(36%) NYHAIII 4(16%) NYHAIV 0 ReducedEF(<52%male,<54% female) 11(44%) PreviousCAD 0
NewlydiagnosedCAD 0
Baselinerhythm Sinus 22(88%) Temporarypacing 1(4%) Permanentpacing 2(8%) Inpatientprocedures 13(52%) Electiveprocedures 12(48%) PreviousRVbiopsy/Previous LVbiopsy 1(5%)/0(0%)
CrCl:creatinineclearance;CAD:coronaryarterydisease; EF: ejectionfraction;LV: left ventricular;NYHA:NewYorkHeart Association;RV:rightventricular.
Results
Baselinepopulationcharacteristics
Twenty-fivepatientswereselectedforintendedLV endomy-ocardialbiopsy. Twopatients underwent theprocedure in thesetting of cardiogenic shock of unknown etiology and were deemed better suited to a transfemoral approach, as mechanical circulatory support was being considered postprocedure.Transradialendomyocardialbiopsywasthus attemptedin25patients.Thebaselinedataareillustrated inTable1.
Technicaldata,successandcomplications
Allpatientsscheduledfortransradialbiopsyunderwentthe procedure successfully, with no cases of cross-over to a femoralapproach.Therewerenomajorcomplications,and only two cases of minor radial spasm. One of these two patientsalsohadarunofnon-sustainedventricular tachy-cardia(Table2).
Regardingthetwoabove-mentionedpatientswho under-wentprogrammedtransfemoralLVendomyocardialbiopsy, theprocedurewasalsosuccessfulwithnomajororminor complications.
Table2 Technicaldata,successandcomplications.
Parameter N(%)ormean± standarddeviation Success 25(100%) Cross-overtofemoral 0(0%) Majorcomplications 0(0%) Perforation 0(0%) Cardiactamponade 0(0%)
Denovoorincreasedmitral regurgitation
0(0%)
Embolization 0(0%)
PermanentAVblock 0(0%)
Tachycardiarequiringterminationby cardioversion 0(0%) Minorcomplications 2(8%)* Arrhythmias 1(4%) Sinusbradycardia 0(0%) TransientAVblock 0(0%)
Otherconductiondisturbance 0(0%)
Supra-ventriculartachycardia 0(0%)
Non-sustainedventricular tachycardia
1(4%)
Sustainedventriculartachycardia 0(0%)
Radialspasm 2(8%)**
Bleeding 0(0%)
Accesssitehematoma 0(0%)
Pseudoaneurysmoraneurysm formation
0(0%)
Rightradial/Leftradial 23(92%)/2(8%)
Concomitantcoronaryangiography 20(80%)
GuideCatheter MP1 19(76%) JR3.5/4 6(24%) Bioptome Cordis5.5Fr104cm 19(76%) Maslanka5.4Fr120cm 6(24%) Proceduraltime*** 35±8 Fluroscopytime*** 9±2 Numberofmyocardiumsamples
Mean±SD 7±1
Range 5-10
AV:atrioventricular;MP:Multipurpose;JR:JudkinsRight.
* Onepatient,twooverlappingminorcomplications. ** Mildradialspasm.
*** Includingcoronaryangiographywhenperformed.
Biopsyindication,resultsandfinalclinical
diagnosis
There were two main clinical settings for performing the procedure:myocarditisandcardiomyopathy.Thedetailsare providedinTable3.
Regardingmyocarditis,eightstudieswereperformed in thesetting of suspectedacutemyocarditis(Figure3Aand 3B).
Threepatientspresentedwithacutecoronarysyndrome chestpain-likesymptoms.Twoofthemunderwentthe pro-cedurebecauseofrecurrentmyocarditis.Thethirdpatient
Table3 Indicationforbiopsyandfinalresult.
Indication---N(%) FinalResult
Acutemyocarditis(clinicallysuspectedmyocarditis) 8(32%) 5confirmed 3ruledout
New-onsetHF 4(16%) 2confirmed
2ruledout
3rddegreeAVblock 1(4%) 1Ruledout
NosignsofHForseriousarrythmias 3(12%) 3confirmed
Chronicmyocarditis
(clinicallysuspected-DCMwithHF)
6(24%) 1confirmed
5ruledout
Hypertrophiccardiomyopathy 11(44%)
AHCMwithclinicalfeaturesofamyloidosis 2(8%) 2ATTRamyloidosis
Suspectedcardiacamyloidosiswithprevious inconclusivestudies
9(36%) 4ALamyloidosis
4ATTRamyloidosis 1ruledout
AHCM:apicalhypertrophiccardiomyopathy;ATTR:transthyretin;AL:amyloidlight-chain;AV:atrioventricular;DCM:dilated cardiomy-opathy;HF:heartfailure.
Figure3 (A)Focallymphocyticmyocarditis.Slightedemaandaprominentlymphocyticinfiltratearepresentintheinterstitium. Absenceoffibrosis(hematoxylinandeosin).(B)Interstitiallymphocyticinfiltrationandmyocytedamageintheformofapoptosis arepresent(hematoxylinandeosin).
underwenttheproceduredue toveryhigh troponinlevels and mildly impaired LV function, despite the absence of clinicalsignsofheartfailure.Allhadafavorableclinical out-comewithnormalizationofLVfunctionafterafewweeks. Theirfinaldiagnosiswasacutelymphocyticmyocarditis.One patienthad a mildly positive parvovirus B19result in the polymerasechainreaction(PCR)test.
Fourpatientsunderwenttheprocedurebecauseof new-onset heart failure of unknown etiology. They had no other characteristics of acute myocarditis but a poten-tially treatable type of myocarditis, such as giant cell myocarditis, was ruled out, thereby excluding an indica-tionforimmunosuppressiontherapy.Twoofthesepatients tested positive for acute lymphocytic myocarditis, onein the setting of Takayasu arteritis, and progressed favor-ably, with normalization of LV function after a few weeks.
One patient wasa 46-year-old patient withnew-onset third degree atrioventricular(AV) block.The biopsy ruled outmyocarditis,butshowedsomedegreeoffibrosis, possi-blyrelatedtopastradiotherapyyearsearlierinthesetting of Hodgkin’s lymphoma. The result helpedto explain the etiologyoftheAVblockatsuchayoungageandreinforced theneed forapermanentpacemaker, asthecauseof the bradycardiawasnotreversible.
Sixpatients underwenttheprocedure in thesetting of dilatedcardiomyopathyforruling outchronicmyocarditis. Theywereyoungpatients(agerange23-56years)refractory tomedicaltherapy for heart failuretitrated tomaximum doses. Only one met the formal pathological criteria of chronicmyocarditis.6ThestudyofviralgenomesbyPCRwas
negative.
Regardingthosepatientswhounderwenttheprocedure in the setting of cardiomyopathy, there were two cases of apical hypertrophy with imaging and clinical features ofconcomitantamyloidosis. Therefore,the exactetiology of their cardiomyopathy was not fully understood. Their finaldiagnosiswasfamilialtransthyretin(ATTR)amyloidosis (V30M mutation) cardiomyopathy. Nine patients under-wentendomyocardialbiopsyduetoamyloidosis(Figure4A, and 4C) of unknown etiology after earlier studies, which included laboratory workup and an abdominal fat biopsy. The echocardiograms of eight patients were highly sug-gestive of amyloidosis. The final diagnosis was amyloid light-chainamyloidosisinfourcases(resultingin hematol-ogyreferralforthestudyoflymphoproliferativediseases), wild type ATTR amyloidosis in four patients. Onepatient wasreferredbyanotherinstitutiontotheamyloidosisclinic becauseof an inconclusive echocardiogram together with a cardiac magnetic resonance raising the possibility of
Figure4 (A)Light-chaincardiacamyloidosis.Hyalinwidening of the interstitial space in the myocardial tissue (hema-toxylin and eosin). (B)Extracellular amyloid deposits inthe endocardiumandsurroundingthecardiomyocytes(Congored staining).(C)Lambda light-chainimmunostainingofthe peri-cellularamyloiddeposits(immunohistochemicalmethod with ananti-lambdalight-chainantibody).
amyloidosis,whichwasruledoutinthecardiacbiopsy.Itis noteworthythatallsixpatientswithATTRamyloiddeposits hadtheirTTRgenesequenced.
Finally, the two previously mentioned patients, who underwent the transfemoral procedure, were also new-onset heart failure cases with cardiogenic shock after cardiacarrest;myocarditiswasruledoutinboth.
Discussion
Inourinitialexperience,transradialendomyocardialbiopsy achieved excellent results, both regarding procedural
success and complications. Our research is supported by an increasing amount of publisheddata onthis particular approachtoendomyocardialbiopsy.
Safetyisthemajorconcernwhenperformingthis tech-nique,asmanypatientsareoftenyoung(especiallyinthe setting of myocarditis) and others have large ventricles withthinwalls.Wedidnotencounter safetyissues, espe-ciallyperforation,embolizationormitralregurgitation.This was likelythe result of specific operator training both in radialinterventionandLVbiopsy,aswellastechnicalsafety precautions. We highlight the useof pressure monitoring, extensive back bleed and catheter aspiration, as well as peri and intra-procedural echocardiography guidance. All oftheseenableconstantmonitoringoftheprocedure and minimizerisks.
As mentioned above, current guidelines regarding endomyocardialbiopsyarenowoveradecadeoldandbase their safety considerations on even older data.2 Indeed,
theserecommendationshighlight alargeseriesof transve-nousRVbiopsieswithanoverall6%complicationrate,a1.2% possibleordefiniteperforationrateand0.4%deathrate.14
Overthepastdecade,however,severalauthorsfrom expe-rienced European centers have published more extensive experience(rangingfrom755to4221procedures)totaling morethan 8000procedures.3,4,15 Inaddition,twoofthese
publications provide extensive data on both left and RV biopsy,therebyprovidingclearerdata.3,4Overall,the
pub-lishedmajorandminorcomplicationrateoftheseauthors rangesfrom0.12%to0.82%and1.35to5.2%,respectively, regardingRVbiopsies.3,4,15 TherateofLVbiopsymajorand
minor complications inLV biopsies was0.33 to0.64% and 2.2% to2.89%, respectively.3,4 Importantly, therewereno
deathsinanyoftheseseries.Mostmajorcomplicationswere perforationwithsubsequenttamponade.Averysmall num-berwerecasesofembolization.Severalminorcomplications includedbleedingorvascular-related.
Thesedataprovidevaluableinsightsintosafety.Firstly, the riskof theprocedure whenperformed in experienced centers is low, and seemingly lower than previously pub-lishedstudies;secondly,LVbiopsyseemsatleastassafe,if notsafer,thanRVbiopsy.
Publishedtransradialendomyocardialbiopsyexperience isquiterecent.Theearliestpublicationsdatebackto201412
and2015.10,11Thelargestseriespublishedtodatewas
mul-ticenterdatacomprisingover100patients.13Inallofthese
recent case series, there were no major complications. Furthermore,thelatter grouppublishedthelargestradial versusfemoralcaseseriescomparingbothapproaches,with 129casesviaradialand134casesviafemoralaccess.There werenomajorcomplicationsandbleedingoccurred exclu-sivelyinthetransfemoralgroup.16
Ourexperiencethus reflects the findingsin contempo-rarydata.Endomyocardialbiopsyisalargelysafetechnique, all the more so when performed via the left ventricle, especiallywiththeaddedsafetybenefitsofthetransradial approach.
Inthe seriespresentedherein, the feasibilityratewas 100%, with no cross-overs and only mild radial spasm observedintwopatients.Thiswaslikelytheresultofpatient selection, spasm prophylaxis administration, the use of hydrophiliccathetersandtheuseoflargesizeintra-luminal sheathlesscatheters,whichallowforcomfortablebioptome
passageandhave areducedexternal caliper.Importantly, patientfeedbackwasverypositiveandonepatient,whohad previously undergone a transjugular RV biopsy at another institution,actively voicedhispreference for the transra-dial technique, because of improved comfort. When the procedureisperformed electively,andifnocomplications occur,same-daydischargeispossible.Ourresultsare simi-lartopreviouslypublisheddata.Infact,inthelargestseries publishedtodate,cross-overtothefemoraltechniquewas requiredinonlyonepatient(0.98%).13
The lastissue regardingthis techniqueis itsdiagnostic yieldandclinicalusefulness.Inourexperience,inwhichLV biopsywasalwaysperformed outsidethesetting of trans-plant,theresultswereclinicallymeaningful,astheyadded totheclinicalquestionathand.Indeed,thesuspected diag-nosis was either confirmed or ruled out, such as in the setting of myocarditis. Additionally, a doubtful diagnosis wasclarified,suchastheetiologyofacardiomyopathy,or amyloidosisinfiltrationand/ortypeincaseswith predomi-nantheartinvolvementandpreviouslyinconclusivestudies. Finally,atypicalformsofLVhypertrophy(i.e.apical)were observedinpatientswithATTR,andtissuebiopsywasmost usefulforconfirmingamyloidosisandrulingouthypertrophy. Importantly,ourpathologist’sfeedbackwasalsovery pos-itive,as thequality andsize of the sampleswasdeemed excellentandbetterthanwhenwehadpreviouslyusedthe RVapproach.
The abovementioned papersfromthetransfemoral era suggestthattheLVapproachissuperiortotheRVapproach outside the transplant setting. Indeed, in the setting of myocarditis, the largest published series reports a 92.1% vs.81.3% diagnostic yield,4 andin thesetting of
predom-inant LVdisease, the differenceis quite large and the LV approachisfavoredwith97.8%vs.53%,respectively.3
Pub-lisheddatafromthetransradialapproachdonotallowfor acomparisonofleftversusright approaches,howeverthe conclusionsaresimilartoours:theresultsaddedtothe clini-caldilemma,confirming,excludingorclarifyingadiagnostic hypothesis.13
Despite its advantages, the transradial LV endomy-ocardial biopsy technique is not without limitations. This approach requires the use of heparin, which may add to the risk of bleeding. In casesin which repeatedbiopsy is required, such as transplant patients, radial patency and the risk of vascular complications may become an issue with frequent procedures. In addition, the LV approach, while apparently less prone to perforation, regardless of the access site, may lead to a more dangerous scenario should perforation occur, given the much higher intra-cavitary pressure of the left ventricle. Also, the risk of cerebral embolization is essentially a concern of the left, rather than the right, approach, and thus it can-not be performed in the presence of LV intracavitary masses.
It is also important to point out the particular limita-tionsofthispaper.Thisanobservationalsingle-centerstudy. Additionally, the sample size is relatively small given the single-centernatureofthedata.Andfinally,anultrasound studyoftheradialarterywasnotperformedafterthe pro-cedure. Thus, although therewas noclinical evidenceof radialpatencycomplications, thesecannotbe completely ruledout.
Conclusion
Transradial LVendomyocardial biopsy provides a safeand feasiblemethodofsamplingthemyocardiumfor histopatho-logicalanalysis,withagooddiagnosticyieldandclinically meaningful results in properly selected patients. This technique should probably be the default method for endomyocardialbiopsyinpatientsundergoingasinglebiopsy procedure outside the setting of cardiac transplant in a radialcenter.
Keypoints
- Whatisknownaboutthetopic?
◦ The indications for endomyocardial biopsy are still debated, partly becauseof safety concerns and doubts abouttheclinicalusefulnessoftheresults;
◦ RecentpaperssuggestthesafetyofLVbiopsyissuperior toRVbiopsy;
◦ Veryrecentdatasuggestthatthetransradialapproachis anewandbettermethodof samplingtheleftventricle whencomparedtothetransfemoralapproach.
- Whatdoesthisstudyadd?
◦ Additional dataconfirming that transradial LV biopsy is feasibleandsafe;
◦ Clinicaldataexplaininghowtheresultswereusefulina varietyofclinicalscenarios;
◦ Datatosupportthegrowingindicationsfor endomyocar-dialbiopsy.
Conflicts
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
References
1.SakakibaraS, Konno S.Endomyocardial biopsy. JpnHeart J. 1962:537---43.
2.Cooper LT, Baughman KL, Feldman AM, et al. The role of endomyocardial biopsyin themanagement ofcardiovascular disease:AScientificStatementfromtheAmericanHeart Asso-ciation,theAmericanCollegeofCardiology,andtheEuropean Society ofCardiology Endorsed bythe Heart Failure Society ofAmericaandtheHeartFailureAssociationoftheEuropean SocietyofCardiology.EurHeartJ.2007;8:3076---93.
3.ChimentiC,FrustaciA.Contributionandrisksofleft ventricu-larendomyocardialbiopsyinpatientswithcardiomyopathies: a retrospective study over a 28-year period. Circulation. 2013;128:1531---41.
4.Yilmaz A, Kindermann I, KindermannM, et al. Comparative evaluationofleftandrightventricularendomyocardialbiopsy: differencesincomplicationrateanddiagnosticperformance. Circulation.2010;122:900---9.
5.ValgimigliM,GagnorA,CalabróP,etal.Radialversusfemoral accessinpatientswithacutecoronarysyndromesundergoing invasivemanagement:arandomisedmulticentretrial.Lancet (London,England).2015;385:2465---76.
6.CaforioALP,PankuweitS,ArbustiniE,etal.,Currentstateof knowledgeonaetiology,diagnosis,management,andtherapy
ofmyocarditis:aposition statementoftheEuropeanSociety ofCardiologyWorkingGrouponMyocardialandPericardial Dis-eases.EurHeartJ.2013;34:2636---48.
7.DominguezF,KühlU,PieskeB,etal.Updateonmyocarditisand inflammatorycardiomyopathy:reemergenceofendomyocardial biopsy.RevEspa˜nolaCardiol(EnglishEd).2016;69:178---87.
8.PintoYM,ElliottPM,ArbustiniE,etal.,Proposalforarevised definitionofdilatedcardiomyopathy,hypokineticnon-dilated cardiomyopathy, and its implications for clinicalpractice: a positionstatementoftheESCworkinggrouponmyocardialand pericardialdiseases.EurHeartJ.2016;37:1850---8.
9.AgewallS,BeltrameJF,ReynoldsHR,etal.ESCworkinggroup position paperonmyocardial infarctionwithnon-obstructive coronaryarteries.EurHeartJ.2016;38,ehw149.
10.SchäufeleTG,SpittlerR,KaragianniA,etal.Transradialleft ventricularendomyocardial biopsy:assessmentof safetyand efficacy.ClinResCardiol.2015;104:773---81.
11.Schulz E, Jabs A, Gori T, et al. Feasibility and safety of leftventricularendomyocardialbiopsyviatransradialaccess: technique andinitialexperience.CatheterCardiovasc Interv. 2015;86:761---5.
12.BagurR,BertrandOF,BéliveauP,etal.Feasibilityofusing a sheathlessguidingcatheterforleftventricularendomyocardial biopsyperformedbytransradialapproach.JInvasiveCardiol. 2014;26:E161---3.
13.ChoudhuryT,SchäufeleTG,LaviS,etal.Transradialapproach for left ventricular endomyocardial biopsy. Can J Cardiol. 2018;34:1283---8.
14.DeckersJW,HareJM,BaughmanKL.Complicationsof transve-nousrightventricularendomyocardialbiopsyinadultpatients withcardiomyopathy:aseven-yearsurveyof546consecutive diagnosticproceduresinatertiaryreferralcenter.JAmColl Cardiol.1992;19:43---7.
15.HolzmannM,NickoA,KühlU,etal.Complicationrateofright ventricularendomyocardial biopsyviathefemoralapproach. Circulation.2008;118:1722---8.
16.ChoudhuryT,LurzP,SchäufeleTG,etal.Radialversusfemoral approachforleftventricularendomyocardialbiopsy. EuroInter-vention.2019.