r e v b r a s o r t o p . 2016;51(5):610–613
SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Case
Report
Anterior
avulsion
fracture
of
the
tibial
tuberosity
in
adolescents
–
Two
case
reports
夽
Aleilimar
Teixeira
da
Silva
Júnior,
Leonardo
Jorge
da
Silva,
Ulbiramar
Correia
da
Silva
Filho,
Edmundo
Medeiros
Teixeira,
Helder
Rocha
Silva
Araújo,
Frederico
Barra
de
Moraes
∗UniversidadeFederaldeGoiás,FaculdadedeMedicina,Goiânia,GO,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received15October2015
Accepted30October2015
Availableonline10August2016
Keywords:
Tibialfractures/surgery
Tibialfractures/radiography
X-raycomputedtomography
Kneeinjuries
a
b
s
t
r
a
c
t
Theobjectiveherewastoreporttworarecasesofanterioravulsionfractureofthetibial
tuberosityinadolescents.Case1wasa15-year-oldmalewhobecameinjuredthrough
land-ingonhisleftkneeandpresentedlimitedextension.Case2wasa16-year-oldbasketball
playerwhopresentedsuddenpainintherightkneeandfunctionalincapacity,afterajump.
Imagingexaminations(radiographsandcomputedtomography)showedanterioravulsion
fracturesofthetibialtuberosity.Surgicalfixationwasperformedusingscrewsandanchors,
whileavoidinggrowthplateinjury.Thecasesevolvedwithoutlower-limbdeformities.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Fratura-avulsão
tuberosidade
anterior
da
tíbia
em
adolescente
–
Relato
de
dois
casos
Palavras-chave:
Fraturasdatíbia/cirurgia
Fraturasdatíbia/radiografia
Tomografiacomputadorizadapor
raiosX
Traumatismosdojoelho
r
e
s
u
m
o
Oobjetivoérelatardoiscasosrarosdefratura-avulsãodatuberosidadeanteriordatíbiaem
adolescentes.Caso1:15anos,masculino,apresentoutraumaematerrissagememjoelho
esquerdo,comlimitac¸ãodaextensão.Caso2:16anos,jogadordebasquetecomdorsúbita
joelhodireitoeincapacidadefuncionalapóssalto.Examesdeimagem(radiografiase
tomo-grafias)evidenciaramasfraturas-avulsãodatuberosidadeanteriordatíbia.Feitafixac¸ão
cirúrgicacomparafusoseâncorasqueevitoualesãofisária.Evoluíramsemdeformidades
emmembrosinferiores.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora
Ltda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudycarriedoutattheUniversidadeFederaldeGoiás,FaculdadedeMedicina,HospitaldasClínicas,DepartamentodeOrtopediae
Traumatologia,Goiânia,GO,Brazil.
∗ Correspondingauthor.
E-mail:fredericobarra@yahoo.com.br(F.B.Moraes).
http://dx.doi.org/10.1016/j.rboe.2016.08.001
2255-4971/©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Thisisanopenaccessarticle
rev bras ortop.2016;51(5):610–613
611
Introduction
Theanteriortibialtuberosity(ATT)developsfromasecondary
ossificationcenterintheanterolateralaspectofthetibiain
contrasttotheossificationcenteroftheproximaltibia.The
ATTisanapophysisanddevelopsundertraction,1whilethe
proximal tibial core is developed under compression. The
developmentofATTisdividedintofourstages:cartilaginous,
apophyseal,epiphysealandbony.2
ATT avulsion-fractures in children and adolescents are
rare,withfewcasesdescribedintheliterature,corresponding
to1%ofallgrowthplateinjuries,3occurringpredominantlyin
males(approximately98%).4Theyaretheresultoftwo
pos-sible mechanisms: (1) abruptknee flexion with quadriceps
contraction,typicalofjumplanding; (2)violent quadriceps
contractionwithafixedfoot,asinjumping.5–7
Theaimofthisstudyistoreporttworarecasesofavulsion
fractureoftheanteriortibialtuberosityinadolescentstreated
surgically.
Case
reports
Case1
A15-year-oldmalepatientunderwenttraumawhilelanding
onhisleftkneeduringsoccerpractice;hedevelopedleftleg
edemaandextensionlimitation.Duringexaminationhe
pre-sentedbruising,painonpalpationoftheATT,edema2+/4+
leftlegextensionimpairment.Radiographies(Fig.1)andCT
scan(Fig.2)ofthekneedisclosuredavulsionfractureofthe
anteriortibialtuberositywithavulsionofthebonefragment.
Thepatient underwent surgicaltreatment through
fixa-tion ofthe avulsed bone fragment with amalleolar screw
andwasher,andreinsertionofthepatellartendonwiththree
anchors (Fig. 3). Early rehabilitationwith fullload and full
rangeofmotionwasperformedwithintwomonths.Sports
practiceresumedaftersixmonthspostoperatively.The
radio-graphic controlshowed normal growth without lower-limb
discrepancy. Thepatientdevelopednorecurvatumor
ante-curvatum.
Case2
A16-year-oldpatient,avarsitybasketballplayer,had
sudden-onset pain intheright kneeand functional disabilityafter
jumpingduringagame.Anavulsionfracturewasdiagnosed,
with the ATT fragment extending into the joint (Fig. 4A
andB).Immediatecarewascarriedoutwithimmobilization
and surgical treatmentwas accomplished sevendaysafter
traumaduetosignificantedema.Fixationusingscrewsand
anchors wasperformed underfluoroscopy controltoavoid
growthplatelesion(Fig.4CandD).Physicaltherapy
rehabil-itationstartedontheseventhpostoperativeday;thepatient
Fig.1–Clinicalaspectoftheleftknee(A)comparedwiththecontralateralone,showingsevereedemaintheanterior region;anteroposteriorradiographyoftheleftknee(B)demonstratingsofttissueedema;inprofile(C)showingtheATT fragmentavulsion.
612
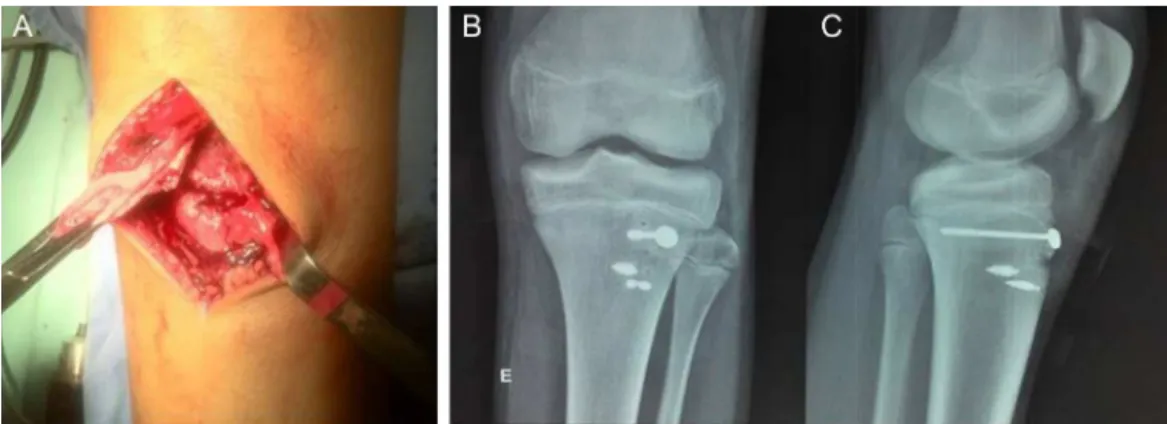
rev bras ortop.2016;51(5):610–613Fig.3–Intraoperativeimage(A)showingavulsedfragmentoftheATT;postoperativecontrolradiographiesin anteroposterior(B)andlateral(C)viewwithfixationusingscrewandanchors.
Fig.4–RadiographiesinAPandprofileoftherightkneeshowingATTavulsionfractureOgdentype3B(AandB); postoperativecontrolradiographies(CandD)after90daysofevolutionshowingconsolidationofATT.
developednolower-limbdeformitiesandreturnedtosports
practiceeightweeksafterthetrauma.
Discussion
Theavulsionfracturesoftheanteriortibialtuberosity
com-prehendahigher numberofinjuriesinmen,probably due
tothe highernumberofmenpracticingactivitiesinvolving
jumping.Inourcases,theyweretheresultsoftwopossible
mechanismsofaction:(1)abruptkneeflexionwithquadriceps
contraction,typicalofjump landing;(2)violent quadriceps
contractionwithafixedfoot,asinjumping.
Theoriginalclassificationsystemwascreatedby
Watson-Jones,8 whodefined threetypes.Type Iisan avulsionofa
smallportionofthetibialtuberosity,distaltothephysisof
theproximaltibia;TypeIIinvolvesthewholephysis,butdoes
notextendtothekneejoint;typeIIIcorrespondstoavulsion
thatextendsproximallytothekneegrowthplate.
ThisclassificationwasmodifiedbyOgdenandSouthwick,1
aimingatamoreaccuratedefinitionofthespecificfracture
patternsandprovidingtreatmentfordifferenttypesof
frac-tures, including displacement and fragmentation. Ryu and
Debenham3thensuggestedaddingatypeIV,whichisa
frac-tureofthetibialtuberositythatextendsposteriorlyalongthe
proximaltibialgrowthplate andcreatesanavulsionofthe
entireproximalepiphysis.Subsequently,theadditionofatype
CwasproposedbyFranklinetal.,9forfractureswith
associ-atedavulsionofthepatellarligament.Finally,atypeVwas
suggestedbyMcKoyandStanitski10alsodescribedbyCurtis,11
whichconsistedofafracturetypeIIIBwithanassociated
frac-turetypeIV,creatingaYconfiguration.
Thetreatmentoftheseinjuriesusingmethodsthatdonot
compromisefuturegrowthofthisregionrenderssome
diffi-cultyinmaintainingasatisfactoryfracturereductionagainst
the constant quadriceps pullforce. However, patientswith
thistypeofinjuryareoftenveryclosetotheendof
cartilagi-nousgrowth,whichallowsreductionandopenfixation,when
indicated,tobecarriedoutsafely.
Thus,typeIAOgdenfracturesareusuallytreated
conserva-tivelywithimmobilizationinextension,whileopenreduction
and rigidinternal fixation are recommended forthe other
types,withearlyphysicaltherapyrehabilitation.12Webelieve
thatearlydiagnosisandearlysurgicaltreatmentallowedgood
functionalresultsandreturntosportspracticeinthesecases.
Among the possible complications of this injury are:
limbdiscrepancy,genorecurvatum,3,4patellabaja,nonunion,
calcificationofthepatellartendonandanteriorcruciate
liga-mentinstability.1Complications,suchasthetibialtuberosity
fractures are relatively uncommon. However,compartment
syndromeisapotentiallyseverecomplicationthatshouldbe
consideredimmediatelyafterinjury.3–5
Conflicts
of
interest
rev bras ortop.2016;51(5):610–613
613
r
e
f
e
r
e
n
c
e
s
1. OgdenJA,SouthwickWO.Osgood–Schlatter’sdiseaseand tibialtuberositydevelopment.ClinOrthopRelatRes. 1976;(116):180–9.
2. EhrenborgG,EngfeldtB.Theinsertionoftheligamentum patellaeonthetibialtuberosity.Someviewsinconnection withtheOsgood–Schlatterlesion.ActaChirScand. 1961;121:491–9.
3. RyuRK,DebenhamJO.Anunusualavulsionfractureofthe proximaltibialepiphysis.Casereportandproposedaddition totheWatson–Jonesclassification.ClinOrthopRelatRes. 1985;194:181–4.
4. PeslT,HavranekP.Acutetibialtubercleavulsionfracturesin children:selectiveuseoftheclosedreductionandinternal fixationmethod.JChildOrthop.2008;2(5):353–6.
5. AlbuquerqueRP,GiordanoV,CarvalhoACP,PuellT, AlbuquerqueMIP,AmaralNP.Fraturaavulsãobilaterale simultâneadatuberosidadetibialemumaadolescente:relato decasoeterapêuticaadotada.RevBrasOrtop.
2012;47(3):56–60.
6.CarvalhoJúniorLH,BenevidesWA,NogueiraFCS,Fonseca WV,AndradeRP.Fraturasdatuberosidadetibialanteriorem adolescentes.Relatodecasoserevisãodaliteratura.RevBras Ortop.1995;30(1):70–3.
7.JakoiA,FreidlM,OldA,JavandelM,TomJ,RealyvasquezJ. Tibialtubercleavulsionfracturesinadolescentbasketball players.Orthopedics.2012;35(8):692–6.
8.Watson-JonesR.Fracturesandjointinjuries.4thed. Baltimore:Williams&Wilkins;1955.
9.FranklU,WasilewskiSA,HealyWL.Avulsionfractureofthe tibialtuberclewithavulsionofthepatellarligament.Report oftwocases.JBoneJointSurgAm.1990;72(9):1411–3.
10.McKoyBE,StanitskiCL.Acutetibialtubercleavulsion fractures.OrthopClinNorthAm.2003;34(3):397–403.
11.CurtisJF.TypeIVtibialtuberclefracturerevisited:acase report.ClinOrthopRelatRes.2001;389:191–5.