w w w . r b o . o r g . b r
Original
Article
Quality-of-life
assessment
among
patients
undergoing
total
knee
arthroplasty
in
Manaus
夽
Marcos
George
de
Souza
Leão
a,∗,
Erika
Santos
Santoro
a,
Rafael
Lima
Avelino
a,
Lucas
Inoue
Coutinho
a,
Ronan
Campos
Granjeiro
b,
Nilton
Orlando
Junior
aaOrthopedicsandTraumatologyService,Fundac¸ãoHospitalAdrianoJorge,Manaus,AM,Brazil bUniversidadedoEstadodoAmazonas,Manaus,AM,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received29November2012 Accepted9April2013
Availableonline27March2014
Keywords:
Knee/surgery Arthroplasty Qualityoflife Assessment
a
b
s
t
r
a
c
t
Objective:thisstudyhadtheaimofassessingthequalityoflifeamongpatientsundergoing totalkneearthroplasty(TKA).Forthis,theSF-36andWOMACquestionnairesrespectively wereusedtomakecomparisonswithpreoperativevalues.
Methods:aprospectiveobservationalcohortstudywasconducted,withblindedanalysison theresultsfrom107TKAsin99patients,betweenJune2010andOctober2011.Thepresent studyincluded55knees/patients,amongwhom73%werefemaleand27%weremale.The patients’meanagewas68years.TheSF-36andWOMACquestionnaires(whichhavebeen validatedforthePortugueselanguage)wereappliedimmediatelybeforeandsixmonths afterthesurgicalprocedure.
Results:thestatisticalandgraphicalanalysesindicatedthatthevariablespresentednormal distribution.Fromthedata,itwasseenthatalltheindicesunderwentpositivechangesafter thesurgery.
Conclusions:despitetheinitialmorbidity,TKAisaverysuccessfulformoftreatmentfor severeosteoarthritisoftheknee(i.e.morethantwojointcompartmentsaffectedand/or Ahlbackclassificationgreaterthan3),fromafunctionalpointofview,withimprovementof thepatients’qualityoflife,asconfirmedinthepresentstudy.Thisstudypresentedevidence levelIV(descriptionofcaseseries),withanalysisontheresults,withoutacomparativestudy. ©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Avaliac¸ão
da
qualidade
de
vida
em
pacientes
submetidos
à
artroplastia
total
do
joelho
em
Manaus
Palavras-chave:
Joelho/cirurgia Artroplastia Qualidadedevida Avaliac¸ão
r
e
s
u
m
o
Objetivo:avaliaraqualidadedevidaempacientessubmetidosàartroplastiatotaldojoelho (ATJ)comousodosquestionáriosSF-36(MedicalOutcomesStudy36–ItemShortForm HealthSurvey)eWOMAC(WesternOntarioandMcMasterUniversitiesOsteoarthritisIndex) ecompará-loscomosvalorespré-operatórios.
夽
WorkconductedattheOrthopedicsandTraumatologyService,Fundac¸ãoHospitalAdrianoJorge,Manaus,AM,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](M.G.deSouzaLeão).
2255-4971/$–seefrontmatter©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
Métodos:foifeitoumestudoprospectivo,observacional,coortecomanálisecegados resulta-dos,com107ATJem99pacientes,dejunhode2010aoutubrode2011.Incluídosnoestudo 55joelhos/pacientes:73%eramdosexofemininoe27%domasculino.Amédiadeidade foide68anos.ForamaplicadososquestionáriosSF-36eWOMAC,validadosparalíngua portuguesa,imediatamenteanteseseismesesapósoprocedimentocirúrgico.
Resultados:aanáliseestatísticaegráficaindicaqueasvariáveistiveramdistribuic¸ãonormal. Observandoosdados,verifica-sequetodososíndicessofreramalterac¸õespositivasdepois dacirurgia.
Conclusões: aartroplastiatotaldojoelho,apesardamorbidadeinicial,éumamodalidade bem-sucedidadetratamentoparaosteoartritegrave(maisdedoiscompartimentos articu-laresacometidose/ouclassificac¸ãodeAhlbackmaiordoque3)dojoelhodopontodevista funcional,commelhoriadaqualidadedevidadospacientes,dadosessesconfirmadosnesta pesquisa.NíveldeevidênciaIV,descric¸ãodesériedecasos,comanálisederesultados,sem estudocomparativo.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Accordingtothe WorldHealthOrganization(WHO),quality oflife(QoL) refersto individuals’perception oftheir posi-tioninlife,withintheculturalcontextandvaluesystemin whichtheyliveandinrelationtotheiraims,expectationsand socialstandards.QoLisasubjectiveconstructthatinvolves self-perceptionand iscomposedofmultiplepositive, nega-tiveandbidirectionaldimensions,suchasphysicalfunction andemotionalandsocialwellbeing.1
Indevelopedcountries,osteoarthrosis(OA)isthemost fre-quentcause ofincapacityamongmusculoskeletaldiseases, andthekneeismostfrequentsiteofinvolvement,with con-siderablydecreasedQoLamongtheindividualsaffected.Ithas beenestimatedthat4%oftheBrazilianpopulationsufferfrom OA.Thekneeisthejointthatissecondmostaffectedbythe disease,with37%ofthecases.2
Oneofthe waysofevaluatingthe functionallosses and treatments associated with knee OA consists of question-nairesinwhichindividualsreporttheirdifficulties.Because ofthe specificityofthe WOMACquestionnaire,it iswidely recommendedforthispurpose.In2002,theversionforthe Por-tugueselanguagewaspresented,withadaptationforBrazilian cultureinordertoeasecomprehensionamongreaders.The measurement, reproducibility and validity properties were welldemonstratedand theoriginalparameterswere main-tained.Hence,itbecameausefulinstrumentforevaluating thequalityoflifeofindividualswithOA.3
Total knee arthroplasty (TKA) has been recognized as oneofthemostsuccessfulorthopedicprocedures,withone ofthe best cost/benefit ratios within the field of orthope-dics. It provides significant QoL improvements and more than95%implantsurvivalafter15 years.4 TKAisareliable procedure forreducing the pain and incapacity associated with many pathological conditions of the knee, particu-larly OA. In conjunction with improvementof pain, gains in knee flexion are an important factor in relation to the resultandfunctional successafterTKA,giventhatthrough achievinggreaterflexion,itseemsthatpatientsareeven ben-efited in relationto going up and down stairs adequately. Theoverall resultsand findingsrelatingtosatisfactionand
improvementofQoLamongpatientsundergoingTKAneedto beconsidered.5
PatientsundergoingTKAexpectthebestresultpossible. Their expectations and satisfaction vary greatly, as do the instruments to measure these factors. Unsurprisingly, the reportsrelatingtopatientsatisfactionshowlargevariations. The role of expectations relating to obtaining satisfactory surgerystillrequiresclarificationintheliterature.Surgeons taketheviewthatexpectationsregardingtheresultsneedto beworkedon,evenbeforethesurgery.6
SF-36, an easily administered and understood generic instrument,canbeusedtoassessQoL.Thisisa multidimen-sionalquestionnairecomprising36itemswithineightscales orcomponents,anditisnotspecificforanygivenage,disease ortreatmentgroup.Itthereforeallowscomparisonsbetween differentpathologicalconditionsordifferenttreatments.7
ThisstudyhadthemainaimofevaluatingQoLandknee functionamongpatientsundergoingTKA,usingtheSF-36and WOMACquestionnaires,appliedbeforetheoperationandsix monthsafterwards,andtocomparethelatterwiththe preop-erativevalues.
Materials
and
methods
This was a prospective observational cohort study with blindedanalysisontheresults,inrelationto107TKA proce-duresthatwereperformedon99patientsbetweenJune2010 andOctober2011,withaminimumfollow-upofsixmonths.
Fromtheestimatedoverallpopulation,thesamplesizewas calculatedbymeansofaformulaforestimatingproportions forafiniteN.
The sample size was estimated in relation tothe total numberofpatientshospitalizedattheorthopedicsclinicof our institutionand wascalculated usingthe mathematical expressionshowninFig.1,inwhich:
ˆ ˆ
Z 2.p.q.N
ˆ ˆ
Z 2.p.q.N
d 2 (N-1) +
n =
N: Estimatedsize ofthe population studied, i.e.the total number ofpatients hospitalized inthe orthopedics clinic betweenJune2010andOctober2011(N=1518);
ˆ
p:Meanproportionofpatientswithintheinclusioncriteria ( ˆp=0.10);
ˆ
q:Non-incidentcases( ˆq=0.9);
d:Marginoferror(d=0.05);
Z:95%confidencecoefficient(Z=1.96).
Theprecisionlevel usedwas 5%,witha95% confidence level.Thus,asamplesizeof32patientswasobtained, consid-eringthattheapproximateproportionofpatientswhowere withintheinclusioncriteriareached10%.
The inclusion criteria were as follows: varus deviation greaterthan15◦;valgusdeviationgreaterthan10◦(measured usingtheanatomicalaxesofthefemurandtibia); femorotib-ialsubluxationinthefrontalplane;anteriorizationofthetibia inrelationtothefemuronlateralradiographs;severe com-promisingoftwoofthethreecompartmentsoftheknee;or arthrotickneeswithoutanyoftheabovealterationsthatwere refractorytoconservativetreatmentforatleastsixmonths. TheAhlbäckclassification,8asmodifiedbyKeyesetal.,9was usedforradiographicstagingofthedegenerativediseaseof theknee,inwhich56.4%ofthepatientspresentedtypeIV. Regardingtheangulardeformity(deviationfromtheaxis),76% ofthekneespresentedvarusdeformity(lessthan5◦valgusin relationtothefemorotibialanatomicalaxis,withameanof 2◦andrangefrom5◦valgusto18◦varus)andonly24%ofthe kneespresentedvalgusdeformity(morethan7◦valgusin rela-tiontothefemorotibialanatomicalaxis,withameanof13◦ andrangefrom8◦to25◦).
Amongthepatientswhofulfilledtheprofileforundergoing thesurgicalprocedure,73%werefemaleand27%weremale, withaminimumageof49yearsandmaximumof91(mean: 68).Therightsideaccountedfor60%ofthecases.
Fifty-fivepatientswereexcludedfromthestudyforthe fol-lowingreasons:undergoingbilateralTKA(16);arthrosisdue toinflammatorycauses (three);death(three);psychological abnormalities that impeded understanding of the protocol (four);refusaltosignthefreeandinformedconsentstatement (seven);secondaryarthrosis(two);infection(three);andloss offollow-up(17).Thus,71operatedkneeswereexcludedand 36kneesremainedtobestudied.Allthepatientssignedan informedconsentstatementbeforetheywereincludedinthe study,andthisstatementhadbeenevaluatedandapproved bythehospital’sethicscommittee,undertheprotocolnumber 01259112.1.0000.0007.
Intheeveningbeforethesurgicalprocedure,thepatient receivedtheWOMACandSF-36protocolstobeansweredand handedinonthemorningofthesurgery.Alltheprocedures were carriedout bythe same knee specialistsurgeon. The operationswereperformedusingthesameanesthetic tech-niqueandthesamejointaccessroute(mediallythroughthe vastus;personalpreference).Thesurgicalprocedurefollowed wasinconformitywiththetechnicalstandardsforTKAand totalkneeprosthesesmadebyBaumer(AKSmodel)wereused. Six months after the operation, the patients were reassessedbyanotherkneespecialistsurgeonwhohadnot had previous outpatient contact and had not participated in the surgical procedure. New radiographs of the knee
wereproducedinanteroposteriorandlateralviewsandnew WOMACandSF-36protocolswerehandedin,inordertorecord andcomparetheresults.SincetheWOMACscaleiscounted from 0(best result) to 96 (worst result),and withthe aim offacilitatingcomprehensionandanalysisoftheresults,we invertedtheLikertscale(thepsychometricresponsescale gen-erallyusedinquestionnairesandtheonemostusedinopinion polls)oftheoriginalquestionnaire.Inansweringa question-nairebasedonthisscale,therespondentsspecifytheirlevelof agreementthroughanaffirmation.Thisscaleisthusnamed becauseofareportpublishedbyLikerttoexplainitsuse10:“1” istheworstresultand“5”isthebest,withineachresponse(in theoriginalquestionnaire,thebestresultwas0andtheworst was4).
For thestatistical analyses,theMinitab14 softwareand theStatisticalPackagefortheSocialSciences(SPSS),version 13.0,wereused.Thedatawerethensubjectedtodescriptive statisticalanalysis.Toassessnormality,theShapiro–Wilktest wasused,andtoevaluateassociationsbetweenthe categor-icalvariables,Pearson’schi-squaretestwasused,orFisher’s exacttestwhennecessary.
Results
One indicationofnormalprobability ongraphs isthat the cloud of pointshas tobe around astraight line. It canbe
seenfromFigs.2–7thatthesepointsarearoundthestraight
line,whichgivesanindicationthattheobservationspresent normality.
Student’sttestandthenonparametricWilcoxontestwere performedtocomparethevariables.TheQoLindexmeasured usingtheSF-36andWOMACquestionnairesimproved signif-icantlyafterthesurgery.
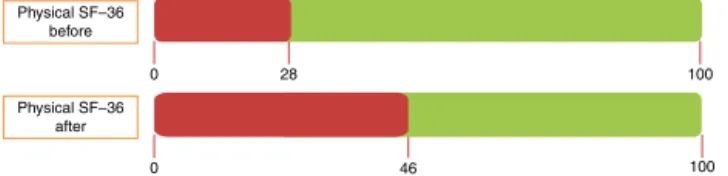
Figs. 8–10show thattheSF-36indicesimprovedin
rela-tiontotheanalysisdonebeforethesurgery,butthatonlytwo variablesreached50%ofthemaximumvalue,whichwerethe mentaldomainofSF-36(meanof39beforetheoperationand 52afterwards)andWOMAC(meanof28beforetheoperation and85afterwards).ThephysicaldomainoftheSF-36didnot reachapostoperativechangeofmorethan50%.Itstartedfrom ameanof28beforetheoperationandreachedameanof46 aftertheoperation.
ItshouldbeemphasizedthatbecauseWOMACisa spe-cificindexforkneeandhipOA,itspostoperativechangeswere morepronounced.
Discussion
Traditionally,the conceptofQoLwas delegatedto philoso-phers and poets. However, amongdoctorsand researchers today, thereisgrowing interest intransformingthis into a quantitativemeasurementthatcouldbeusedinclinicaltrials andfromwhichtheresultsthusobtainedcouldbecompared betweendifferentpopulationsandevenbetweendifferent dis-eases.
99
95
90
80 70 60 50 40 30 20
10
5
1
10 20 30 40 50
Physical SF before operation Normal probability plot for physical SF-36 before operation
Mean 27.96
7.400 55 0.141 <0.010 Standard Deviation N
KS p-value
P
e
rcent
Fig.2–NormalprobabilityofthephysicalvariableofSF-36beforetheoperation.
99
95
90
80
70
60 50 40 30
20
10
20 30 40 50 60 70
5
1
P
ercent
Mean 45.73 9.154 55 0.139 < 0.010 Standard Deviation N
KS p-value
Normal probability plot for physical SF-36 after operation
Physical SF after operation
Fig.3–NormalprobabilityofthephysicalvariableofSF-36aftertheoperation.
99
95
90
80
70
60 50
40 30
20
10
5
1
P
ercent
0 10 20 30 40 50 60 70 80 90
Mental SF before operation
Mean 39.11 13.21 55 0.095 > 0.150 Standard Deviation N
KS p-value
Normal probability plot for mental SF-36 before operation
99
95
90
80
70
60 50 40
30
20
10
5
1
P
ercent
Normal probability plot for mental SF-36 after operation
Mean 52.38 7.595 55 0.100 > 0.150 Standard Deviation N
KS p-value
30 40 50 60 70
Mental SF after operation
Fig.5–NormalprobabilityofthementalvariableofSF-36aftertheoperation.
99
95
90
80
70 60 50 40 30
20
10
5
1
P
ercent
Normal probability plot of WOMAC before operation
Mean 28.47 14.98 55 0.142 <0.010 Standard Deviation N
KS p-value
–10 0 10 20 30 40 50 60 70
WOMAC before operation
Fig.6–NormalprobabilityoftheWOMACvariablebeforetheoperation.
99
95
90
80
70
60
50 40
30
20
10
5
1
P
ercent
Normal probability plot of WOMAC after operation
Mean 83.10 10.22 55 0.151 >0.010 Standard Deviation N
KS p-value
50 60 70 80 90 100 110
WOMAC after operation
0
0
28
46
100
100 Physical SF–36
after Physical SF–36
before
Fig.8–MeanscoresforthephysicalvariableofSF-36 beforeandaftertheoperation.
0 39
52 0
100
100 Mental SF–36
after Mental SF–36
before
Fig.9–MeanscoresforthementalvariableofSF-36before andaftertheoperation.
WOMAC before
WOMAC after 0
0
28
85 100 100
Fig.10–MeanscoresfortheWOMACvariablesbeforeand aftertheoperation.
and alsothe decreasedbirthrate, healthcarepolicies have been ledto focus fullattention on elderly people’shealth. Inenvironmentswithlimitationsonresources,resultsfrom questionnairesareofparticularimportanceforcomparingthe cost/benefitratiosofmedicalinterventions.11
SF-36isagenericinstrumentforassessingQoLthatwas created in1976.12 Itiseasy toadministerand understand, butitisnotasextensiveaspreviousprotocols.Itisa multidi-mensionalquestionnaireformedby36itemsthataregrouped intoeightscalesorcomponents:functionalcapacity,physical aspects,pain,generalstateofhealth,vitality,socialaspects, emotionalaspectsandmentalhealth.Thesearegroupedinto twomajordomains (physicalandmental)thatcanbe ana-lyzedindependently.Theypresentafinalscorefrom0to100, inwhich0correspondstotheworstgeneralstateofhealth and100tothebeststate.13
OAismanifestedmainlythroughjointpain.Inthe begin-ning,it ismild,intermittent andoflowintensity.Withthe progressionofthedisease,it becomescontinuous and dif-fuse,withbasicallymechanicalcharacteristics.Theevolution oftheprocessleadstograduallossofjointstabilityand conse-quentlytopainofgreaterintensity,withfunctionallimitation ofthejoint.14
WOMACis aninstrument developed in19825–16 foruse amongpatientswithkneeorhipOAanditcontains24 ques-tionedthat aregroupedinthreedimensions:fivetoassess pain, two for joint stiffness and 17 for physical capacity. WOMACscorescanrangefrom0and96andcanbedivided intothreedifferentscores:pain(0–20),articularstiffness(0–8) andphysicalcapacity(0–68).Thehigherthescoreis,theworse
thedimensionevaluatedis.Itiswidelyusedinclinicaltrials asameasurementoftheevolutionoftreatmentresults,and alsoinpopulation-basedstudies.17
TKAhastheaimsofrelievingpain,correctingdeformities, enablingfunctionalrangeofmotionandmaintainingstability andfunctionofthekneeforday-to-dayactivities.18,19
Surgery is indicated if conservative treatment fails. In planningthisapproach,thepatient’sage,physicaldemands, expectationsregardingthetreatmentresults,typeof arthro-sis,bodyweightanddiseaseevolutionneedtobetakeninto consideration.20
The indication forTKA is based on the deviationfrom theaxis,compromisingofthekneejointcompartmentsand patient’s age, along with the functional incapacity caused bypainthat isrefractorytoconservative treatmentandby diminishedrangeofmotion.Classically,thesetof deformi-tiesdeterminesthecriteriaforindicatingTKA:varusdeviation greaterthan15◦;valgusdeviationgreaterthan10◦; femorotib-ialsubluxationinthefrontalplane;anteriorizationofthetibia inrelationtothefemuronlateralradiographsandsevere com-promisingoftwoofthethreekneejointcompartments,going from obliterationof the joint space and major outgrowths of osteophytosis to femorotibial subluxationin the frontal plane.14
AccordingtoBugała-Szpak etal.,21 age, sex,presenceof otherimplantsandpreoperativekneecontracturedonotgive rise to significant differences in the scores of knee ques-tionnairesforevaluatingQoL,andthiswascorroboratedby Mahomedetal.22However,theresultsfromarthroplastywere betteramongpatientswhosepreoperativerange ofmotion was greater than 90◦ and this is importantfrom a clinical point of view,since the functional resultalso depends on the patients’ capacity toflex the operatedknee. The posi-tive effects from the surgery, functional rehabilitation and improvement ofQoL could beseen as early as the fourth weekoffollow-upafterTKAinthestudybyBertschetal.23 andalsoaspredictorsofself-perceivedhealthoneyearafter surgery,accordingtoBaumannetal.24Thisimprovementof QoL occurred mainly in the domains of physical function and emotionalstatus. Personalsatisfactionisanimportant indicator of health that is rapidly available to doctors. In 2012,Lavernia etal.25 stated thatthe biggestimprovement ofpain and physicalfunction occurred withinthree tosix monthsafterthesurgery,whichcorroboratedtheapplication ofquestionnairessixmonthsafterthesurgicalprocedure.The improvementinhealthrelating toQoLaftersurgeryisalso evidentandincludesdomainssuchassocialfunction,mental healthandvigor.25
According to Babazadehet al.,26 changes to the height of the joint line ofthe prosthesiswere related to changes tothe range ofmotionand significantlyaffected the func-tionalresults.TherecentresultsfromthestudybyHofmann et al.27 showed that there was a correlation between the postoperativeradiographicevaluationandthevarious clini-calscores.TheseauthorssuggestedthattheQoLscoreshould beincludedintheTKAfollow-up.Inthisstudy,theclinical resultsobtainedwere betterwhenthejointlinewas repro-ducedanatomically.
ThepatientsatisfactionrateafterTKAishigh(90%)and93% ofthe patientswould undergo this procedure again.29 The QoL results demonstrated that TKA presents an excellent cost/benefitrelationship and analysison publishedstudies showsthatitisahighlyeffectiveprocedure,withfavorable resultsfromsurgicalinterventions.21–25Thedimensionscores from WOMAC, especially pain, improved significantly after sevenyearsand were influencednegatively byobesityand complicationsafterhospitaldischarge,accordingtoastudy byNú ˜nezetal.30
Although the advantages of TKA have already become established,someauthors31–37 demonstratedthatonly81% ofthepatientsexpressedtotalsatisfactionwithprimaryTKA and,whenaskedaboutimprovementsinpainandfunction withregardtoperformingactivitiesofdailyliving,theranges were from 72% to86% and from 70% to 84%,respectively. Themainfactorsassociatedwiththisdissatisfactionwerethe patients’realexpectations;lowpreoperativeWOMACscore; lowWOMACscoreafteroneyearoffollow-up;and complica-tionsthatledtoreadmissiontohospital.
Inthepresentstudy,therewasalargeandstatistically sig-nificantimprovementinpostoperative WOMACscore, with datasimilartotheliterature.30–35
Despitetheshorttimeintervalbetweenthesurgical pro-cedureandapplicationofthequestionnaires,thereisbacking intheliteratureforthis24andthescoresfoundinthepresent studyweresimilartothoseofpreviousstudiescitedabove.
Withtheaimofdiminishingthebiasinapplyingthe ques-tionnaires,theywere filledout bythe patientsthemselves; thesix-monthassessmentwasconductedbyanothersurgeon whohadnotparticipatedinthesurgeryandthepatientswere notregisteredinthissurgeon’soutpatientclinic.The limita-tionsofthepresentstudythatcanbecitedincludethelack ofdivisionofthe patientsaccordingtothetypeofimplant (withorwithoutpreservationoftheposteriorcruciate liga-ment),useofpatellaresurfacingornotandthedegreeand typeofdeformity(varusorvalgus).However,thesewerenot objectivesofthepresentstudy.
Conclusion
Withthesampleevaluated,theresultswereabsolutely coher-ent in relation to the literature. They confirm TKA as an establishedprocedurewithsubstantialimprovementofQoL.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. DiasRC,DiasJMD.Avaliac¸ãodaqualidadedevida
relacionadaàsaúdeemidososcomosteoartritedejoelhos.
RevBrasFisioter.2002;3(6):105–11.
2. VasconcelosKSS,DiasJMD,DiasRC.Relac¸ãoentre
intensidadededorecapacidadefuncionalemindivíduos
obesoscomosteoartrosedejoelho.RevBrasFisioter.
2006;2(10):213–8.
3.FernandesMI.Traduc¸ãoevalidac¸ãodoquestionáriode
qualidadedevidaparaosteoartroseWomac(WesternOntario
McMasterUniversities)paraalínguaportuguesa[tese].São
Paulo:UniversidadeFederaldeSãoPaulo;2002.
4.MatosLFC,AlvesALQ,SobreiroAL,GiordanoMN,
AlbuquerqueRSP,CarvalhoACP.Navegac¸ãonaartroplastia
totaldojoelho:existevantagem?ActaOrtopBras.
2011;19(4):144–8.
5.MeneghiniRM,PiersonJL,BagsbyD,Ziemba-DavisM,Berend
ME,RitterMA.Isthereafunctionalbenefittoobtaininghigh
flexionaftertotalkneearthroplasty?JArthroplasty.2007;226
Suppl.2:43–6.
6.CullitonSE,BryantDM,OverendTJ,MacDonaldSJ,Chesworth
BM.Therelationshipbetweenexpectationsandsatisfaction
inpatientsundergoingprimarytotalkneearthroplasty.J
Arthroplasty.2012;27(3):490–2.
7.HayesV,MorrisJ,WolfeC,MorganM.TheSF-36healthsurvey
questionnaire:isitsuitableforusewitholderadults?Age
Ageing.1995;24(2):120–5.
8.AhlbäckS.Osteoarthrosisoftheknee.Aradiographic
investigation.ActaRadiolDiagn(Stockh).1968;277:7–72.
9.KeyesGW,CarrAJ,MillerRK,GoodfellowJW.Theradiographic
classificationofmedialgonarthrosis.Correlationwith
operationmethodsin200knees.ActaOrthopScand.
1992;63(5):497–501.
10.LikertR.Atechniqueforthemeasurementofattitudes.Arch
Psychol.1932;140:1–55.
11.WiklundI,RomanusB.Acomparisonofqualityoflifebefore
andafterarthroplastyinpatientswhohadarthrosisofthe
hipjoint.JBoneJointSurgAm.1991;73(5):765–9.
12.WareJrJE.Scalesformeasuringgeneralhealthperceptions.
HealthServRes.1976;11(4):396–415.
13.CiconelliRM.Traduc¸ãoparaoportuguêsevalidac¸ãodo
questionáriogenéricodeavaliac¸ãodequalidadedevida
MedicalOutcomesStudy36–ItemShortFormHealthSurvey
(SF-36)[tese].SãoPaulo:UniversidadeFederaldeSãoPaulo;
1997.
14.RodriguesMB,FullerR.Artrosenojoelho.In:PécoraJR,
HernandezAJ,CamanhoGL,editors.Artrosedojoelho–
Gêneseesoluc¸ões.SãoPaulo:Atheneu;2010.p.44–50.
15.BellamyN.Osteoarthritis–anevaluativeindexforclinical
trials[thesis].Hamilton,Ontario,Canada:McMaster
University;1982.
16.BellamyN.Womacosteoarthritisindexuserguide.Version
VII.Australia:Brisbane;2005.
17.MedeirosM,Sousa,D.Instrumentopararastreamentodedor nojoelho(Knest)emnívelprimáriodesaúde:traduc¸ão, adaptac¸ãoculturaleresultadosdesuaaplicac¸ãoemidosos residentesdeumaáreaurbanadoBrasil.Availablefrom:
http://www.clinicapinheirofranco.com.br/PDF/questionario
qualidadedevida2.pdf
18.BuechelFF,PappasMJ.Long-termsurvivorshipanalysisof
cruciate-sparingversuscruciate-sacrificingkneeprostheses
usingmeniscalbearings.ClinOrthopRelatRes.
1990;(260):162–9.
19.BongMR,CesarePE.Rigidezapósartroplastiatotaldejoelho.J
AmAcadOrthopSurg.2004;2:227–34.
20.MelloJuniorWA,PenteadoPCF,BritoWE,StumpX.Joelhodo
adulto.In:HebertS,editor.Ortopediaetraumatologia:
princípioseprática.4thed.PortoAlegre:Artmed;2009.p.
506–13.
21.Bugała-SzpakJ,KuszD,Dyner-JamaI.Earlyevaluationof
qualityoflifeandclinicalparametersaftertotalknee
arthroplasty.OrtopTraumatolRehabil.2010;12(1):41–9.
22.MahomedNN,LiangMH,CookEF,DaltroyLH,FortinPR,
FosselAH,etal.Theimportanceofpatientexpectationsin
predictingfunctionaloutcomesaftertotaljointarthroplasty.J
23.BertschC,HolzU,KonradG,VakiliA,OberstM.Earlyclinical
outcomeafternavigatedtotalkneearthroplasty.Comparison
withconventionalimplantationinTKA:acontrolledand
prospectiveanalysis.Orthopade.2007;36(8):
739–45.
24.BaumannC,RatAC,MainardD,CunyC,GuilleminF.
Importanceofpatientsatisfactionwithcareinpredicting
osteoarthritis-specifichealth-relatedqualityoflifeoneyear
aftertotaljointarthroplasty.QualLifeRes.2011;20(10):1581–8.
25.LaverniaCJ,AlcerroJC,BrooksLG,RossiMD.Mentalhealth
andoutcomesinprimarytotaljointarthroplasty.J
Arthroplasty.2012;27(7):1276–82.
26.BabazadehS,DowseyMM,SwanJD,StoneyJD,ChoongPF.
Jointlinepositioncorrelateswithfunctionafterprimarytotal
kneereplacement:arandomizedcontrolledtrialcomparing
conventionalandcomputer-assistedsurgery.JBoneJoint
SurgBr.2011;93(9):1223–31.
27.HofmannAA,KurtinSM,LyonsS,TannerAM,BolognesiMP.
Clinicalandradiographicanalysisofaccuraterestorationof
thejointlineinrevisiontotalkneearthroplasty.J
Arthroplasty.2006;21(8):1154–62.
28.VandenBoomLG,BrouwerRW,vandenAkker-ScheekI,
BulstraSK,vanRaaijJJ.Retentionoftheposteriorcruciate
ligamentversustheposteriorstabilizeddesignintotalknee
arthroplasty:aprospectiverandomizedcontrolledclinical
trial.BMCMusculoskeletDisord.2009;10:119.
29.BourneRB.Measuringtoolsforfunctionaloutcomesintotal
kneearthroplasty.ClinOrthopRelatRes.2008;466(11):
2634–8.
30.Nú ˜nezM,LozanoL,Nú ˜nezE,SegurJM,SastreS,MaculéF,
etal.Totalkneereplacementandhealth-relatedqualityof
life:factorsinfluencinglong-termoutcomes.Arthritis
Rheum.2009;61(8):1062–9.
31.AndersonJG,WixsonRL,TsaiD,StulbergSD,ChangRW.
Functionaloutcomeandpatientsatisfactionintotalknee
patientsovertheageof75.JArthroplasty.1996;11(7):831–40.
32.DunbarMJ,RobertssonO,RydL,LidgrenL.Appropriate
questionnairesforkneearthroplasty.Resultsofasurveyof
3600patientsfromTheSwedishKneeArthroplastyRegistry.J
BoneJointSurgBr.2001;83(3):339–44.
33.HawkerG,WrightJ,CoyteP,PaulJ,DittusR,CroxfordR,etal.
Health-relatedqualityoflifeafterkneereplacement.JBone
JointSurgAm.1998;80(2):163–73.
34.JanseAJ,GemkeRJ,UiterwaalCS,vanderTweelI,KimpenJL,
SinnemaG.Qualityoflife:patientsanddoctorsdon’talways
agree:ameta-analysis.JClinEpidemiol.2004;57(7):653–61.
35.JornLP,JohnssonR,Toksvig-LarsenS.Patientsatisfaction,
function,andreturntoworkafterkneearthroplasty.Acta
OrthopScand.1999;70(4):343–7.
36.KaneR,SalehK,WiltT,BershadskyB,CrossW3rd,
MacDonaldR,etal.Totalkneereplacement.Evidencereport. TechnologyAssessment(PreparedbytheMinnesota Evidence-BasedPracticeCenter,Minneapolis,MN).AHRQ Publication,no.04-E006-2;2003;8:1–8.
37.MäntyselkäP,KumpusaloE,AhonenR,TakalaJ.Patients’
versusgeneralpractitioners’assessmentsofpainintensityin
primarycarepatientswithnon-cancerpain.BrJGenPract.