249
Rev Bras Psiquiatr 2003;25(4):249-52
Quality of life: presentation of the concept
In modern medicine the traditional way of assessing change in patients has been to focus on objective clinical or biological tests. While these do offer important information about patho-logical processes, it is impossible to separate the disease itself from an individual’s personal point of view and social perspec-tive. One way of capturing these particular perspectives is by using quality of life (QOL) measurements.1
Although the notions of good life and the nature of health have been considered by philosophers, theologians, and scien-tists for centuries, the concept of ‘quality of life’ is a fairly new
atualização
“Quality of life”: a brand new concept for research and
practice in psychiatry
“Qualidade de vida”: um novo conceito para a pesquisa e prática em
psiquiatria
Marcelo T Berlima and Marcelo P A Fleckb
aMood Disorders Program (PROTHUM), Hospital de Clínicas de Porto Alegre (HCPA). Porto Alegre, RS, Brazil. bDepartment of Psychiatry and Forensic
Medicine, Federal University of Rio Grande do Sul (UFRGS), and PROTHUM, HCPA. Porto Alegre, RS, Brazil
This work was performed at the Department of Psychiatry and Forensic Medicine, Federal University of Rio Grande do Sul. None financial support and conflict of interest.
Received on 6/11/2002. Approved on 30/5/2003.
Since the ‘70s, the assessment of quality of life (QOL) has grown from a ‘small cottage’ industry to a formal discipline within a coherent theoretical framework, accepted methods, and manifold applications. In recent years, QOL has become increasingly popular as a useful variable tailored to assess the overall impact of diseases and medical treatments from the patient’s point of view. In this updating paper, we describe the most frequently used instruments, and discuss the conceptual and practical issues concerning QOL evaluation, as applied to the study of mental disorders. In addition, we present a unifying definition of QOL that has recently been developed by the World Health Organization. Finally, we conclude that QOL measures are potentially useful methods to be applied to research and clinical practice in psychiatry - especially when used to demonstrate the impact of mental illnesses and the possible benefits of therapeutic interventions.
Psychiatry. Quality of life. Scientific research. Clinical practice.
Desde os anos 70, a avaliação da qualidade de vida (QV) cresceu de uma atividade relativamente restrita para uma disciplina formal com uma estrutura teórica coesa, métodos consagrados e diversas aplicações. Nos últi-mos anos, a QV vem se tornando cada vez mais popular como uma variável útil para determinar o impacto global das doenças e dos tratamentos médicos a partir da perspectiva do paciente. Nesse artigo de atualização, nós descrevemos os instrumentos mais freqüentemente utilizados e discutimos as questões conceituais e práti-cas envolvidas na avaliação da QV quando aplicada ao estudo dos transtornos mentais. Além disso, nós apre-sentamos uma definição unificada de QV, recentemente desenvolvida pela Organização Mundial de Saúde. Por fim, concluímos que as medidas de QV são potencialmente úteis para aplicação na pesquisa e na prática clínica em Psiquiatria – especialmente para demonstrar o impacto das doenças mentais e o possível benefício das intervenções terapêuticas.
Psiquiatria. Qualidade de vida. Pesquisa científica. Prática clínica.
Abstract
Keywords
Resumo
Descritores
one. It was introduced in 1975 as a key term in medical in-dexes, and its systematic study started in the early ‘80s mainly within oncology, since physicians were confronted with the problem that the cure could be too high a price to pay for the resulting increase in life expectation.2,3 Indeed, oncologists were
among the first physicians confronted with the dilemma: ‘Should we add years to life or life to years?’.
Rev Bras Psiquiatr 2003;25(4):249-52
250
Quality of life: a new concept for psychiatry Berlim MT & Fleck MPA
how patients feel and how satisfied they are with treatment, besides the traditional focus on disease outcomes.1,4 Since the
term embraces a whole spectrum of uses and meanings, and is employed both as a fashionable catch-phrase and a scientific concept, it needs careful evaluation. All too easily can it be-come a vague label for a state of subjective well-being, with questionable scientific value.4
When adequately measured, QOL has been used to distin-guish different patients or groups of patients, to predict indi-vidual outcomes, and to evaluate the effectiveness of thera-peutic interventions.5-7 In addition, QOL evaluation has a
num-ber of potential uses in aiding routine clinical practice: it can help physicians to prioritize problems, to communicate better with patients, to screen for potential adversities, and to iden-tify patients’ preferences.1,8 Fortunately, these measures are now
becoming more valued in psychiatry, particularly in those branches dealing with chronic disabling disorders.2
However, when applying the QOL concept to the field of mental health, its strengths and weaknesses become especially obvious, and both result from the fact that QOL is an open self-evaluated construct. Its strengths lie in its potential for in-tegrating the views of different players in the mental healthcare field, while its weaknesses reside in its large scope, at the risk of becoming vague. Indeed, despite the proliferation of instru-ments and the burgeoning theoretical literature devoted to the assessment of QOL, no unified approach has been devised for its measurement, and little agreement has been attained on what it means.2,4 In fact, the term ‘quality of life’, as applied in the
medical literature, may not have a distinctive or unique mean-ing.5,6 Current concepts range from those with a holistic
em-phasis on the social, environmental, and physical well-being of patients after treatment to those that describe the impact of a person’s health on his/her ability to lead a fulfilling life.8,9
Ad-ditionally, many investigators seem to substitute QOL for other terms intended either to describe patients’ health (such as ‘health/functional status’) or to summarize those aspects of life quality or function which are impacted by one’s health status (the ‘health-related QOL’).
However, QOL is a much broader concept that encompasses both medical and non-medical aspects, including physical func-tioning (e.g., ability to perform daily activities), psychological functioning (e.g., emotional and mental well-being), social func-tioning (e.g., relationships with others and participation in so-cial activities), and perception of health status, pain, and over-all satisfaction with life.5,7,9,10
In summary, the evaluation of QOL puts patients at the cen-ter of inquiry, and gives due weight to their opinions. As pointed out by Orley et al,7 it ‘responds to patients’ concerns not to be treated as cases but as human beings, who have lives with many facets not connected directly to their disease’.
Quality of life: a proposed definition
Research designed to measure QOL suffers from various problems relating to theory and method. Prominent is the pov-erty of its theoretical foundation. Without a comprehensive theory of QOL to guide the design of instruments, it is difficult
to determine what and how to measure.11 Owing to this
situa-tion, in 1991 a panel of researchers of the World Health Orga-nization (WHO) started to develop a unifying and transcultural definition of QOL. They conceived it as ‘the individual’s per-ception of his or her position in life, within the cultural context and value system he or she lives in, and in relation to his or her goals, expectations, parameters and social relations. It is a broad ranging concept affected in a complex way by the person’s physical health, psychological state, level of independence, social relationships and their relationship to salient features of their environment.12
The emphasis within this definition was first, on the subjec-tive nature of QOL (which was conceived as an internal experi-ence influexperi-enced by what is happening ‘out there’, but colored by the subject’s earlier experiences, mental state, personality, and expectations) and, second, on the need to explore all those as-pects of life considered as having a significant impact on QOL. This ‘subjective’ definition, in turn, brought a degree of unity to the evaluation, as if it were purely objective, QOL being com-posed by a whole range of possibly disconnected and uncorrelated items.7,13 In addition, WHO’s definition of QOL may be the first
one that has directly and formally incorporated cultural compo-nents as integrating its theoretical basis rather than acknowledg-ing cultural influence as an extraneous variable.14
Finally, as a very broad range of facets probably influence QOL, it is unlikely to have a marked daily change or to be influenced by a change in one facet unless that in turn affects many other facets. Furthermore, it is unlikely that all illnesses markedly affect QOL in this broad sense, or that all treatments, even if effective in alleviating symptoms, necessarily improve it.13 The consequence is that the ‘sensitivity to change’ - a key
psychometric property used to evaluate clinical response - of QOL instruments (specially of the ‘generic’ ones [see below]) is frequently criticized.
Quality of life: measurement issues
The ongoing discussion on how QOL should be assessed can be summarized in the following dilemmas:
251
Quality of life: a new concept for psychiatry Berlim MT & Fleck MPA Rev Bras Psiquiatr 2003;25(4):249-52
number of studies indicated that the seeking of medical attention is more closely related to how patients feel their condition has impacted on their lives, rather then to the presence of symptoms per se. Furthermore, compliance with any subsequent treatment is dependent on whether or not the patients consider that their condition has improved. Finally, it is now generally accepted that where interventions are designed to make life more comfortable rather than to cure, the only valid source of outcome information is the patient. In sum, it is inappropriate to rely only on the clinician’s perception, particularly when the degree of disagreement between the physician and the patient is taken into consideration, and more emphasis should be placed on the latter’s viewpoint.2,3,9,14 As seen above, WHO’s definition
of QOL emphasizes the subjective nature of the construct (and a conceptual problem of including objective items to evaluate QOL is that by doing this one could be trespassing
the concept’s boundaries). As Orley et al7 pointed out: ‘This is not to say that objective questions are not useful in an assessment of a patient. Any good assessment of a patient requires a combination of instruments, but each needs definition, so that it is clear as to whether it is following an objective or subjective approach, or it is dealing with QOL or with disabilities or with symptoms’.
• Generic scales (developed for comparisons between
different diseases, and applicable to virtually all people)
versus disease-specific scales (developed for those individuals with particular diseases or conditions). The rationale for the latter is that there are particular issues that contribute to a much greater extent to the QOL of subjects with certain diseases. Another point is that a more specific measure will be more sensitive to changes in that condition.3
If, however, an objective is to assess the influence of a disease (or its symptoms) on QOL, including thus items
aAdapted from Rabkin J, Wagner G, Griffin KW. Quality of life measures. In: Rush AJ, Pincus HA, First MB, et al (eds.). Handbook of Psychiatric Measures. Washington, DC: American
Psychiatric Association Press, 2000, pp. 135-150.
bAdapted from Brazier JE, Harper R, Jones NM et al. Validating the SF-36 health survey questionnaire: new outcome measure for primary care. BMJ 1992; 305:160-4. cAdapted from McKenna SP, Doward LC, Kohlmann T et al. International development of the Quality of Life in Depression Scale (QLDS). J Affect Dis 2001; 63:189-99.
dAdapted from The WHOQOL Group. The World Health Organization Quality of Life Assessment (WHOQOL): development and general psychometric properties. Soc Sci Med 1998;
46:1569-1585.
Measure
Quality of Life Interview (QOLI)a
Quality of Life Scale (QLS)a
Wisconsin Quality of Life Index (W-QLI)a
Medical Outcomes Study Short Form – 36 Items (SF-36) b
Quality of Life Enjoyment & Satisfaction Questionnaire (Q-LES-Q)a
Quality of Life Index (QLI)a
Quality of Life Inventory (QOLI)a
Quality of Life In Depression Scale (QLDS)c
Psychosocial Adjustment to Illness Scale, interview version (PAIS), and Self-Report Version (PAIS-SR)a
Spitzer Quality of Life Index (Spitzer QL-Index)a
World Health Organization’s Quality of Life Instrument (WHOQOL)d
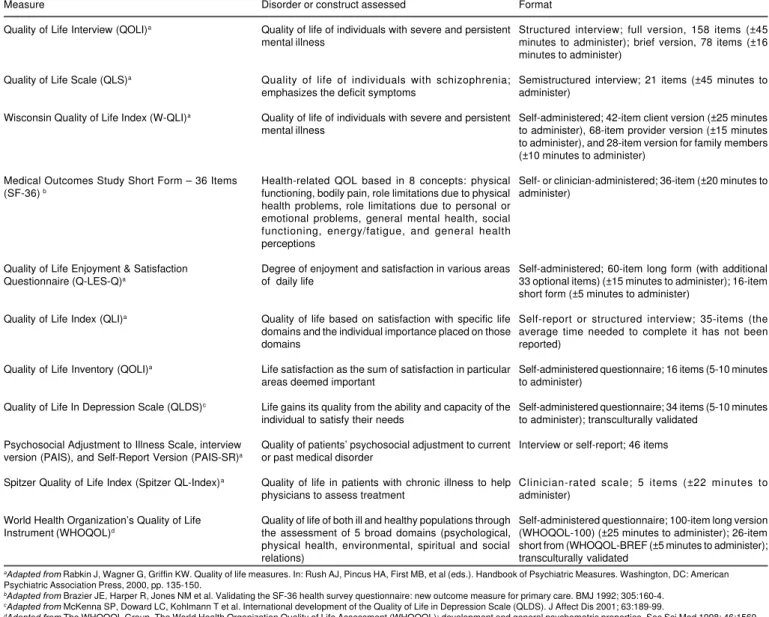
Table - Most commonly used quality of life instruments.
Disorder or construct assessed
Quality of life of individuals with severe and persistent mental illness
Quality of life of individuals with schizophrenia; emphasizes the deficit symptoms
Quality of life of individuals with severe and persistent mental illness
Health-related QOL based in 8 concepts: physical functioning, bodily pain, role limitations due to physical health problems, role limitations due to personal or emotional problems, general mental health, social functioning, energy/fatigue, and general health perceptions
Degree of enjoyment and satisfaction in various areas of daily life
Quality of life based on satisfaction with specific life domains and the individual importance placed on those domains
Life satisfaction as the sum of satisfaction in particular areas deemed important
Life gains its quality from the ability and capacity of the individual to satisfy their needs
Quality of patients’ psychosocial adjustment to current or past medical disorder
Quality of life in patients with chronic illness to help physicians to assess treatment
Quality of life of both ill and healthy populations through the assessment of 5 broad domains (psychological, physical health, environmental, spiritual and social relations)
Format
Structured interview; full version, 158 items (±45 minutes to administer); brief version, 78 items (±16 minutes to administer)
Semistructured interview; 21 items (±45 minutes to administer)
Self-administered; 42-item client version (±25 minutes to administer), 68-item provider version (±15 minutes to administer), and 28-item version for family members (±10 minutes to administer)
Self- or clinician-administered; 36-item (±20 minutes to administer)
Self-administered; 60-item long form (with additional 33 optional items) (±15 minutes to administer); 16-item short form (±5 minutes to administer)
Self-report or structured interview; 35-items (the average time needed to complete it has not been reported)
Self-administered questionnaire; 16 items (5-10 minutes to administer)
Self-administered questionnaire; 34 items (5-10 minutes to administer); transculturally validated
Interview or self-report; 46 items
Clinician-rated scale; 5 items (±22 minutes to administer)
Rev Bras Psiquiatr 2003;25(4):249-52
252
Quality of life: a new concept for psychiatry Berlim MT & Fleck MPA
closely related to, say, symptoms, in the assessment of QOL serves only to confound the dependent with independent variables. For this reason, there are strong arguments for using generic instruments of quality of life as main outcomes, although illness-specific measures may occasionally be used as complementary data.7,14 Another
limitation of specific QOL instruments is that they lack a key feature of the concept: the ability to compare the QOL of different clinical conditions.
• A medical model versus a mediational model. Currently, there is still a common belief that QOL is mainly the product of symptoms and side-effects of medication (medical model). However, there is a growing body of evidence showing that two patients can have different levels of QOL for the same disorder severity and for the same level of treatment side-effects. Patients characteristics can indeed mediate between quality of life and symptoms/side-effects (mediational model).2,13
• Scales reflecting a functionalist approach (i.e., individuals being able to perform roles that are deemed ‘normal’ for people in Western societies [e.g., physical mobility, employment, socialization processes], and deviation from normality resulting in reduced QOL) versus a needs-based approach (i.e., individuals being able to satisfy their physical needs such as shelter, food and security and their psychological needs such as self-respect, autonomy, companionship, and pleasure [that is, physical mobility, employment, and socialization are important only insofar as they provide the means by which these needs can be fulfilled]). Summing up, proponents of the functionalist approach postulate that illness only becomes a problem when it affects role performance, whereas proponents of the needs-based approach postulate that life gains its quality from the ability and capacity of individuals to satisfy their needs.9,13
Quality of life: commonly used instruments
Despite the limitations of virtually all the scales designed to measure QOL, this is a field that needs fewer rather than more assessment candidates.3 Indeed, a recent review of the
litera-ture found that 159 different instruments were used in research, including 136 that were used only in a single study.5
Table presents some of the most commonly used QOL measures.
Quality of life: future perspectives
In Psychiatry, the art and science of QOL assessment consist in capturing a patient’s QOL midway between the two extremes of writing a novel on one hand and summarizing the phenom-enon into a single index on the other.
This type of assessment will be useful for psychiatric re-search and clinical practice only if the conceptual and method-ological requirements described above are taken into consid-eration; only then can the potential ‘breath of fresh air’ which accompanies QOL be used in a profitable way for the whole mental health field. On one hand, QOL is a construct that chal-lenges one of the most difficult aspects of our field: How to measure the subjective domain. On the other hand, it has an intrinsic value since improving patients’ QOL is the intuitive goal of any healthcare intervention and ultimately the ethical justification for the existence of psychiatry (and even of medi-cine). Nevertheless, there are many issues that still need to be solved. Some of them require conceptual clarification, but the majority will only be answered with the accumulation of em-pirical data.
Concluding, the future will show whether QOL research was a fashionable and transient movement at the end of the 20th
century or a serious endeavor with profound implications for the daily practice of psychiatry, including outcome assessment in clinical trials and health services research, population health needs evaluation, and resource allocation.
References
1. Higginson IJ, Carr AJ. Using quality of life measures in the clinical setting. BMJ 2001;322:1297-300.
2. Demyttenaere K, Fruyt JD, Huygens R. Measuring quality of life in depression. Curr Opin Psychiatry 2002;15:89-92.
3. Rabkin J, Wagner G, Griffin KW. Quality of life measures. In: Rush AJ, Pincus HA, First MB, eds. Handbook of Psychiatric Measures. Washing-ton (DC): American Psychiatric Association Press; 2000. p. 135-50. 4. Katschnig H, Freeman H, Sartorius N, eds. Quality of Life in Mental
Disorders. New York: John Wiley & Sons; 1997.
5. Gill TM, Feinstein AR. A critical appraisal of the quality of quality-of-life measurements. JAMA 1994;272:619-26.
6. Bech P. Quality of life measurements in major depression. Eur Psychiatry 1996;11:123-6.
7. Orley J, Saxena S, Herrman H. Quality of life and mental illness: reflections from the perspective of the WHOQOL. Br J Psychiatry 1998;172:291-93. 8. Carr AJ, Higginson IJ. Are quality of life measures patient centred? BMJ
2001;322:1357-60.
9. McKenna SP, Whalley D. Can quality of life scales tell us when patients begin to feel the benefits of antidepressants? Eur Psychiatry 1998;13:146-53.
10. Sanders C, Egger M, Donovan J, Tallon D, Frankel S. Reporting quality of life in randomized controlled trials: bibliographic study. BMJ 1998;317:1191-4.
11. Anonymous. Quality of life [editorial]. Lancet 1991;338:350-1. 12. The WHOQOL Group. The World Health Organization Quality of Life
Assessment (WHOQOL): development and general psychometric properties. Soc Sci Med 1998;46:1569-85.
13. Fleck MPA. Avaliação da qualidade de vida. In: Fráguas R, Figueiró JAB, eds. Depressões em Medicina interna e em outras condições médicas – depressões secundárias. São Paulo: Atheneu; 2001. p. 33-43.
14. Skevington SM. Advancing cross-cultural research on quality of life: observations drawn from the WHOQOL development. Qual Life Res 2002;11:135-44.
Correspondence:
Marcelo T Berlim Rua Santana, 312/201