www.jped.com.br
ORIGINAL
ARTICLE
Cognitive
and
behavioral
heterogeneity
in
genetic
syndromes
夽
Luiz
F.L.
Pegoraro
a,b,∗,
Carlos
E.
Steiner
c,
Eloisa
H.R.V.
Celeri
a,
Claudio
E.M.
Banzato
a,
Paulo
Dalgalarrondo
a,baDepartmentofMedicalPsychologyandPsychiatry,FacultyofMedicalSciences,UniversidadedeCampinas,Campinas,SP,Brazil bPediatricResearchCenter,DepartmentofPediatrics,FacultyofMedicalSciences,UniversidadedeCampinas,Campinas,SP,
Brazil
cDepartmentofMedicalGenetics,FacultyofMedicalSciences,UniversidadedeCampinas,Campinas,SP,Brazil
Received22March2013;accepted19June2013 Availableonline30October2013
KEYWORDS Cognition; Behavior; Williams-Beuren syndrome; Prader-Willi syndrome;
FragileXsyndrome
Abstract
Objective: thisstudyaimedtoinvestigatethecognitiveandbehavioralprofiles,aswellasthe psychiatricsymptomsanddisordersinchildren withthreedifferentgeneticsyndromeswith similarsocioculturalandsocioeconomicbackgrounds.
Methods: thirty-four children aged 6 to 16 years, with Williams-Beuren syndrome (n=10), Prader-Willisyndrome(n=11),andFragileXsyndrome(n=13)fromtheoutpatientclinicsof ChildPsychiatryandMedicalGeneticsDepartmentwerecognitivelyassessedthroughthe Wech-sler Intelligence Scalefor Children (WISC-III). Afterwards,a full-scaleintelligence quotient (IQ),verbalIQ,performanceIQ,standardsubtestscores,aswellasfrequencyofpsychiatric symptomsanddisorderswerecomparedamongthethreesyndromes.
Results: significant differences werefound among thesyndromes concerning verbalIQ and verbalandperformancesubtests.Post-hocanalysisdemonstratedthatvocabularyand compre-hensionsubtestscoresweresignificantlyhigherinWilliams-Beurensyndromeincomparisonwith Prader-WilliandFragileXsyndromes,andblockdesignandobjectassemblyscoreswere signifi-cantlyhigherinPrader-WillisyndromecomparedwithWilliams-BeurenandFragileXsyndromes. Additionally,thereweresignificantdifferencesbetweenthesyndromesconcerningbehavioral featuresandpsychiatricsymptoms.ThePrader-Willisyndromegrouppresentedahigher fre-quency ofhyperphagia andself-injurious behaviors. The Fragile X syndrome group showed a higherfrequency of social interactiondeficits; such differencenearly reachedstatistical significance.
Conclusion: thethreegeneticsyndromesexhibiteddistinctivecognitive,behavioral,and psy-chiatricpatterns.
©2013SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:PegoraroLF,SteinerCE,CeleriEH,BanzatoCE,DalgalarrondoP.Cognitiveandbehavioralheterogeneityin
geneticsyndromes.JPediatr(RioJ).2014;90:155---60.
∗Correspondingauthor.
E-mail:[email protected](L.F.L.Pegoraro).
PALAVRAS-CHAVE Cognic¸ão;
Comportamento; Síndromede Williams-Beuren; Síndromede Prader-Willi; SíndromedoX-Frágil
Heterogeneidadecognitivaecomportamentalemsíndromesgenéticas
Resumo
Objetivo: investigar operfil cognitivoecomportamental,sintomase transtornos psiquiátri-cosemcrianc¸ascomtrêsdiferentessíndromesgenéticas,comantecedentessocioculturaise socioeconômicossemelhantes.
Métodos: trinta equatro crianc¸as,entre6e16anos,comassíndromesdeWilliams-Beuren (n=10),dePrader-Willi(n=11)edoX-Frágil(n=13),dosambulatóriosdePsiquiatriaInfantil eGenéticaMédica,foramavaliadascognitivamentepelaEscalaWechslerdeInteligênciapara Crianc¸as(WISC-III).Posteriormente,oQItotal,oQIVerbal,oQIdeExecuc¸ão,osescores pon-deradosdossubtesteseafrequênciadesintomasetranstornospsiquiátricosforamcomparados entreassíndromes.
Resultados: diferenc¸assignificativasforamencontradasentreassíndromesquantoaoQI Ver-bal e os subtestes verbais e de execuc¸ão. A análise Post-hoc demonstrou que os escores dossubtestesvocabulárioecompreensãoforamsignificativamentesuperioresnasíndromede Williams-Beurenemrelac¸ãoàssíndromesdePrader-WilliedoX-Frágil,eosescoresdos sub-testescubosearmarobjetosforamsignificativamentesuperioresnasíndromedePrader-Willi emrelac¸ãoàssíndromesdeWilliams-BeurenedoX-Frágil.Alémdisso,houvediferenc¸a significa-tivaentreassíndromesquantoàscaracterísticascomportamentaiseossintomaspsiquiátricos. OgrupocomsíndromedePrader-Williapresentou maiorfrequênciadehiperfagiae compor-tamentosautolesivos.JáogrupocomsíndromedoX-Frágilapresentoumaiorfrequênciado déficitdainterac¸ãosocial.Estadiferenc¸aquasealcanc¸ouasignificânciaestatística.
Conclusão: astrêssíndromesgenéticasapresentaramumpadrãocognitivo,comportamentale psiquiátricodiferenciadoquandoforamcomparadasentresi.
©2013SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Intellectual disability (ID), the current term for mental retardation, is one of the most commonly observed neu-ropsychiatricdisordersthat impairssocial functioningand adaptivebehaviorofchildrenandadolescents.1In
underde-velopedcountries,theprevalenceofIDisalmosttwotimes higherthanindevelopedcountries.2
Common causes of ID are genetic diseases, problems during pregnancy or birth, birth defects that affect the brain,andproblemsduringinfancy,childhood,and adoles-cence,such asinjuries,diseases, or brain abnormalities.3
Inunderdevelopedanddevelopingcountries,malnutrition, socio-culturaldeprivation,andpoorhealthcarearealso fac-torsfrequentlyassociatedwithID.4
PatientswithIDpresent higher risk for psychiatric dis-ordersthanthegeneralpopulation.Therateofpsychiatric disordersinthispopulationrangesfrom30%to50%.4
Despite the high prevalence of ID and strong associa-tionwithpsychiatricdisorders,mentalhealthprofessionals often fail to give proper attention to ID.5,6 When caring
for less prevalent conditions in mental healthcare, such asgeneticsyndromeswithID,7cliniciansfrequentlyignore
theirspecificcognitive,behavioral,andpsychopathological characteristics.
ThreegeneticsyndromesfeaturingIDhavebeen receiv-ingincreasingattentionbyspecialistsinthecareofchildren withgeneticsyndromes duetotheirdiverseexpression of cognitiveandbehaviorcharacteristics:Williams-Beuren syn-drome (WBS), Prader-Willi syndrome(PWS), and Fragile X syndrome(FXS).8---10
WBS, a rare neurodevelopmental disorder caused by a submicroscopicdeletiononchromosome7q11.23,is charac-terizedbydysmorphicfacialfeatures,elastinarteriopathy, short stature, connective tissue abnormalities, infantile hypercalcemia,andID.11 ChildrenwithWBSusuallydisplay
high sociability, excessive empathy (which may be inap-propriate), anxiety,preoccupationsand fears,impulsivity, inattention, sadness and depression, generalized anxi-ety disorder, phobias, and attention deficit hyperactivity disorder.7,12Relativelygoodlanguageskillsandverbal
short-termmemory,andamarkeddeficitinvisuospatialskillshave beendescribedinWBS.8,13
PWS, a genetic disorder that results from abnormal-ity or loss of a critical region of chromosome 15q11---13, is characterized by neonatal hypotonia, hyperphagiawith eventual obesity,andID.7 ChildrenwithPWSusuallyhave
goodperformanceinvisuospatialconstructiontasks,5,9but
presentimportantdeficitsinmathematics14 andexpressive
language.15
Individuals with PWS exhibit a distinctive behavioral phenotype, with temper tantrums, stubbornness, and excessive interest in food; as well asobsessive, compul-sive, manipulative, oppositional, and defiant behaviors.16
The psychiatric features commonly reported in PWS are obsessive-compulsive disorder, depression/mood disorder, psychosis,andself-injuriousbehaviors(skinpicking).7
FXS, a disorder caused by an unusually large tri-nucleotide repeat (CGG) expansion in the long arm of the X chromosome, is the most common cause of inher-ited ID.10 The cognitive profile in FXS includes deficits in
as in pragmatic language and morphosyntax, but not in vocabulary.18
Males with FXS present more severe cognitive
impair-ments when compared to females with the same
syndrome,19 and frequently manifest behaviors from the
autisticspectrum,suchasgazeaversion,socialavoidance, andstereotypicalandrepetitivebehavior.20
Individuals with FXS often meet criteria for attention deficit hyperactivity disorder, oppositional defiant disor-der, enuresis, encopresis, and exhibit isolated symptoms and behaviors that do not always fit into the diag-nostic categories employed by Diagnostic and Statistical Manual of Mental Disorders (DSM), such as anxiety and compulsive symptoms,labile mood,irritability, aggressive outbursts,self-injurious behavior,impaired attention, and hyperactivity.21
Although each of these individual genetic syndromes associatedwithIDhavebeen individuallyinvestigateddue totheirdiverseexpressionofcognitiveandbehavior charac-teristics,studiesthatcomparethem,enrollingparticipants fromsimilarsocial andcultural background andusing the same methodology for cognitive and behavior/psychiatric assessmentsarestillscarce.
Thus,thepresentstudyaimedtoinvestigatethe cogni-tiveprofilesandbehavioralfeatures,aswellaspsychiatric symptoms and disorders in children and adolescents with WBS,PWS,andFXS.
Methods
Thiswasananalyticalcross-sectionalstudythatuseda con-venience sample. All children and adolescentswith WBS, PWS, or FXS fromthe outpatient clinics of the Child and AdolescentPsychiatryandMedicalGeneticsDepartmentof theUniversityHospitaloftheUniversityofCampinas (Uni-camp -Campinas, Brazil)wereenrolled inthis study.Two participantswithWBScamefromaninstitutionspecialized inthecare ofchildrenwithID(Campinas,Brazil). Consid-eringthat WBSisa relativelyraresyndrome,thisstrategy wasadoptedinordertomakethesamplesizeofthethree groupscomparable.
This study was approved by the Institutional Review Board of the Faculty of Medical Sciences, Unicamp. The sample obtained consistedof 34 children andadolescents aged6to16years;tenparticipantshadWBS(sevenmales and three females); 11 participants had PWS (five males and six females); and 13 participants had FXS (12 males andonefemale).Theparticipantshadsimilarsociocultural and socioeconomic backgrounds (Table 1). Consent forms approvedbytheInstitutionalReviewBoardofUnicampwere signedbytheparents.
ChildrenandadolescentswithclinicaldiagnosisofWBS, PWS, or FXS confirmed by cytogenetic exams that were assessedbyaclinicalpsychiatristfromtheoutpatient clin-icsoftheChildandAdolescentPsychiatryDepartmentwere included in the study. Patients who did not develop lan-guage,whichwouldpreventthepsychologicalassessment, wereexcluded.
WBS diagnosis wasconfirmed through the fluorescence in-situ hybridization technique. All participants withPWS had their diagnosis confirmed by fluorescence in-situ
hybridizationtechniqueand/or by methylationanalysisof theSNRPNgene. Allparticipants withFXShad their diag-nosisconfirmedbymolecularstudyoftheFRAXAmutation, usingtheSouthernblottingtechnique.
Clinical psychiatrists (EHRV and PD) diagnosed the participants using the fourth edition of the DSM, Text Revision.22 Psychiatricsymptomsanddiagnoses,behavioral
characteristics (e.g., explosiveness, oppositional behav-ior, hyperphagia), and sociocultural and socioeconomic features (i.e., family income, per capita income, and educational level of the participants and their parents) wereobtainedbymedicalchartreviewbeforethecognitive evaluation of each participant. These data were previ-ously acquired during psychiatric assessment/anamnesis with participants’ caregivers, through a structured protocol.
The Brazilianversionof WechslerIntelligenceScale for Children(WISC-III), third edition,23 was applied by a
psy-chologist(LFLP) after the psychiatric assessment of each children and adolescent. The WISC-III is an individually administered measure of intelligence intended for chil-dren aged 6 to 16 years and 11 months. The WISC-III is dividedinto tensubtests (see Appendix),which are orga-nizedintoverbalandperformancescales.Thesubtestsyield threecompositescores:verbalIQ,performanceIQ,and full-scaleIQ-whichestimatetheindividual’sverballanguage, nonverbal/visual-spatial/visual-motor,andgeneral intellec-tualabilities,respectively.
Comparison of age, compositeIQ scores, and standard subtestsscoreswereperformedbyusingtheKruskal-Wallis test,followedbytheDunntestforpost-hocanalysis. Gen-eralized Fisher’s exact test was used for comparison of gender,andpsychiatricsymptomsanddisordersamongthe syndromes. All analyses were performed using SAS soft-wareversion 9.1.3 for Windows, witha significance level of5%.
Results
Thesample’ssociodemographiccharacteristicsaredetailed inTable1.Amongthefewparticipants whoattended reg-ular school (17%), only two (33%) completed elementary school.Table 2presents thecomparison amongthe three syndromesregardingage,compositeIQ,andsubtestscores. Frequenciesofspecificbehaviorsandpsychiatricsymptoms anddisordersaredisplayedinTable3.
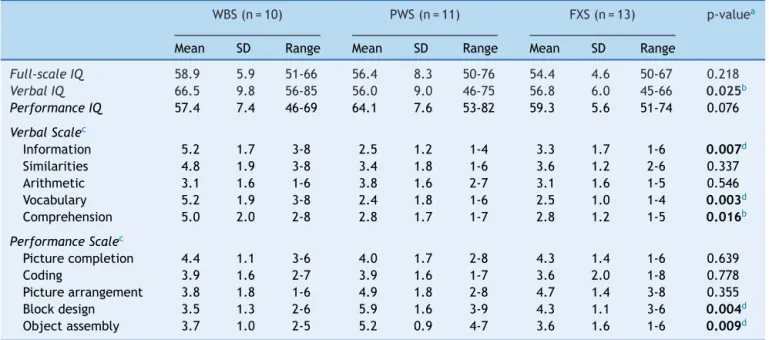
Significantdifferenceswerefoundamongthethree syn-dromes regarding verbal IQ and verbal and performance subtests(Table2).Post-hocanalysisrevealedthattheWBS grouppresentedsignificantlyhigherscoresinrelationtothe PWSgroup concerningverbalIQ andinformation, vocabu-lary,andcomprehensionsubtests(p<0.05),andsignificantly higherscoresinrelationtotheFXSgroupregarding vocabu-laryandcomprehensionsubtests(p<0.05).Additionally,the PWSgrouppresented significantlyhigherscoresinrelation totheWBSandFXSgroupsconcerningtheblockdesignand objectassemblysubtests(p<0.05).
Table1 Sociodemographiccharacteristics.
WBS(n=10) PWS(n=11) FXS(n=13) p-value
Age---Mean(SD) 11.7(3.6) 11.1(2.7) 12.0(3.0) 0.70a
Gender 0.04b
Male 7(70%) 5(46%) 12(92%)
Female 3(30%) 6(54%) 1(8%)
Typeofeducation 0.99b
Specialschool 8(80%) 9(82%) 11(84%)
Regularschool 2(20%) 2(18%) 2(16%)
FamilyIncomec 0.98b
≤2.0 4(40%) 6(55%) 6(46%)
2.1-3.0 3(30%) 3(27%) 4(31%)
>3.0 3(30%) 2(18%) 3(23%)
Percapitaincomec 0.74b
≤1.0 8(80%) 10(91%) 10(77%)
>1.0 2(20%) 1(9%) 3(23%)
FXS,FragileXsyndrome;PWS,Prader-Willisyndrome;WBS,Williams-Beurensyndrome. Significantvaluesinbold.
ap-valuesfromtheKruskal-Wallistest(␣=0.05).
b p-valuesfromthegeneralizedFisher’sexacttest(␣=0,05).
c Monthlyfamilyincomeandpercapitaincomeinminimumwages(R$678.00orapproximatelyUS$340.00).
Discussion
Although the present sample was relatively small, tothe authors’ knowledge, this is the first study to specifically compare these three genetic syndromes using the same
methodologyof cognitiveandbehavior/psychiatric assess-mentinthedevelopingworld.
Inthisstudy,itwasobserved thatchildrenand adoles-centswithgeneticsyndromesandID,whoshareequivalent degreesof intellectual impairmentandcomefromsimilar
Table2 Means,standarddeviations,ageranges,andWISC-IIIsubtestsinWBS,PWS,andFXS.
WBS(n=10) PWS(n=11) FXS(n=13) p-valuea
Mean SD Range Mean SD Range Mean SD Range
Full-scaleIQ 58.9 5.9 51-66 56.4 8.3 50-76 54.4 4.6 50-67 0.218
VerbalIQ 66.5 9.8 56-85 56.0 9.0 46-75 56.8 6.0 45-66 0.025b
PerformanceIQ 57.4 7.4 46-69 64.1 7.6 53-82 59.3 5.6 51-74 0.076
VerbalScalec
Information 5.2 1.7 3-8 2.5 1.2 1-4 3.3 1.7 1-6 0.007d
Similarities 4.8 1.9 3-8 3.4 1.8 1-6 3.6 1.2 2-6 0.337
Arithmetic 3.1 1.6 1-6 3.8 1.6 2-7 3.1 1.6 1-5 0.546
Vocabulary 5.2 1.9 3-8 2.4 1.8 1-6 2.5 1.0 1-4 0.003d
Comprehension 5.0 2.0 2-8 2.8 1.7 1-7 2.8 1.2 1-5 0.016b
PerformanceScalec
Picturecompletion 4.4 1.1 3-6 4.0 1.7 2-8 4.3 1.4 1-6 0.639
Coding 3.9 1.6 2-7 3.9 1.6 1-7 3.6 2.0 1-8 0.778
Picturearrangement 3.8 1.8 1-6 4.9 1.8 2-8 4.7 1.4 3-8 0.355
Blockdesign 3.5 1.3 2-6 5.9 1.6 3-9 4.3 1.1 3-6 0.004d
Objectassembly 3.7 1.0 2-5 5.2 0.9 4-7 3.6 1.6 1-6 0.009d
FXS,FragileXsyndrome;PWS,Prader-Willisyndrome;WBS,Williams-Beurensyndrome;WISC-III,WechslerIntelligenceScaleforChildren, thirdedition.
Significantvaluesinbold.
ap-valuesfromtheKruskal-Wallistest(␣=0.05).
b p<0.05.
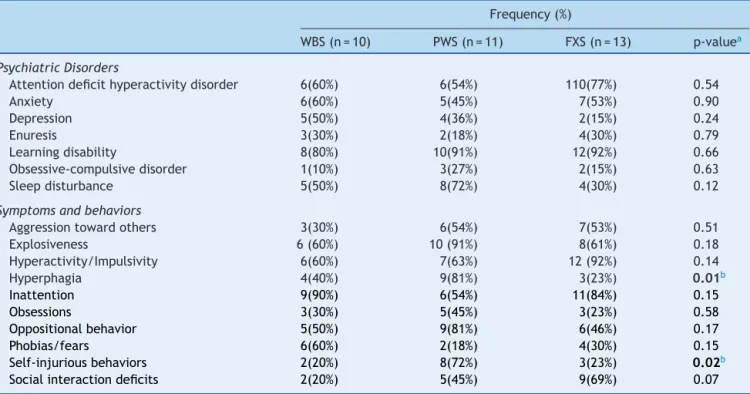
Table3 Frequenciesofpsychiatricdisorders/symptomsandbehavioralfeaturesinWBS,PWS,andFXS.
Frequency(%)
WBS(n=10) PWS(n=11) FXS(n=13) p-valuea
PsychiatricDisorders
Attentiondeficithyperactivitydisorder 6(60%) 6(54%) 110(77%) 0.54
Anxiety 6(60%) 5(45%) 7(53%) 0.90
Depression 5(50%) 4(36%) 2(15%) 0.24
Enuresis 3(30%) 2(18%) 4(30%) 0.79
Learningdisability 8(80%) 10(91%) 12(92%) 0.66
Obsessive-compulsivedisorder 1(10%) 3(27%) 2(15%) 0.63
Sleepdisturbance 5(50%) 8(72%) 4(30%) 0.12
Symptomsandbehaviors
Aggressiontowardothers 3(30%) 6(54%) 7(53%) 0.51
Explosiveness 6(60%) 10(91%) 8(61%) 0.18
Hyperactivity/Impulsivity 6(60%) 7(63%) 12(92%) 0.14
Hyperphagia 4(40%) 9(81%) 3(23%) 0.01b
Inattention 9(90%) 6(54%) 11(84%) 0.15
Obsessions 3(30%) 5(45%) 3(23%) 0.58
Oppositionalbehavior 5(50%) 9(81%) 6(46%) 0.17
Phobias/fears 6(60%) 2(18%) 4(30%) 0.15
Self-injuriousbehaviors 2(20%) 8(72%) 3(23%) 0.02b
Socialinteractiondeficits 2(20%) 5(45%) 9(69%) 0.07
FXS,FragileXsyndrome;PWS,Prader-Willisyndrome;WBS,Williams-Beurensyndrome. Significantvaluesinbold.
a p-valuesfromthegeneralizedFisher’sexacttest(˛=0.05). b p<0.05.
social and economic contexts, exhibited a heterogeneous cognitive,behavioral,andpsychopathologicalprofile.
Predominanceoflanguageskillsovervisuospatialskillsin childrenandadolescentswithWBSwashighlightedinsome studies;8,13howeveritwasnotidentifiedinothers.24,25Inthe
presentstudy,goodperformanceinverballanguage activi-ties(i.e.,theabilitytounderstandothersandcommunicate appropriately)ofchildrenandadolescentswithWBSbecame evenmoreapparentwhenthissyndromewascomparedwith FXSandPWS.
Another relevant result of this study was a signifi-cantly higher score obtained by children with PWS in visuospatial construction abilities (e.g., jigsaw puzzles, buildingmodelswithbricksandpieces),whichcorroborates results from some previous studies5,9,26 and differs from
others.27,28
These findings may help to raise the awareness of pediatriciansandotherhealthcareprofessionalsabout the peculiarneuropsychomotordevelopmentandcognitiveskills of individuals with these geneticsyndromes, which could possiblyleadtobetterinformedrehabilitationefforts pro-motedbyhealthcareprofessionals.
Regarding the distinctive behavior profile among the three syndromes, Sarimski29 found a higher association
betweeninsatiableappetiteandchildrenwithPWS;higher frequencyofself-injuriousbehaviors,hyperactivity, aggres-sion, and oppositional behavior in children with FXS; and higher prevalence of sleepdisturbances and bettersocial interaction in children with WBS. Di Nuovo and Buono30
reportedlowercommunication skills inchildren withWBS comparedtochildrenwithFXS.
Inthepresentstudy,thecomparisonamongchildrenwith WBS,PWS,andFXSregardingbehaviorfeaturesand psychi-atricssymptoms/disordersrevealedthatthefrequenciesof hyperphagiaandself-injuriousbehaviorsweresignificantly higherinthePWSgroupthanintheWBSandFSXgroups.
Phobiasandfears,inattention,anddepressionweremore prevalentinWBSgroup.ChildrenwithPWSexhibitedmore oppositional behavior, explosiveness, sleep disturbance, obsessions,andobsessive-compulsivedisorder. Hyperactiv-ityandimpulsivity,socialinteractiondeficits,andattention deficithyperactivitydisorderweremorefrequentintheFXS group.
The differences in prevalence of psychiatric symp-toms/disorders and specific behaviors between the syn-dromes justify a targeted care for these individuals. Pediatriciansandother healthcareprofessionalsshouldbe familiarwiththebehavioralphenotypeofdifferentgenetic syndromeswithID,tailoringpharmacologicaltreatmentand rehabilitationforeachcondition.
The study sample wasrelativelysmall, itwasselected byconvenience,and sample sizecalculation wasnot per-formed.Thus,theresultsachievedinthisstudy shouldbe regarded with caution regarding to their generalizability. Nevertheless,thedatapresented inthisexploratorystudy aresufficientlyrobusttosupporttheclaimthatthesethree syndromeshaveadistinctivecognitiveandbehavioral pro-file.
According to Salvador-Carulla and Bertelli,6 caring for
genetic syndromes with relative low prevalence, such as WBS,PWS,andFXS,theknowledgegaponthepartof health-careprofessionalsisevengreater.
For the pediatricians and other health professionals, betterunderstandingofthecognitive,behavioral,and psy-chopathological profiles of children and adolescents with geneticsyndromesandwithdistinctformsofIDcaninform thechoiceof thestrategies for careandrehabilitation of theseindividuals.Asaresearchtopic,itmayilluminatethe complexrelationship between genes, brain development, and expression of specific cognitive, behavioral and psy-chopathologicalfeatures.
Conflicts
of
interest
Theauthorsdeclarenoconflitsofinterest.
Acknowledgements
Theauthorswouldliketothankthepatientsandtheir fam-iliesfortheirparticipation.
References
1.Vasconcelos MM. Retardo mental. J Pediatr (Rio J). 2004;80:S71---82.
2.Maulik PK, Mascarenhas MN, Mathers CD, Duad T, Saxena S. Prevalence of intellectual disability: a meta-analysis of population-basedstudies.ResDevDisabil.2011;32:419---36. 3.PrattHD,GreydanusDE.Intellectualdisability(mental
retarda-tion)inchildrenandadolescents.PrimCareClinOfficePract. 2007;34:375---86.
4.Einfeld SL, Ellis LA, Emerson E. Comorbidity of intellectual disabilityandmentaldisorderinchildrenandadolescents:A systematicreview.JIntellectDevDisabil.2011;36:137---43. 5.Ly TM, Hodapp RM. Children with Prader-Willi syndrome vs
Williamssyndrome:Indirecteffectsonparentsduringajigsaw puzzletask.JIntellectlDisabilRes.2005;49:929---39.
6.Salvador-CarullaL,BertelliM.‘Mentalretardation’or ‘intellec-tualdisability’:timeforaconceptualchange.Psychopathology. 2008;41:10---6.
7.Siegel MS, Smith WE. Psychiatric features in children with geneticsyndromes:towardfunctionalphenotypes.Child Ado-lescPsychiatricClinNAm.2010;19:229---61.
8.Bellugi U, Bihrle A, Jernigan T, Trauner D, Doherty S. Neu-ropsychological,neurological,and neuroanatomicalprofileof Williamssyndrome.AmJMedGenet.1990;6:115---25. 9.Dykens E. Are jigsaw puzzle skills ‘spared’ in persons
with Prader-Willi syndrome? J Child Psychol Psychiatry. 2002;43:343---52.
10.Fisch GS. Psychology genetics. Am J Med Genet. 2000;97:109---11.
11.MorrisCA.Introduction:Williamssyndrome.AmJMedGenetC SeminMedGenet.2010;154C:203---8.
12.Pérez-García D, Granero R, Gallastegui F, Pérez-Jurado LA, Brun-Gasca C. Behavioral features of Williams-Beuren syn-drome compared to Fragile X syndrome and subjects with
intellectualdisabilitywithoutdefinedetiology.ResDevDisabil. 2011;32:643---52.
13.Karmiloff-SmithA,TylerLK,VoiceK,SimsK,UdwinO,HowlinP, etal.LinguisticdissociationsinWilliamssyndrome:Evaluating receptivesyntaxinon-lineandoff-linetasks.Neuropsychologia. 1998;36:343---51.
14.BertellaL,GirelliL,GrugniG,MarchiS,MolinariE,SemenzaC. MathematicalskillsinPrader---WilliSyndrome.JIntellectDisabil Res.2005;49:159---69.
15.VanBorselJ,DefloorT,CurfsLM.Expressivelanguageinpersons withPrader-Willisyndrome.GenetCouns.2007;18:17---28. 16.CassidySB,SchwartzS,MillerJL,DriscollDJ.Prader-Willi
syn-drome.GenetMed.2012;14:10---26.
17.CornishKM,LiL, KoganCS, JacquemontS,TurkJ,DaltonA, etal.Age-dependentcognitivechangesincarriersofthefragile Xsyndrome.Cortex.2008;44:628---36.
18.Abbeduto L, Brady N, Kover ST. Language development and fragileXsyndrome:Profiles,syndrome-specificity,and within-syndrome differences. Ment Retard Dev Disabil Res Rev. 2007;13:36---46.
19.FischGS, CarpenterN,Holden JJ,Howard-PeeblesPN, Mad-dalenaA,BorghgraefM,etal.Longitudinalchangesincognitive andadaptivebehaviorinfragileXfemales:Aprospective mul-ticenteranalysis.AmJMedGenet.1999;83:308---12.
20.VanLieshoutCF,DeMeyerRE,CurfsLM,FrynsJP.Family con-texts,parentalbehaviour,andpersonalityprofilesofchildren andadolescentswithPrader-Willi,fragile-X,orWilliams syn-drome.JChildPsycholPsychiatry.1998;39:699---710.
21.TranfagliaMR,FragileX.syndrome:apsychiatricperspective. ResultsProblCellDiffer.2012;54:281---95.
22.Associac¸ãoAmericanadePsiquiatria.DSM-IV-TR:manual diag-nósticoeestatísticodetranstornosmentais.4aed.rev.Porto
Alegre:Artmed;2002.
23.WechslerD.ManualfortheWechslerintelligencescalefor chil-dren.3rded.SanAntonio:ThePsychologicalCorporation;1991. 24.GreerMK,BrownFR,PaiGS,ChoudrySH,KleinAJ.Cognitive, adaptive,andbehavioralcharacteristicsofWilliamsSyndrome. AmJMedGenet.1997;74:521---5.
25.SampaioA,FérnandezM,HenriquesM,CarracedoA,SousaN, Gonc¸alvesOF.Cognitive functioning inWilliamssyndrome: A studyinPortugueseandSpanishpatients.EurJPaediatrNeurol. 2009;13:337---42.
26.WoodcockKA,OliverC,HumphreysGW.Task-switchingdeficits and repetitive behaviour in genetic neurodevelopmental disorders:DatafromchildrenwithPrader-Willisyndrome chro-mosome15q11-q13deletionandboyswithFragileXsyndrome. CognNeuropsychol.2009;26:172---94.
27.FotiF,MenghiniD,PetrosiniL, etal.Spatialcompetences in Prader-Willisyndrome:aradialarmmazestudy.BehavGenet. 2011;41:445---56.
28.Fisch GS, CarpenterN, Howard-Peebles PN, Holden JJ, Tar-letonJ,SimensenR,etal.Studiesofage-correlatedfeatures ofcognitive-behavioral developmentin children and adoles-centswithgeneticdisorders.AmJMedGenet A.2007;143A: 2478---89.
29.SarimskiK.Behaviouralphenotypesandfamilystressinthree mentalretardation syndromes.EurChild Adolesc Psychiatry. 1997;6:26---31.