REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
The
association
between
thenar
eminence
and
I-gel
TM
dimensions
in
paediatric
patients
夽
Ozgun
Cuvas
Apan
∗,
Alparslan
Apan
GiresunUniversityMedicalFaculty,DepartmentofAnaesthesiologyandIntensiveCareMedicine,Giresun,Turkey
Received4May2014;accepted7August2014 Availableonline27November2014
KEYWORDS
Thenareminence; I-gelTMairwaydevice;
Paediatric
Abstract
Objectives: Apracticalanatomiclandmarkmaybehelpfultoperformtheappropriatesizeof theairwaydeviceseasilyinpaediatricpatients.Theaimofthisstudywastoinvestigatethe associationbetweenthenareminenceandI-geldimensionsinchildren.
Methods:AfterInstitutionalEthicsCommitteeapproval,twohundredandseventyASAClass I---IIpatientsbetween0and12yearsold,whowerescheduledfor electiveproceduresunder generalanaesthesianotrequiring trachealintubation,wererecruitedtothestudy.The size oftheI-gelselectedwasbasedonthepatient’sbodyweightaccordingtothemanufacturer’s recommendation. After successful insertionofthe I-gel, thenar eminence dimensionswere determined.Long-axis(Th-l)wasmeasuredfromjunctionpointofthethumbtowristcurland short-axis (Th-w)constitutesthelargestportionofthethenar eminencefromlateralendof thethumbtothefirsthandline.Themanufacturer’sdimensionsoftheI-gelwhichwasinserted intothepatientswerecomparedwiththemeasurementsobtainedfromthenareminence.
Results:Themean(SD)valuesfor(Ig-w)and(Ig-l)were2.98cm(0.53)and4.54cm(0.82),and themean(SD)valuesfor(Th-w)and(Th-l)were2.99cm(0.60)and3.88cm(0.93),respectively. TherewasastatisticallysignificantcorrelationbetweenTh-wandIg-w(r=0.794,p<0.001), andbetweenTh-landIg-l(r=0.820,p<0.001).
Conclusion: Thedimensionsofthenareminencewerefittedtothatoftheweightbasedsizeof I-gelandthisanatomiclandmarkmaybeapracticaltooltoassessappropriatesizeforpaediatric patients.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
夽 ThestudywasapprovedbytheEthicsCommitteeofKirikkaleUniversity,Kirikkale,TurkeyandcarriedoutattheKirikkaleandGiresun
Universities.
∗Correspondingauthor.
E-mail:[email protected](O.CuvasApan).
http://dx.doi.org/10.1016/j.bjane.2014.08.003
I-gelfoibaseadanopesocorporaldopaciente,deacordocomarecomendac¸ãodofabricante. Apósainserc¸ãobem-sucedidadoI-gel,adimensãodaeminência tênareradeterminada.O eixolongo(Th-l)foimedidodopontodejunc¸ãodopolegaraovincodopulsoeoeixocurto (Th-w)constituiamaiorpartedaeminênciatênardaextremidadelateraldopolegaràprimeira linhadamão.AsdimensõesdefábricadoI-gelinseridonopacienteforamcomparadascomas dimensõesobtidasapartirdaeminênciatênar.
Resultados: Asmédias(DP)dosvalorespara(Ig-w)e(Ig-l)foram2,98cm(0,53)e4,54cm(0,82) easmédias(DP)dosvalorespara(Th-w)e(THl)foram2,99cm(0,60)e3,88cm(0,93), respec-tivamente.Houveumacorrelac¸ãoestatisticamentesignificativaentreTh-weIg-w(r=0,794, p<0,001)eentreTh-leIg-l(r=0,820,p<0,001).
Conclusão:Asdimensões da eminência tênar foram ajustadasàquelas do tamanhodo I-gel baseadonopesoeessareferênciaanatômicapodeserumaferramentapráticaparaavaliaro tamanhoapropriadoempacientespediátricos.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
TheI-gelTM(Intersurgical,Wokingham,UK)isasupraglottic
airwaymanagementdevice,madeofamedicalgrade ther-moplasticelastomer,whichissoft,gel-likeandtransparent. ItwasreportedthattheI-gelseemstobeasafeand effi-cientairwaydeviceforpaediatricpatients.1PaediatricI-gel isavailableinfoursizes(1,1.5,2,2.5)onthebasisofbody weight.Inaninterestingstudy,itwasstatedthatthesizeof theexternalearcouldbeusedasaproxyfortheappropriate sizeoflaryngealmaskairway(LMA)inchildren.2According totheshapeof the I-gel’scuff we decidedtoinvestigate anotheranatomicallandmark whichmay have an associa-tionwiththesizeoftheI-gel.Thereisawidespreadattitude amonganaesthesiologistsaboutthesizeofthelittlefingerof achild.Thismeasurementprovidesaroughestimationofthe sizeofthetuberequired.3Wemeasuredanother anatomi-calregioninthehand.Thethenareminencereferstothe group of muscles on the palm of the human hand at the baseofthethumb.Theaimofthisstudywastoinvestigate the association between thenar eminence and the I-gel’s cuff dimensions regarding width and length in paediatric patients.
Methods
ThestudywasapprovedbytheInstitutionalEthics Commit-teeandwritteninformedconsentwasobtainedfromallthe parents.TwohundredandseventyASAClassIorIIpatients between0and12yearsold,whowerescheduledforelective surgery or magnetic resonance imaging of <1h estimated
duration undergeneralanaesthesianot requiring tracheal intubation, were recruited to this prospective, descrip-tive study during May toSeptember 2013. The study was conducted inaccordance withthe lastversion ofHelsinki Declaration. Childrenwithrisk factors for difficult airway orregurgitationandsyndromeordisordersinfluencingbone or soft tissue growth were excluded. Operation was can-celledinsevenpatientsonthescheduleddayduetoactive respiratoryillness(cough,fever,rhinorrhea).
Oral midazolam 0.3mgkg−1 was given 30min before
inductioninpatientsoveroneage.Patientsinthe operat-ingroomweremonitoredforstandardelectrocardiography (ECG),bloodpressurenon-invasivelyandperipheraloxygen saturation(SpO2).Afterpreoxygenation,anaesthesia
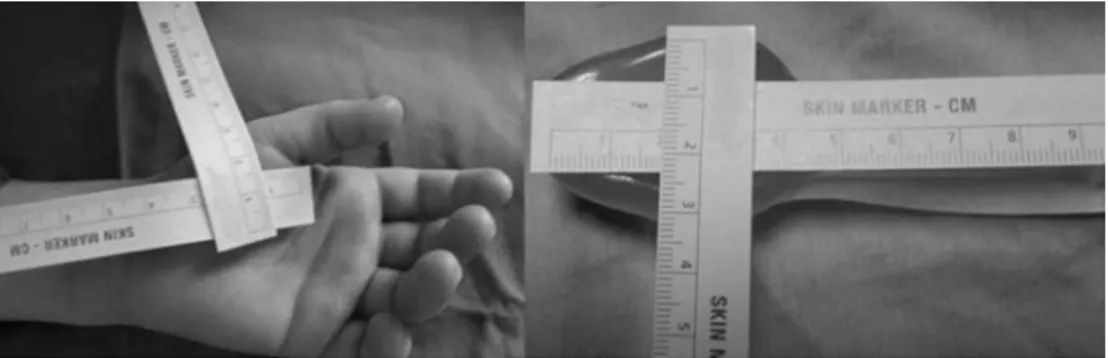
Figure1 Measuringthe vertical andhorizontaldimensionsofthethenar eminenceandthe I-gelTM airwaydevicewhich was
insertedintothepatient.
wasperformedinallpatientsexceptinthosesize1I-gelwas placed.Thenumberofinsertionattemptswasnoted,andit wasconsideredafailureiftheinsertionwasnotsuccessful inthreeattempts. Inthiscase,the patientwasintubated andexcludedfromthestudy.
After insertion of the I-gel, thenar eminence dimen-sions were determined with a ruler from left hand while fingers were placed in neutral position. Long axis (Th-l) was measured from junction point of the thumb to wrist curl and short axis (Th-w) constitutes the largest portion of the thenar eminence from lateral end of the thumb to the first hand line. Width (Ig-w) and length (Ig-l) of the I-gel’s soft non-inflatable cuff wasmeasured (Fig.1).The manufacturer’sdimensions oftheI-gelwhich was inserted into the patients were compared with the measurements obtained from thenar eminence. Patients wereventilatedwithpressure-controlledventilation(Drager Primus, Lubeck, Germany). The respiratory rate was set to maintain an end-tidal CO2 between 35 and 40mmHg.
Patients received 2%---3% sevoflurane in 50% oxygen with nitrous oxide.After completionof the surgery, inhalation anaesthesia wasdiscontinued. If adequate spontan venti-lation (more than 6mLkg−1) was achieved, the I-gel was
removed. Complicationsafter removalof the device such ascoughing,laryngospasm,hipoxia(SpO2<90%)andblood
stainingonthedevicewerenoted.
Theprimaryoutcomeofthisstudywastodeterminethe associationbetweenthenareminenceandI-gel’scuff mea-surements regardingfor widthand length. The secondary outcomewasthenumberofthepatientsinwhomtheI-gel wasplacedsuccessfullyatthefirstattempt.
Statistical
analysis
Atotalsamplesize of258wasrequiredtodetectatleast 0.20correlationsbetweenthenareminenceandI-gel’scuff measurementswithapower of90% at the5% significance level.The0.20degreeofassociationwastakenfrompilot study.SamplesizeestimationwasperformedbyusingNCSS and PASS 2000 (Hintze J. 2001. NCSS and PASS. Number Cruncher Statistical Systems. Kaysville, Utah.) software. Thisstudy wasdesignedtoenrol270patientstoallowfor potentialdropoutofsubjects.
Data analysis was performed by using SPSS for Win-dows,version11.5(SPSSInc.,Chicago,IL, UnitedStates). Whilemetricdiscreteandcontinuousvariableswereshown
as mean±SD (min---max), number of cases and (%) were usedfornominaldata.Degreesofassociationbetween con-tinuousvariableswerecalculatedby Pearson’scorrelation coefficient.SimpleLinearRegressionanalyseswereapplied fordeterminingtheeffectofsizeoftheI-gelondifferences inbothTh-widthandalsoTh-lengthmeasurements. Coeffi-cientofregressionand95%confidenceintervals werealso calculated.Ap-valuelessthan0.05wasconsidered statis-ticallysignificant.
Results
Twohundredand seventypatients were initiallyscreened forthisstudy.Operationwascancelledinsevenpatientson thescheduledday. Patientcharacteristics andtypeofthe proceduresarepresentedinTable1.Themean(SD)agewas 47.3months(34.7)andmean(SD)weightwas16.4kg(8.0). Themost commonly usedLMA sizewas2, insertedin 127 (48.8%)patients,followed byLMA size1.5, inserted in61 (23.4%).LMAsize2.5and1wereusedin40(15.3%)and32 (12.3%),respectively.
Table 1 Demographic data and type of the procedures (n=260).
Age(month) 47.3±34.7(0---144)
Weight(kg) 16.4±8.0(2---36)
Gender
Male 158(61%)
Female 102(39%)
ASAclassification
1 223(86%)
2 37(14%)
Typeoftheprocedures
Herniotomy 130(50%) Circumcision 37(14%) Ophthalmologyoperations 40(15%) Minororthopaedicprocedures 19(7%) Reconstructionofminorlimb
deformities
13(5%)
Magneticresonanceimaging undergeneralanaesthesia
21(8%)
Valuesaremean±standarddeviation(minimum---maximum)or
Figure3 Thenareminenceofa19-month-oldgirlweighing11kgandsize1.5I-gelTMairwaydevicethatiscompatiblewiththe patient’sweight.
Themean(SD)valuesfor(Ig-w)and(Ig-l)were2.98cm (0.53) and 4.54cm (0.82), and the mean (SD) values for (Th-w)and(Th-l)were2.99cm(0.60)and3.88cm(0.93), respectively.Therewasastatisticallysignificantcorrelation betweenTh-wandIg-w(r=0.794,p<0.001).Astatistically significantcorrelationwasalsoobservedbetweenTh-land Ig-l (r=0.820, p<0.001)(Figs. 2 and3).According tothe simplelinearregressionanalyses,each1cmincreaseinIg-w measurementresulted in 0.906cm increase in Th-w mea-surement(95%confidenceinterval,0.821---0.991;p<0.001), and each 1cm increase in Ig-l measurement resulted in 0.925cm increase in Th-l measurement (95% confidence interval,0.846---1.004;p<0.001),
Successful insertion of the I-gel was achieved in 250 (95.0%)patients on thefirst attempt. Tenpatients (3.8%) requiredsecondattempt.Failurewasobservedin3(1.1%) patients(2children fromsize1.5and1 fromsize 2).The device couldnot beadvanced in the mouth in 2 patients (1fromsize1.5and1fromsize2),andsufficient ventila-tion(tidalvolume>6mLkg−1)couldnotbeachievedinone
patientfromsize1.5.In34childrenweighing10---12kgsize 1.5I-gelwassuccessfullyinsertedonthefirstattempt.The results for 260 patients were included in the study. Suc-cess rates and causes of failure of insertion of the I-gel onfirstattemptwereshown inTable2.Agastric catheter wasplacedthroughthe gastric channel successfullyin all patientsexceptinthosesize1I-gelwasplaced.
Laryngospasmoccurredin5(1.9%)patientsafterremoval of the device and resulted in brief episodes of hypoxia (1.9%).Bloodstainingonthedevicewasobservedin2(0.7%) patientsinwhomthedevicecouldbeinserted atthe sec-ondattempt. Coughoccurred in 10(3.8%) children inthe recoveryroom,andresolvedspontaneously.
Discussion
This studyshows thatthe dimensions of thenareminence werefittedtothatofweightbasedsizeoftheI-gel.Although
sizeselectiononaweightbasisshouldbeapplicabletothe majorityofpatients,individualanatomicalvariationsmean theweightguidanceprovidedshouldalwaysbeconsidered in conjunction with aclinical assessment of the patient’s anatomy.Zahooretal.suggestedthatphysicianscanapply ear-size method when using LMA in children.2 The I-gel differsfromtheLMAforitsshape,dimensionsand weight-basedscale. Accordingtoourfirstobservation,shapeand sizeofthethenareminenceweresimilartothatoftheI-gel’s cuff.Therefore wedecidedtoinvestigate thisanatomical region. We chose the size of the I-gel according to the patient’sweighttopreventabiasraisedfrominvestigator’s observation.Aftersuccessfulinsertionandadequate venti-lationwereconfirmed,wemeasured thethenareminence dimensionsofthepatient.
Inpreviousstudies,itwasseenthatonlytheperformance of theI-gelwasinvestigatedor itsperformancewas com-paredwiththatoftheothersupraglotticdevices.Size1I-gel wasnotevaluatedin thesestudies.1,5---9 Similarly, children undertheageof6monthswerenotrecruitedtothestudy in whichear-sized methodwassuggestedwhenusing LMA in children.2 An advantageof ourstudy comparedto oth-erswasthatallpaediatricsizesofI-gelwereinvestigated.
Table2 Successratesandcausesoffailureofinsertionof theI-gel.
Successrate
Firstattempt 250(95%) Secondattempt 10(3.8%)
Failure 3(1.1%)
Causesoffailureonfirstattempt
Incorrectplacementand inadequateventilation
11(84.6%)
Failureofinsertionofthedevicein themouth
2(15.3%)
Inaddition,therewerenodatainthe literatureaboutan alternativemethodforsizeselectionoftheI-gelinchildren. Accordingtoourresults,astatisticallysignificant correla-tionbetweenthedimensionofthethenareminenceandthe manufacturer’sdimensions oftheI-gelwhichwasinserted into the patients was found. Therefore, we can say that thenareminencemaybeusedasalandmarkwhenchoosing thesizeoftheI-gelinpaediatricpatients.
The successrateoftheinsertionat thefirstattemptin thestudy wascomparablewiththe reportedrates in pre-vious studies.5,6,8 Successfully insertionof the nasogastric tubeinallpatientsinwhomsize1.5,2and2.5I-gelwere insertedconfirmed theplaceofthedevice.Easy insertion ofanasogastrictubeiscorrelatedwithgoodpositioningof thedevice,andsofibreopticconfirmationisnotrequired.10 Correctplacementofthesize1I-gelwasevaluatedby sym-metric chest expansion, square wave of the capnograph trace,andabsenceofaudibleleakbecausesize1I-gelhasno gastricchannel.Accordingtooursuccessratewecanstate that sizeselection based onpatient’s weightis areliable method, but an additional method toconfirm the appro-priatenessoftheselectedsizemaybeusefulespeciallyin emergencysituations.Supraglotticairwaydevicescouldbe agoodsubstituteforairwaymanagementduring cardiopul-monary resuscitation. Gatward et al. reported that time takenforI-gelinsertionwasapproximately50%thatofother airwaydevices,suchasthetrachealtube,classicLMAand ProSealLMAduringchestcompressionforcardiopulmonary resuscitation.11ClinicianswhousetheI-gelinseldomwhen comparedtoanaesthesiologistsmaydoubtaboutsize selec-tion.Thenareminencemayalsobehelpfulinthissituation. Complication ratesobserved inthisstudy were compa-rable with that of previous studies.8,9 I-gel has a soft, non-inflatablecuff.Thischaracteristicoffersadvantagefor maintaining the blood supply to laryngeal and perilaryn-gealframework.Cuff inflationcancausetissueinjuriesor ischaemiathat may beobserved asa complication in the managementofthesupraglotticairwaydeviceswith inflat-ablecuff.12
Onelimitationofthisstudyisthatweinvestigatedthis anatomicalregioninhealthychildrenandit maynotbea landmarkinchildrenwithsyndromeordisordersinfluencing boneorsofttissuegrowth.
Summary
This descriptive study in children evaluating the associa-tionbetweensizesofthethenareminenceandI-gel’scuff showsthatthisanatomicalregionmaybeusedasalandmark
whenusingallpaediatricsizesoftheI-gel.Thereliabilityof theweight-basedmethodandtheperformanceoftheI-gel inpaediatric patientswereapprovedonceagain.Asimple methodlikethenareminencedimensionmaybeespecially relevantforambulancestaffandemergencyphysicians.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.BeylacqL,BordesM,SemjanF,etal. TheI-gel,asingle-use supraglotticairway device witha non-inflatablecuff and an esophagealvent:anobservationalstudyinchildren.Acta Anaes-thesiolScand.2009;53:376---9.
2.ZahoorA,AhmadN,SerecheG,etal.Anovelmethodfor laryn-geal maskairway sizeselection inpaediatricpatients. EurJ Anaesthesiol.2012;29:386---90.
3.Gregory GA.Induction ofanesthesia.In: GregoryGA,editor. Paediatricanesthesia,2nded.NewYork:ChurcillLivingstone; 1989.p.539---60.
4.Intersurgical:Userguide:I-gel® supraglotticairway,adultand paediatricsizes.Wokingham,Berkshire,UnitedKingdom: Inter-surgical;2010.
5.Goyal R, Shukla RV, Kumar G. Comparison of size 2 I-gel supraglotticairway with LMA-ProsealTM and LMA-ClassicTM in spontaneouslybreathingchildrenundergoingelectivesurgery. PaediatrAnaesth.2012;22:355---9.
6.AbukawaY,HirokiK, Ozaki M.InitialexperienceoftheI-gel supraglottic airway bythe residents inpediatric patients. J Anesth.2012;26:357---61.
7.FukuharaA,OkutaniR,OdaY.Arandomizedcomparisonofthe I-gelandtheProSeallaryngealmaskairwayinpediatricpatients: performanceandfiberopticfindings.JAnesth.2013;27:1---6.
8.JagannathanN,SommersK,SohnLE,etal.Arandomized equiv-alencetrialcomparingtheI-gelTM andlaryngealmaskairway SupremeTMinchildren.PaediatrAnaesth.2013;23:127---33.
9.TheilerLG,Kleine-BrueggeneyM,LuepoldB,etal.Performance ofthepediatric-sizedI-gelcomparedwiththeAmbuAuraOnce laryngealmaskinanesthetizedandventilatedchildren. Anes-thesiology.2011;115:102---10.
10.BrimacombeJ,KellerC.Aspirationofgastriccontentsduring useofaProSeallaryngealmaskairwaysecondarytounidentified foldovermalposition.AnesthAnalg.2003;97:1192---4.
11.GatwardJJ,ThomasMJ,NolanJP,etal.Effectofchest com-pressionsonthe timetaken toinsertion airway devicesina manikin.BrJAnaesth.2008;100:351---6.