www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
REVIEW
ARTICLE
Clinicopathological
characteristics
and
perineural
invasion
in
adenoid
cystic
carcinoma:
a
systematic
review
夽
,
夽夽
Afonso
Nóbrega
Dantas
a,
Everton
Freitas
de
Morais
a,
Rômulo
Augusto
de
Paiva
Macedo
a,
João
Maria
de
Lima
Tinôco
a,∗,
Maria
de
Lourdes
Silva
de
Arruda
Morais
a,b,c,daUniversidadePotiguar(UnP),Natal,RN,Brazil
bUniversidadedoEstadodoRioGrandedoNorte(UERN),Natal,RN,Brazil cLigaNorte-RiogradensecontraoCâncer,Natal,RN,Brazil
dUniversidadeFederaldoRioGrandedoNorte(UFRN),Natal,RN,Brazil
Received15June2014;accepted22July2014 Availableonline30March2015
KEYWORDS
Salivarygland neoplasms; Salivaryglands; Mouthneoplasms
Abstract
Introduction:Adenoid cystic carcinoma is the most frequent malignant tumor of the sub-mandibularglandandtheminorsalivaryglands.Itisamalignantneoplasmthat,despiteits slowgrowth,showsanunfavorableprognosis.
Objectives: The aimofthis study was toperform asystematic reviewof theliterature on Adenoidcysticcarcinomaintheheadandneckregionanditsclinicopathologicalcharacteristics, withemphasisontheperineuralinvasioncapacityofthetumor.
Methods:A systematicsearchofarticlespublishedbetween January2000andJanuary 2014 wasperformedinthePubMed/MEDLINE,SciELO,ScienceDirect,andScopusdatabases. Results:Ninearticleswereselectedforthissystematicreview.Thesedemonstratedthatthe femalegenderwasmoreoftenaffectedandthatmalignanttumorsshowedahighrateofdistant metastasis,recurrence,andalowsurvivalrate.Thepresenceofperineuralinvasionrangedfrom 29.4%to62.5%andwasassociatedwithlocaltumorrecurrence.
Conclusion: Adenoidcysticcarcinomaiscommonlycharacterizedbythepresenceofpain,high rateofrecurrence,metastasis,andalowsurvivalrate.Reportingstudieswithpatient follow-upisofutmostimportanceforabetterclinical-pathologicalunderstandingandtoimprovethe prognosisofthispathology.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:DantasAN,deMoraisEF,MacedoRA,TinôcoJM,MoraisML.Clinicopathologicalcharacteristicsandperineural
invasioninadenoidcysticcarcinoma:asystematicreview.BrazJOtorhinolaryngol.2015;81:329---35.
夽夽Institution:UniversidadePotiguar(UnP),Natal,RN,Brazil.
∗Correspondingauthor.
E-mail:[email protected](J.M.d.L.Tinôco).
http://dx.doi.org/10.1016/j.bjorl.2014.07.016
PALAVRAS-CHAVE
Neoplasiasdas glândulassalivares; Glândulassalivares; Neoplasiasbucais
Característicasclinicopatológicaseinvasãoperineuraldocarcinomaadenoidecístico
Resumo
Introduc¸ão:Ocarcinomaadenoidecístico(CAC)éotumormalignomaisfrequentedaglândula Submandibularedasglândulassalivaresmenores.Sendoumaneoplasiamaligna,apesardeter crescimentolento,apresentaumprognósticodesfavorável.
Objetivos: Oobjetivodestetrabalhofoirealizarumarevisãosistemáticadeliteraturasobre ocarcinoma adenóidecístico naregião decabec¸a epescoc¸o e suascaracterísticas clínico-patológicascomênfasenacapacidadedeinfiltrac¸ãoperineuraldotumor.
Método: Umabuscasistemáticadeartigospublicadosentrejaneirode2000ajaneirode2014 foiexecutadanasbasesdedadosPubMed/MEDLINE,SciELO,ScienceDirecteScopus.
Resultados: Noveartigosforamselecionadospararealizac¸ãodarevisãosistemática.Nestes,o sexofemininofoiomaisafetadoeotumormalignoapresentouumaaltataxademetástase adistância,recidivaebaixataxadesobrevida.Apresenc¸adeinvasãoperineuralvariouentre 29,4%a62,5%efoirelacionadaàrecidivalocaldotumor.
Conclusão:OCACé comumentecaracterizado pela presenc¸a dedor, altataxade recidiva, metástase ebaixa sobrevida. A realizac¸ãode estudos comacompanhamento dospacientes édeextrema importânciapara umamelhoravaliac¸ão clinico-patológicavisandomelhoraro prognósticodadoenc¸a.
©2015Associac¸ãoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Salivaryglandneoplasmsareunusualandaccountforonly about2---6.5%oftumorsoftheheadandneckregion.1The frequency of different types of malignant tumors varies according to the site of origin. However, adenoid cystic carcinoma (ACC) appears to be the most common malig-nanttumorofthesubmandibularsalivaryandminorsalivary glands.2
TheACCisamalignantneoplasmthat,inspiteofitsslow growth,hasapoorprognosisduetoaggressivetumor inva-sionandahighrateofrecurrence.3Thisneoplasmwasfirst describedbyBillrothin1856.4
It candevelop in several anatomicalsites, suchasthe majorandminorsalivaryglands,lacrimalglands,andupper aerodigestive tract glands.5 In the buccal-maxillofacial region,it accountsforapproximately22%ofneoplasms of major and minor salivary glands, with the minor salivary glandsof the hard palate representing the main affected site.2
ACCismoreprevalentinmiddle-agedadultsand accord-ing to many studies, it is more frequent in the female gender.5,6Distantmetastasisiscommon;thelungisthemost commonlyaffectedsite.7
Itmaypresentclinicallyasahardenedlump,andpainis animportantandcommonfindingintheinitialcourseofthe disease.Anulceratedlesioncanbeseenonthepalate,with bonedestructionidentifiedradiographically.8
Histopathologically,ACCcanmanifestasdifferenttypes, withthreemain recognizedpatterns9: the cribriformand tubularpatterns, which are lessaggressive, and thesolid pattern,whichshowscellpleomorphismandmitotic activ-ity,aswellasnecroticfociinthecentralregionofneoplastic cellislands.5,6
Perineuralinvasionisacommonhistologicalfinding,and isconsideredapossibleroutefortumorcelldissemination.5 Perineuralinvolvementoccursin approximately22---46% of casesofACC,whetheratmacro-ormicroscopiclevel.5
Surgeryisthetreatmentof choiceforACCandmaybe followedbyradiationtherapyand,inrarecases, chemother-apy. The frequency of local recurrence for ACC is high, requiringadditionalsurgicalresections.Severalstudieshave evaluated this development as a negative one, with the tumorcausingthepatient’sdeath.9
Dentalsurgeonsneedtodetect anychangesintheoral mucosaof theirpatients.Earlydiagnosis ofACCresults in betterqualityoflifeandhighersurvivalrate.Theobjective ofthisstudywastoperformasystematicreviewof litera-tureonACCoftheheadandneckregionanditsclinicaland pathological features, withemphasis on tumor perineural invasioncapacity.
Methods
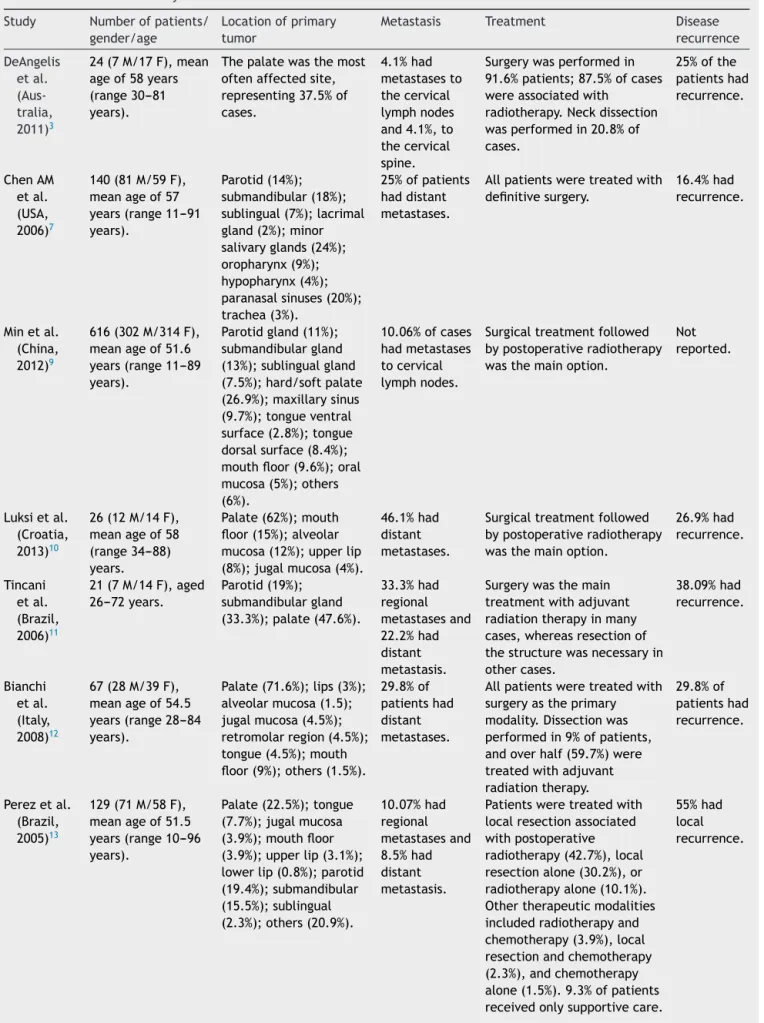
Table1 Resultsobtainedbytheselectedstudies. Study Numberofpatients/
gender/age
Locationofprimary tumor
Metastasis Treatment Disease
recurrence DeAngelis etal. (Aus-tralia, 2011)3
24(7M/17F),mean ageof58years (range30---81 years).
Thepalatewasthemost oftenaffectedsite, representing37.5%of cases.
4.1%had metastasesto thecervical lymphnodes and4.1%,to thecervical spine.
Surgerywasperformedin 91.6%patients;87.5%ofcases wereassociatedwith
radiotherapy.Neckdissection wasperformedin20.8%of cases.
25%ofthe patientshad recurrence. ChenAM etal. (USA, 2006)7
140(81M/59F), meanageof57 years(range11---91 years).
Parotid(14%); submandibular(18%); sublingual(7%);lacrimal gland(2%);minor salivaryglands(24%); oropharynx(9%); hypopharynx(4%); paranasalsinuses(20%); trachea(3%).
25%ofpatients haddistant metastases.
Allpatientsweretreatedwith definitivesurgery.
16.4%had recurrence.
Minetal. (China, 2012)9
616(302M/314F), meanageof51.6 years(range11---89 years).
Parotidgland(11%); submandibulargland (13%);sublingualgland (7.5%);hard/softpalate (26.9%);maxillarysinus (9.7%);tongueventral surface(2.8%);tongue dorsalsurface(8.4%); mouthfloor(9.6%);oral mucosa(5%);others (6%).
10.06%ofcases hadmetastases tocervical lymphnodes.
Surgicaltreatmentfollowed bypostoperativeradiotherapy wasthemainoption.
Not reported.
Luksietal. (Croatia, 2013)10
26(12M/14F), meanageof58 (range34---88) years.
Palate(62%);mouth floor(15%);alveolar mucosa(12%);upperlip (8%);jugalmucosa(4%).
46.1%had distant metastases.
Surgicaltreatmentfollowed bypostoperativeradiotherapy wasthemainoption.
26.9%had recurrence. Tincani etal. (Brazil, 2006)11
21(7M/14F),aged 26---72years.
Parotid(19%); submandibulargland (33.3%);palate(47.6%).
33.3%had regional metastasesand 22.2%had distant metastasis.
Surgerywasthemain treatmentwithadjuvant radiationtherapyinmany cases,whereasresectionof thestructurewasnecessaryin othercases. 38.09%had recurrence. Bianchi etal. (Italy, 2008)12
67(28M/39F), meanageof54.5 years(range28---84 years).
Palate(71.6%);lips(3%); alveolarmucosa(1.5); jugalmucosa(4.5%); retromolarregion(4.5%); tongue(4.5%);mouth floor(9%);others(1.5%).
29.8%of patientshad distant metastases.
Allpatientsweretreatedwith surgeryastheprimary modality.Dissectionwas performedin9%ofpatients, andoverhalf(59.7%)were treatedwithadjuvant radiationtherapy.
29.8%of patientshad recurrence.
Perezetal. (Brazil, 2005)13
129(71M/58F), meanageof51.5 years(range10---96 years).
Palate(22.5%);tongue (7.7%);jugalmucosa (3.9%);mouthfloor (3.9%);upperlip(3.1%); lowerlip(0.8%);parotid (19.4%);submandibular (15.5%);sublingual (2.3%);others(20.9%).
10.07%had regional metastasesand 8.5%had distant metastasis.
Patientsweretreatedwith localresectionassociated withpostoperative radiotherapy(42.7%),local resectionalone(30.2%),or radiotherapyalone(10.1%). Othertherapeuticmodalities includedradiotherapyand chemotherapy(3.9%),local resectionandchemotherapy (2.3%),andchemotherapy alone(1.5%).9.3%ofpatients receivedonlysupportivecare.
Table1(Continued)
Study Numberofpatients/ gender/age
Locationofprimary tumor
Metastasis Treatment Disease
recurrence
Khanetal. (USA, 2001)14
68(30M/38F), meanageat diagnosisof52 years.
Themostaffectedsites weretheoropharynx (23.5%),parotid (22.05%),submandibular gland(16.17%).
10.2%had pulmonary metastasisand 5.8%hadlymph node
metastasis.
Theprimarytreatmentwas surgery.8.8%ofpatients underwentradiation,7.3%of patientswerepoorsurgical candidatesdueto
comorbidities,andwere treatedwithcurativeintent, while1.4%ofpatientswere treatedwithpalliativecare.
42.6%had recurrence.
Sungetal. (Korea, 2003)15
94(44M/50F),age of44.5years(range 20---78years).
Themostaffectedsites weretheminorsalivary glands(69.1%)andthe majorsalivaryglands (30.8%).
26.5%of patientshad distant metastasesand 3.1%had regional metastasis.
Incasesofpatientswith distantmetastases,10.6% weretreatedwithsurgery, 8.5%withradiotherapy,and 29.7%withboth.Inpatients withoutdistantmetastasis, 6.3%weretreatedwith surgery,7.4%with
radiotherapy,and37.2%with both.
18.08%had recurrence.
M,male;F,female.
Theinclusioncriteriawere:studiespublishedinEnglish, Portuguese, or Spanish; cross-sectional and longitudinal studiesaimedatevaluatingACCoftheheadandneckregion anditsperineuralinvasioncapacity;articlespublishedfrom Januaryof2000onward.Theexclusioncriteriawere:review articles,populationthatdidnotmatchtheresearch stan-dards,clinicalcases,andarticlespublishedbeforetheyear 2000orinadifferentlanguagefromthoseselectedforthis systematicreview.
Thefirststepinstudyselectionwasanalysisoftitlesand abstracts.Subsequently,allstudieswhosetitlesorabstracts were considered relevant were obtained and analyzed in full;finally,thearticlesanalyzedandselectedbythe eval-uators after a consensus meeting were included in the systematizationofdata.
Results
Among the initiallyselected studies, 29 showedpotential tobeincludedinthesystematicreview;however,afterfull analysisofthestudiesanddiscussionoftheircontentsbythe evaluators,theyagreedthatonlyninearticlesmetall inclu-sioncriteria.3,7,9---15Amongtheselectedstudies,threewere carriedout in developing countries9,11,13 and six in devel-opedones.3,7,10,12,14,15Articlemethodsandresultsareshown inTables1and2.
Regarding the study profiles, sample size ranged from 2111to6169patients,withthetotalsamplesizebeing1185 patientswithamean age>50 years.The selectedstudies werepublishedbetweentheyears2001and2013.Allofthe selectedstudieswereretrospective.
Theobjectivesoftheselectedstudieswere:toperform theanalysisoftheclinicalandpathologicalcharacteristics ofACC,analyzingvariablessuchasgender,3,7,9---15age,3,7,9---15
metastasis,3,7,9---15 recurrence,3,7,10---15 perineural invasion capacity,3,7,9---15survivalrates,3,7,9---15andtreatment.3,7,9---15
Among thestudies selected for thissystematic review, sevenshoweddifferencebetweengenders,withthefemale gendermoresusceptibletoACC.3,9---12,14,15Onlytwostudies showedahighernumberofcasesinmales.7,13
Thepalatewasthemostoftenaffectedsiteinthe major-ityoftheselectedstudies,3,9---13 reaching71.6%ofcasesin thestudybyBianchietal.12InthestudybyKhanetal.,14the most oftenaffected sitewastheoropharynx, followed by theparotidandsubmandibularglands.Amongtheselected studies,allassessedthepresenceofmetastasis(Table1).
Thepresenceofperineuralinvasionwasaconstantinthe selectedstudies.IntheretrospectiveanalysisbyMinetal.,9 328patientshadperineuralinvasion,with40patients show-ingpositiveproximalmetastasisand288negative.Fifteen caseswererecordedinthestudybyDeAngelisetal.3and13 casesinthestudybyLuksiéetal.10Tincanietal.11reported ninecasesofperineural invasion,whereasBianchietal.12 reported39cases.TheretrospectivestudybyPerezetal.13 reported the presence of 58 cases, whereas Chen etal.7 reported82cases.Khanetal.14reportedthepresenceof20 casesofperineuralinvasion,whileSungetal.15reported29 patients,12withpositivedistantmetastasesand17 nega-tive.InthestudyperformedbyLukisietal.,10therewasno significant associationbetweenthepresenceof perineural invasion andprimarytumor size, presence of proximalor distantmetastasis,orinvasionofmargins;however,itwas associatedwithlocaltumorextent.
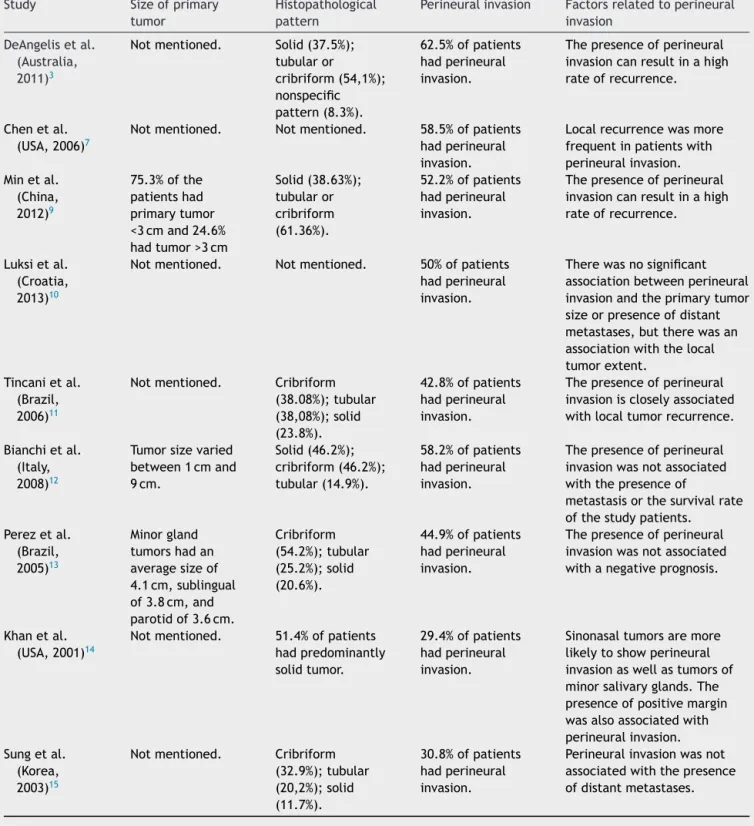
Table2 Tumorcharacteristicsandperineuralinvasion.
Study Sizeofprimary
tumor
Histopathological pattern
Perineuralinvasion Factorsrelatedtoperineural invasion
DeAngelisetal. (Australia, 2011)3
Notmentioned. Solid(37.5%); tubularor cribriform(54,1%); nonspecific pattern(8.3%).
62.5%ofpatients hadperineural invasion.
Thepresenceofperineural invasioncanresultinahigh rateofrecurrence.
Chenetal. (USA,2006)7
Notmentioned. Notmentioned. 58.5%ofpatients hadperineural invasion.
Localrecurrencewasmore frequentinpatientswith perineuralinvasion. Minetal.
(China, 2012)9
75.3%ofthe patientshad primarytumor <3cmand24.6% hadtumor>3cm
Solid(38.63%); tubularor cribriform (61.36%).
52.2%ofpatients hadperineural invasion.
Thepresenceofperineural invasioncanresultinahigh rateofrecurrence.
Luksietal. (Croatia, 2013)10
Notmentioned. Notmentioned. 50%ofpatients hadperineural invasion.
Therewasnosignificant associationbetweenperineural invasionandtheprimarytumor sizeorpresenceofdistant metastases,buttherewasan associationwiththelocal tumorextent.
Tincanietal. (Brazil, 2006)11
Notmentioned. Cribriform (38.08%);tubular (38,08%);solid (23.8%).
42.8%ofpatients hadperineural invasion.
Thepresenceofperineural invasioniscloselyassociated withlocaltumorrecurrence.
Bianchietal. (Italy, 2008)12
Tumorsizevaried between1cmand 9cm.
Solid(46.2%); cribriform(46.2%); tubular(14.9%).
58.2%ofpatients hadperineural invasion.
Thepresenceofperineural invasionwasnotassociated withthepresenceof
metastasisorthesurvivalrate ofthestudypatients. Perezetal.
(Brazil, 2005)13
Minorgland tumorshadan averagesizeof 4.1cm,sublingual of3.8cm,and parotidof3.6cm.
Cribriform (54.2%);tubular (25.2%);solid (20.6%).
44.9%ofpatients hadperineural invasion.
Thepresenceofperineural invasionwasnotassociated withanegativeprognosis.
Khanetal. (USA,2001)14
Notmentioned. 51.4%ofpatients hadpredominantly solidtumor.
29.4%ofpatients hadperineural invasion.
Sinonasaltumorsaremore likelytoshowperineural invasionaswellastumorsof minorsalivaryglands.The presenceofpositivemargin wasalsoassociatedwith perineuralinvasion. Sungetal.
(Korea, 2003)15
Notmentioned. Cribriform (32.9%);tubular (20,2%);solid (11.7%).
30.8%ofpatients hadperineural invasion.
Perineuralinvasionwasnot associatedwiththepresence ofdistantmetastases.
totalof71patients(55%)withrecurrence.Minetal.9does not mention the presence of recurrence. Overall survival rateswerevariablebetweenstudies.Inthestudyby DeAn-gelis etal.,3 overall survival rates at 5, 10,and 20 years were,respectively,92%,72%,and54%.InthestudybyMin etal.,9thesurvivalratewascorrelatedwiththeoccurrence ofmetastases,withanoverallfive-yearsurvivalinpatients withlymphnode metastasis of 48%,and in thosewithout lymphnodemetastasis,77%.InthestudybyLuksietal.,10
survivalrateswere62%atfiveyears,53%at10years,and 27%at15years.
Discussion
tumors were more frequently found among the female population,3,10---15 whereastwo studies showed the tumors weremorefrequent in themalegender.7,9In spite ofthe divergence,thescientificliteraturedemonstratesagreater susceptibilityinwomen.16
InthestudybyPerezetal.,13themostcommonclinical signsandsymptomswerethepresenceofnodular enlarge-ment(92.1%), pain(59.8%),paresthesia (12.6%)andnasal congestion(11.8%).IntheanalysisbyBianchietal.,12 pri-marytumorsizevariedbetween1cmand9cm.Studieshave shownthattumors>3cmmayhaveahighmetastaticrate, apartfromotherfactorssuchasgender,age,andperineural invasion.17,18
Among the studies that evaluated histopathological types,the most frequent wasthe cribriformpattern, fol-lowedbytubularandsolidpatterns.3,9,11,13,15Inthestudyby Khanetal.,14 therewasa predominanceof thesolid pat-tern,whereasinthestudybyBianchietal.,12 thenumber ofaffectedcasesshowingthecribriformandsolidpatterns weresimilar.
Thepalatewasthemostoftenaffectedsiteinthe major-ityofthe selectedstudies,which isconsistent withother studies.1,2,4 Only the study by Khan etal.14 mentions the oropharynxas the most often affected site. A study per-formed in 2007 shows that tumor location in the minor salivary glands may favor tumor recurrence and a worse prognosis.18
Allselectedstudiesanalyzedthepresenceofmetastases inpatients withACC. Inthestudy bySung etal.,15 which assessedthe predictive factors and the impactof distant metastases in ACC in a total of 94 patients, 25 had dis-tantmetastases,whilethreehadregionalmetastasis.Other studies have shown similarresults, where the most com-monsites ofmetastasis werethelungs(80%),bone(15%), andliverandothersites(5%);thesemetastasesmayappear even20yearsafterprimarytumor resection,representing themajorcauseoftreatmentfailure.19,20However,among theselectedstudies,thereweresimilaritiesbetweencases ofdistantandregionalmetastasis.11,13
RecurrenceisfrequentamongpatientswithACC.3,7,10---15 Tumor location in the minor salivary glands favors recur-renceandappearstobeassociatedwiththemoreadvanced casesandworseprognosis.18InthestudybyKhanetal.,1429 patientshadlocalrecurrenceandtheauthorassociatedthe presenceofperineural invasionwithincreasedrecurrence rates, as well as a higher incidence of positive margins, which is consistent with the other selected studies.3,7,9,11 Astudy conductedin1997found adecreasein recurrence ratesovertheyearsduetotheeffectsofradiotherapyuse, butwithnosignificantimpactondistantmetastasisrates.17 Pain and discomfort complaints are not unusual and are often attributed to tumor invasive behavior. Tumor cells tend to invade and disseminate peripherally to the nervefascicles. Perineuralinvasionis a common histolog-icalfinding, andis considered a possible route for tumor cell dissemination.5,18 In the study by Khan et al.,14 per-ineuralinvasionwasassociatedwithhigherrecurrencerate andpositivesurgicalmargins;however,thestudybyPerez etal.13 did not show similar results. None of the studies associatedthepresenceofperineuralinvasiontometastasis orsurvivalrate;however,studieshaveshownthatpatients withperineuralinvasionrequireradiotherapy.21,22
Themostcommonlyusedtreatmentmodalitywas surgi-cal,whetheror notfollowedbyradiotherapy.Inthestudy by deDeAngelisetal.,3 neckdissectionwasperformed in five cases, whereasfor Khan et al.,14 this treatment was used only in cases that showed some clinical or imaging signthatjustifieditsuse,consideringthelowrateofnodal metastaticinvolvement.Perezetal.13 alsoreportedcases treatedwithassociatedchemotherapy;however,the impor-tanceofadjuvantchemotherapyaftersurgeryhasnotbeen systematicallyexplored.23
Thesurvivalratevariedamongthe selectedstudies. In thestudy byDeAngelis etal.,3overall survivalrates were 92%atfiveyears,72%at10years,and54%in20years.In thestudybyLuksicetal.,14 survivalrateswere62%atfive years,53%at10years,and27%at15years.ForMinetal.,9 lifeexpectancywasdirectlyassociatedwiththeoccurrence ofmetastasesandtheoverallfive-yearsurvivalofpatients withlymphnodemetastasiswas48%,whereasitwas77%in patientswithoutmetastasis.Perezetal.13 mentionedthat the solidpattern hasa lowersurvival rate;the impactof the solidtumorsonsurvivalcan beexplained,inpart, by theirgreatermetastaticpotential.DeAngelisetal.3 demon-stratedthatpatientsurvivalratedecreasesconsiderablyin serieswithafollow-uplastingmorethan15years.
Conclusion
ACCisamalignantneoplasmofglandulartissuethathasa higherincidenceinfemalesandiscommonlycharacterized bythepresenceofpain,highrateofrecurrence, metasta-sis,andpoorsurvival.The presenceofperineuralinvasion wasnotassociatedwithmetastasisorsurvivalrate,butwas associatedwiththepresenceoflocalrecurrenceandmargin involvement,inadditiontoinfluencingappropriatepatient treatment.Studieswithlong-termfollow-upofpatientsto evaluate the clinical aspects of the tumor are extremely importantforbetterunderstandingofACC,aswellas bet-terclinical-pathologicalevaluation inordertoimproveits prognosis.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.SantosGC,Martins MR,PellacaniLB,Vieira ACT,Nascimento LA, AbrahãoM.Neoplasias de glândulassalivares:estudo de 119casos.JBrasPatolMedLab.2003;39:371---5.
2.WangD,LiY,HeH,LiuL,WuL,HeZ.Intraoralminorsalivary glandtumorsinaChinesepopulation:aretrospectivestudyon 737cases.OralSurgOralMedOralPatholOralRadiolEndod. 2007;104:94---100.
3.DeAngelisAF, Tsui A, Wiesenfeld D,Chandu A. Outcomes of patientswithadenoid cysticcarcinomaoftheminorsalivary glands.IntJOralMaxillofacSurg.2011;40:710---4.
4.KokemuellerH,EckardtA,BrachvogelP,HausamenJE.Adenoid cysticcarcinomaoftheheadandneck---a20yearsexperience. IntJOralMaxillofacSurg.2004;33:25---31.
6.EllisGL,Auclair PL.Atlas oftumor pathology tumors ofthe salivaryglands.3rded.AFIP;1996.p.155---373.
7.ChenAM,BucciMK,WeinbergV,GarciaJ,QuiveyJM,Schechter NR, et al. Adenoid cystic carcinoma of the head and neck treatedbysurgerywithorwithoutpostoperativeradiation ther-apy:prognosticfeaturesofrecurrence.IntJRadiatOncolBiol Phys.2006;66:152---9.
8.SantosMESM,IbrahimD,SilvaNetoJC,SilvaUH,SobralAPV. Adenoid cysticcarcinoma: a case report. RevCir Traumatol Buco-Maxilo-Fac.2006;5:49---54.
9.MinR,SiyiL,WenjunY,OwA,LizhengW,MinjunD,etal. Sali-varyglandadenoidcysticcarcinomawithcervicallymphnode metastasis:apreliminarystudyof62cases.IntJOralMaxillofac Surg.2012;41:952---7.
10.Lukˇsi´cI,SutonP,Macan D,DinjarK.Intraoraladenoid cystic carcinoma:isthe presenceofperineural invasion associated withthesizeoftheprimarytumour,localextension,surgical margins,distantmetastases,andoutcome.BrJOralMaxillofac Surg.2014;52:214---8.
11.TincaniAJ,NegroAD,AraújoPPC,AkashiHK,MartinsAS, Alte-maniAM,et al.Managementofsalivaryglandadenoidcystic carcinoma:institutionalexperienceofacaseseries.SaoPaulo MedJ.2006;124:26---30.
12.BianchiB,CopelliC,CocchiR,FerrariS,PederneschiN,Sesenna E.Adenoidcysticcarcinomaofintraoralminorsalivaryglands. OralOncol.2008;44:1026---31.
13.PerezDEC,AlvesFAA,NishimotoIN,AlmeidaOP,KowalskiLP. Prognosticfactorsinheadandneckadenoidcysticcarcinoma. OralOncol.2006;42:139---46.
14.KhanAJ,DiGiovannaMP,RossDA,SasakiCT,CarterD,SonYH. Adenoidcysticcarcinoma:aretrospectiveclinicalreview.IntJ Cancer.2001;96:149---58.
15.SungMW,KimKH,KimJW,Min YG,SeongWJ,RohJL,etal. Clinicopathologicpredictors andimpactofdistantmetastasis from adenoid cystic carcinoma of the head and neck. Arch OtolaryngolHeadNeckSurg.2003;129:1193---7.
16.TriantafillidouK,DimitrakopoulosJ,IordanidisF,Koufogiannis D.Managementofadenoidcysticcarcinomaofminorsalivary glands.JOralMaxillofacSurg.2006;64:1114---20.
17.SpiroRH.Distantmetastasisinadenoidcysticcarcinomaof sali-varyorigin.AmJSurg.1997;174:495---8.
18.KoYH,LeeMA,HongYS,LeeKS,JungC,KimYS,etal. Pro-gnosticfactorsaffectingtheclinicaloutcomeofadenoidcystic carcinoma oftheheadandneck. JpnJClinOncol.2007;37: 805---11.
19.GuzzoM,LocatiLD,ProttFJ,GattaG,McgurkM,LicitraL,etal. Majorandminorsalivaryglandtumors.CritRevOncolHematol. 2010;74:134---48.
20.WahlbergP,AndersonH,BiörklundA,MöllerT,EperfektR. Car-cinomaoftheparotidandsubmandibularglands---astudyof survivalin2465patients.OralOncol.2002;38:706---13.
21.Cohen AN, Damrose EJ, Huang RY, Nelson SD, BlackwellKE, Calcaterra TC, et al. Adenoid cystic carcinoma of the sub-mandibulargland:a35-yearreview.JOtolaryngolHeadNeck Surg.2004;131:994---1000.
22.Garden AS, Weber RS, Morrison WH, Ang KK, Peters LJ. Theinfluence ofpositivemarginsandnerve invasionin ade-noid cystic carcinoma of the head and neck treated with surgeryand radiation.IntJRadiat Oncol BiolPhys.1995;32: 619---26.