BrazJOtorhinolaryngol.2016;82(5):614---617
www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
CASE
REPORT
Orbital
metastasis
as
the
primary
presentation
of
nasopharyngeal
carcinoma
夽
Metástase
orbital
como
apresentac
¸ão
primária
de
carcinoma
de
nasofaringe
Sung-Chan
Shin
a,
Sung-Lyong
Hong
a,
Chang-Hoon
Lee
b,
Kyu-Sup
Cho
a,∗aPusanNationalUniversityHospital,PusanNationalUniversitySchoolofMedicine,DepartmentofOtorhinolaryngologyand
BiomedicalResearchInstitute,Busan,SouthKorea
bPusanNationalUniversityHospital,PusanNationalUniversitySchoolofMedicine,DepartmentofPathology,Busan,SouthKorea
Received17March2015;accepted27April2015 Availableonline9September2015
Introduction
Metastasis to the orbit, which is uncommon due to the character of the orbital volume withrelative stenosis, is estimated to account for 1---13% of all orbital tumors.1
Orbital metastasis is believed to occur in approximately
2---3% of patients with systemic cancer.2 The incidence
of metastatic orbital tumors varies widely, according to
geographicalareaandrace;themostcommonprimary
can-cers that metastasize to the orbit are breast, prostate,
liver,andlungcancer.1,2Althoughnasopharyngealcarcinoma
(NPC) involves the orbits through direct extension tothe
orbitalapex,metastasisofNPCtotheorbithasrarelybeen
reported.This reportdescribes twocases of intraorbital,
extrabulbarmetastasesfromNPC.
夽 Pleasecitethisarticleas:ShinS-C,HongS-L,LeeC-H,ChoK-S.
Orbitalmetastasisastheprimarypresentationofnasopharyngeal carcinoma.BrazJOtorhinolaryngol.2016;82:614---7.
∗Correspondingauthor.
E-mail:[email protected](K.-S.Cho).
Case
reports
Case1
A52-year-oldmalewithabrupt-onsethoarsenessvisitedthe
authors’clinic.Hismedicalhistorywasotherwise
unremark-able.A1×1cmhard,fixedlymphnodewaspalpableinthe
rightlevelIIarea.Flexiblefiberopticlaryngoscopyrevealed
right vocal cord paralysis. An ulcerative nasopharyngeal
masswasobservedbynasalendoscopy.Computed
tomogra-phy(CT)oftheneckrevealedanenormousnasopharyngeal
mass extending into the right oropharyngeal, masticator,
carotid,prevertebral, andparavertebral space,with
mul-tiplebilateralcervicallymphnodesmetastases.Transnasal
endoscopic biopsy under localanesthesia and fine needle
aspiration on the right level II lymph node were
per-formed.Histopathologicexaminationrevealedkeratinizing
squamouscellcarcinoma(SCC)inboththenasopharyngeal
massandrightcervicallymphnode(Fig.1A).
Thepatientreceiveddocetaxelandcisplatin
chemother-apy. However, chemotherapy was stopped after the first
cycle due to neutropenic septic shock. Therefore, early
http://dx.doi.org/10.1016/j.bjorl.2015.04.006
Orbitalmetastasisofnasopharyngealcarcinoma 615
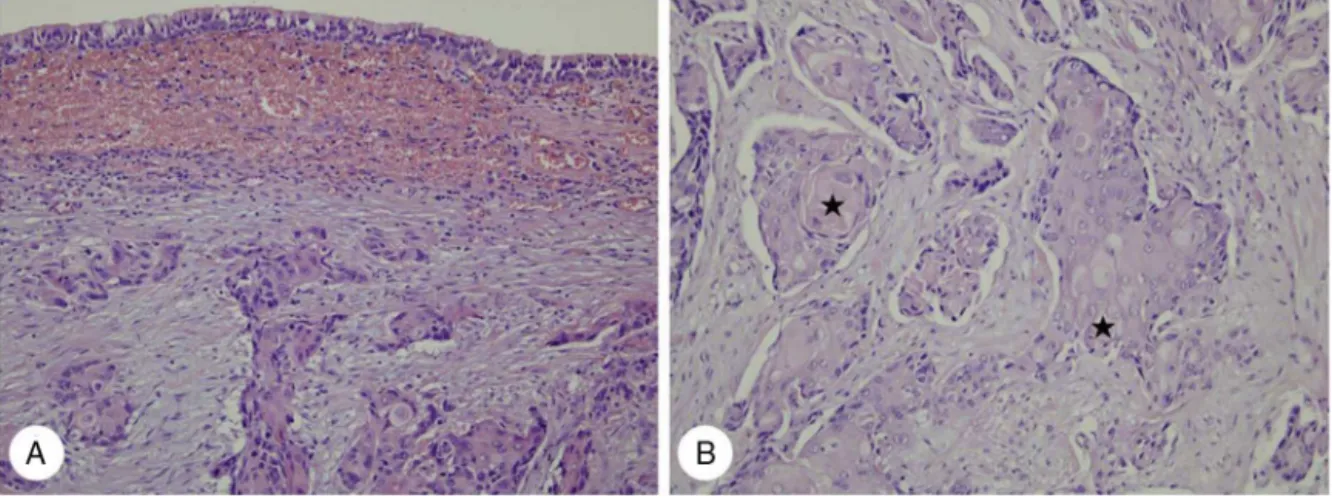
Figure1 Histopathologicfindingsofcase1.(A)Infiltratingkeratinizingcarcinomaofthenasopharynxisnotedbeneathnormal ciliatedcolumnarpseudostratifiedepithelium(H&E,×200).(B)Nasopharyngealkeratinizingcarcinomainfiltratingorbitalsofttissue
exhibitsdistinctcytoplasmickeratinformationwithpearlformation( )(H&E,×400).
radiotherapyofthenasopharynxandcervicallymphnodes
(totaldose=70Gy)wascompleted.Afteronemonth,mild
swellingintherightmedialcanthalareawasnoted.Visual
acuity,intraocularpressure,andocularmotilitywerewithin
normal limits and there was no exophthalmos. Orbit CT
revealed a newly developed 1.0×0.9cmsoft tissue mass
withindistinctmarginsontheinferomedialsideoftheright
orbit(Fig. 2Aand B). Magnetic resonance (MR) imagesof
thenasopharynxrevealedan oval-shapedorbitalmass
dis-playinglowsignalintensityonT1-weightedimages(T1WIs),
616 ShinS-Cetal.
intermediatesignalintensity onT2WIs, andmild
enhance-mentongadolinium-T1WIs(Fig.2CandD).Thiswasfollowed
by excisional biopsy that confirmed the diagnosis of
ker-atinizing SCC(Fig. 1B). On positron emission tomography
(PET)/CTscan,multipleareasofincreased
fluorodeoxyglu-cose(FDG)uptakeweredetectedintheliver,diagnosedas
distantlivermetastases.Therefore,thepatientreceivedsix
cyclesofpalliative chemotherapywithTS-1andcisplatin.
AlthoughprimaryNPCandorbitalmetastasisdidnotrecur,
thepatientdied17monthsafterdiagnosisoforbital
metas-tasisduetoliverfailure.
Case2
A 67-year-old male presented with abrupt-onset ocular
pain and blurred vision, which he had first noticed one
month prior to presentation. He was seen by a
neuro-ophthalmologist, who observed visual loss to no light
perceptionontheright.The patient’smedicalhistorywas
otherwiseunremarkable.Nasalendoscopyrevealed amild
contourprotrusionwithoutmucosalulcerationornecrosisin
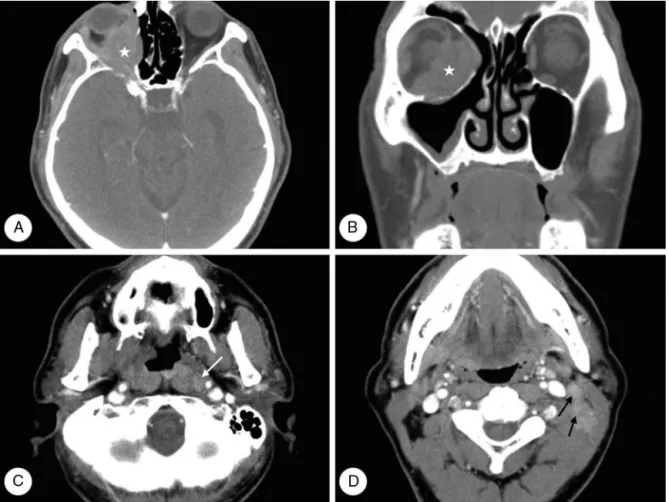
thenasopharynx.NeckCTrevealedasofttissuemassinthe
extraconalandintraconalspaceoftherightorbit.Moreover,
asymmetryof the left nasopharynx andmetastatic lymph
nodeswerepresentintheleftlevelII,III,IV,and
retropha-ryngealareas (Fig.3).On PET/CT scan, the mainmass in
therightorbitwasofahypermetabolicnaturewitha
maxi-mumstandardizeduptakevalue(maxSUV)of3.5.Abnormal
FDGuptakewaspresentinmultipleleftnecklymphnodes,
identical to CT findings. Transnasal endoscopic biopsy, of
the right orbital mass and left nasopharyngeal mucosa,
was performed undergeneral anesthesia. Histopathologic
examination of both specimens revealed undifferentiated
carcinoma(Fig.4).
Thepatient receivedtwocyclesof chemotherapywith
docetaxelandcisplatin.However,herefusedfurther
treat-mentforeconomicreasonsanddiedsixmonthsafterorbital
metastasisdiagnosis.
Discussion
NPC is a tumor that arises from epithelial cells covering
thesurfaceandliningofthenasopharynx.3Threesubtypes
of NPC are recognizedby the World HealthOrganization:
keratinizingSCC, nonkeratinizingcarcinoma, and
undiffer-entiatedcarcinoma.3AlthoughNPCcommonlymetastasizes
tocervical lymphnodes,orbital metastasesarerare.The
majority of orbital involvement cases involvedirect
inva-sion, typically via the pterygopalatine fossa and inferior
orbitalfissure,butoccasionally throughthe ethmoidsinus
and sphenoid sinus, into the apex, causing proptosis and
muscleparalysis.4
Orbitalmetastasisofnasopharyngealcarcinoma 617
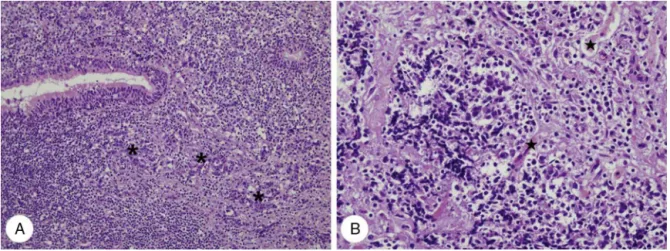
Figure4 Histopathologicfindingsofcase2.(A)Infiltratingundifferentiatednon-keratinizingcarcinoma(*)ofthenasopharynxis notedbeneathnormalciliatedcolumnarpseudostratifiedepithelium(H&E,×200).(B)Nasopharyngealundifferentiatedcarcinoma
infiltratesorbitalsofttissueanddestroysextraocularstriatedmuscles( )(H&E,×400).
Orbital metastatictumors are characterized by rather
abruptonsetofdiplopia,blurredvision,andpain.Avisible
lumpmayalsobepresentbeneaththeeyelidandprogress
isrelativelyrapid.Examinationmaydiscloseproptosis,
dis-placement of the globe, blepharoptosis, and a visible or
palpablemass.1,2 Thefindings inthepresent casesaccord
withprevious reports: orbital metastases becameevident
fivemonthsafter NPCdiagnosis inone patientand
repre-sentedthefirstsignofNPCintheother.
The diagnosisoforbitalmetastasisshouldbesuspected
whenapatientwithahistoryofcancerexhibitsthe
afore-mentionedsymptoms.Ifthepatienthasnohistoryofcancer,
suchfindingsshouldpromptasystemicsurveytodetect a
primaryneoplasm andother sites ofmetastasis. Although
theultimatediagnosisoforbitalmetastasis isrenderedby
biopsyorfine-needleaspiration,CTorMRIorbitalimaging
studiesshouldalsobepreformed.CTistypicallyemployed
firstbecauseitprovidesbetterevaluationofbone.However,
MRIusuallyprovidesthebestresolution fororbital
metas-tasisevaluationbecausethemajorityoforbitalmetastases
principallyaffect orbitalsofttissues.MRItypicallyreveals
aninhomogeneouslowsignalmassonT1images,increased
signalintensityonT2images,andadegreeofenhancement
withcontrastagents.5Inthepresentcases,orbital
metasta-sisfromNPCwascharacterizedbyadiffuseorwell-defined
softtissuemass,withlowsignalintensityonT1WIsand
inter-mediatesignalintensityonT2WIswithmildenhancement.
The main aimduringtreatment oforbital metastasisis
toalleviate sufferingand maintainvisual function.
Radio-therapy is the mainstay treatment for orbital metastasis
fromNPC,due toitssensitivity,but chemotherapyis also
usedincertainpatients.4Ifthetumoriswell-circumscribed
and amenableto complete removal, it should be treated
bycompleteexcisionalbiopsy.1Prognosisisgenerallypoor,
becausepatientsaretypicallyatanadvancedstageof
dis-ease.Theoverallmeansurvivaltimeafterorbitaldiagnosis
is 15 months;1 oneof this report’s patients died after 17
months,theotheraftersixmonths.
Conclusion
Although NPC with orbital metastasis is rare, NPC can
develop metastases in orbital and ocular regions. If NPC
patients complain of ophthalmological symptoms such as
localpain,impairedvision,eyelidswelling,ordiplopia,itis
importanttoconsiderorbitalorocularmetastaticdisease.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Shields JA, Shields CL, Brotman HK, Carvalho C, Perez N, EagleRC Jr. Cancer metastatic tothe orbit: the2000 Robert M. Curts Lecture. Ophthal Plast Reconstr Surg. 2001;17: 346---54.
2.Amemiya T, Hayashida H, Dake Y. Metastatic orbital tumors in Japan: a review of the literature. Ophthal Epidemiol. 2002;9:35---47.
3.Brennan B. Nasopharyngeal carcinoma. Orphanet J Rare Dis. 2006;1:23.
4.ColacoRJ,BettsG,DonneA,SwindellR,YapBK,SykesAJ,etal. Nasopharyngeal carcinoma: a retrospective review of demo-graphics,treatmentandpatientoutcomeinasinglecentre.Clin Oncol(RCollRadiol).2013;25:171---7.