Rev. Nutr. vol.30 número6
Texto
Imagem
Documentos relacionados
O método em forno de microondas pode ser utilizado na preparação de farinha de minhoca por não alterar o teor de proteína da carne de minhoca da espécie
Monthly variation of the fluctuation indexes of environmental variables and the density of the main species (most abundant and frequent species) of cladocerans from a temporary
The aim of our study was to investigate the association of fibrosis stage and inflammatory activity with HCV genotypes and other risk factors in blood donors in the Botucatu
Objective: The aim of the study was to assess the treatment outcome of tuberculosis patients and investigate the association of demographic and clinical factors with treatment
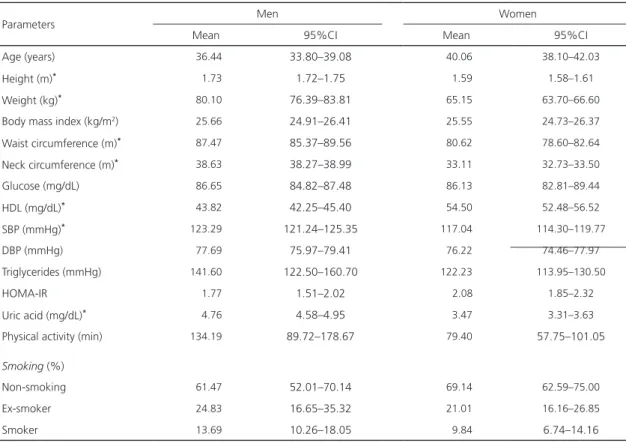
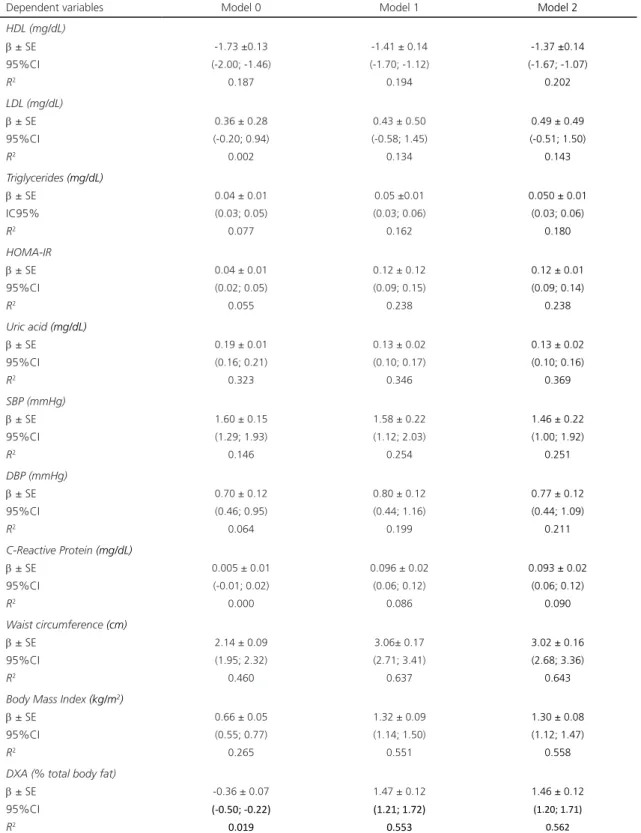
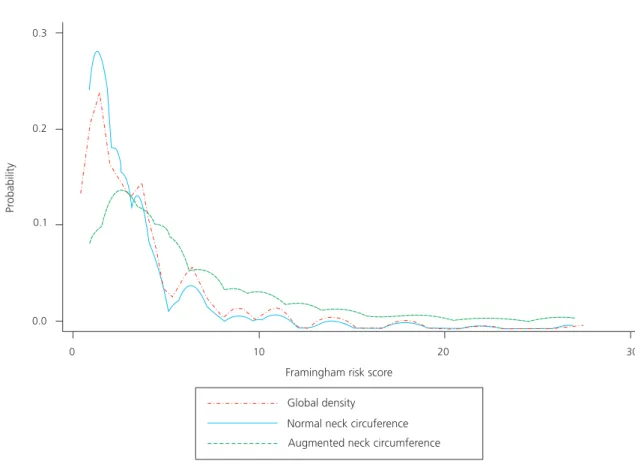
The objective of this investigation was to analyze the association between total fat (BMI) and body fat distribution (waist circumference) anthropometric markers and
The aim of this study was to investigate the prevalence, clustering and associated factors of four major risk factors for non-communicable diseases (smoking, alcohol, physical
hus, the aim of this study was to investigate the association between the four components (body composition, lexibility, muscular strength and cardiorespiratory endurance)
herefore, the aim of this study was to estimate the prevalence of overweight and investigate its association with sociodemographic factors, physical activity
