SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Relationship
of
age
and
type
of
obstetric
brachial
plexus
paralysis
in
forearm
pronosupination
夽
Yussef
Ali
Abdouni
a,∗,
Gabriel
Faria
Checoli
a,
Valdênia
das
Grac¸as
Nascimento
b,
Antonio
Carlos
da
Costa
a,
Ivan
Chakkour
a,
Patricia
Maria
de
Moraes
Barros
Fucs
aaFaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo,DepartamentodeOrtopediaeTraumatologia,SãoPaulo,SP,Brazil
bUniversidadeFederaldoTriânguloMineiro,DepartamentodeOrtopediaeTraumatologia,Uberaba,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received29June2016 Accepted22August2016 Availableonline23August2017
Keywords: Brachialplexus Obstetricparalysis Supination Forearm
a
b
s
t
r
a
c
t
Objective:Toevaluatethearcofforearmpronosupinationofpatientswithsequelaeofbirth paralysisandcorrelatewiththesevariables.
Methods:32childrenagedbetween4and14yearswithtotalorpartiallesionsofthebrachial plexuswereevaluated;measurementsofpronationandsupination,activeandpassive,were made,bothontheinjuredsideandtheunaffectedside.
Results:Astatisticallysignificantdifferencewasobservedbetweentheinjuredsideandthe normalside,buttherewasnodifferencebetweenthegroupsregardingageortypeofinjury. Conclusion:Theageandtypeofinjurydidnot impacton thelimitationoftheforearm pronosupinationinchildrenwithsequelaeofbirthparalysis.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Relac¸ão
entre
a
idade
e
o
tipo
de
paralisia
obstétrica
do
plexo
braquial
com
o
movimento
de
pronossupinac¸ão
do
antebrac¸o
Palavras-chave: Plexobraquial Paralisiaobstétrica Supinac¸ão Antebrac¸o
r
e
s
u
m
o
Objetivo:Avaliaroarcodepronossupinac¸ãodoantebrac¸odospacientescomsequelade paralisiaobstétricadoplexobraquialecorrelacionarcomessasvariáveis.
Métodos:Foramavaliadas32crianc¸asentre4e14anos,comlesõestotaisouparciaisdo plexobraquial,foramtiradasasmedidasdepronac¸ãoesupinac¸ão,ativaepassiva,tantodo ladolesionadoquantodoladonãoafetado.
Resultados:Observou-sediferenc¸aestatisticamentesignificativaentreoladolesionadoeo ladonormal,porémnãohouvediferenc¸aentreosgruposporfaixasetárias,nemquantoao tipodelesão.
夽
PaperdevelopedatHospitaldaIrmandadedaSantaCasadeSãoPaulo,DepartamentodeOrtopediaeTraumatologia,SãoPaulo,SP, Brazil.
∗ Correspondingauthor.
E-mail:[email protected](Y.A.Abdouni).
http://dx.doi.org/10.1016/j.rboe.2017.08.006
Conclusão: Osfatoresidadeetipodelesãonãotiveramefeitosobreapronossupinac¸ãonas crianc¸asportadorasdesequeladeparalisiaobstétricadoplexobraquial.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Brachialplexuslesioninnewbornsoccursduringtheperiodof delivery,andisoftenassociatedwithshoulderdystocia, gesta-tionalorpre-gestationaldiabetes,andmacrosomicfetuses,or evenlow-weightchildrenwithpelvicpresentation.Thefirst clinicaldescriptionoccurredin1764,whenSmelliereported bilateral paralysis in a pelvic newborn. However, the term obstetricparalysiswasattributedtoDuchennein1872.Itis characterizedbyaflaccid paralysis,whichaffects the limb partiallyortotally,dependingonthenumberofrootsinvolved. Theincidenceofobstetricbrachialplexusparalysis(OBPP) intheUnitedStatesis0.38–2.6per onethousandfull-term children,affectingbothgendersequally.Inspiteofadvances inobstetrics,thisincidencehasnotbeenreduced.1
Narakas2classifiedthechildrenwithOBPPintofourgroups: group1withlesionsofonlyC5andC6(extendedErb)roots, group2withinvolvementofC5,C6andC7roots(extended Erb),group3withlesionsofallplexusroots,andgroup4that hastheClaudeBernard-Hornersignassociatedwiththetotal lesion.
MostOBPPpatientshavespontaneousrecovery;itisgreater than 80% in groups 1 and 2.2,3 Normal limb function is expectedifrecoveryoccursinthefirstfouryearsoflife. How-ever,inaconsiderableportion,suchrecoverywillnotoccur.4 Residualparalysisanditssequelaeindailylifeactivitiesare relatedtotheseverityoftheinitialinjury,andmayrangefrom minimallossofupperlimbfunctiontocompleteparalysis.5
Patientswith proximal rootlesions (C5, C6,C7) or with totalbrachialplexuslesions whohad partialrecoverytend to develop a deformity in supination of the forearm over time, due tothe imbalance between the active supination muscles and paralyzed pronator muscles. This imbalance occursbecause thebiceps, innervatedbythe musculocuta-neousnerve,andthesupinator,innervatedbytheradialnerve recover,whilethepronatorsteresandquadratus,innervated bythemediannervedonotusuallyrecover.5–7 Initially,the deformitycanbecorrectedpassively,butwithdevelopment, thedeformity becomesfixeddue tothe contractureofthe interosseous membrane. The hand assumes a position in supinationandhyperextension,aggravatedbythelackofwrist flexors.
Bahm and Gilbert,6 Zancolli,8 Masse,9 Manske et al.,10 amongotherauthors,recommendtendontransfersinthe ini-tialphases,whenthedeformityisnotyetfixed.
Kapandji11 described a progressive radius deformity, in whichitscurvaturewasnotformedduetotheparalysisofthe pronatormusculature,whichfurtherlimitedthepronation.
When a fixed deformity already exists, the pronation osteotomyoftheforearmisusedtoachieveabetter position-ingofthehand,thusconferringgreaterusetotheaffected limb.11–13
Theaimofthisstudywastoevaluatethedegreeof fore-armpronosupinationinchildrenwithOBPPsequelae,andto correlatethedeformitywiththetypeoflesionand theage group.
Material
and
method
ThispaperwasapprovedbytheEthicsCommitteeofthe insti-tutionundernumberCAAE-03724712.1.0000.5479.
Aretrospective cross-sectionalstudy wascarriedout,in which36childrenwithOBPPanduppertrunklesions(C5and C6),upperandmediumtrunk(C5,C6andC7)ortotallesions whohadpartialrecoveryandwhohadnotundergonea sur-gicalprocedureontheforearmwereevaluatedbetweenJuly andDecember2012.Threechildrenwithassociatedcerebral palsy,andonechildwithbilateralbrachialplexuslesionwere excluded.
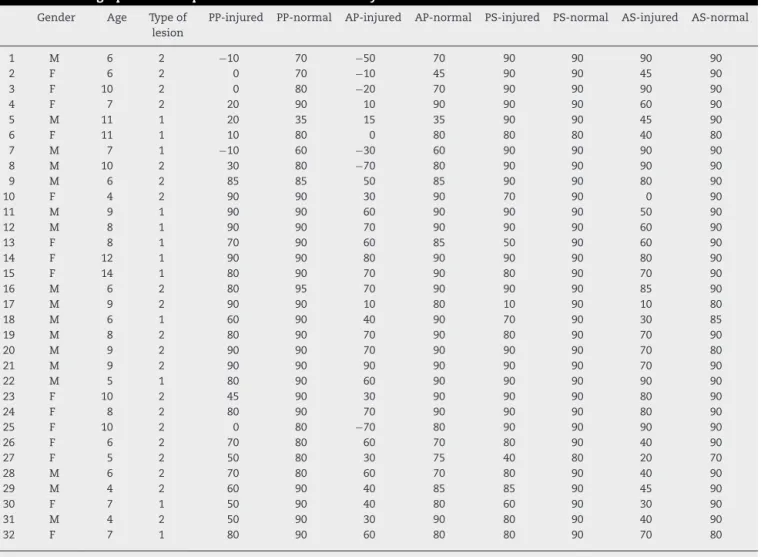
Thepassive(PS)andactive(AS)supination degrees,and passive(PP)andactive(AP)pronationdegreesweremeasured ontheinjuredandnormalsides.Measurementsweretaken whenthechildkepttheshouldernearthetrunk,andwiththe elbowat90degrees;thiswasalwaysperformedbythesame evaluator,withtheaidofagoniometerandexpressedinangle degrees.TheresultsareshowninTable1.
Forstatisticalanalysis,weusedthesoftwareIBM-SPSS (Sta-tisticalPackage forSocialSciences) version17.0, andExcel Office2010.Wecomparedthemeasurementsoftheaffected limbwiththoseofthenormallimb,withtheanatomical clas-sification, and withage.Weused thepaired Studentt test tocomparetheaffectedlimbandthenormallimb measure-ments.Inordertoevaluatewhethertherewasarelationof ageortypeofinjurytothemeasurementsperformedonthe injuredsideofthesechildren,weusedtheAnovatest(Analysis ofvariance).WealsousedtheKruskal–Wallistesttocompare agegroups,andtheMann–Whitneytesttocomparetypesof injury(totalorpartial).Weconsiderp<0.05asstatistical sig-nificant.
Results
Thirty-twochildrenwereselectedforthestudy,18weremale and14female.Regardingtheaffectedside,17hadlesionson therightsideand15ontheleftside.Theagerangedfromfour to14years,withanaverageof7.6.
Table1–Demographicdataofpatientsincludedinthestudy.
Gender Age Typeof lesion
PP-injured PP-normal AP-injured AP-normal PS-injured PS-normal AS-injured AS-normal
1 M 6 2 −10 70 −50 70 90 90 90 90
2 F 6 2 0 70 −10 45 90 90 45 90
3 F 10 2 0 80 −20 70 90 90 90 90
4 F 7 2 20 90 10 90 90 90 60 90
5 M 11 1 20 35 15 35 90 90 45 90
6 F 11 1 10 80 0 80 80 80 40 80
7 M 7 1 −10 60 −30 60 90 90 90 90
8 M 10 2 30 80 −70 80 90 90 90 90
9 M 6 2 85 85 50 85 90 90 80 90
10 F 4 2 90 90 30 90 70 90 0 90
11 M 9 1 90 90 60 90 90 90 50 90
12 M 8 1 90 90 70 90 90 90 60 90
13 F 8 1 70 90 60 85 50 90 60 90
14 F 12 1 90 90 80 90 90 90 80 90
15 F 14 1 80 90 70 90 80 90 70 90
16 M 6 2 80 95 70 90 90 90 85 90
17 M 9 2 90 90 10 80 10 90 10 80
18 M 6 1 60 90 40 90 70 90 30 85
19 M 8 2 80 90 70 90 80 90 70 90
20 M 9 2 90 90 70 90 90 90 70 80
21 M 9 2 90 90 90 90 90 90 70 90
22 M 5 1 80 90 60 90 90 90 90 90
23 F 10 2 45 90 30 90 90 90 80 90
24 F 8 2 80 90 70 90 90 90 80 90
25 F 10 2 0 80 −70 80 90 90 90 90
26 F 6 2 70 80 60 70 80 90 40 90
27 F 5 2 50 80 30 75 40 80 20 70
28 M 6 2 70 80 60 70 80 90 40 90
29 M 4 2 60 90 40 85 85 90 45 90
30 F 7 1 50 90 40 80 60 90 30 90
31 M 4 2 50 90 30 90 80 90 40 90
32 F 7 1 80 90 60 80 80 90 70 80
AP,activepronation;PP,passivepronation;AS,activesupination;SP,passivesupination.
Afterstatisticaltestapplication,astatisticallysignificant
difference was observed between the normal and affected
sidesinallmeasurements(Table2).
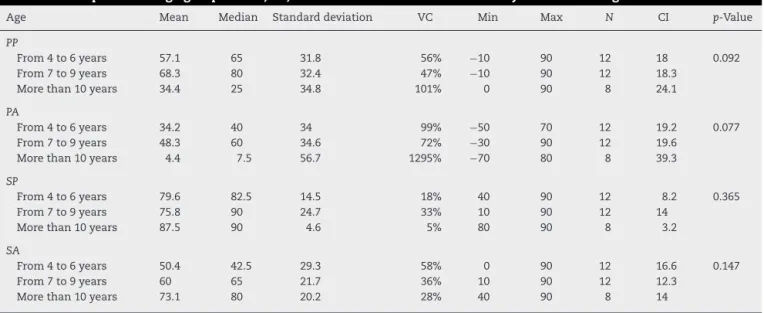
Then, considering only the results on the injured side (Table3)andtheuseofAnova,wecomparedtheagegroups
foreachofthevariables.Wefoundthatthereisnomean dif-ferencebetweenagegroups,thatis,thereisnoeffectofage onPP,AP,PSandASresults.
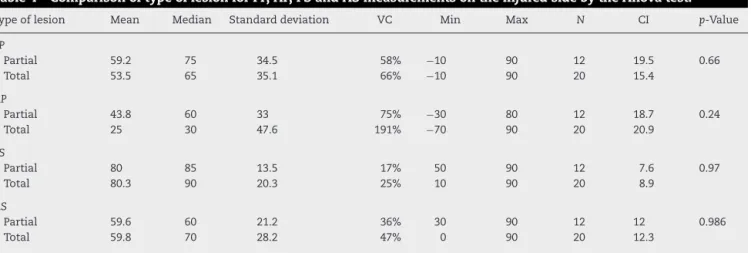
Finally, wecompared the typeof lesions and,similarly, aftertheapplicationofAnova,weconcludedthatthereisno
Table2–AngulationvaluesofthePP,AP,PSandASmovements,measuredinthenormallimbandontheaffectedside ofallpatients.
Mean Median Standard
deviation
VC Min Max N CI p-Value
PP
Injured 55.6 70 34.4 62% −10 90 32 11.9 <0.001
Normal 83.9 90 11.8 14% 35 95 32 4.1
PA
Injured 32 40 43.1 135% −70 90 32 14.9 <0.001
Normal 80.6 85 13.5 17% 35 90 32 4.7
SP
Injured 80.2 90 17.8 22% 10 90 32 6.2 0.005
Normal 89.4 90 2.5 3% 80 90 32 0.9
SA
Injured 59.7 65 25.4 43% 0 90 32 8.8 <0.001
Normal 88 90 4.7 5% 70 90 32 1.6
1 Total lesions (66%) 2 Partial lesions (34%)
Fig.1–Distributionaccordingtothetypeoflesion.
statisticallysignificantmeandifferencebetweenthegroups withpartialandtotallesionsfortheevaluatedvariables.These resultsareexpressedinTable4.
Discussion
OBPPleads toanatomicalalterations inthepatients upper limbs,causingdifficultyindailylifeactivities,besidesesthetic damage.
AlthoughaOBPPsupinationconditionoccursmoreintotal paralyzes,ithasalsobeenobservedinpatientswithC5/C6/C7 paralyzes.In thesecases, withthe biceps impairment,the forearmremainssupinatedduetotheactionofthesupinator muscle.
Yam et al.14 founda supination deformity incidence of 6.9%.Theyalsoobservedthatthisconditionwasnotpresent
8
7
6
5
4
3
2
1
1 2 3 4 5 6 7 8 9 10 11 12 13 14 0
Fig.2–Distributionaccordingtoagegroup.
inpatientsingroupIofNarakas.IntypeII,supination contrac-tureoccurredin5.7%ofpatients,9.6%intypeIIIand23.4%in typeIV.Ourstudydidnotassesstheincidenceofdeformitybut agreeswithYam’sarticlebecauseitdidnotfindthedeformity inNarakasgroupI.However,wedidnotobserveasignificant differencebetweenthelesionsofgroupIIandtotallesions.
BahmandGilbert6andZancolli8affirmthatthedeformity isprogressiveandbecomesfixedwithage.Zancolli8relates thefixeddeformitywithinterosseousmembranecontracture. Inourseries,13patientspresentedpassivepronationthatwas lowerthanorequalto50◦(40.6%),betweenfourand11yearsof age,associatedwithprogressiveretractionoftheinterosseous membrane.
Kapandji11describesthelossofradiuscurvature.Seringue and Dubousset15 describethreestagesofsupination defor-mity,inthethirdstagethereisdislocationoftheradiushead. Inourstudywedidnotobserveanydifferencebetweenthe age groups, there were children with lossof pronosupina-tioninthethreegroups.Therefore,webelievethatthefixed deformitycouldbemorerelatedtothelackofanearly reha-bilitationprogramthantoageitself,sincemanypatientsin ourenvironmentarriveatthespecializedcentersalreadywith the establishedcontracture,withoutundergoing aprevious
Table3–ComparisonofagegroupsforPP,AP,PSandASmeasurementsontheinjuredsidethroughtheAnovatest.
Age Mean Median Standarddeviation VC Min Max N CI p-Value
PP
From4to6years 57.1 65 31.8 56% −10 90 12 18 0.092
From7to9years 68.3 80 32.4 47% −10 90 12 18.3
Morethan10years 34.4 25 34.8 101% 0 90 8 24.1
PA
From4to6years 34.2 40 34 99% −50 70 12 19.2 0.077
From7to9years 48.3 60 34.6 72% −30 90 12 19.6
Morethan10years 4.4 7.5 56.7 1295% −70 80 8 39.3
SP
From4to6years 79.6 82.5 14.5 18% 40 90 12 8.2 0.365
From7to9years 75.8 90 24.7 33% 10 90 12 14
Morethan10years 87.5 90 4.6 5% 80 90 8 3.2
SA
From4to6years 50.4 42.5 29.3 58% 0 90 12 16.6 0.147
From7to9years 60 65 21.7 36% 10 90 12 12.3
Morethan10years 73.1 80 20.2 28% 40 90 8 14
Table4–ComparisonoftypeoflesionforPP,AP,PSandASmeasurementsontheinjuredsidebytheAnovatest.
Typeoflesion Mean Median Standarddeviation VC Min Max N CI p-Value
PP
Partial 59.2 75 34.5 58% −10 90 12 19.5 0.66
Total 53.5 65 35.1 66% −10 90 20 15.4
AP
Partial 43.8 60 33 75% −30 80 12 18.7 0.24
Total 25 30 47.6 191% −70 90 20 20.9
PS
Partial 80 85 13.5 17% 50 90 12 7.6 0.97
Total 80.3 90 20.3 25% 10 90 20 8.9
AS
Partial 59.6 60 21.2 36% 30 90 12 12 0.986
Total 59.8 70 28.2 47% 0 90 20 12.3
VC,variationcoefficient;CI,confidenceinterval;AP,activepronation;PP,passivepronation;AS,activesupination;PS,passivesupination.
rehabilitationtreatment.Inaddition,wealsoobservedsome difficultyforpatientsandtheirrelativesinjoininga
rehabil-itationprogramduetosocioeconomicreasons.Thecommon
characteristicamongourpatientswastheabsenceofaregular physicaltherapytreatment.
Zancolli8 states that a vigorous rehabilitation program, along with the use of a nocturnal orthosis in forearm pronationposition,maypreventinterosseousmembrane con-tracture.Price et al.16 emphasized the role ofmaintaining passivemobilityinthedevelopmentofjointstructuresand, later,Sutcliffe17 statedthattreatmentcould bedone exclu-sively withphysicaltherapy and occupationaltherapy and discard surgery. When relating these observations to the resultsobtainedinthepresentstudy,wereinforceour impres-sionthatrehabilitationwouldplayamoredecisiverolethan ageorleveloflesion.
Despite the decrease in active pronation observed in patients with total lesion compared to those with partial lesion,andinchildreninthegroupabove10yearsinrelation to other age groups, the statistical tests did not indicate a significant difference. These results suggest that these variableswould notbedeterminantforthelossofforearm pronosupination.
Conclusion
We concluded that there were patients with loss of fore-armpronosupinationinallgroupsevaluated.However,this limitationinchildrenwithOBPPsequelaewasnotobserved regardingtheeffectofageandtypeoflesion.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. GilbertA,BrockmanR,CarliozH.Surgicaltreatmentof brachialplexusbirthpalsy.ClinOrthopRelatRes. 1991;(264):39–47.
2.NarakasAO.Obstetricalbrachialplexusinjuries.In:Lamb DW,editor.Theparalysedhand.Edimburgh:Churchill Livingstone;1987.p.116–35.
3.MollbergM,HagbergH,BagerB,LiljaH,LadforsL.High birthweightandshoulderdystocia:thestrongestriskfactors forobstetricalbrachialplexuspalsyinaSwedish
population-basedstudy.ActaObstetGynecolScand. 2005;84(7):654–9.
4.BagerB.Perinatallyacquiredbrachialplexuspalsy–a persistingchallenge.ActaPaediatr.1997;86(11):1214–9.
5.ZafeiriouDI,PsychogiouK.Obstetricalbrachialplexuspalsy. PediatrNeurol.2008;38(4):235–42.
6.BahmJ,GilbertA.Surgicalcorrectionofsupinationdeformity inchildrenwithobstetricbrachialplexuspalsy.JHandSurg Br.2002;27(1):20–3.
7.BrunelliG.Technique:obliqueradialosteotomyfor supinationsyndrome.JHandSurgAm.2004;4(1):50–4.
8.ZancolliEA.Paralyticsupinationcontractureoftheforearm.J BoneJointSurgAm.1967;49(7):1275–84.
9.MasseP.Obstetricalparalysisofthebrachialplexus.II. Therapeutics.Treatmentofsequelae.Surgicalpossibilitiesfor theelbowandthehand.RevChirOrthopReparatriceAppar Mot.1972;58Suppl.1:196–220.
10.ManskePR,McCarrollHRJr,HaleR.Bicepstendonrerouting andpercutaneousosteoclasisinthetreatmentofsupination deformityinobstetricalpalsy.JHandSurgAm.
1980;5(2):153–9.
11.KapandjiIA.Fisiologiaarticular.Membrosuperior.SãoPaulo: Manole;1982.
12.DunhamEA.Obstetricalbrachialplexuspalsy.OrthopNurs. 2003;22(2):106–16.
13.BlountWP.Osteoclasisforsupinationdeformitiesinchildren. JBoneJointSurgAm.1940;22:300–14.
14.YamA,FulliloveS,SinisiM,FoxM.Thesupinationdeformity andassociateddeformitiesoftheupperlimbinseverebirth lesionsofthebrachialplexus.JBoneJointSurgBr.
2009;91(4):511–6.
15.SeringeR,DuboussetJF.Attitudeoftheparalyticsupination oftheforearminchildren.Surgicaltreatmentin19cases.Rev ChirOrthopReparatriceApparMot.1977;63(7):687–99.
16.PriceA,TidwellM,GrossmanJA.Improvingshoulderand elbowfunctioninchildrenwithErb’spalsy.SeminPediatr Neurol.2000;7(1):44–51.