w w w . r b o . o r g . b r
Original
Article
Magnetic
resonance
study
on
the
anatomical
relationship
between
the
posterior
proximal
region
of
the
tibia
and
the
popliteal
artery
夽
Rogério
Franco
de
Araujo
Goes
a,∗,
Augusto
Cardoso
Filho
a,
Gabriel
Novaes
Pillar
de
Oliveira
Castro
a,
Fabricio
Bolpato
Loures
a,
Idemar
Monteiro
Da
Palma
b,
André
Kinder
c,
Pedro
José
Labronici
aa“Prof.Dr.DonatoD’Ângelo”OrthopedicsandTraumatologyService,HospitalSantaTeresa,Petrópolis,RJ,Brazil bKneeGroup,InstitutoNacionaldeTraumatologiaeOrtopedia(INTO),RiodeJaneiro,RJ,Brazil
cUniversidadeFederaldoRiodeJaneiro,RiodeJaneiro,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received19January2014 Accepted29July2014 Availableonline30July2015
Keywords:
Knee
Magneticresonance Poplitealartery Anatomy
a
b
s
t
r
a
c
t
Objective:Toanalyzeanddescribethedistancefromthepoplitealarterytothreespecific areasoftheproximalregionofthetibia,withthekneeextended,bymeansofmagnetic resonance.
Methods:Imagesof100kneesofpatientswhounderwentmagneticresonanceexaminations wereanalyzed.Thelocationofthepoplitealarterywasmeasuredinthreedifferentareasof theposteriorproximalregionofthetibia.Thefirstmeasurementwasmadeatthelevelof thekneejoint(tibialplateau).Thesecondwas9mmdistallytothetibialplateau.Thethird wasattheleveloftheanteriortuberosityofthetibia(ATT).
Results:ThedistancesbetweenthepoplitealarteryandthetibialplateauandATTregion weresignificantlygreaterinmalesthaninfemales.Thedistancesbetweenthepopliteal arteryandtheregions9mmdistallytothetibialplateauandtheATTweresignificantly greaterintheagegroupover36yearsthaninthegroup≤36years.
Conclusion:Knowledgeoftheanatomicalpositionofthepoplitealartery,asdemonstrated throughmagneticresonancestudies,isofgreatrelevanceinplanningsurgicalprocedures thatinvolvethekneejoint.Inthismanner,devastatingiatrogenicinjuriescanbeavoided, particularlyinregionsthatareproximaltothetibialplateauandinyoungpatients.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
Workperformedinthe“Prof.Dr.DonatoD’Ângelo”OrthopedicsandTraumatologyService,HospitalSantaTeresa,Petrópolis,RJ,and theFaculdadedeMedicinadePetrópolis,Petrópolis,RJ,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](R.F.deAraujoGoes).
http://dx.doi.org/10.1016/j.rboe.2015.07.005
Estudo
por
ressonância
magnética
da
relac¸ão
anatômica
entre
a
região
proximal
posterior
da
tíbia
e
a
artéria
poplítea
Palavras-chave:
Joelho
Ressonânciamagnética Artériapoplítea Anatomia
r
e
s
u
m
o
Objetivo:Analisaredescrever,comojoelhoemextensão,adistânciadaartériapoplíteaem trêsáreasespecíficasdaregiãoproximaldatíbia,pormeioderessonânciamagnética.
Métodos:Foramanalisadasasimagensde100joelhosdepacientessubmetidosaexamepor ressonânciamagnética.Alocalizac¸ãodaartériapoplíteafoimedidaemtrêsáreasdistintas daregiãoproximalposteriordatíbia.Aprimeiramedidafoifeitanoníveldaarticulac¸ão dojoelho(platôtibial).Asegunda,a9mm distaldoplatôtibial.Aterceira,aonívelda tuberosidadeanteriordatíbia(TAT).
Resultados: AsdistânciasentreaartériapoplíteaeoplatôtibialearegiãodaTATforam significativamentemaioresnosexomasculinodoquenofeminino.Asdistânciasentre aartériapoplíteaearegião9mmdistaldoplatôtibialeaTATforamsignificativamente maioresnafaixaacimade36anosdoquenafaixa≤36anos.
Conclusão: Oconhecimentodaposic¸ãoanatômicada artériapoplítea,demonstradapor estudosdeRM,édegranderelevâncianoplanejamentodeprocedimentoscirúrgicosque envolvamaarticulac¸ãodojoelho.Comisso,podem-seevitarlesõesiatrogênicas devasta-doras,principalmenteemregiõesproximaisaoplatôtibialeempacientesjovens.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Posterior neurovascular structures of the proximal region ofthetibia canbeinjured duringsurgical procedures.The chancesthatiatrogenicinjuriestothepoplitealarterymight occur, with formation of pseudoaneurysm, may be up to around 37.5%.1 Vascular complicationshave been reported in procedures such as arthroscopic surgery, upper tibial osteotomy,osteotomyattheleveloftheanteriortuberosityof thetibia(ATT)andfixationoffracturesofthetibialplateau.2–6 Althoughrare, vascular injury is one ofthe complications thatmaycompromisetheresultsfromtotalkneearthroplasty (TKA).7–18Itsincidenceisapproximately0.2%.19–21Theriskof vascularinjuryisgreateramongpatientswithprevious vascu-larinsufficiency.22–25DirectlacerationofthearteryduringTKA isalsorare.12,18,26Thisinjuryhasalsobeendescribedduring reconstructionofanteriorandposteriorcruciateligaments,27 andalsoduringmeniscectomythrougharthroscopy.28
In normal anatomical situations, the popliteal artery is located laterally to the intercondylar fossa and passes obliquely along the medial border of the popliteal mus-cle,whereit dividesin tothe anterior and posterior tibial arteries.6,21,22Theinferiorlateralgeniculararteryoriginates 1–2cmbelowthejointlineandcirclesthetibiadeeply.The inferiormedialgeniculararteryoriginatesposteriorlybetween thesoleusmuscleandthelateralheadofthegastrocnemius.6 Severalauthorshaveidentifiedthelocationofthepopliteal arteryinkneeswithosteoarthrosisorinthekneesof cadav-ers,usingmagneticresonanceimaging(MRI),arteriographyor ultrasonography.23–28
Theobjectiveofthepresentstudywastoanalyzethe dis-tancetothepoplitealarterywiththekneeextended,inthree specificareasoftheproximalregionofthetibia,bymeansof
MRI,andtocomparetheresultsbetweenpatientsoverand under36yearsofage.
Materials
and
methods
BetweenMayandAugust2012,thepositioningofthepopliteal arteryin100kneesofpatientsundergoingMRIexaminations wasretrospectivelyanalyzed.All theimageswereobtained withthe knee completelyextended.Theimageswere cho-senbyexcludingpatientswhopresentedhistoriesoffractures, tumorsordeformitiesoftheknee,orprevioussurgical proce-dures.PatientswhoseMRIpresentedanysoft-tissueorbone abnormalities intheproximal regionofthetibia werealso excluded.
The MRI examinations were performed using a 1.5T machine (Magneton Essenza®, Siemens, Germany), with the patient in dorsal decubitus and the knee joint com-pletely extended. The following sequences were obtained: T1-weighted sagittal sequence with repetitiontime (RT)of 540ms,echotime(ET) of13ms, thicknessof4mm,fieldof view(FOV)of160/160mmandmatrixof230/7384;andproton density-weightedwithfatsuppressionintheaxialplane(RT 3920,ET35,thickness3mm,FOV160/160andmatrix192/320), sagittalplane(RT2800,ET35,thickness4,FOV160/160and matrix230/320)andcoronalplane(RT2550,ET:32,thickness 3.5,FOV160/160andmatrix224/320).
Level of the ATT and at 9 mm from the joint on the tibial plateau
Fig.1–Locationofthedistancemeasurementsbetweenthe poplitealarteryandtheposteriortibialcortex,atthelevel oftheATTandat9mmfromthejointonthetibialplateau.
TKA.Thethirdwasmadeattheleveloftheanterior tuberos-ityofthetibia(ATT),whereproximalosteotomyofthetibiais performed.
ThemeasurementswereobtainedbymeansofMRI,onTI sagittalsliceswiththekneecompletelyextended.Atalllevels, theposteriorcortexoftheproximalregionofthetibiaandthe anteriorwallofthepoplitealarterywereusedasreferences (Fig.1).
Characterization
of
the
sample
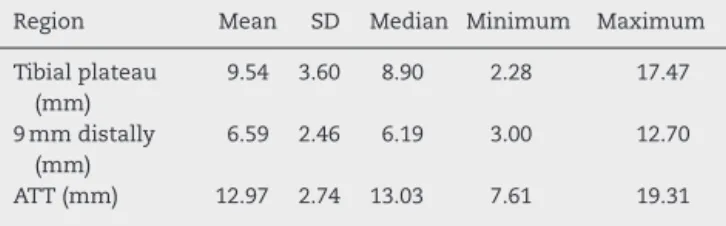
Table1presentsadescriptiveanalysisonthestudysample
of100knees,regardingthe distances(in mm)inthe three
Table1–Descriptionofthedistancesinthethree regions,inthesampleof100knees.
Region Mean SD Median Minimum Maximum
Tibialplateau (mm)
9.54 3.60 8.90 2.28 17.47
9mmdistally (mm)
6.59 2.46 6.19 3.00 12.70
ATT(mm) 12.97 2.74 13.03 7.61 19.31
Source:Hospitalservicefiles.
SD,standarddeviation.
regions,whichweredefinedthus:thetibialplateauatthelevel ofthejointinterline;9mmdistallytothetibialplateau;and attheleveloftheATT.
Statistical
analysis
Thedescriptiveanalysispresentedtheobserveddatainthe formoftables,expressedusingmeans,standarddeviations andmedians,alongwithillustrativegraphs.
The inferential analysiswas composed ofthe following methods:
- Numericalvariableswerecomparedbetweenpairsof sub-groupsusingtheMann–Whitneytest;and
- Spearman’scorrelationcoefficient(rs)wasusedtomeasure thedegreeofassociationbetweenthe distance measure-mentsanalyzed,i.e.betweenpairsofnumericalvariables. Itcanrangefrom −1to1.Thecloseritisto1or−1,the strongertheassociationis;andthecloseritistozero,the weakertherelationshipbetweenthetwovariablesis.
Non-parametricmethodswereused,becausethevariables didnotpresentnormal(Gaussian)distribution,giventhewide dispersion of the data and rejection of the hypothesis of normalityaccordingtotheKolmogorov–Smirnovtest.The cri-terionusedfordeterminingsignificancewasthelevelof5%. ThestatisticalanalysiswasprocessedusingtheSAS6.11 com-putersoftware(SASInstitute,Inc.,Cary,NC,USA).
Results
Thefirstobjectivewastoascertainwhethertherewereany significantdifferencesinthedistancesbetweenthepopliteal arteryandthethreeregions(tibialplateau,9mdistallytothe tibialplateauandATT)inthestudysampleof100knees,with regardtosexandagegroup.Tables2and3presentthemean, standarddeviation(SD)andmedianofthedistancestothe threeregions,accordingtosexandagegroup(≤36yearsand >36years),respectively,andthecorrespondingdescriptive lev-elsfromtheMann–Whitneytest.
Itwas observedthatthe distancebetweenthepopliteal arteryandthe posteriortibialcortexatthelevelofthe tib-ial plateau (p=0.037)and atthe level ofthe ATT(p=0.016) wassignificantlygreateramongmalesthanamongfemales. Therewasnosignificantdifference(atthe5%level)inthat dis-tance,intheregion9mmdistallytothetibialplateau(p=0.46) betweenthesexes.
It was demonstrated that the distances between the poplitealarteryandtheposteriortibialcortexintheregion 9mmdistallytothetibialplateau(p=0.006)andattheATT level(p=0.005)weresignificantlygreaterintheagegroupover 36yearsthaninthegroup≤36years.Therewasnosignificant difference(atthe5%level)inthedistanceintheregionofthe tibialplateau(p=0.14)betweentheagegroups.
Table2–Analysisonthedistancesfromthethreeregionsaccordingtosex.
Variable Male(n=56) Female(n=44) pvaluea
Mean±SD Median Mean±SD Median
Distance
Age(years) 37.3±15.2 34 44.0±19.2 43 0.078
Tibialplateau(mm) 10.1±3.5 10.1 8.8±3.6 8.1 0.037
9mmdistally(mm) 6.7±2.4 6.5 6.4±2.5 5.8 0.46
ATT(mm) 13.5±2.5 13.7 12.3±2.9 12.5 0.016
Source:Hospitalservicefiles.
SD,standarddeviation.
a Mann–Whitneytest.
Table3–Analysisonthedistancesfromthethreeregionsaccordingtoagegroup.
Variable ≤36years(n=47) >36years(n=53) pvaluea
Mean±SD Median Mean±SD Median
Distance
Tibialplateau(mm) 9.0±3.6 8.6 10.1±3.6 9.0 0.14
9mmdistally(mm) 5.9±2.2 5.6 7.2±2.5 6.8 0.006
ATT(mm) 12.1±2.6 12.4 13.8±2.6 13.3 0.005
Source:Hospitalservicefiles.
SD,standarddeviation.
a Mann–Whitneytest.
Thefollowingwasobserved:
- Thedistancebetweenthepoplitealarteryandthe poste-rior tibialcortexinthe region9mmdistally tothe tibial plateaupresentedasignificantdirectcorrelationwithage, inyears(rs=0.238;p=0.017),althoughthiscorrelationwas
oflowstrength;
- Thedistancebetweenthepoplitealarteryandtheposterior tibialcortexintheregionoftheATTpresenteda signifi-cantdirectcorrelationwithage,inyears(rs=0.258;p=0.017),
althoughthiscorrelationtoowasoflowstrength;and - Thedistancebetweenthepoplitealarteryandtheposterior
tibialcortexintheregionofthetibialplateaudidnotpresent anysignificantcorrelationatthe5%levelwithageinyears (p=0.13).
Table4–Correlationbetweenthedistancesfromthe threeregions.
Distancefromtheregion
Tibialplateau 9mmdistally ATT
Age(years) rs 0.151 0.238 0.258 p 0.13 0.017 0.010 9mmdistally(cm) rs 0.770
p 0.0001
ATT(cm) rs 0.365 0.523 p 0.0002 0.0001
Source:Hospitalservicefiles.
rs,Spearmancorrelationcoefficient;p,descriptivelevel.
Figs.2and3illustratethecorrelationofagewiththe
dis-tances betweenthe poplitealarteryand theposteriortibial cortexintheregions9mmdistallytothetibialplateauandat theleveloftheATT,respectively.
Thefollowingwasobserved:
- Thedistancebetweenthepoplitealarteryandthe poste-riortibial cortexinthe region9mmdistallytothe tibial plateaupresentedasignificantdirectcorrelation(rs=0.770;
p=0.0001);
- The distance between the popliteal artery and the pos-terior tibial cortex in the region of the tibial plateau presentedasignificantdirectcorrelationwiththeATT dis-tance (rs=0.365; p=0.0002), although this correlation too
wasoflowstrength;and
y = 0.0309x + 5.3443 R = 0.0472²
Distance from the regio
n 9 mm distally to the
tibial plateau (cm)
Age (years)
y = 0.0465x + 11.093 R² = 0.0867
Distance from the ATT region (cm)
Age (years)
Fig.3–Agedispersionaccordingtodistancefromthe poplitealarterytotheposteriortibialcortexintheATT region.
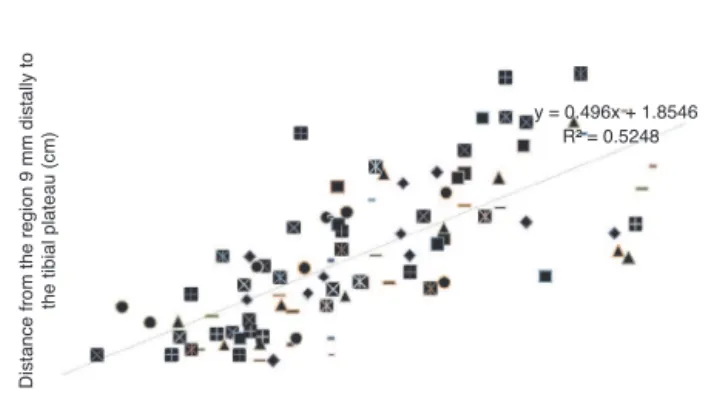
y = 0.496x + 1.8546 R² = 0.5248
Distance from the region 9 mm distally to
the tibial plateau (cm)
Distance between the popliteal artery and the posterior tibial cortex in the region of the tibial plateau (cm)
Fig.4–Dispersionofthedistancesbetweentheregion 9mmdistallytothetibialplateauandthelevelofthetibial plateau.
- Thedistancebetweenthepoplitealarteryandtheposterior tibialcortexintheregion9mmdistallytothetibialplateau presentedasignificantdirectcorrelationwiththedistance intheATTregion(rs=0.523;p=0.0001).
Figs.4–6illustratethecorrelationsbetweenthedistance
measurementsintheregionsstudied.
y = 0.2548x + 10.535 R² = 0.1121
Distance from the ATT region (cm) Distance between the popliteal artery and the posterior tibial cortex in the region of the tibial plateau (cm)
Fig.5–Dispersionofthedistancesbetweenthedistal regionandthetibialplateauandATT.
y = 0.6208x + 8.8768 R² = 0.3119
Distance from the ATT region (cm) Distance between the popliteal artery and the posterior
tibial cortex in the region of the tibial plateau (cm)
Fig.6–Dispersionofthedistancesbetweentheregion 9mmdistallytothetibialplateauandtheregionattheATT level.
Discussion
Thepoplitealarteryisthemostanteriorstructureofthe neu-rovascularbundleoftheposteriorregionoftheknee.Itisa fixedstructureandisclosesttothejointintheregionofthe insertionoftheposteriorcruciateligament,neartothefibrous arcadeofthesoleusmuscle.29
Insurgeryinvolvingtheproximalregionofthetibia, iatro-genic injuriestothe posteriorneurovascular structuresare devastatingandmayputthelimbatrisk.30Thisdangerzone islocatedslightlylaterallytotheintercondylarfossa.
Small31 reportedon12 casesofvascular injuries,which represented0.54%ofallcomplicationsinthecaseseries.There wereninecasesofdirecttraumatothepoplitealartery,one of displacement of the fibrous arcade and twoof nonspe-cificinjuries.Tawesetal.32reportedonthreecasesinwhich thepoplitealarterywasinjuredduringarthroscopic menis-cectomy butthiswasdiagnosedonlylateron,whichledto amputation. Morethan 50%ofthepatientswithinjuriesto thepoplitealarterypresentdeficientcirculation,despite pre-sentingapalpabledistalpulse.33
femalepatients.Thismeansthatevengreatercareneedsto betakenwhenproceduresareperformedonfemalepatients. Paceand Wahl34 analyzedkneesfrom cadaversinorder tostudytheposteriorregionofthekneeandobservedthat themeanageofthespecimensstudiedwas70years. How-ever,theyreported thattheydidnotknowhow thismight change the anatomical relationships, in comparison with youngindividuals.Ourstudycorrelatedthedistancesbetween thepoplitealartery and theposterior tibialcortexin three anatomicalregionsofthekneejointwiththepatients’ages. Using a cutoffline of36 years,the distancesbetween the poplitealarteryandtheposteriortibialcortexintheregions 9mmdistallytothetibialplateauandattheleveloftheATT showed thatthe greater the patient’s age was, the greater thisdistancewasrs=0.258;p=0.017;andrs=0.238;p=0.017,
respectively.
Several studies have reported occurrences of iatrogenic neurovascularinjuriesin thepoplitealfossa during arthro-scopicreconstructionoftheposteriorcruciateligament(PCL), which may have been caused by aguidewire or by adrill bit.35,36 Matava et al.37 analyzed 14 knees from cadavers andshowedthatthepoplitealarterywaslocatedposteriorly and laterally to the insertion of the PCL and anteriorly to thepoplitealvein and sciaticnerve, inall the kneeswhen extended(0◦ or 180◦)and whenflexedat45◦, 60◦ and 90◦.
Keseretal.23reportedthatatthelevelofthekneejoint,the poplitealarterywaslocatedposteriorlytotheinsertionofthe PCLin19cases(5.7%).Thislocationmaycauseinjurytothe poplitealarteryincasesofrepairtoorexcisionofthe poste-riorcornuofthelateralmeniscus,andalsoinproceduresfor PCLreconstruction.Ahnetal.38performedarthroscopicPCL reconstructionwithslightreleaseoftheposteriorcapsuleat thelevelofitsinsertion.Usingangiography,theymeasured thedistancebetweenthetibialinsertionofthePCLandthe poplitealarterybeforeandaftercapsulerelease.Theyfound thatthedistancefromthemidpointofthePCLtothepopliteal arterybecamesignificantlygreateraftercapsulerelease:from 4.4±3.2mmto14.7±4.1mm.Cosgareaetal.39analyzedknees fromcadaversandobservedthatthemeandistancefromthe midpointofthePCLtothepoplitealarterywas29.1±11mm (rangefrom 18 to55mm).Pace and Wahl34 found thatthe meandistancefromthePCLtothepoplitealarterywas19mm, withthekneeflexedat90◦atthelevelofthejointline.Inthe
presentstudy,themeansobtainedfromMRIshowedthatat theleveloftheknee joint,themeandistancebetweenthe poplitealarteryandtheposteriortibialcortexwas9.54mm (rangefrom2.80 to17.47mm). Itwas alsoobservedthat in relationtosex,thisdistanceatthelevelofthetibialplateau wassignificantlygreateramongmalesthanamongfemales (10.1±3.5mmand8.8±3.6mm,respectively).
Theincidenceofvascularinjuryaftertotalknee arthro-plasty (TKA) is fortunately minimal (estimated at around 0.2%).9,40 In the present study, the distance between the poplitealarteryandtheposteriortibialcortexwasanalyzed intheregion9mmdistallytothetibialplateau,whichisthe locationwhere,onaverage,thecutforplacementofthe tib-ialcomponentismadeinTKAprocedures.Ninomiyaetal.41 conductedastudyoncadaversbymeansofMRI,inorderto investigatethemechanismforpoplitealarteryinjuryduring TKA,andobservedthat this arterywaslocatedlaterally to
thetibialplateauin95%ofthespecimens.Proximitytothe posteriorjointcapsulemakesthearterysusceptibletoinjury duringTKA. Takedaet al.42 emphasizedthe importanceof greater caseinpositioningseparators,withuseofan oscil-latorysawandosteotomesintheposteriorregionoftheknee duringTKA.Theyobservedthatalongthearcofkneeflexion, thepositioningofthepoplitealarteryvariedamong individ-ualswhohadundergoneTKA.Mureebeetal.43reportedtwo casesofpatientswhopresentedinjuriestothepoplitealartery afterTKAandrequiredarteryreconstructionsurgerytosave thelimb.OurstudydemonstratedthroughMRIthatthemean distancebetweenthepoplitealarteryandtheposterior tib-ialcortexintheregion9mmdistallytothetibialplateauwas 6.59mm(rangefrom3to12.70).Thiswasthelocationatwhich thearterywasclosesttotheposteriortibialcortex.Wedidnot find anysignificant differencebetweenthe sexesregarding thedistancesmeasuredbetweenthepoplitealarteryandthe posterior tibialcortex inthe threeregions ofthe proximal tibiathatwereevaluated.However,inrelationtoagegroup, thedistancebetweenthepoplitealarteryand theposterior tibialcortexintheregion9mmdistallytothetibialplateau wassignificantlygreaterintheagegroupover36years.This means thatthegreaterthepatient’sagewas(p=0.006),the greaterthedistancebetweenthepoplitealarteryandthe pos-teriortibialcortex(age≤36years,5.9±2.2mmand>36years, 7.2±2.5mm).
Althoughrare,injurytothepoplitealarteryduring prox-imal osteotomy of the tibia at the level of the anterior tuberositymayhavedevastatingconsequences.Osteotomyof thetibialtuberosity,whichinvolvesviolationoftheposterior tibialcortexusingdrillbitsandscrews,maygiverisetoinjury tothepoplitealartery.44Onlyafewstudiesintheliterature havedemonstrateddirectinjurytothepoplitealarteryduring proximalosteotomyofthetibia.6,45 Zaidietal.6studiedthe positioningofthepoplitealarteryin20knees,bymeansof duplexultrasonographyattheleveloftheregioninwhichthe proximalosteotomywouldbeperformed.In12knees(60%), thearterywaslocatedclosetothetibia,withthekneeflexed at90◦. Somestudieshaveshownthepresenceof
pseudoa-neurysm subsequent to proximal tibial isteotomy.46,47 Kim et al.48 reportedthatthe poplitealarterybecameseparated fromtheposteriortibialcortexwhenthekneewasflexedat 90◦.However,whentheangleoftheosteotomycutwasgreater
than30◦,inthecoronalplane,itwasseenthattherecouldbea
riskofinjurytoneurovascularstructures.Smithetal.24 stud-iedninevolunteersbymeansofMRI,withthekneecompletely extendedandflexedat90◦,anddemonstratedthatevenwith
thekneeflexedat90◦,thisdidnotmeanthatthepopliteal
distantfromtheposteriortibialcortexthepoplitealarterywas located.
Thegreatestlimitationofourstudywasthatthe measure-mentsonthethreeregionsofthekneewereonlyascertained withtheknee extended.There ismajorcontroversyinthe literature regardingthe extent to which knee flexion may increase the distance between the popliteal neurovascular structuresandtheposteriortibialcortex.Someauthorshave arguedthatinallregionsoftheknee,thedistancebetweenthe poplitealarteryandtheposteriortibialcortexwouldincrease with the knee flexed. However, other authors have main-tainedthatevenwiththekneeflexed,therewouldnotbeany changedinthe distanceintheregion9mmfromthe tibial plateau(TKAlevel)oratthelevelofvalgusosteotomyofthe tibia.6,26,28,30
Conclusion
Knowledgeoftheanatomicalpositionofthepoplitealartery, asdemonstratedthroughMRI,isofgreatrelevancein plan-ningsurgicalproceduresthatinvolvethekneejoint.Through this,devastatingiatrogenicinjuriescanbeavoided.Thus, pro-ceduresclosertothetibialplateaubecomemoredangerous, particularlyinyoungpatients.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. MegalopoulosA,SiminasS,TrelopoulosG.Traumatic
pseudoaneurysmofthepoplitealarteryafterblunttrauma:
casereportandareviewoftheliterature.VascEndovascular
Surg.2006;40(6):499–504.
2. HanKJ,WonYY,KhangSY.Pseudaneurysmaftertibial
nailing.ClinOrthopRelatRes.2004;(418):209–12.
3. KarkosCD,ThomsonGJ,D’SouzaSP,PrasadV.Falseaneurysm
ofthepoplitealartery:ararecomplicationoftotalknee
replacement.KneeSurgSportsTraumatolArthrosc.
2000;8(1):53–5.
4. RubensF,WellingtonJL,BouchardAG.Poplitealarteryinjury
aftertibialosteotomy:areportoftwocases.CanJSurg.
1990;33(4):294–7.
5. YooJH,ChangCB,LeeTS,SeongSC,KimTK.Delayed
recurrenthemarthrosisafterstaplefixationoftibialavulsion
fractureoftheposteriorcruciateligament:acasereport.
KneeSurgSportsTraumatolArthrosc.2006;14(9):854–8.
6. ZaidiSH,CobbAG,BentleyG.Dangertothepoplitealarteryin
hightibialosteotomy.JBoneJointSurgBr.1995;77(3):384–6.
7. AustJC,BredenbergCE,MurrayDG.Mechanismsofarterial
injuriesassociatedwithtotalhipreplacement.ArchSurg.
1981;116(3):345–9.
8. BergerC,AnzbockW,LangeA,WinklerH,KleinG,EngelA.
Arterialocclusionaftertotalkneearthroplasty:successful
managementofanuncommoncomplicationbypercutaneous
thrombusaspiration.JArthroplasty.2002;17(2):227–9.
9. CalligaroKD,DelaurentisDA,BoothRE,RothmanRH,
SavareseRP,DoughertyMJ.Acutearterialthrombosis
associatedwithtotalkneearthroplasty.JVascSurg.
1994;20(6):927–32.
10.DoiS,MotoyamaY,ItohH.Externaliliacveininjuryduring
totalhiparthroplastyresultingindelayedshock.BrJ
Anaesth.2005;94(6):866-L869.
11.LewallenDG.Neurovascularinjuryassociatedwithhip
arthroplasty.InstrCourseLect.1998;47:275–83.
12.ShoenfeldNA,StuchinSA,PearlR,HavesonS.The
managementofvascularinjuriesassociatedwithtotalhip
arthroplasty.JVascSurg.1990;11(4):549–55.
13.CalligaroKD,DoughertyMJ,RyanS,BoothRE.Acutearterial
complicationsassociatedwithtotalhipandknee
arthroplasty.JVascSurg.2003;38(6):1170–7.
14.NachburB,MeyerRP,VerkkalaK,ZürcherR.Themechanisms
ofseverearterialinjuryinsurgeryofthehipjoint.Clin
OrthopRelatRes.1979;(141):122–33.
15.RandJA.Vascularcomplicationsoftotalkneearthroplasty.
Reportofthreecases.JArthroplasty.1987;2(2):89–93.
16.BarrackRL,ButlerRA.Avoidanceandmanagementof
neurovascularinjuriesintotalhiparthroplasty.InstrCourse
Lect.2003;52:267–74.
17.BarrackRL.Neurovascularinjury:avoidingcatastrophe.J
Arthroplasty.2004;194Suppl.1:104-L107.
18.SmithDE,McGrawRW,TaylorDC,MasriBA.Arterial
complicationsandtotalkneearthroplasty.JAmAcadOrthop
Surg.2001;9(4):253–7.
19.RothJH,BrayRC.Poplietalarteryinjuryduringanterior
cruciantligamentreconstruction:briefreport.JBoneJoint
SurgBr.1988;70(5):840–5.
20.PotterD,Morris-JonesW.Poplitealarteryinjurycomplicating
arthroscopicmeniscectomy.Arthroscopy.1995;11(6):
723–6.
21.WilliamsPL,WarwickR,editors.Gray’sanatomy.Edinburgh:
ChurchillLivingstone;1980.
22.McMinnRM,editor.Last’sanatomy.Regionalandapplied.8th
edEdinburgh:ChurchillLivingstone;1990.
23.KeserS,SavranlarA,BayarA,UlukentSC,OzerT,TuncayI.
Anatomiclocalizationofthepoplitealarteryatthelevelof
thekneejoint:amagneticresonanceimagingstudy.
Arthroscopy.2006;22(6):656–9.
24.SmithPN,GelinasJ,KennedyK,ThainL,RorabeckCH,Bourne
RB.Popliealvesselsinkneesurgery.Amagneticresonance
imagingstudy.ClinOrthopRelatRes.1999;(367):158–64.
25.VernonP,DelattreJF,JohnsonEJ,PalotJP,ClémentC.Dynamic
modificationsofthepoplitealarterialaxisinthesagittal
planeduringflexionoftheknee.SurgRadiolAnat.
1987;9(1):37–41.
26.FarringtonWJ,CharnleyGJ,HarriesSR,FoxBM,SharpR,
HughesPM.Thepositionofthepoplitealarteryinthe
arthriticknee.JArthroplasty.1999;14(7):800–2.
27.ShettyAA,TindallAJ,QureshiF,DivekarM,FernandoKW.
Theeffectofkneeflexiononthepoplitealarteryandits
surgicalsignificance.JBoneJointSurgBr.2003;85(2):218–22.
28.CoventryMB.Osteotomyaboutthekneefordegenerativeand
rheumatoidarthritis.JBoneJointSurgAm.1973;55(1):23–48.
29.KramerD,BahkM,CascioB,CosgareaAJ.Posteriorknee
arthroscopy:anatomy,technique,application.JBoneJoint
SurgAm.2006;88Suppl.4:110–21.
30.YangD,ZhouY,TangQ,XuH,YangX.Anatomical
relationshipbetweentheproximaltibiaandposterior
neurovascularstructures:asafezoneforsurgeriesinvolving
theproximaltibia.JArthroplasty.2011;26(7):1123–7.
31.SmallNC.Complicationsinarthroscopy:thekneeandother
joints.Arthroscopy.1986;2(4):253–8.
32.TawesRL,EtheridgeSN,WebbRL,EnloeLJ,StalloneRJ.
Poplitealarteryinjurycomplicatingarthroscopic
meniscectomy.AmJSurg.1988;156(2):136–8.
33.DeLeeJC.Complicationsofarthroscopyandarthroscopic
surgery:resultsofanationalsurvey.Arthroscopy.
34.PaceJ,WahlC.Arthroscopyoftheposteriorknee
compartments:neurovascularanatomicrelationshipsduring
arthroscopictransversecapsulotomy.Arthroscopy.
2010;26(5):637–42.
35.DunnPM,PostRH,JonesSR.Thromboemboliccomplications
ofkneearthroscopy.WestJMed.1984;140(2):291.
36.SimpsonLA,BarrettJP.Factsassociatedwithpoorresults
followingarthroscopicsubcutaneouslateralrelease.Clin
OrthopRelatRes.1984;(186):165–71.
37.MatavaMJ,SethiNS,TottyWG.Proximityofthe
posteriorcruciateligamentinsertiontothepoplitealarteryas
afunctionofthekneeflexionangle:implicationsfor
posteriorcruciateligamentreconstruction.Arthroscopy.
2000;16(8):796–804.
38.AhnJH,WangJH,LeeSH,YooJC,JeonWJ.Increasingthe
distancebetweentheposteriorcruciateligamentandthe
poplitealneurovascularbundlebyalimitedposterior
capsularreleaseduringarthroscopictranstibialposterior
cruciateligamentreconstruction:acadavericangiographic
study.AmJSportsMed.2007;35(5):787–92.
39.CosgareaAJ,KramerDE,BahkMS,TottyWG,MatavaMJ.
ProximityofthepoplitealarterytothePCLduringsimulated
kneearthroscopy:implicationsforestablishingtheposterior
trans-septalportal.JKneeSurg.2006;19(3):181–5.
40.KumarSN,ChapmanJA,RawlinsI.Vascularinjuriesintotal
kneearthroplasty.Areviewoftheproblemwithspecial
referencetothepossibleeffectsofthetourniquet.J
Arthroplasty.1998;13(2):211–6.
41.NinomiyaJT,DeanJC,GoldbergVM.Injurytothepopliteal
arteryanditsanatomiclocationintotalkneearthroplasty.J
Arthroplasty.1999;14(7):803–9.
42.TakedaM,IshiiY,NoguchiH,SatoJ.Changeinthepositionof
thepolitealarterywithkneeflexionaftertotalknee
arthroplasty.JBoneJointSurgAm.2011;93(21):
e1231–6.
43.MureebeL,GahtanV,KahnMB,KersteinMD,RobertsAB.
Poplitealarteryinjuryaftertotalkneearthroplasty.AmSurg.
1996;62(5):366–8.
44.ShettyAA,TindalAJ,NickolaouN,JamesKD,IgnotusP.Asafe
zoneforthepassageofscrewsthroughtheposteriortibial
cortexintibialtubercletransfer.Knee.2005;12(2):99–101.
45.InsallJ.Surgeryoftheknee.Edinburgh:ChurchillLivingstone;
1984.
46.RubensF,WellingtonJL,BouchardAG.Poplitealarteryinjury
intibialosteotomy:reportoftwocases.CanJSurg.
1990;33(4):294–7.
47.HanK,WonY,KhangS.Pseudaneurysmaftertibialnailing.
ClinOrthopRelatRes.2004;(418):209–12.
48.KimJ,AllaireR,HarnerCD.Vascularsafetyduringhightibial
osteotomy:acadavericangiographicstudy.AmJSportsMed.