w w w . r b o . o r g . b r
Original
Article
Evaluation
of
intraoperative
radioscopy
on
the
coronal
alignment
of
the
tibial
component
in
primary
knee
arthroplasty
夽
Hugo
Cobra,
Marcio
Bruno
Hadid,
Daniel
Torres
Jácome,
Eduardo
Branco
de
Sousa,
Alan
de
Paula
Mozella,
Rodrigo
Pires
e
Albuquerque
∗KneeSurgeryCenter,InstitutoNacionaldeTraumatologiaeOrtopedia(INTO),RiodeJaneiro,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received15July2014 Accepted23September2014 Availableonline20August2015
Keywords: Arthroplasty Radiology Knee
a
b
s
t
r
a
c
t
Objectives: Thepresentstudyhadtheobjectiveofevaluatingtheeffectoftheuseof intraop-erativeradioscopyincasesofprimarykneearthroplasty,onthefinalalignmentofthetibial component.
Methods:Patientswhounderwenttotalkneearthroplasty(TKA)betweenApril13,2013,and April20,2013,wereincludedinthestudy.Thesepatientswereevaluatedretrospectivelyand twogroupswereidentified:oneinwhichintraoperativeradioscopywasusedtoassessthe positioningofthetibialcomponentduringthesurgeryandtheotherinwhichthisresource wasnotused.
Results:Themeanangleofalignmentofthetibialcomponentinrelationtothetibial dia-physiswasgreaterinthegroupwithoutuseofintraoperativeradioscopy(90.82)thaninthe groupwithradioscopy(90.63),whichwasastatisticallysignificantresult(p<0.05). Conclusion: Useof intraoperativeradioscopy during TKAproduceda bettermean angle ofalignmentbetweenthetibialcomponentandthetibialdiaphysis,incomparisonwith nonuse.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Avaliac¸ão
da
radioscopia
intraoperatória
no
alinhamento
coronal
do
componente
tibial
em
artroplastias
primárias
de
joelho
Palavras-chave: Artroplastia Radiologia Joelho
r
e
s
u
m
o
Objetivos:Avaliaroefeitodousodaradioscopiaintraoperatóriaemartroplastiasprimárias dejoelhosobreoalinhamentofinaldocomponentetibial.
Métodos:Foramincluídosnoestudoospacientessubmetidosàartroplastiatotaldojoelho (ATJ)entre13/04/2013e20/04/2013.Ospacientesforamavaliadosretrospectivamenteedois
夽
WorkperformedattheInstitutoNacionaldeTraumatologiaeOrtopedia(INTO),RiodeJaneiro,RJ,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](R.P.eAlbuquerque).
http://dx.doi.org/10.1016/j.rboe.2015.08.004
gruposforamidentificados,umcomusoderadioscopiaintraoperatóriaparaavaliac¸ãodo posicionamentodocomponentetibialduranteacirurgiaeosegundosemusodesserecurso. Resultados: Amédiadoângulodealinhamentodocomponentetibialemrelac¸ãoàdiáfiseda tíbiafoisuperiornogruposemusoderadioscopiaintraoperatória(90,82)emcomparac¸ão comogrupocomradioscopia(90,63),comresultadoestatisticamentesignificativo(p<0,05). Conclusão: OusoderadioscopianointraoperatóriodeATJproduzmelhormédiadeângulo dealinhamentoentreocomponentetibialemrelac¸ãoàdiáfisedatíbiaquandocomparado aonãouso.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Thetotalnumberofkneearthroplastyproceduresperformed everyyearhasincreasedexponentiallyandthemeanageof thepatientsundergoingthisinterventionhasdecreased,such thatthetopicoflongevityorsurvivalofimplantshasgained greaterattention.1,2
Thesuccessofthisprocedureisrelatedtoachievingproper alignment and correct management of ligament balance, alongwithprecisepositioningofitscomponents.3–5
Manyauthorshaveinvestigatedtheoutcomesfromtotal kneearthroplasty(TKA)andtheyhavereportedthatvarusor valgusmisalignmentsgreaterthan3◦resultingreaterchances
of aseptic loosening and failure of the implant.5,6 Berend etal.7 investigatedthemechanismsthroughwhichthe tib-ialcomponentfailedandconcludedthatmisalignmentofthis componentgreaterthan3◦wouldincreasethefailurerate.
Duringsurgicalprocedures,themethodsthatphysicians have available to them for verifying satisfactory position-ingofthecomponentsincludeclassicalalignmentguidance systems, evaluationmethodsusingnavigatedsurgery, con-ventionalradiographsandintraoperativeradioscopy.2,3,8
Aftertheoperation,the alignmentofprosthetic compo-nentscanbeevaluatedbymeansofsimpleradiographs,as recommendedbythe KneeSociety.1,9 On panoramic radio-graphsinAPview,thetibialcomponentshouldbeat90◦ in
relationtothelongaxisofthetibia1(Fig.1).
Thepresentstudyhadtheobjectiveofevaluatingtheeffect ofusingintraoperativeradioscopyonthefinalalignmentof thetibialcomponent,incasesofprimarykneearthroplasty.
Materials
and
methods
We retrospectively evaluated 115 patients who underwent totalkneearthroplastybetweenApril13and20,2013:53in agroupwithoutuse ofintraoperativeradioscopy and62 in agroupwithuseofradioscopy.Allthepatientshad indica-tionsforundergoingtotalkneearthroplasty,withadiagnosis ofprimaryosteoarthrosis.Theexclusioncriteriawere previ-oussurgery,bodymassindex>35,extra-articulardeformity, varusand valgusdeformity>10◦, flexion>10◦,bonedefects
greaterthan5mmandrheumaticdiseases.Allofthepatients constitutedahomogenousgroupwithoutseriousdeformities andwithmoderatekneeosteoarthrosis.
Fig.1– Postoperativeradiographicalignment.
The primary arthroplasty was performed in accordance withtheclassicaltechniquesthathavebeendescribed,with the onlydifferencethat intraoperativeradioscopy mightor might notbeused, accordingto thepreferenceofthe sur-geonofthegroup.Inthegroupinwhichitwasdecidedtouse radioscopywithaPhilips®imageintensifier,asingleAPview
ofthekneewasproducedontheoperatedkneejustafterthe tibialcutshadbeenmadeandthetestcomponenthadbeen emplaced.Thismadeitpossibleforthesurgeontointerfere inthefinalresultfrompositioningthetibialcomponent,such thattheviewedpositioncouldbeacceptedorcouldbealtered throughmakingabonecut.
After analysis on the sample, patients with incomplete medical documentation or absence of complete pre and postoperative routine radiological examinations would be excluded.However,noneofthepatientsinoursamplewere excluded.
Table1–Meansoftheabsolutevalues.
Withradioscopy Withoutradioscopy
Mean 90.63 90.82
Source:Hospitalservicefiles.
thelongaxisoftheleg.Theseareproducedinastandardized mannerbytheradiologyservice.Thepanoramicradiographs ofthelong axis oftheleg were producedin APprojection withthekneeextended,andthiswasdoneforallthepatients aftertheoperation.Thetube-filmdistancewastwometers. Carewas taken to place the lower limb ina neutral posi-tion, suchthat the patella would be directed anteriorly. A ShimatzoX-ray machine was used, with atechnique con-sistingof50kVand40mA.Theradiographswereevaluated regardingthecoronalalignmentofthetibialcomponent,on APpanoramicradiographsthatincludedthelongaxisofthe leg.Theanglebetweenalineparalleltothesurfaceofthe tib-ialcomponentandalinealongthelongaxisofthetibiawas calculated.Thiscalculationwasdoneusingtheangle mea-surementtoolsbelongingtotheMdicomViewerversion3.0 (27)digitalradiologicalviewingsoftware(MicrodataSystem). Inaddition,objectiveanalysiswasperformedonthemedical filesofthepatientsallocatedtoeachgroupanditwasverified fromthepostoperativeprotocolcardwhetherradioscopyhad beenusedornot.Ifithadbeenused,therewasachangeto thesurgicalstrategyregardingthetibialcut,withtheaimof ensuringbetterfinalalignmentofthetibialcomponent.The radiological analysisand viewingofthe medicalfiles were doneblindlybyasinglephysicianwhoisatitularmember oftheBrazilianSocietyofOrthopedicsandTraumatology,and whodidnotparticipateinthesurgicalprocedures.
Thedataweresubjectedtostatisticalanalysis,inorderto investigatetherelationship betweenthecoronalalignment anglesofthetibialcomponentofthegroupswithand with-out use ofintraoperativeradioscopy.Analysis bymeans of Student’s t test was used to ascertain whether there was anysignificantdifferencebetweenthegroups.Forthis,p val-ues<0.05weretakentobesignificant.
Results
Theresultsfrom thetwogroupsinquestionwere analyzed retrospectively.Thegroupforwhichintraoperativeradioscopy wasusedwascomposedof53patientsandthegroupwithout thiscomprised62patients.
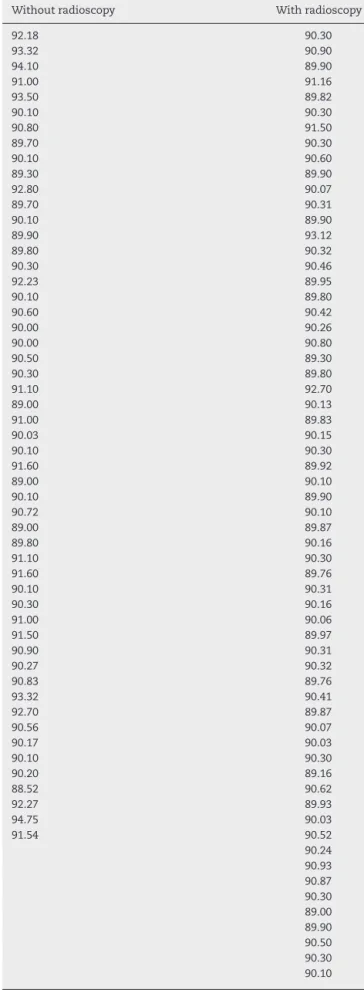
Themeanalignmentangleofthetibialcomponentin rela-tiontothediaphysisofthetibiawas90.82±1.34inthegroup withoutuseofintraoperativeradioscopyand90.63±0.64in thegroupwithuseofradioscopy(Table1).Therangeinthe groupwithoutuseofradioscopywasfrom88.52to94.25and inthegroupwithuseofradioscopy,89.00–93.12(Table2).
Fromtheresultsofthettest,itcanbestatedthattherewas evidencefromthesamplethatindicatedthatthemean dis-placementswouldbedifferentbetweenthegroups(p=0.0069). In the group without use of radioscopy, five patients obtained alignment angles for the tibial component in
Table2–Valuesoftheanglesinthegroupswithand withoutradioscopy.
Withoutradioscopy Withradioscopy
92.18 90.30 93.32 90.90 94.10 89.90 91.00 91.16 93.50 89.82 90.10 90.30 90.80 91.50 89.70 90.30 90.10 90.60 89.30 89.90 92.80 90.07 89.70 90.31 90.10 89.90 89.90 93.12 89.80 90.32 90.30 90.46 92.23 89.95 90.10 89.80 90.60 90.42 90.00 90.26 90.00 90.80 90.50 89.30 90.30 89.80 91.10 92.70 89.00 90.13 91.00 89.83 90.03 90.15 90.10 90.30 91.60 89.92 89.00 90.10 90.10 89.90 90.72 90.10 89.00 89.87 89.80 90.16 91.10 90.30 91.60 89.76 90.10 90.31 90.30 90.16 91.00 90.06 91.50 89.97 90.90 90.31 90.27 90.32 90.83 89.76 93.32 90.41 92.70 89.87 90.56 90.07 90.17 90.03 90.10 90.30 90.20 89.16 88.52 90.62 92.27 89.93 94.75 90.03 91.54 90.52 90.24 90.93 90.87 90.30 89.00 89.90 90.50 90.30 90.10
relationtothediaphysisofthetibiathatweregreaterthan 93◦.Inthegroupwithuseofradioscopy,onepatientobtained
ananglegreaterthan93◦.
Discussion
Studiesintheliteratureareunequivocalregardingthe impor-tanceofproperalignmentoftheprosthetic componentsof total knee arthroplasty for the final result relating to the functionaloutcome.Likewise,thecomplicationsinherentto pooralignment,especiallywithregardtomechanicalfailure, havebeenwelldocumented.4Thus,therelevanceofassessing intraoperativemethodsforguidingtheprecisionofthe align-menthasbeenincreasing.Nonetheless,thestudiessofarhave beeninconclusiveregardingwhatwouldconstitutethegold standard.Forthisreason,ourstudyevaluatedthefinal align-ment subsequentto totalknee arthroplasty, inaccordance withtheusualroutineofourkneesurgeons,andcompared groupswithorwithoutuseofintraoperativeradioscopy.
Theclassicalmethod,andtheonemostusedinmedical practice, is the mechanical method, making use of align-ment rodsdesignedfrom test components that havebeen implanted.Ourthinkingisthattheanatomicalparametersare important,butthatthehumaneyeisflawedandmaygiverise todeviationsofmorethan3◦.
AuthorssuchasMullajietal.4andHourlieretal.10 have indicatedradioscopyasaneffectiveoptionalmethodfor guid-ingtheintraoperativealignment,withfavorableresults.Our studyshowedthatarthroplastyproceduresthatwerechecked usingintraoperativeradioscopytendedtoobtainbetterfinal coronalalignmentofthetibialcomponent,evenifthe differ-encewasonlysmall,incomparisonwiththeclassicalmethods thatdonothavethisverification.Hence,wecorroboratethe affirmationscitedaboveandconfirmthatgoodpositioningof theimplantinassociationwithdurabilityisimportant.Onthe otherhand,onenegativefactorinthismethodistheradiation towhichpatientsareexposedthroughuseofradioscopy.Our thinkingisthatwhentherisksarecomparedwiththebenefits, thereisanadvantageinusingradioscopy.
Anotherfactorofrelevanceinfavoring thistechniqueis theobservedlargenumberofbonecutsfortibialcorrection(30 cuts,i.e.48.4%ofthisgroup)thatwasperformedsubsequently tofluoroscopy.Theseweremadeviablethroughthis immedi-ateassessmentofthefinalresult,providedthroughtheadvent ofradioscopy,withtheaimofimprovingthepositioningofthe tibialcomponent.
Thedifferenceinthemeansofthealignmentangleofthe tibialcomponent,inrelationtothediaphysisofthetibiain thetwogroups,wasstatisticallysignificant(p=0.0069). More-over,thegroupwithradioscopyshowedameananglecloser totheneutralaxis(90◦)thanthatofthegroupwithoutuse
ofradioscopy(90.63versus90.82,respectively,whichdepicts thegreatertendencyofthisfirstgrouptocorrectlyattainthe targetaxis.
Theliteratureshowsthatvarusorvalgusmisalignments greaterthan3◦resultingreaterchancesofasepticloosening
andimplantfailure.5,6Itwasobservedinthisstudythatinthe groupwithuseofradioscopy,onlyonepatientpresentedvarus greaterthan3◦,whileinthegroupwithoutuseofradioscopy,
fivepatientspresentedvarusgreaterthan3◦.Thisshowsthat
therewasatendencytowardgreaterchanceofmisalignment inthegroupwithoutuseofradioscopy.
Navigated surgeryfortotalknee arthroplasty isanother technique in which the aim is to achieve a well-aligned implant,therebyleadingtogreaterdurabilityofthis prosthe-sis.Thenavigatedsurgerytechniquehasbeenpresentedasan importantoptionforaddressingthedeficiencyofprecisionof traditionalguides,butitaddstothedurationoftheoperation andtothefinalcost.2,11–14Forthisreason,weadvocatetheuse ofradioscopyintotalkneearthroplastyprocedures.Thiscan beusedinmosthospitalsinBrazil,giventhatsoftwareand sensorsare unnecessary.Thenavigationtechniqueusedin totalkneearthroplastyproceduresmaysometimeshavetobe abortedduetoproblemswiththesensorsorwithanatomical referencepointsthataremarkederroneously.
The strong points of this study that we can highlight includethelargesamplethatwasachievedoverashortperiod oftime,providedthroughakneereferralcenterandthe cen-ter’sexperiencedgroupofkneesurgeonswiththecapacityto useauniformtechniquethatdivergedonlyinafewoperative stages, particularlywithregardtouseofradioscopy,which wasthefocusofourstudy.Moreover,ourpatientsconstituted ahomogenous groupwithoutserious deformitiesandwith moderatekneeosteoarthrosis.Anotherpositivepointwasthe blindingofasingleevaluatorofthefinalanglesobtained.
Thefactsthatthesurgicalprocedureswerenotperformed byasinglesurgeonandthatnopostoperativedescriptionsof thecutsmadeinthegroupwithoutradioscopywereincluded inthefilescanbetakentobeweaknessesofourstudy.
Conclusion
Use of intraoperative radioscopy during total knee arthro-plastyproducesabettermeanalignmentanglebetweenthe tibialcomponentandthediaphysisofthetibia,incomparison withnonuse.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.WindsorRE,ScuderiGR,MoranMC,InsallJN.Mechanismsof
failureofthefemoralandtibialcomponentsintotalknee
arthroplasty.ClinOrthopRelatRes.1989;248:15–9.
2.WengYJ,HsuRW,HsuWH.Comparisonofcomputer-assisted
navigationandconventionalinstrumentationforbilateral
totalkneearthroplasty.JArthroplast.2009;24(5):668–73.
3.HuangTW,HsuWH,PengKT,HsuRW,WengYJ,ShenWJ.
Totalkneearthroplastywithuseofcomputer-assisted
navigationcomparedwithconventionalguidingsystemsin
thesamepatient:radiographicresultsinAsianpatients.J
BoneJointSurgAm.2011;93(13):1197–202.
4.MullajiA,KannaR,MarawarS,KohliA,SharmaA.
Comparisonoflimbandcomponentalignmentusing
computer-assistednavigationversusimageintensifier-guided
randomized,single-surgeonstudyof467knees.JArthroplast. 2007;22(7):953–9.
5. KimSJ,MacDonaldM,HernandezJ,WixsonRL.Computer
assistednavigationintotalkneearthroplasty:improved
coronalalignment.JArthroplast.2005;207Suppl.3:123–31.
6. JeffcoteB,ShakespeareD.Varus/valgusalignmentofthetibial
componentintotalkneearthroplasty.Knee.2003;10(3):243–7.
7. BerendME,RitterMA,MedingJB,FarisPM,KeatingEM,
RedelmanR,etal.Tibial-componentfailuremechanismsin
totalkneearthroplasty.ClinOrthopRelatRes.2004;
428:26–34.
8. BolognesiM,HofmannA.Computernavigationversus
standardinstrumentationforTKA:asingle-surgeon
experience.ClinOrthopRelatRes.2005;440:162–9.
9. SatoT,KogaY,OmoriG.Three-dimensionallowerextremity
alignmentassessmentsystem:applicationtoevaluationof
componentpositionaftertotalkneearthroplasty.J
Arthroplast.2004;19(5):620–8.
10.HourlierH,FennemaP.Intraoperativefluoroscopyimproves
surgicalprecisioninconventionalTKA.KneeSurgSports
TraumatolArthrosc.2014;22(7):1619–25.
11.NovakEJ,SilversteinMD,BozicKJ.Thecost-effectivenessof
computer-assistednavigationintotalkneearthroplasty.J
BoneJointSurgAm.2007;89(11):2389–97.
12.AndersonKC,BuehlerKC,MarkelDC.Computerassisted
navigationintotalkneearthroplasty:comparisonwith
conventionalmethods.JArthroplast.2005;207Suppl.3:132–8.
13.EkET,DowseyMM,TseLF,RiaziA,LoveBR,StoneyJD,etal.
Comparisonoffunctionalandradiologicaloutcomesafter
computer-assistedversusconventionaltotalknee
arthroplasty:amatched-controlretrospectivestudy.JOrthop
Surg(HongKong).2008;16(2):192–6.
14.ChauhanSK,ScottRG,BreidahlW,BeaverRJ.
Computer-assistedkneearthroplastyversusaconventional
jig-basedtechnique.Arandomised,prospectivetrial.JBone