SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Anthropometric
study
of
the
knee
and
its
correlation
with
the
size
of
three
implants
available
for
arthroplasty
夽
Fabrício
Bolpato
Loures
a,∗,
Rogério
Franco
de
Araújo
Góes
a,
Idemar
Monteiro
da
Palma
b,
Pedro
José
Labronici
c,
José
Mauro
Granjeiro
d,
Beni
Olej
caHospitalSantaTeresa,Petrópolis,RJ,Brazil
bInstitutoNacionaldeTraumatologiaeOrtopedia(INTO),RiodeJaneiro,RJ,Brazil
cUniversidadeFederalFluminense,Niterói,RJ,Brazil
dInstitutoNacionaldeMetrologia,QualidadeeTecnologia(Inmetro),RiodeJaneiro,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received9May2015 Accepted2July2015 Availableonline8April2016
Keywords: Arthroplastyknee Anthropometry Femur
Tibia
a
b
s
t
r
a
c
t
Objective:TodefinetheanthropometricprofileofthekneeinaBrazilianpopulationwith gonarthrosisusingintraoperativemeasurements;andtoevaluatethecompatibilityofthree implantsavailablefortotalkneearthroplasty.
Methods:Morphometricdatawerecollectedprospectivelyfrom117subjectswith gonarthro-sis.Sixdimensionsinthedistalfemurandtwointheproximaltibiaweredocumentedin118 kneeswhileperformingtotalarthroplasty.Thesedatawerecomparedwiththedimensions ofthreeimplantsavailablefortotalkneearthroplasty.
Results:Thestatisticalanalysisshowedthatmorethanaquarterofthepatientspresented anunsatisfactoryrelationshipbetweenthekneeandprosthesis.
Conclusion:TheimplantsevaluatedneedtobeadjustedtobetterfitBrazilianpatients. ©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Estudo
antropométrico
do
joelho
e
sua
correlac¸ão
com
o
tamanho
de
três
implantes
disponíveis
para
artroplastia
Palavras-chave: Artroplastiadojoelho Antropometria Fêmur Tíbia
r
e
s
u
m
o
Objetivo:Definiroperfilantropométricodojoelhoempopulac¸ãobrasileiraportadorade gonartrose,comousodamensurac¸ãointraoperatória,eavaliaracompatibilidadedetrês implantesdisponíveisparaartroplastiatotaldojoelho.
Métodos:Foramcoletados,deformaprospectiva,osdadosmorfométricosde117pacientes portadoresdegonartrose.Documentaram-seseisdimensõesnofêmurdistaleduasnatíbia
夽
StudyconductedatHospitalSantaTeresadePetrópolis,RJ,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](F.B.Loures). http://dx.doi.org/10.1016/j.rboe.2015.07.009
proximalem118joelhos,duranteaartroplastiatotal.Essesdadosforamcomparadoscom asdimensõesdostrêsimplantesdisponíveisparaartroplastiatotaldojoelho.
Resultados: Aanáliseestatísticarevelouquemaisdeumquartodospacientesapresentou relac¸ãoinadequadaentreosjoelhoseaspróteses.
Conclusão:Osimplantesavaliadosnecessitamdeajustesparamelhoratenderaospacientes brasileiros.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.EsteéumartigoOpenAccesssobalicençadeCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Osteoarthrosis (OA) is the main cause of musculoskeletal disability in the elderly and the main cause of total knee arthroplasty(TKA).1 Theagingprocess,the geneticburden, andfemalegenderarenon-modifiablefactorsassociatedwith theoriginofthedisease.2Obesityandactivitieswithloadalso haveadirectparticipationinthisdisease.IntheBrazilian pop-ulationabove19 yearsofage, 5.2%ofthe individuals have sometypeofarthrosis (nearly10million individuals). This numberwillprobablyincreaseandreach12.4millionin2015.3 OAincidencehasadirectrelationwithage,affecting85%of thepopulationabove75years.4Accordingtoprojectionsof theBrazilianInstituteofGeographyandStatistics(Instituto BrasileirodeGeografiaeEstatística[IBGE]),in2030Brazilwill probablyhavethesixtholdestpopulationintheworld,5afact that,associatedwiththeincreaseofobesityrates,will signif-icantlyincreasetheprevalenceofthisdisease.
Even though thereare noofficial statistics for Brazil,it isestimatedthat 70,000knee arthroplastiesare performed yearly.6TheincreaseoftheBrazilianmeanincomehas facil-itated the access to healthcareservices and increasedthe numberofTKAcandidates,seekingbetterqualityoflifeand higherphysicalcapacity.7
Prosthesisimplantationisasurgeryofprecision,andthe similarity between the implant and the resected bone is essentialforagood clinicalresultand thedurabilityofthe replacement.8 Theknee anatomy presents greatvariability regardinggender,8–14ethnicity,10,15–20andbodytype.21
AfterresearchingtheliteratureinPortugueseandEnglish language,theauthorsdidnotretrievestudiesdefiningknee dimensions in the Brazilian population with gonarthrosis. Thus,prosthesesdevelopedforCaucasianswereintroduced inthecountrywithoutanymodification.Apossible incompat-ibility,evenifpartial,increasesthecomplexityofthesurgery andhinderstheappropriatematchingoftheimplantwiththe bone.
Thisstudyaimedtodefinetheanthropometrickneeprofile intheBrazilianpopulationwithgonarthrosisusing intraoper-ativemensuration,andtocomparethebonedimensionswith threeavailableimplantsforarthroplasties.
Material
and
methods
Afterapprovalofthestudybytheinstitution’sResearchEthics Committee,underNo.CEP68542,118kneesof117patients whounderwentTKAbetweenAugust2012andDecember2013
were prospectivelystudied.Thestudy includedall patients whoacceptedtoparticipatebysigningtheinformedconsent form. Caseswith history ofprior knee fracture or surgery, patientswhopresentedbonelossesthatneededgrafting,and thosewithvarusorvalgusdeformitygreaterthan15◦ were excluded.
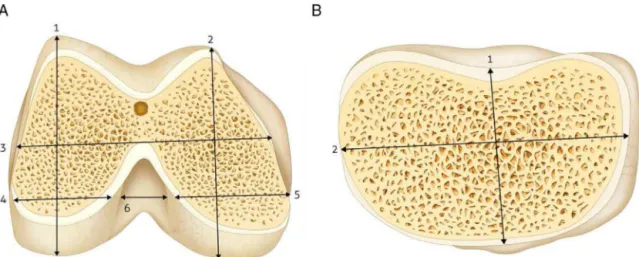
Three metal pachymeters were purchased and sent to the National Institute of Metrology, Quality, and Technol-ogy(InstitutoNacionaldeMetrologia,QualidadeeTecnologia [Inmetro]),whichconfirmedtheprecisionoftheinstruments. During the surgicalprocedure, the leadsurgeonconducted sixmensurationsofthefemur:heightandwidthofthe lat-eralandmedialcondyles,totalmediolateralandintercondyle width(Fig.1A),andtwoonthetibia:mediolateraland antero-posterior width(Fig. 1B).Thedimensions wererecorded in millimeters,aftertwomeasurementsperformedbythemain investigator,inordertoavoidanyinterobserveralteration.The arithmeticmeanwasusedforanalysis.
Prior to the measurements, the distal cut ofthe femur and the proximalcut ofthe tibia were performed, and all osteophyteswere removed.This maneuverallowedforthe identificationoftheactualdimensionsofthebonesurfaces thatwouldbeincontactwiththeimplant.Themediolateral femoraldistancewasmeasured atthelevel ofthe surgical transepicondylaraxis.Thewidthofeachfemoralcondylewas measuredat8mmoftheposteriorarticularsurfaceofthe lat-eralcondyleandat10mmoftheposteriorarticularsurfaceof the medialcondyle,simulating theexternalrotationofthe femur. The anteroposteriormeasurements were performed priortothecuts,inordertoassesswhetheroverstuffingwould occur.Theanteroposteriorwidthofthetibiawasmeasured fromthecenteroftheposteriorcruciateligament(PCL)tothe medialthirdofthepatellartendon.Themediolateralwidth wasthelargestperpendiculardistancetothefirst measure-ment.
Theimplantswerechosenbythesimilaritywiththeheight ofthelateralcondyleanditswidthcomparedwiththetotal width of the femurafterthe distal cut.Therelative index (RI)betweentotalwidthandheightofthelateralcondyle,as describedbyHittetal.,wasalsoassessed.9
Considering the objective of the study, the following assumptionsweremadeforthecalculationofthesamplesize: significancelevel of5%(˛),statistical power of80% (1−),
Fig.1–Intraoperativemeasurement(A)rightdistalfemur:1–heightofthelateralcondyle;2–heightofthemedialcondyle; 3–totalwidthofthefemur;4–widthofthelateralcondyle;5–widthofthemedialcondyle;6–intercondylarfossa;(B)right proximaltibia:1–anteroposteriorwidth;2–mediolateralwidth.
Thedescriptiveanalysiswaspresentedontablesand illus-trativecharts.Theobserveddata wereexpressed asmean, standard deviation, median, minimum, and maximum for numericaldata,byfrequency(n)andpercentage(%)for cat-egoricaldata.
The intraclass correlation coefficient (ICC) was used to assessthecompatibilityofthreeimplantsfrequentlyavailable inBrazil:Scorpio®(StrykerHowmedicaOsteonics),NexGen® (Zimmer,Warsaw,Indiana),andNativeKnee®(Zimmer, War-saw,Indiana).TheMcNemartest wasusedtocomparethe threeimplantsbrands.
Non-parametricmethodswereused,asthevariablesdid notpresentaGaussiandistributionasshownbytherejection oftheShapiro–Wilksnormalitytest.Theadoptedsignificance criterion was the level of 5%. Statistical analysis was per-formedusingthestatisticalsoftwareSAS®version6.1.
Results
Thestudyincluded118kneesfrom117patients;33patients weremaleand84werefemale.Onefemalepatientunderwent bilateralTKA.Table1presentsthedistributionofthesample regardinggender,operatedside,andethnicity.
Theanalysisofthedistalfemurdatashowedsignificantly greaterabsolutevaluesformalepatients.TheRIbetweentotal widthofthefemurandheightofthelateralcondylewas sim-ilarforbothgenders(Table2).
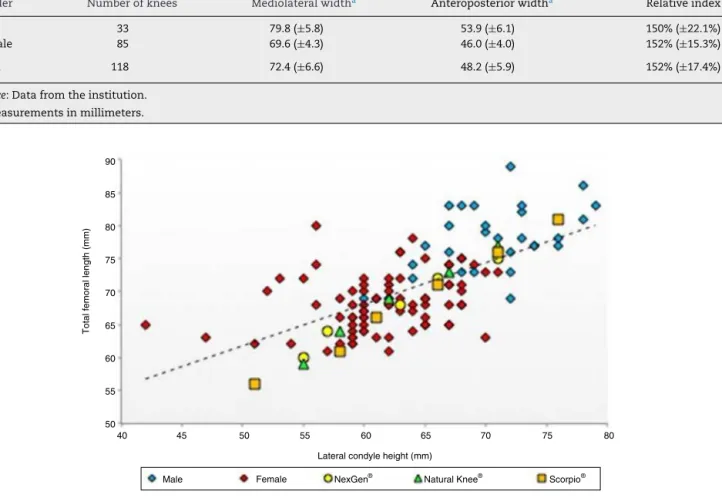
Similarlytothedistalfemur,thetibialmeasurespresented significantlygreatervaluesformalepatients.TheRIbetween themediolateral andanteroposterior widthwasgreater for femalepatients.Thatsuggeststhatthesetibiasmaybewider. However,thisdifferencewasnotsignificant(p=0.26;Table3). Therewasgreatvariationoftherelationbetweenthetotal width of the femur and the height of the lateral condyle, regardlessofthesizeofthefemur(patientheight).
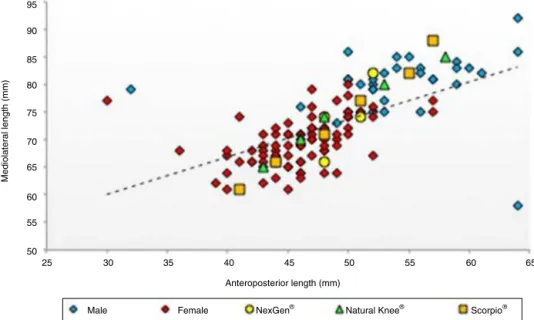
Figs.2and3showtherelationoftheprosthesiswiththe bonesurfacesalreadypreparedtoreceivetheimplant.
Table1–Samplecharacterization.
Variable Numberofknees Percentage
Gender
Male 33 28.0%
Female 85 72.0%
Side
Right 60 50.8%
Left 58 49.2%
Ethnicity
White 105 89.0%
Mixed-race 9 7.6%
Black 4 3.4%
Source:Datafromtheinstitution.
Thecorrelationofthefemoralimplantswiththeresected bonesreceivedgreaterattention,asthesearedirectlyrelated toappropriatejointbalanceandnormalgait.Toassessthis relation,theICCwasused,whichrevealedasignificant,albeit moderate,conformityofthreeimplantstothedistalfemurof thestudiedsample(p<0.0001,Table4).
Adifferenceequaltoorgreaterthan3mmwasconsidered unbearableforimplantover-orunderhanginthe mediolat-eralsense.Thisstudyobservedthat29.7%ofthepatientswho usedScorpio®,28.8%ofthosewhousedNexGen®,and27.9%of thosewhousedNativeKnee®presentedinadequacies. Under-hangwasthemostfrequentproblem,presentin20.9%ofthe patients,anditwastwiceascommonamongmalepatients. Mediolateraloverhangwaspresentin7.9%ofthepatientsand wasthreetimesascommonamongfemalepatients.The dis-tributionofincompatibilitiesequaltoorgreaterthan3mmis presentedinTable5.
Table2–Distalfemur.
Gender Numberofknees Totalwidtha Heightofthelateralcondylea Relativeindex
Male 33 77.7(±4.9) 70.3(±4.7) 111%(±7.1%)
Female 85 67.8(±4.0) 61.5(±4.9) 111%(±10.4%)
Total 118 70.6(±6.1) 64.0(±6.3) 111%(±9.6%)
Source:Datafromtheinstitution. a Measurementsinmillimeters.
Table3–Proximaltibia.
Gender Numberofknees Mediolateralwidtha Anteroposteriorwidtha Relativeindex
Male 33 79.8(±5.8) 53.9(±6.1) 150%(±22.1%)
Female 85 69.6(±4.3) 46.0(±4.0) 152%(±15.3%)
Total 118 72.4(±6.6) 48.2(±5.9) 152%(±17.4%)
Source:Datafromtheinstitution. a Measurementsinmillimeters.
90
85
75
65
55
50
60 50
45 40
Lateral condyle height (mm)
Total femoral length (mm)
80
70 75
65 55
60 70 80
Male Female NexGen® Natural Knee® Scorpio®
Fig.2–Relationbetweenimplantsanddistalfemur. Source:Datafromtheinstitution.
Discussion
Brazilhasbeenpresentingtypicalsocialchangesof develop-ingcountries,suchaspopulationaging23andthegrowthof obesity.24Thesefactorsaredirectlyconnectedtothegenesisof osteoarthrosis,whichallowsustopredictthatthedemandfor jointreplacementswillgrowexponentiallyinthenearfuture. FollowingtheprinciplesofTKAandimplantingthe appro-priateprosthesissizearefundamentalfactorsforthesuccess ofjointreplacementsurgery.Correct ligamentbalance and maximum bone coverage by the implant are pursued, in order to reduce the stress on the bone–implant surface.15 Mismatchingsinthisrelationincreasethecomplexityofthe surgery.19
Table4–Relationbetweendistalfemurandimplants.
Prosthesis ICC 95%CI p-value
Scorpio® 0.592 0.462–0.698 <0.0001
NaturalKnee® 0.534 0.392–0.651 <0.0001
NexGen® 0.547 0.407–0.661 <0.0001
Source:Datafromtheinstitution.
ICC,intraclasscorrelationcoefficient;CI,confidenceinterval.
95
90
85
75
65
55
50
45 40
35 50 60
30 25
Anteroposterior length (mm)
Mediolateral length (mm)
65 55
60 70 80
Male Female NexGen® Natural Knee® Scorpio®
Fig.3–Relationbetweenimplantsandproximaltibia. Source:Datafromtheinstitution.
Table5–Distributionoftheincompatibilities≥3mm.
Gender Male Female
Prosthesis/incompatibility Underhanga Overhanga Underhanga Overhanga
Scorpio® 9 1 18 7
NexGen® 13 1 12 8
NaturalKnee® 9 1 13 10
Total 31(31.3%) 3(3%) 43(16.9%) 25(9.8%)
Source:Datafromtheinstitution. a Numberofpatients.
bonedimensionsthatwouldbeincontactwiththeimplants. Additionally,everypatientofthesamplepresentedtheclinical andradiographicdiagnosisofkneeosteoarthrosis,and there-forepresentedthetypicalanatomicalchangesofthisdisease. Theseaspectsincreasedthereliabilityofthestudy,sincethe dimensionsofosteoarthritickneesaredifferentfromthoseof normalknees.8
ThemeanRIofthefemuramongmalepatientswas111%, rangingfrom 101%to124%. Femalepatientspresentedthe samemean,howeverwithamuchwiderrange,from90%to 143%.Thisfactrevealsthegreateranatomicalvariabilityof thedistalfemurinthisgender. Thisvalueisinagreement withthedimensionsfoundforKoreans(111%)19;howeverthey are larger than those of the Chinese (109%)10 and smaller thanthoseoftheJapanese(129%)populations.19Thestudied implantspresentedanRIvariationbetween105%and112%, indicatingthattherecanbebothunder-andoverhang.
Ha et al.19 found a tendency of underhang forsmaller femurs,andofoverhangforlargerfemurs.Thistendencywas notobservedinthepresentsample.Agreatvariabilityofthe totalwidthofthefemurwasobservedforthesame height ofthelateralcondyle.Thestudiedimplants presentedonly onewidthforeachheight,whichappearsnottobetheideal format.
Table6–Comparisonbetweentheimplants.
Prosthesis p-valuea
Scorpio®vs.NexGen® 0.88 Scorpio®vs.NaturalKnee® 0.23 NexGen®vs.NaturalKnee® 0.15
Source:Datafromtheinstitution. a p-valuefor5%.
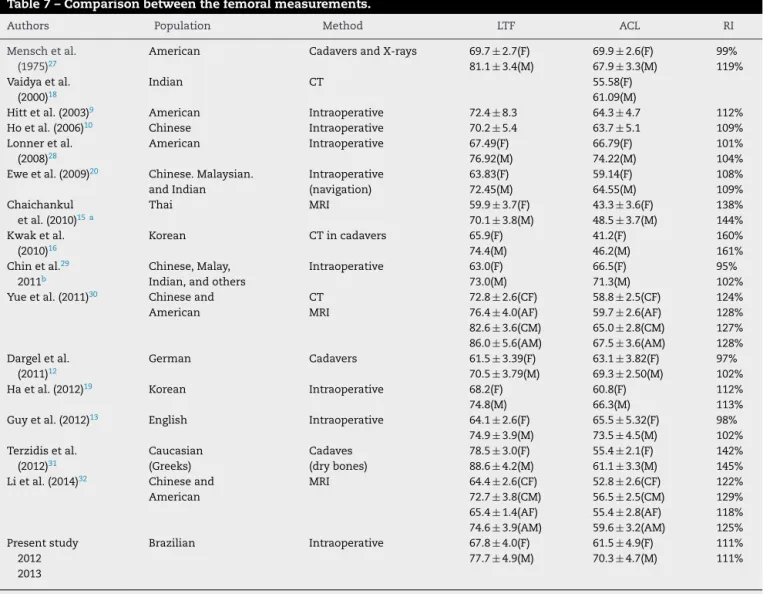
Table7–Comparisonbetweenthefemoralmeasurements.
Authors Population Method LTF ACL RI
Menschetal. (1975)27
American CadaversandX-rays 69.7±2.7(F) 81.1±3.4(M)
69.9±2.6(F) 67.9±3.3(M)
99% 119% Vaidyaetal.
(2000)18
Indian CT 55.58(F)
61.09(M)
Hittetal.(2003)9 American Intraoperative 72.4±8.3 64.3±4.7 112% Hoetal.(2006)10 Chinese Intraoperative 70.2±5.4 63.7±5.1 109% Lonneretal.
(2008)28
American Intraoperative 67.49(F)
76.92(M)
66.79(F) 74.22(M)
101% 104% Eweetal.(2009)20 Chinese.Malaysian.
andIndian Intraoperative (navigation) 63.83(F) 72.45(M) 59.14(F) 64.55(M) 108% 109% Chaichankul
etal.(2010)15 a
Thai MRI 59.9±3.7(F)
70.1±3.8(M)
43.3±3.6(F) 48.5±3.7(M)
138% 144% Kwaketal.
(2010)16
Korean CTincadavers 65.9(F)
74.4(M)
41.2(F) 46.2(M)
160% 161% Chinetal.29
2011b
Chinese,Malay, Indian,andothers
Intraoperative 63.0(F) 73.0(M) 66.5(F) 71.3(M) 95% 102% Yueetal.(2011)30 Chineseand
American
CT MRI
72.8±2.6(CF) 76.4±4.0(AF) 82.6±3.6(CM) 86.0±5.6(AM)
58.8±2.5(CF) 59.7±2.6(AF) 65.0±2.8(CM) 67.5±3.6(AM)
124% 128% 127% 128% Dargeletal.
(2011)12
German Cadavers 61.5±3.39(F)
70.5±3.79(M)
63.1±3.82(F) 69.3±2.50(M)
97% 102% Haetal.(2012)19 Korean Intraoperative 68.2(F)
74.8(M)
60.8(F) 66.3(M)
112% 113% Guyetal.(2012)13 English Intraoperative 64.1±2.6(F)
74.9±3.9(M)
65.5±5.32(F) 73.5±4.5(M)
98% 102% Terzidisetal.
(2012)31
Caucasian (Greeks)
Cadaves (drybones)
78.5±3.0(F) 88.6±4.2(M)
55.4±2.1(F) 61.1±3.3(M)
142% 145% Lietal.(2014)32 Chineseand
American
MRI 64.4±2.6(CF)
72.7±3.8(CM) 65.4±1.4(AF) 74.6±3.9(AM)
52.8±2.6(CF) 56.5±2.5(CM) 55.4±2.8(AF) 59.6±3.2(AM)
122% 129% 118% 125% Presentstudy 2012 2013
Brazilian Intraoperative 67.8±4.0(F) 77.7±4.9(M)
61.5±4.9(F) 70.3±4.7(M)
111% 111%
F,female;M,male;AF,Americanfemale;CF,Chinesefemale;AM,Americanmale;CM,Chinesemale. a Chaichankuldidnotusethesameanatomicalparameters.
b APmeasurementafterthetrochlearcut.
Thestudiedimplantsweredevelopedbasedon anthropo-metricstudiesinCaucasianpopulations.Theauthors’initial hypothesiswas that valuesforknee anthropometry inthe Brazilianpopulationwouldbedifferentfromthatother pop-ulation.Whenthemeasurementsofthepresentstudywere compared with other studies that assessed different eth-nicities, the mean Brazilian values were similar to those describedforCaucasians,whichleadstothebeliefthatthe incompatibilities are not a consequence of ethnic differ-ences.Theconflictbetween the small number ofavailable implants and the great anatomical variability of the dis-tal femurcan bethe cause ofthese incompatibilities. The main assessedanthropometric studies are summarized in Table7.9,13,15,17–20,27–32
Thegreatnumberofpatientswhoself-declaredaswhite mightbeafactor.Penaetal.33conductedageneticstudyof theBrazilianpopulationanddemonstratedthattheAfrican ancestryinwhitesubjectsfromtheBrazilianSoutheastwas upto32%,whiletheEuropeanancestryinblacksubjectsfrom
thatregionreachedupto49%.Thatprovesthattherelation betweenskincolorandgeneticinheritanceinBrazilisvery weak. Afterfive centuriesof racial mixing, the phenotypic manifestationofskincolorhaslittleornovalueinmedical practice.
highertibialcoverage,thecorrectrotationalalignmentoccurs more frequently in asymmetrical implant, as the match-ing betweenrotationand coverage iseasierinthis typeof prosthesis.
Conclusions
AsignificantnumberofpatientswhoundergoTKAinBrazil presentdifferencesabovetheacceptablebetweenthe dimen-sionsofthekneesandofthestudiedimplants,whichmay compromise the clinical result and the durability of the surgeryresults.Thestudy indicatesthat adjustmentsneed tobemadesothattheimplantscanappropriatelymeetthis growingdemand.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. CenterforDiseaseControlandPrevention.Prevalenceof doctor-diagnosedarthritisandarthritis-attributableactivity limitation–UnitedStates,2007–2009.MMWR.
2010;59(39):1261–5.
2. FelsonDT.Theepidemiologyofkneeosteoarthritis:results fromtheFraminghamstudy.SeminArthritisRheum.1990;20 (30)Suppl1:42–50.
3. CoimbraIB,RezendeMU,PlaperPG.Osteoartite(artrose)– cenárioatualetendênciasnoBrasil.SãoPaulo:Limay;2012. 4. VailTP,LangJE,SikesCV.Surgicaltechniquesand
instrumentationintotalkneearthroplasty.In:ScottW,editor. Norman.Insaal&ScottSurgeryoftheknee.5ed.
Philadelphia:ElsevierChurchillLivingstone;2012. p.1042–99.
5. IBGE–InstitutoBrasileirodeGeografiaeEstatística. Indicadoressociodemográficos.ProspectivosparaoBrasil 1991/2030.RiodeJaneiro:Arbeit;2006.
6. SaladeImprensa.Artroplastiaéparaalíviodador.Available from:http://www.boehringer.com.br/conteudoimprensa texto.asp?conteudo=12&texto=988[accessed02.06.14]. 7. FilhoGRM,CavanellasN.Artroplastiaminimamenteinvasiva
dojoelho.RevBrasOrtop.2007;42(9):269–77.
8. ChengCK,LungCY,LeeYM,HuangCH.Anewapproachof designingthetibialbaseplateoftotalkneeprostheses.Clin Biomech(Bristol,Avon).1999;14(2):112–7.
9. HittK,ShurmanJR2nd,GreeneK,McCarthyJ,MoskalJ, HoemanT,etal.Anthropometricmeasurementsofthe humanknee:correlationtothesizingofcurrentknee arthroplastysystems.JBoneJointSurgAm.2003;85Suppl. 4:115–22.
10.HoWP,ChengCK,LiauJJ.Morphometricalmeasurementsof resectedsurfaceoffemursinChineseknees:correlationto thesizingofcurrentfemoralimplants.Knee.2006;13(1):12–4. 11.ChinKR,DaluryDF,ZurakowskiD,ScottRD.Intraoperative
measurementsofmaleandfemaledistalfemursduring primarytotalkneearthroplasty.JKneeSurg.2002;15(4): 213–7.
12.DargelJ,MichaelJW,FeiserJ,IvoR,KoebkeJ.Humanknee jointanatomyrevisited:morphometryinthelightof sex-specifictotalkneearthroplasty.JArthroplasty. 2011;26(3):346–53.
13.GuySP,FarndonMA,SidhomS,Al-LamiM,BennettC,London NJ.Genderdifferencesindistalfemoralmorphologyandthe roleofgenderspecificimplantsintotalkneereplacement:a prospectiveclinicalstudy.Knee.2012;19(1):28–31.
14.ConleyS,RosenbergA,CrowninshieldR.Thefemaleknee: anatomicvariations.JAmAcadOrthopSurg.2007;15Suppl. 1:S31–6.
15.ChaichankulC,TanavaleeA,ItiravivongP.Anthropometric measurementsofkneejointsinThaipopulation:correlation tothesizingofcurrentkneeprostheses.Knee.2011;18(1): 5–10.
16.KwakDS,HanS,HanCW,HanSH.Resectedfemoral anthropometryfordesignofthefemoralcomponentofthe totalkneeprosthesisinaKoreanpopulation.AnatCellBiol. 2010;43(3):252–9.
17.UrabeK,MahoneyOM,MabuchiK,ItomanM.Morphologic differencesofthedistalfemurbetweenCaucasianand Japanesewomen.JOrthopSurg(HongKong).2008;16(3):312–5. 18.VaidyaSV,RanawatCS,AroojisA,LaudNS.Anthropometric
measurementstodesigntotalkneeprosthesesfortheIndian population.JArthroplasty.2000;15(1):79–85.
19.HaCW,NaSE.Thecorrectnessoffitofcurrenttotalknee prosthesescomparedwithintra-operativeanthropometric measurementsinKoreanknees.JBoneJointSurgBr. 2012;94(5):638–41.
20.EweTW,AngHL,CheeEK,NgWM.Ananalysisofthe relationshipbetweenthemorphometryofthedistalfemur andtotalkneearthroplastydesign.MalOrthopJ.
2009;3(2):24–8.
21.BellemansJ,CarpentierK,VandenneuckerH,VanlauweJ, VictorJ.Bothmorphotypeandgenderinfluencetheshapeof thekneeinpatientsundergoingTKA.ClinOrthopRelatRes. 2010;468(1):29–36.
22.CohenJ.Statisticalpoweranalysisforthebehaviorsciences. NewYork:AcademicPress;1969.p.415.
23.IBGE–InstitutoBrasileirodeGeografiaeEstatística. Observac¸õessobreaevoluc¸ãodamortalidadenoBrasil:o passado,opresenteeperspectivas.RiodeJaneiro,2010. Availablefrom:http://www.ibge.gov.br/home/estatistica/ populacao/tabuadevida/2009/notastecnicas.pdf[accessed 06.05.14].
24.KhanA.Americatopslistof10mostobesecountries.In: USNEWS;2014.Availablefrom:http://health.usnews.com/ health-news/health-wellness/articles/2014/05/28/america-tops-list-of-10-most-obese-countries[accessed12.08.14]. 25.PiriouP,MabitC,BonnevialleP,PeronneE,VersierG.Are
gender-specificfemoralimplantsfortotalkneearthroplasty necessary?JArthroplasty.2014;29(4):742–8.
26.MahoneyOM,KinseyT.Overhangofthefemoralcomponent intotalkneearthroplasty:riskfactorsandclinical
consequences.JBoneJointSurgAm.2010;92(5): 1115–21.
27.MenschJS,AmstutzHC.Kneemorphologyasaguidetoknee replacement.ClinOrthopRelatRes.1975;23(112):1–42. 28.LonnerJH,JaskoJG,ThomasBS.Anthropometricdifferences
betweenthedistalfemoraofmenandwoman.ClinOrthop RelatRes.2008;(466):2724–9.
29.ChinLP,TeyTT,IbrahimMYB,ChiaSL,YeoJS,LoNN. Intraoperativemorphometricstudyofgenderdifferencesin Asianfemurs.JArthroplasty.2011;26:984–8.
30.YueB,VaradarajanK,AiS,TangT,RubashHE,LiG. DifferencesofKneeanthropometrybetweenChineseand Whitemenandwoman.JArthroplasty.2011;26(1): 124–30.
32.LiP,TsaiTY,LiJS,ZhangY,KwonYM,RubashHE,etal. Morphologicalmeasurementoftheknee:raceandsex effects.ActaOrthopBelg.2014;80(2):260–8.
33.PenaSDJ.Razõesparabaniroconceitoderac¸adamedicina brasileira.HistCiencSaúde-Manguinhos.2005;12(1): 321–46.
34.LiuZ,YuanG,ZhangW,ShenY,DengL.Anthropometryof theproximaltibiaofpatientswithkneearthritisinShanghai. JArthroplasty.2013;28(5):778–83.