Artigo Original
Aline Rodrigues Padovani1 Danielle Pedroni Moraes2 Fernanda Chiarion Sassi3 Claudia Regina Furquim de Andrade3
Descritores
Fonoaudiologia Transtornos da deglutição Unidades de terapia intensiva Métodos Deglutição
Keywords
Speech, language and hearing sciences Deglutition disorders Intensive care units Methods Deglutition
Correspondence address:
Claudia Regina Furquim de Andrade R. Cipotânea, 51, Campus Cidade Uni-versitária, São Paulo (SP), Brasil, CEP: 05360-160.
E-mail: [email protected]
Received: 7/6/2011
Accepted: 11/30/2011
Study conducted at the Department of Physical Therapy, Speech-Language Pathology and Audiology, and Oc-cupational Therapy, School of Medicine, Universidade de São Paulo – USP – São Paulo (SP), Brazil. (1) Graduate Program (Masters degree) in Rehabilitation Sciences, Department of Physical Therapy, Speech-Language Pathology and Audiology, and Occupational Therapy, School of Medicine, Universidade de São Paulo – USP – São Paulo (SP), Brazil.
(2) Graduate Program (PhD) in Rehabilitation Sciences, Department of Physical Therapy, Speech-Language Pathology and Audiology, and Occupational Therapy, School of Medicine, Universidade de São Paulo – USP – São Paulo (SP), Brazil.
(3) Department of Physical Therapy, Speech-Language Pathology and Audiology, and Occupational Therapy, School of Medicine, Universidade de São Paulo – USP – São Paulo (SP), Brazil.
Conflict of interests: None
Avaliação clínica da deglutição em unidade de terapia
intensiva
ABSTRACT
Purpose: To report the results of the full clinical swallowing assessment in acute-care population in a large Brazilian teaching hospital. Methods: A prospective, descriptive clinical study was conducted during three months in a 30-bed adult clinical emergency ICU from a large Brazilian teaching hospital. Thirty-five patients consecutively referred to the Speech-Language Pathology Service according to our standard clinical practice were included. A full clinical swallowing assessment was completed and includes a Preliminary Assessment Protocol (PAP), a Dysphagia Risk Evaluation Protocol (DREP)and an Oral Feeding Transition Protocol (OFTP). Results: In this study, the prevalence of OD in the ICU setting was of 63%, most of which were classi-fied as moderate and moderate-severe (39%). Patients submitted to orotracheal intubation were very frequently referred to swallowing assessment (74%). The results of the statistical analyses revealed clinical indicators that could correctly classify patients as either having or not having OD on clinical tests. These include cough strength, coordination between breathing and speaking, dysphonia severity, and laryngeal elevation. Twenty six patients (74%) completed all protocols. Of these total, 38% were able to eat a regular diet. Conclusion:
The practice with standardized protocols adds an important option for the management of oropharyngeal dysphagia in intensive care unit.
RESUMO
INTRODUCTION
Oropharyngeal dysphagia (OD) is potentially life-threa-tening with consequences such as: malnutrition, dehydration, aspiration pneumonia, increased risk of complications, dis-charge to nursing home and higher mortality(1). There are also financial costs, including longer length of intensive care unit (ICU), expenses for antibiotics, X-rays, increased nursing time and physician consultations(2,3).
As many as 12-30% of hospitalized patients have dyspha-gia that results in aspiration of oral contents(4,5). The etiologic agents differ according to the studied population, duration of hospital stay, and time after intubation. The development of post-extubation swallowing dysfunction is well documented in the literature with high prevalence in most studies, ranging from 44 to 87%(6-10). Risk factors include age, pulmonary diseases, tracheostomy, neurological diseases, and head and neck cancer. When patients are admitted to the ICU, they are at increased risk of having more frequent aspiration events because of a variety of factors. These factors include depressed level of conscious-ness (often caused by excessive analgesia and sedation), forced supine position, and the presence of tracheostomy, nasogastric or endotracheal tubes(11-15).
In most cases, medical assessment, therapy, and management of dysphagia start in the ICU environment. The early identifi-cation of the disturbance is necessary for the safe provision of foods, liquids and oral medications(5). Clinical bedside asses-sment currently is the most widely used form of swallowing assessment. It is used frequently by health professionals as a first-line (and on occasion, as the only) means for investigating a clinical suspicion of a swallowing disorder. It is inexpensive, noninvasive, time efficient, and consumes few resources(16,17).
The full clinical swallowing assessment typically includes gathering information regarding the current swallowing pro-blem, reviewing medical history, observing signs relevant to the patient’s medical status, conducting a structural/functional exa-mination of speech and swallowing structures, and observing the patient during trial swallows. Generally, this is recognized as one component of the comprehensive evaluation. The results of this examination determine whether further instrumental assessment of dysphagia is warranted(18).
Screening procedures are generally designed to be quick (~15minutes), relatively noninvasive, with little risk to patient while identifying the symptoms of dysphagia requiring in-depth diagnostic assessment(19). Few data are available on full clinical swallowing assessment in intensive care unit. The aim of this study was to report the results of the full clinical swallowing assessment in acute-care population in a large Brazilian tea-ching hospital.
METHODS
A prospective, descriptive clinical study was conducted during three months in a 30-bed adult clinical emergency ICU from a large Brazilian teaching hospital. Thirty-five patients who were consecutively referred to the Speech-Language Pathology Service were included in the experiment. This
research was done in accordance with the appropriate institu-tional ethics committee and carried out in conformity with the ethical standards set forth in the Helsinki Declaration of 1975. All patients were treated according to our standard clinical practice. Thus, all patients who were at increased risk for oral dysphagia (OD) were referred to clinical assessment of swallo-wing. Some independent or associated risk factors are conside-red for the development of dysphagia in the ICU: orotracheal intubation for more than 48 hours, tracheostomy, neurological diseases,delirium or another elective clinical condition.
Swallowing assessment in Intensive Care Unit (ICU)
A clinical swallowing assessment was completed under some conditions, based on medical records and report of the multidisciplinary team. The full assessment was performed 24 hours after extubation, if the patient was alert and clinically stable. The full clinical swallowing assessment in ICU of our Institution includes a Preliminary Assessment Protocol (PAP)(20), a Dysphagia Risk Evaluation Protocol (DREP)(19) and an Oral Feeding Transition Protocol (OFTP)(21).
The PAP(20) is an instrument that aims to describe overall aspects of breathing, speech, voice and of the orofacial and cervical structures of individuals undergoing a swallowing evaluation. The purpose of the protocol is to conduct the exa-miner in the decision process of testing different liquid and food consistencies. The protocol also gives support to understanding the pathophysiology of dysphagia.
The clinical measures of the PAP(20) considered for statistical analyses were: diagnosis; vital signs, alertness; tube feeding; orientation status; ability to follow single-step verbal com-mands; oxygen saturation; breathing pattern; dependence on oxygen; speech intelligibility; coordination between breathing and speaking; dysphonia; orofacial motor ability, dentition; gag reflex, cough quality, laryngeal elevation and saliva.
The DREP(19) is a protocol for the early detection of dys-phagia risk. It includes the controlled offer of water and puree volumes. This instrument aims to guide the speech pathologist during the process of identifying and interpreting alterations of the swallowing process. It also characterizes clinical signs that are suggestive of laryngeal penetration or aspiration, the severity of dysphagia and it helps to determine how the case will be conducted. For the statistical analysis the results of pass/ fail and the risk level for dysphagia were considered.
According to this protocol, the classification of dysphagia is based on five levels. The examiner should follow the clinical rationale proposed in each item of the protocol based on the signs presented by the patient. For the classification of dys-phagia, the patient must present at least one sign that classifies his/hers swallowing as different from what is described on the previous level:
- Level I – Normal swallowing: Normal for liquid and pasty food for all of the assessed items. Oral feeding is recom-mended.
aspiration. Oral feeding is recommended, but additional time may be necessary to complete this task.
- Level III – Mild oropharyngeal dysphagia: A swallowing disorder is present; cues are given during the act of swallo-wing. Small diet modifications are necessary; spontaneous and effective cough is present; mild oral alterations are present with adequate compensation.
- Level IV – Mild to moderate oropharyngeal dysphagia: The risk for aspiration is present; however this is reduced with the use of maneuvers and therapeutic techniques. Needs sporadic supervision to perform therapeutic techni-ques; signs of aspiration and food consistency restriction; involuntary cough is weak and voluntary cough is strong. The time spent with feeding is considerably longer and supplementary nutrition is indicated.
- Level V – Moderate oropharyngeal dysphagia: Significant risk for aspiration exists. Oral feeding is supplemented with the use of alternative feeding methods; signs of aspiration for both of the tested food consistencies. The patient is able to eat a few food consistencies using specific therapeutic techniques to minimize possible aspiration and/or to faci-litate swallowing; needs supervision. Involuntary cough is weak or absent.
- Level VI – Moderate to severe oropharyngeal dysphagia: tolerates only one food consistency with supervision at all times; signs of aspiration needing to use clearing strategies; aspiration of two or more food consistencies; absence of involuntary cough; voluntary cough is weak and ineffective. If lung condition is compromised, the suspension of oral feeding is necessary.
- Level VII – Severe oropharyngeal dysphagia: Oral feeding is not possible. Chokes and has difficulty to recover; presence of cyanoses or bronchospasms; silent aspiration for two or more food consistencies; voluntary cough is ineffective; inability to begin the swallowing process.
The OFTP(21) is used for patients who have obtained good scores in the PAP and DREP. The aim of this protocol is to guide the recommendation for oral or non-oral feeding in patients who are at risk for OD. Its methodology incorporates signs and symptoms commonly observed in the clinical practice of clinicians who work with dysphagia. In addition, it provides information regarding oral intake and effectiveness of thera-peutic techniques.
The OFTP(21) is based in the model presented by the American Dietetic Association(22) – the National Dysphagia Diet – that established different levels of food and liquids intake by mouth (Chart 1). For statistical analysis the criteria of pass/fail in each level was adopted, considering the use of therapeutic strategies.
A complete clinical evaluation was conducted in accordance to Figure 1. The instrumental evaluation of swallowing was indicated whenever the results of the protocols were biased.
Data analysis
The Fisher’s Exact Test was used to examine the ability of each single variable of PAP to predict fail in clinical trials of
swallowing. The adopted value of significance was of 0.05. EpiInfo statistical software was used for this analysis.
A descriptive analysis is presented for the results obtained in the DREP and OFTP.
RESULTS
Disposition of patients
A total of 35 patients were referred for clinical swallo-wing assessment. All patients exhibited Glasgow Coma Scale above fourteen points. No patient received tracheostomy during hospitalization. Patients presented a mean age of 54 years (SD=20.1), and 51% were female. Table 1 presents the clinical characteristics of the 35 participants correlated with the prevalence of OD. The dysphagia severity classification is illustrated in Figure 2.
All patients underwent the procedures determined in the PAP and DREP. Sixteen patients failed at least in one of the textures tested in the DREP. The DREP could not be fully completed in 17% of the patients. The main reasons for the interruption of the tests were ineffective airway clearing and nausea.
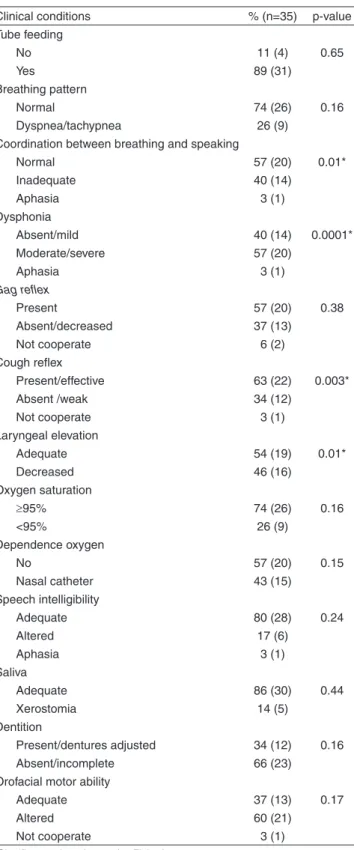
Table 2 shows the results for the Fisher’s Exact Test ap-plied to the correlation between the clinical conditions asses-sed by the PAP(20) and the fail results of the DREP(19) (Table 3), as described in the methods section. For this analysis, only the common items for both protocols were considered. These items are described in the same table, as well as the distribution of the results obtained for the 35 participants. The statistical analysis indicates that the most relevant items
Chart 1. OFTP: levels of food and liquid intake by mouth
Diet level
Level 1: homogenous puree, very cohesive, pudding-like, requiring very little chewing ability. Examples: Mashed fruits, jam, mashed vegetables, and creamy soup.
Level 2: heterogeneous puree, cohesive, moist semisolids food, requiring some chewing. Examples: heterogeneous creamy soup (mixed with noodles or soft vegetables), mixed fruits and vegetables. Exclude: Bread and crackers, unless they moist and mixed with puree.
Level 3: Soft foods that require more chewing ability. Examples: little piece fruits (mango, banana, and papaya), pasta, shredded beef, soft vegetables, and soft bread. Exclude grains, crusty, greens, and another hard chewing food.
Level 4: regular diet. All foods allowed, include any hard food. Examples: raw vegetables, meat, green salad, bread, and grains.
Liquid level
Thin: similar to water in its natural state. Examples: water, juice, tea, milk, and coffee, without thick.
Honey: slightly thickened liquids. Examples: yogurt drinks, some fruit juices (e.g., mango juice) and any other liquid thickened slightly (with thickener or other types of starch).
were: coordination between breathing and speech (p=0.01); presence of dysphonia (p=0.01); involuntary cough (p=0.003) and laryngeal elevation (p=0.01). The results suggest that alterations of these items in the PAP can predict possible fail results in the DREP(15).
The OFTP(21) was not conducted in nine patients (26%). The main reason was the presence of moderate to severe oropharyngeal dysphagia, determined by the DREP(19) (78%). Twenty six patients (74%) completed all protocols. Of these total, 38% were able to eat a regular diet. The remaining 62% failed or could not be tested at all levels. The main reasons that prevented these patients from eating a regular diet were: necessity for compensatory strategies during swallowing (38%),
Figure 1. Full clinical swallowing assessment in the ICU
Table 1. Clinical characteristics and prevalence of OD
Characteristics
OD
Total % (n) No
% (n)
Yes % (n)
Age, years
≤60 50 (8) 50 (8) 45 (16) >60 26 (5) 74 (14) 55 (19)
Etiology of clinical condition
Cardiovascular 75 (3) 25 (1) 11 (4)
Gastrointestinal 50 (2) 50 (2) 11 (4)
Neurological 33 (2) 67 (4) 17 (6)
Pulmonary 30 (3) 70 (7) 29 (10)
Infection 50 (1) 50 (1) 6 (2)
Other clinical conditions 22 (2) 78 (7) 26 (9)
Referred Pattern
Orotracheal intubation ≥48h 35 (9) 65 (17) 74 (26)
Neurological condition 33 (2) 67 (4) 17 (6)
Delirium 67 (2) 33 (1) 9 (3)
Total 37 (13) 63 (22)* 100 (35)
* Prevalence of OD in this population
Note: OD = oropharyngeal dysfagia
absence of teeth (38%), reduced alertness (13%), dyspnea (6%), and odynophagia (6%). The OFTP was not conducted in nine patients (26%). The most important reason was the presence of moderate-severe OD during the conduction of the DREP (78%). Table 3 shows the results of full clinical evaluation of swallowing in the ICU.
Table 2. Clinical conditions in the PAP
Clinical conditions % (n=35) p-value Tube feeding
No 11 (4) 0.65
Yes 89 (31)
Breathing pattern
Normal 74 (26) 0.16
Dyspnea/tachypnea 26 (9) Coordination between breathing and speaking
Normal 57 (20) 0.01*
Inadequate 40 (14)
Aphasia 3 (1)
Dysphonia
Absent/mild 40 (14) 0.0001* Moderate/severe 57 (20)
Aphasia 3 (1)
Gag reflex
Present 57 (20) 0.38
Absent/decreased 37 (13)
Not cooperate 6 (2)
Cough reflex
Present/effective 63 (22) 0.003*
Absent /weak 34 (12)
Not cooperate 3 (1)
Laryngeal elevation
Adequate 54 (19) 0.01*
Decreased 46 (16)
Oxygen saturation
≥95% 74 (26) 0.16
<95% 26 (9)
Dependence oxygen
No 57 (20) 0.15
Nasal catheter 43 (15) Speech intelligibility
Adequate 80 (28) 0.24
Altered 17 (6)
Aphasia 3 (1)
Saliva
Adequate 86 (30) 0.44
Xerostomia 14 (5)
Dentition
Present/dentures adjusted 34 (12) 0.16 Absent/incomplete 66 (23)
Orofacial motor ability
Adequate 37 (13) 0.17
Altered 60 (21)
Not cooperate 3 (1)
Significant values (p<0.05) – Fisher’s exact test
Note: PAP = Preliminary Assessment Protocol
DISCUSSION
Until this moment there is no universally accepted standard OD full evaluation protocol(15) For this study, a sequence of be-dside protocols comprising clinical measures already described in the literature were used(12).
Traditionally, videofluoroscopy has been considered the gold standard for swallowing evaluation(17). However, the clinical utility of this test is compromised by the need to trans-port often fairly ill patients to the radiology department and the requirement for specialized equipment and personnel that are not readily available in many hospitals(24). When looking at developing countries, the prolonged intensive medical and nursing care required by many patients places extra demands on an already stretched healthcare budget(5,17,18,25).
Cervical auscultation is increasingly being used to supple-ment clinical swallowing assesssupple-ment. The sounds associated with swallowing have been investigated using accelerometers and microphones for acoustic characteristics and possible prediction of aspiration(10,14,17,26,27). The use of cervical aus-cultation varies in its reported reliability, and validity in terms of comparison to videofluoroscopic swallow study (VFSS)(17,25,27,28). However, VFSS itself has poor reliability for intra- and interjudge rating.
The literature shows that an average of 50% of patients submitted to orotracheal intubation have OD, especially in elderly(29). A lot of emphasis has been placed on the early identification and best management of OD in acute stroke patients(1,14). However, the situation differs significantly when considering ICU patients who require specific skills of profes-sionals experienced in swallowing rehabilitation(5).
Authors(30) revealed some clinical indicators significantly related to aspiration in stroke patients: dysphonia, dysarthria, abnormal gag reflex, abnormal volitional cough, cough after swallow, and vocal changes after swallow. Other authors(26) reported that reduced laryngeal elevation on trial swallows was identified correctly in 70% of the patients classified as having or not a pharyngeal stage disorder. The coordination between breathing and speaking was not examined in these studies. However, incoordination between respiratory and deglutition functions have been described as an increased risk for aspiration(29,30).
Table 3. Results of full clinical swallowing assessment in the ICU
Assessment protocols Pass % (n)
Fail % (n)
Pass with intervention technique
% (n)
Fail with intervention technique
% (n)
Not performed % (n)
PAP 100 (35) 0 (0) - -
-DREP
Water 60 (21) 40 (14) - - 0 (0)
Puree 69 (24) 26 (9) - - 5 (2)
PITA
Level 1 57 (20) 0 (0) 6 (2) 9 (3) 28 (10)
Level 2 11 (4) 6 (2) 0 (0) 0 (0) 83 (29)
Level 3 14 (5) 3 (1) 0 (0) 0 (0) 83 (29)
Level 4 29 (10) 3 (1) 0 (0) 0 (0) 68 (24)
Thin liquids 43 (15) 9 (3) 11 (4) 11 (4) 26 (09)
Note: PAP = Preliminary Assessment Protocol; DREP = Dysphagia Risk Evaluation Protocol; OFTP = Oral Feeding Transition Protocol
and therefore need specific training for the correct application. When looking at developing countries, the prolonged intensi-ve medical and nursing care required by many patients place extra demands on an already stretched healthcare budget. Intervention by a speech pathologist could mean that time in the ICU would be reduced as well as the number of re-admissions due to com-plication(29,30). Early identification of swallowing disorders is overriding to reduce morbidity in this high risk population(10).
CONCLUSION
The results indicate a prevalence of 63% of OD in a clinical intensive care unit. Patients who are submitted to orotracheal in-tubation were very frequently referred in this setting. However, our findings should be confirmed in further studies of larger cohorts by extensive repetition of the current procedures. The practice with standardized protocols adds an important option for the management of oropharyngeal dysphagia in intensive care unit.
* ARP was responsible for data collection and tabulation; DPM contributed with data collection and tabulation, and supervised data collection; FCS monitored data collection and contributed com data analysis; CRFA was responsible for the study’s project and design, and for general supervision of the execution and manuscript elaboration stages.
REFERENCES
1. Cichero JAY, Heaton S, Bassett L. Triaging dysphagia: nurse screening for dysphagia in an acute hospital. J Clin Nurs. 2009 Jun;18(11):1649-59. 2. Odderson IR, Keaton JC, McKenna BS. Swallow management in patients
on an acute stroke pathway: quality is cost effective. Arch Phys Med Rehabil. 1995 Dec;76(12):1130-3.
3. Lin LC, Wu SC, Chen HS, Wang TG, Chen MY. Prevalence of impaired swallowing in institutionalized older people in Taiwan. J Am Geriatr Soc. 2002 Jun;50(6)1118-23.
4. Groher ME, Bukatman R. The prevalence of swallowing disorders in two teaching hospitals. Dysphagia. 1986;1(1):3-6.
5. Schindler A, Vincon E, Grosso E, Miletto AM, Di Rosa R, Schindler O. Rehabilitative management of oropharyngeal dysphagia in acute care settings: data from a large Italian teaching hospital. Dysphagia. 2008 Sep;23(3):230-6.
6. Leder SB, Cohn SM, Moller BA. Fiberoptic endoscopic documentation of the high incidence of aspiration following extubation in critically ill trauma patients. Dysphagia. 1998;13(4):208-12.
7. Barquist E, Brown M, Cohn S, Lundy D, Jackowski J. Postextubation fiberoptic endoscopic evaluation of swallowing after prolonged endotracheal intubation: a randomized, prospective trial. Crit Care Med. 2001;29(9):1710-13.
8. Partik B, Pokieser P, Schima W, Schober E, Stadler A, Eisenhuber E, et al. Videofluoroscopy of swallowing in symptomatic patients who have undergone longterm intubation. AJR Am J Roentgenol. 2000 May;174(5):1409-12.
9. Kozlow JH, Berenholtz SM, Garret E, Dorman T, Pronovost PJ. Epidemiology and impact of aspiration pneumonia in patients undergoing surgery in Maryland, 1999-2000. Crit Care Med. 2003 Jul; 31(7):1930-7. 10. Medeiros GC, Andrade CRF. Disfagia orofaríngea em pacientes
submetidos à intubação orotraqueal prolongada em UTIs. [dissertação] São Paulo: Faculdade de Medicina, Universidade de São Paulo; 2012. 11. Hafner G, Neuhuber A, Hirtenfelder S, Schmedler B, Eckel HE.
Fiberoptic endoscopic evaluation of swallowing in intensive care unit patients. Eur Arch Otorhinolaryngol. 2008 Apr;265(4):441-6.
12. Edelman DA, Sheehy-Deardorff DA, White MT. Bedside assessment of swallowing is predictive of an abnormal barium swallow examination. J Burn Care Res. 2008 Jan-Feb;29(1):89-96.
13. Baumgartner CA, Bewyer E, Bruner D. Management of communication and swallowing in intensive care: the role of the speech pathologist. AACN Adv Crit Care. 2008 Oct-Dec;19(4):433-43.
14. Bours GJ, Speyer R, Lemmens J, Limburg M, Wit R. Bedside screening tests vs. videofluoroscopy or fibreroptic endoscopic evaluation of swallowing to detect dysphagia in patients with neurological disorders: systematic review. J Adv Nurs. 2009 Mar;65(3):477-93.
15. Leder SB, Suiter DM, Warner HL. Answering orientation questions and following single-step verbal commands: effect on aspiration status. Dysphagia. 2009 Sep;24(3):290-5.
16. Mann G. Effectiveness and efficiency: state of the art in dysphagia rehabilitation after stroke. Aust Comm Quarterly. 1996;4:25-7. 17. Carnaby-Mann G, Lenius K. The bedside examination in dysphagia. Phys
Med Rehabil Clin N Am. 2008 Nov;19(4):747-68.
18. Mathers-Schmidt BA, Kurlinski M. Dysphagia evaluation practices: inconsistencies in clinical assessment and instrumental examination decision-making. Dysphagia. 2003;18(2):114-25.
19. Padovani AR, Moraes DP, Mangilli LD, Andrade CRF. Protocolo de Avaliação do Risco para a Disfagia (PARD). In: Andrade CRF, Limongi SCO (Org). Disfagia: prática baseada em evidências. São Paulo: Sarvier; 2012. p. 62-73.
20. Mangilli LD, Moraes DP, Medeiros GC. Protocolo de avaliação fonoaudiológica preliminar. In: Andrade CRF, Limongi SCO (Org). Disfagia: prática baseada em evidências. São Paulo: Sarvier; 2012. p. 45-61.
de introdução e transição da alimentação por via oral (PITA). In: Andrade CRF, Limongi SCO (Org). Disfagia: prática baseada em evidências. São Paulo: Sarvier; 2012; p. 74-85.
22. McCallum SL. The national dysphagia diet: implementation at a regional rehabilitation center and hospital system. J Am Diet Assoc 2003;103(3):381-4.
23. Tesdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974 Jul 13;2(7872):81-4.
24. ASHA: American Speech-Language-Hearing Association [Internet] 2000 Clinical indicators for instrumental assessment of dysphagia [Guidelines]. ASHA Practice Policy. Available from: http://www.asha. org/policy/GL2000-00047.htm
25. Ramsey DJ, Smithard DG, Kalra L. Early assessments of dysphagia and aspiration risk in acute stroke patients. Stroke. 2003;34(5):1252-7.
26. Logemann JA, Veis S, Colangelo L. A screening procedure for oropharyngeal dysphagia. Dysphagia. 1999;14(1):44-51.
27. Pettigrew CM, O’Toole C. Dysphagia evaluation practices of speech and language therapists in Ireland: clinical assessment and instrumental examination decision-making. Dysphagia. 2007 Jul;22(3):235-44. 28. Bateman C, Leslie P, Drinnan MJ. Adult dysphagia assessment in the
UK and Ireland: are SLTs assessing the same factors? Dysphagia. 2007 Jul;22(3):174-86.
29. El Solh A, Okada M, Bhat A, Pietrantoni C. Swallowing disorders post orotracheal intubation in the elderly. Intensive Care Med. 2003 Sep;29(9):1451-5. Epub 2003 Aug 2.