Biocompatibility assessment of calcium-silicate based endodontic sealers: in vitro studies
Texto
Imagem

Documentos relacionados
O tratamento com ayahuasca na maior dose (fêmeas) aumentou significativamente os níveis de BDNF na formação hipocampal em relação ao peso total do encéfalo. No grupo
Este trabalho teve como objetivos mostrar através de revisão bibliográfica a agregação de Indicadores ambientais, a realidade das praias urbanas de Fortaleza, utilizando o
The aim of this study was to evaluate the physicochemical properties and the apical dentin bond strength of the tricalcium silicate-based Biodentine in comparison to white MTA
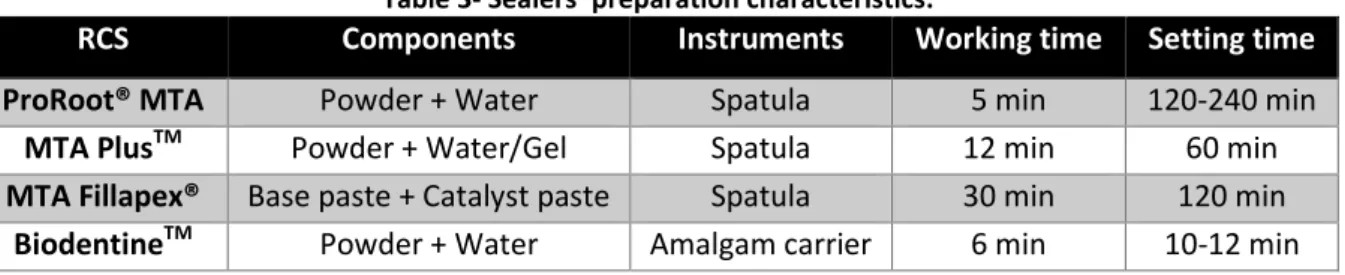
In our study, it was used materials (experimental calcium- based root canal sealers based on MTA and salicylate resins) with different chemical composition, structure, and physical
Table 1 presents the annual number of students enrolled on Portuguese higher education by subsystem and type of education from the academic year of 2006/07 (first year
Isso sugere que um processo de descentralização dos poderes dentro de um sistema federal não implica automaticamente em desconcentração do poder econômico, indicando que
In this study, two calcium silicate MTA based cements, each containing a different radiopacifying agent alternative to bismuth oxide, were compared with conventional MTA
Mas uma coisa sabe, tem de ficar em casa de quarentena para se proteger a si, à família, aos amigos, a todos os por- tugueses e a todas as pessoas do mundo inteirinho, porque o
