REVIEW
Association of polymorphism +874 A/T of interferon-γ
and susceptibility to the development of tuberculosis:
meta-analysis
A. C. de Albuquerque&L. Q. Rocha&
A. H. de Morais Batista&A. B. Teixeira&
D. B. dos Santos&N. A. P. Nogueira
Received: 6 February 2012 / Accepted: 15 May 2012 / Published online: 9 June 2012
#Springer-Verlag 2012
Abstract The immune defence againstMycobacterium
tu-berculosis is complex and involves multiple interacting cells. Studies in subjects with polymorphisms in genes for IFN or its receptor gene evaluate their relationship with mycobacterium infections. The purpose of this study was to analyze the evidence of the effect of polymorphism +874 A/T from interferon-γon the occurrence of tuberculosis. We
per-formed a meta-analysis of studies published between June 2002 and April 2012. The articles analyzed assessed the relationship between the polymorphism +874 A/T and the development of tuberculosis. The meta-analysis was per-formed with a random effect model, considering the hetero-geneity among studies. Genotype TT showed a protective effect (OR, 0.77; 95% CI00.67–0.88) while genotype AA
may be associated with increased susceptibility to developing tuberculosis (OR, 1.51; 95% CI01.38–1.65). In relation to
alleles, we can verify that the A allele is related to the devel-opment of tuberculosis (OR, 1.56; 95% CI01.42–1.71). This
information reinforces the importance of host genetics in the
development of infectious diseases. Studies in this area can result in the promotion of new and more accurate genetic markers.
Introduction
Tuberculosis is a chronic infectious disease that occurs world-wide. In 1993, the World Health Organization (WHO) de-scribed the disease as a global emergency and it is currently responsible for the death of thousands of persons around the world [1]. About 8 million new cases and nearly 1.8 million deaths attributable to TB occur each year [1]. Brazil is the 18th ranked country in the world in cases of tuberculosis, as esti-mated by the WHO (with an incidence rate of 48 per 100,000 in 2007) [2]. In many populations, this situation is aggravated by an increased prevalence of virus infection by human im-munodeficiency virus (HIV) [3].
The immune defence againstMycobacterium tuberculosis
is complex and involves the interaction between cells T CD4, lymphocytes T CD8, macrophages and monocytes, along with the production of cytokines, interferon-γ(IFN-γ) and tumour
necrosis factor (TNF) [4]. A growing body of evidence is presented to define the role of genetics in the host’s
suscepti-bility to developing infections [5]. Owing to the nature of this type of disease and the complex immune response after expo-sure, it is presumed that many host genes play an important role in determining susceptibility to the disease [6,7].
Among the evidence related to the function of human genetics in the disease development are the twin studies that indicate that TB rates among monozygotic twins are more than twice as high as the rate of dizygotic and genotypic differences demonstrated between different ethnic groups [8,9].
A. C. de Albuquerque
:
L. Q. Rocha:
A. H. de Morais Batista:
A. B. Teixeira
:
N. A. P. NogueiraResearch Laboratory of Applied Microbiology, Federal University of Ceará,
Ceará, Fortaleza, Brazil
D. B. dos Santos
Center for Health Sciences,
Federal Universityof Recôncavo da Bahia, Santo Antônio de Jesus, Salvador, Bahia, Brazil
A. C. de Albuquerque (*)
Department of Clinical and Toxicological Analysis, Federal University of Ceará,
Capitão Francisco Pedro, 1210—Porangabussu(Fortaleza, Ceará,
Brazil
According to the Manual of Recommendations for Tu-berculosis Control in Brazil, a factor among the genetic aspects of risk are single-base polymorphisms in genes encoding substances involved in the defence of the body, mainly cytokines and their receptors [10]. Studies in sub-jects with polymorphisms in genes for IFN or its receptor gene evaluate their relationship with mycobacterium infec-tions [11,12]. In addition, some studies have linked the low production of IFN and active tuberculosis [13].
The most significant single-base polymorphism found in the gene for IFN-γis presented as polymorphism +874 A/T
located in intron I, which binds to the site of transcription factor NFkB [14]. Studies showed that the variant allele +874 A is related to low production of IFN-γ[14].
In the last decade, numerous studies about the association between the polymorphism +874 A/T of interferon-γ and
tuberculosis emerged. In 2008, a meta-analysis on the subject was published, which analyzed 13 studies published up to August 2007 [15]. This article also examined the polymor-phisms interleukin-10−1082G/A and tumour necrosis factor α −308G/A, which evaluated only the protective effect of
allele T.
The meta-analysis extracts information from existing data through the union of the results of several studies and the application of statistical techniques can synthesize their find-ings or draw a new conclusion [16]. The purpose of this study was to analyze the evidence of the effect of polymorphism +874 A/T interferon-γon the occurrence of tuberculosis.
Materials and methods
Identification and selection of articles
This review was restricted to case–control articles published
comparing polymorphism +874 A/T interferon-γ with the
development of active tuberculosis, according to the method-ology described in the PRISMA Statement [17]. These studies were identified by searching the PubMed database for publi-cations from June 2002 to April 2012. Despite not having search language restrictions, only English language articles were selected. The keywords used were "tuberculosis", "poly-morphism", "interferon", "susceptibility" and "874". The ref-erence lists of identified publications were searched. We selected 19 articles that analyzed individuals affected with both pulmonary and extrapulmonary tuberculosis in selected health centers or in the community. Only studies that provided sufficient data for statistical calculations were chosen.
Quality evaluation
These articles were evaluated and rated according to method-ological criteria proposed by Downs and Black [18], which
were applicable to the design of articles to assess their quality. These criteria assess the quality of information, internal valid-ity (bias and confounding), the external validvalid-ity and the abilvalid-ity to detect a significant effect of the study.
Inclusion and exclusion criteria
We included studies that linked polymorphism +874 A/T with susceptibility to developing tuberculosis and that provided sufficient data for statistical analysis. In the 11 articles that reported the relationship of the polymorphism of another gene to susceptibility to tuberculosis was considered the only data on the polymorphism of interferon-γ. We included two studies
that presented derivation of the Hardy–Weinberg equilibrium,
whereas the inclusion of these items in a previous meta-analysis did not alter the results significantly [15, 19, 20]. We excluded articles that were reviews or meta-analyses, articles that related polymorphism +874 A/T to other diseases and studies that related tuberculosis to the polymorphism of other genes.
Data collected
In the extraction of data, the following information was collected: first author and year of publication, distribution of genotypes and alleles for each polymorphism between cases and controls, whether the tuberculosis studied in the article was only pulmonary or pulmonary and extrapulmo-nary, the presence or absence of HIV cases and controls and the region of origin of the article.
Statistical analysis
The statistical package Stata version 9.0 was used in the data analysis. The Q test was used to assess heterogeneity be-tween studies and, in case of heterogeneity, we used the random effects model. We then calculated the OR and CI, confidence level of 95% for each genotype first and then the combination of alleles, through the fixed effect models (FEM) and random effects (MEA). The group reference was the AT genotype. We use the dominant model to ana-lyze the effect of genetic polymorphisms of IFNG on the risk of TB. We used the Q test for the calculation of statis-tical heterogeneity, considering the value of thep>0.1 level of significance to accept that the results are similar.
Results
identified, there were more studies with other combinations of words in order to refine the search. Initially, research was carried out with the words tuberculosis, polymorphism and interferon; we found 79 articles and selected 21. In the following search, the word susceptibility was added, 61 studies were identified and 22 selected. In the latest survey, the number of the position of the polymorphism (874) was added and 19 articles were found. Among these, 14 were chosen. The result of these three searches was a total of 23 articles that linked the polymorphism with the development of tuberculosis. After analyzing the selected articles, 4 stud-ies were excluded: 3 did not provide the data needed for statistical analysis and the other dealt with patients with tuberculosis associated with silicosis, thus resulting in a total of 19 studies.
Table1 describes the 19 articles (19 studies) that were included in the meta-analysis. Of the studies analyzed, in 3 the cases were of European origin, 4 African, 6 Asian, 4 Americans and 2 Eurasian (Turkish). In studies conducted in Canada and the UAE, different ethnic groups were analyzed together, considering the large number of articles evaluated [21, 22]. Different studies have looked at cases from both health centres (73.68%) and the community (10.52%) and
others did not specify this information (15.80%). In articles written in West Africa and Malawi, they make it clear that both HIV-positive and -negative subjects were used, or in other articles the author uses only HIV-negative subjects or did not cite the fact [23, 24]. Two studies assessed the polymorphism in children [25,26].
Considering the high value found for the heterogene-ity in both tests (TT genotype, 74.80%, and AA geno-type, 85.90%), we used the random effect model for data analysis. The results described in Fig. 2 show a greater susceptibility to developing tuberculosis in indi-viduals with the AA genotype (OR, 1.51; 95% CI01.38–
1.65). Figure 3 shows the protective role that provides individuals with the TT genotype (OR, 0.77; 95% CI0
0.67–0.88). Besides these aspects, a predisposition to
the disease may also be associated with the presence of an A allele through the analysis of individuals’ heterozygous AT genotype shown in Fig. 4 (OR, 0.76; 95% CI00.70–
0.83). Of the 19 articles evaluated, only 11 provided sufficient data for a statistical analysis of the prevalence of alleles A and T. According to Fig. 5, the role of the A allele in the development course of tuberculosis is clear (OR, 1.56; 95% CI01.42–1.71).
19 articles were included in the meta-analysis
We excluded four articles: one relates polymorphism with tuberculosis with silicosis and another did not provide
sufficient data 2199 articles were found with the
combination of tuberculosis and polymorphism
59 articles were found with the combination tuberculosis susceptibility
polymorphism, interferon 79 articles were found with the
combination tuberculosis, polymorphism and interferon
19 articles were found with the combination tuberculosis, susceptibility,
polymorphism, interferon, 874
We selected 20 articles. Excluded: 6 general, 6 other issues, 6 other diseases,
3 other diseases with other genes, 18 other genes
We selected 21articles. Excluded: 9 general, 14 other subjects,3 other diseases, 6 other diseases with other
genes, 26 other genes
14 articles were selected. Excluded: 3 other diseases, 1 other subject, 1other
genes
We analyzed 23 articles
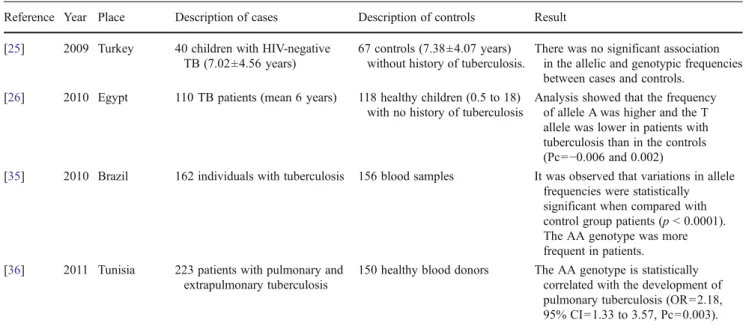
Table 1 Studies of the association of polymorphism +874 A/T of interferon-γand susceptibility to tuberculosis
Reference Year Place Description of cases Description of controls Result
[11] 2002 Italy 45 patients, the Health Unit (35–60 years)
97 healthy subjects matched for age and sex
Results showed an association between the TT and +874 homozygote, a reduced frequency of pulmonary tuberculosis conical (p00.04521) [31] 2003 South Africa 313 patients with pulmonary
tuberculosis and tuberculous meningitis
235 controls with more than 15 years with no history of tuberculosis
Statistical analysis showed a significant association of both the genotype (p00.017) and allele (p00.0055) [32] 2003 Spain 113 newly diagnosed patients
(PPD-positive and -negative).
207 close contacts (PPD ±). 100 healthy donors (PPD ±).
Individuals with AA homozygote are 3.75 times more likely to develop tuberculosis. (OR03.75, 95% CI02.26 to 6.23,p00.0017). [24] 2004 Malawi 451 cases, HIV-positive
and -negative
703 controls This SNP was not associated with TB susceptibility in Malawi. [19] 2005 Croatia 253 patients from a clinic,
71.6% men (48.5±12 years)
519 controls, 78.6 % men (42.4±9 years)
Patients and controls had similar distributions, and the genotype of the heterozygote frequency was higher (50.4%)
[33] 2005 Hong Kong 385 patients pulmonary and extrapulmonary TB
Controls 451 blood donors of the Red Cross (29±10 years)
The frequency of AA genotype is significantly higher in patients (p<0.001, OR03.79, 95% CI01.93 to 7.45) [22] 2006 United States 240 African–Americans,
161 Caucasians, 319 Hispanics with pulmonary and extrapulmonary tuberculosis
174 African– Americans, 64 Caucasians and 98 Hispanics with no history of tuberculosis
The A allele was more common among African–Americans and Hispanics than in Caucasians. No significant difference was observed between cases and controls in any of the three ethnic groups. [29] 2006 Turkey 361 patients with various
forms of tuberculosis.
115 healthy subjects with no history of tuberculosis.
It has been shown that a TT genotype decreases the risk of developing pulmonary TB in 30%, while the AA genotype increases the risk 1.41 times. [12] 2006 Africa - West 682 cases. Both cases of
HIV + / - were included
619 controls The AA genotype was found in a greater quantity in cases, but not statistically significantly, stopping. [13] 2006 India 129 patients with pulmonary
tuberculosis in the early stage of the disease (36±12.3 years)
127 healthy subjects (30±9.2 years)
The frequencies of IFN three genotypes (AA, A and TT) and allele frequencies did not differ significantly between cases and controls.
[27] 2007 South Korea 80 patients with pulmonary tuberculosis (16 to 75 years)
80 unrelated healthy volunteers (range 20-48 years).
There was no significant difference in the frequency distribution of alleles between patients and controls. [37] 2007 China 301 patients with pulmonary and
extrapulmonary tuberculosis
310 controls, the same ethnic Han
The A allele was more representative in tuberculosis (p00.0023). The AA genotype was associated with tuberculosis (OR01.98, 95% CI01.08 to 3.63,p00.035) [20] 2007 Brazil 93 patients with pulmonary and
extrapulmonary tuberculosis
266 health care professionals asymptomatic (PPD + / -)
Considering all the controls (PPD positive and negative), there was an association between the presence of the A allele and the development of tuberculosis.
[21] 2008 Canada For ethnicity Dené, 61 patients and Cree, 42 patients
91 Caucasian controls with mean age of 52 years.
Compared with Caucasians, both Cree and Dene had a higher frequency of allele A.
[34] 2009 Pakistan 188 patients with pulmonary and extrapulmonary tuberculosis
Discussion
The study identified through the meta-analysis that the AA genotype and A allele are related to the development of tuberculosis, while the TT genotype and T allele are at-tached to the protective effect against the disease. The development of tuberculosis is caused by the interaction of several factors, be they related to the environment, host or
microorganism. According to the World Health Organiza-tion, elements that alter host immunity (infectious diseases like HIV, low weight, immunosuppressive therapy) and other conditions such as a state of confinement, alcohol and smoking increase the likelihood of a person infected withM. tuberculosisdeveloping the disease [1]. The genetic profile of an individual can certainly determine the occur-rence of active disease. One can find literature evidence
Table 1 (continued)
Reference Year Place Description of cases Description of controls Result
[25] 2009 Turkey 40 children with HIV-negative TB (7.02±4.56 years)
67 controls (7.38±4.07 years) without history of tuberculosis.
There was no significant association in the allelic and genotypic frequencies between cases and controls.
[26] 2010 Egypt 110 TB patients (mean 6 years) 118 healthy children (0.5 to 18) with no history of tuberculosis
Analysis showed that the frequency of allele A was higher and the T allele was lower in patients with tuberculosis than in the controls (Pc0−0.006 and 0.002)
[35] 2010 Brazil 162 individuals with tuberculosis 156 blood samples It was observed that variations in allele frequencies were statistically significant when compared with control group patients (p< 0.0001). The AA genotype was more frequent in patients. [36] 2011 Tunisia 223 patients with pulmonary and
extrapulmonary tuberculosis
150 healthy blood donors The AA genotype is statistically correlated with the development of pulmonary tuberculosis (OR02.18, 95% CI01.33 to 3.57, Pc00.003).
Overall (I-squared = 85.9%, p = 0.000) Shiping Ding et al (2007) M. Vidyarani et al (2006)
Lucia H.L.V.Amim et al (2007) Manda Rossouw et al (2003)
Antonio C.R.Vallinnoto et al (2010) Ambreen Ansari et al (2009) Dolores Lopez-Maderuelo et al (2003)
Jodene Fitness et al (2004) ID
Huseyin Onay et al (2009) D. Lio et al (2002)
W alid Ben Selma et al (2011) Jung Hye Hwang et al (2007)
Linda A. Larcombe et al (2008) Nilgün Sallakci et al (2006) G. E. Etokebe et al (2005)
A. Moran et al (2006)
Y. M. Mosaad et al (2010) HW Tso et al (2005)
Graham S.Cooke (2006) Study
1.51 (1.38, 1.65) 1.59 (1.15, 2.20) 1.17 (0.72, 1.92)
1.91 (1.18, 3.08) 1.64 (1.16, 2.30)
3.22 (2.03, 5.13) 0.80 (0.52, 1.21) 2.71 (1.54, 4.75)
1.06 (0.82, 1.36) OR (95% CI)
1.00 (0.39, 2.52) 0.93 (0.41, 2.11)
2.09 (1.34, 3.26) 1.68 (0.78, 3.60)
12.34 (6.24, 24.41) 1.51 (0.95, 2.40) 1.03 (0.74, 1.46)
0.95 (0.73, 1.23)
3.65 (1.39, 9.58) 3.49 (2.58, 4.72)
1.18 (0.92, 1.50)
100.00 7.16 3.61
3.00 6.36
2.47 6.09 1.83
14.60 W eight
1.10 1.48
3.42 1.28
0.58 3.73 7.98
14.43
0.60 5.72
14.55 %
1.51 (1.38, 1.65) 1.59 (1.15, 2.20) 1.17 (0.72, 1.92)
1.91 (1.18, 3.08) 1.64 (1.16, 2.30)
3.22 (2.03, 5.13) 0.80 (0.52, 1.21) 2.71 (1.54, 4.75)
1.06 (0.82, 1.36) OR (95% CI)
1.00 (0.39, 2.52) 0.93 (0.41, 2.11)
2.09 (1.34, 3.26) 1.68 (0.78, 3.60)
12.34 (6.24, 24.41) 1.51 (0.95, 2.40) 1.03 (0.74, 1.46)
0.95 (0.73, 1.23)
3.65 (1.39, 9.58) 3.49 (2.58, 4.72)
1.18 (0.92, 1.50)
100.00 7.16 3.61
3.00 6.36
2.47 6.09 1.83
14.60 W eight
1.10 1.48
3.42 1.28
0.58 3.73 7.98
14.43
0.60 5.72
14.55 %
1
.041 24.4
Fig. 2 Meta-analysis of the association between
tuberculosis and polymorphism +874 AA genotype of
interferon-γ(number of cases
supporting the role of genetics in the development of tuber-culosis [5–7]. The meta-analysis evaluated the allelic and
genotypic frequencies of the IFNG gene (874 A/T) among patients with tuberculosis and a healthy control group in 19 articles, this type of analysis being classified as a case–control
study. We assessed the following aspects: the protective effect of the TT genotype and T allele and increased susceptibility to developing tuberculosis in individuals with genotype AA.
Among the studies analyzed, 7 (36.84%) did not show in their results a significant association between the
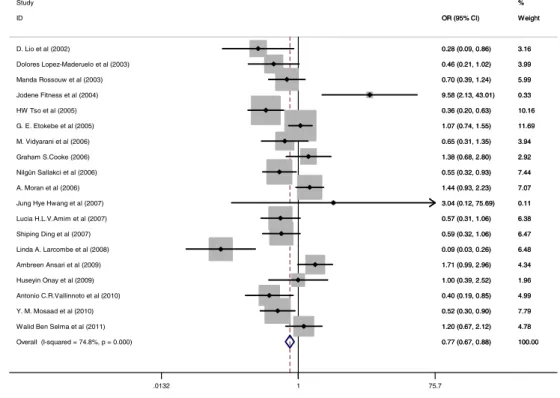
polymor-Overall (I-squared = 74.8%, p = 0.000) Antonio C.R.Vallinnoto et al (2010) Graham S.Cooke (2006)
Walid Ben Selma et al (2011) Ambreen Ansari et al (2009) Lucia H.L.V.Amim et al (2007) M. Vidyarani et al (2006)
Linda A. Larcombe et al (2008)
Huseyin Onay et al (2009) Manda Rossouw et al (2003) D. Lio et al (2002)
G. E. Etokebe et al (2005)
Nilgün Sallakci et al (2006) Jodene Fitness et al (2004)
Shiping Ding et al (2007)
Y. M. Mosaad et al (2010) A. Moran et al (2006) ID
Jung Hye Hwang et al (2007) Dolores Lopez-Maderuelo et al (2003)
HW Tso et al (2005) Study
0.77 (0.67, 0.88) 0.40 (0.19, 0.85) 1.38 (0.68, 2.80)
1.20 (0.67, 2.12) 1.71 (0.99, 2.96) 0.57 (0.31, 1.06) 0.65 (0.31, 1.35)
0.09 (0.03, 0.26)
1.00 (0.39, 2.52) 0.70 (0.39, 1.24) 0.28 (0.09, 0.86)
1.07 (0.74, 1.55)
0.55 (0.32, 0.93) 9.58 (2.13, 43.01)
0.59 (0.32, 1.06)
0.52 (0.30, 0.90) 1.44 (0.93, 2.23) OR (95% CI)
3.04 (0.12, 75.69) 0.46 (0.21, 1.02)
0.36 (0.20, 0.63)
100.00 4.99 2.92 4.78 4.34 6.38 3.94 6.48 1.96 5.99 3.16 11.69 7.44 0.33 6.47 7.79 7.07 Weight 0.11 3.99 10.16 %
0.77 (0.67, 0.88) 0.40 (0.19, 0.85) 1.38 (0.68, 2.80)
1.20 (0.67, 2.12) 1.71 (0.99, 2.96) 0.57 (0.31, 1.06) 0.65 (0.31, 1.35)
0.09 (0.03, 0.26)
1.00 (0.39, 2.52) 0.70 (0.39, 1.24) 0.28 (0.09, 0.86)
1.07 (0.74, 1.55)
0.55 (0.32, 0.93) 9.58 (2.13, 43.01)
0.59 (0.32, 1.06)
0.52 (0.30, 0.90) 1.44 (0.93, 2.23) OR (95% CI)
3.04 (0.12, 75.69) 0.46 (0.21, 1.02)
0.36 (0.20, 0.63)
100.00 4.99 2.92 4.78 4.34 6.38 3.94 6.48 1.96 5.99 3.16 11.69 7.44 0.33 6.47 7.79 7.07 Weight 0.11 3.99 10.16 % 1 .0132 75.7
Fig. 3 Odds ratios for the results of the TT genotype (number of cases with the TT genotype)
Overall (I-squared = 63.9%, p = 0.000) Study
Lucia H.L.V.Amim et al (2007)
Ambreen Ansari et al (2009) G. E. Etokebe et al (2005) ID
Y. M. Mosaad et al (2010) Nilgün Sallakci et al (2006)
Walid Ben Selma et al (2011) Jung Hye Hwang et al (2007) Jodene Fitness et al (2004)
Huseyin Onay et al (2009) A. Moran et al (2006) Manda Rossouw et al (2003)
Shiping Ding et al (2007) Graham S.Cooke (2006) M. Vidyarani et al (2006) HW Tso et al (2005)
Linda A. Larcombe et al (2008) Dolores Lopez-Maderuelo et al (2003) D. Lio et al (2002)
Antonio C.R.Vallinnoto et al (2010)
0.76 (0.70, 0.83) 0.74 (0.44, 1.26)
0.92 (0.61, 1.38) 0.78 (0.58, 1.06) OR (95% CI)
1.16 (0.69, 1.95) 1.00 (0.66, 1.52)
0.46 (0.30, 0.70) 0.55 (0.25, 1.18) 0.93 (0.72, 1.21)
1.26 (0.58, 2.74) 0.92 (0.71, 1.21) 0.68 (0.48, 0.96)
0.72 (0.51, 1.01) 0.81 (0.63, 1.04) 1.04 (0.63, 1.71) 0.54 (0.40, 0.73)
0.25 (0.13, 0.48) 0.55 (0.32, 0.95) 2.13 (1.02, 4.44)
0.45 (0.29, 0.71)
100.00 % 2.90 4.23 8.33 Weight 2.29 3.80 5.54 1.53 10.47 0.99 9.70 6.57 6.89 11.64 2.65 10.51 3.20 2.98 0.86 4.90
0.76 (0.70, 0.83) 0.74 (0.44, 1.26)
0.92 (0.61, 1.38) 0.78 (0.58, 1.06) OR (95% CI)
1.16 (0.69, 1.95) 1.00 (0.66, 1.52)
0.46 (0.30, 0.70) 0.55 (0.25, 1.18) 0.93 (0.72, 1.21)
1.26 (0.58, 2.74) 0.92 (0.71, 1.21) 0.68 (0.48, 0.96)
0.72 (0.51, 1.01) 0.81 (0.63, 1.04) 1.04 (0.63, 1.71) 0.54 (0.40, 0.73)
0.25 (0.13, 0.48) 0.55 (0.32, 0.95) 2.13 (1.02, 4.44)
0.45 (0.29, 0.71)
100.00 % 2.90 4.23 8.33 Weight 2.29 3.80 5.54 1.53 10.47 0.99 9.70 6.57 6.89 11.64 2.65 10.51 3.20 2.98 0.86 4.90 1
.128 1 7.79
phism and the development of tuberculosis. Among the possible explanations given by different authors are the frequency of alleles in a distinct population and the possible influence of other genes, considering that the immune chain against mycobacteria involves other cytokines [15,19,22,
24]. In a survey conducted in West Africa, a large sample was used (682 cases) and even in those conditions, the association was not found [23]. The author explains that, even in a population this size, there may not be enough power on behalf of other factors, such as malnutrition, that might dilute any genotypic effect. Undiagnosed cases of tuberculosis in the control group may have affected the final result of the research [27].
When first combined, the results for the AA genotype described in Fig. 1, despite the high heterogeneity found (I2085.9%), demonstrated a well-established relationship
with the development of tuberculosis. The studies that most contributed to this outcome have been made in Malawi, in the UAE and West Africa, respectively (16.60%, 14.55% and 14.43%) [22–24]. In studies of infected populations, the
polymorphism was associated with low levels of
interferon-γ, which strongly shows that the polymorphism analysis is
linked to reduced cytokine production, decreasing the acti-vation of cellular immunity, which is essential for combat-ingM. tuberculosisand increasing the chances of infection [28–30].
In Fig.3, a protective role of the TT genotype (OR, 0.77; 95% CI00.67–0.88) is clearly shown. In another
meta-analysis of the subject, despite the relatively modest protec-tive effect (32%), this was also demonstrated [15]. Besides these aspects, the presence of the T allele may also be
associated with a predisposition to the disease through the analysis of AT in individuals of heterozygous genotype as shown in Fig.4(OR, 0.76; 95% CI00.70–0.83). Of the 19
articles evaluated, only 11 provided sufficient data for a statistical analysis of the prevalence of alleles A and T. According to Fig. 5, once again the role of the A allele is evident in the development of tuberculosis (OR, 1.56; 95% CI01.42–1.71).
Publication bias is a potentially serious limitation to any meta-analysis. If the results of unpublished studies are systematically different from those of published studies, particularly with respect to the magnitude and/ or direction of the findings, their omission from a meta-analysis would yield a biased summary estimate (assum-ing that the quality of the unpublished studies is at least equal to the quality of the published studies). Of course, the results will be more accurate as more data become available and this underscores the need for publication of even nonsignificant results to avoid publication bias in meta-analysis studies.
In conclusion, the result of this meta-analysis suggests a consistent association between polymorphism and tubercu-losis in different populations, which reinforces the fact that interferon-γplays an important role in host defence against
the development of tuberculosis. Although there is a need for more studies to make certain of the association, it is highly likely that the low level of interferon-γ, caused by
the presence of the AA genotype, increases the risk of active tuberculosis. In the present study, it was found that the studied polymorphism is a strong candidate marker for genetic susceptibility to tuberculosis.
Overall (I-squared = 82.9%, p = 0.000) Huseyin Onay et al (2009) ID
Manda Rossouw et al (2003)
Walid Ben Selma et al (2011) M. Vidyarani et al (2006)
Y. M. Mosaad et al (2010) HW Tso et al (2005)
Nilgün Sallakci et al (2006) Study
G. E. Etokebe et al (2005)
Antonio C.R.Vallinnoto et al (2010) Linda A. Larcombe et al (2008) Shiping Ding et al (2007)
1.56 (1.42, 1.71) 1.00 (0.57, 1.74) OR (95% CI)
1.46 (1.12, 1.91)
1.35 (1.00, 1.83) 1.09 (0.65, 1.81)
1.80 (1.22, 2.64) 2.34 (1.86, 2.96)
1.43 (1.06, 1.93) 1.00 (0.80, 1.24)
2.33 (1.66, 3.26) 5.23 (3.00, 9.12) 1.51 (1.16, 1.96)
100.00 3.41 Weight
12.10
10.00 3.89
5.26 13.25
9.69 %
22.45
6.04 1.40 12.52
1.56 (1.42, 1.71) 1.00 (0.57, 1.74) OR (95% CI)
1.46 (1.12, 1.91)
1.35 (1.00, 1.83) 1.09 (0.65, 1.81)
1.80 (1.22, 2.64) 2.34 (1.86, 2.96)
1.43 (1.06, 1.93) 1.00 (0.80, 1.24)
2.33 (1.66, 3.26) 5.23 (3.00, 9.12) 1.51 (1.16, 1.96)
100.00 3.41 Weight
12.10
10.00 3.89
5.26 13.25
9.69 %
22.45
6.04 1.40 12.52
1
.11 9.12
Conflict of interest The authors declare that they have no conflict of interest.
References
1. World Health Organization (WHO) (2007) Tuberculosis fact sheet. 104 ed
2. Brasil. Ministério da Saúde (2009) Secretaria de Vigilância em Saúde. Departamento de Vigilância Epidemiológica. Guia de Vigi-lância Epidemiológica. 7ª ed. Brasília: Ministério da Saúde. p 816 3. Corbett EL, Watt CJ, Walker N, Maher D, Williams BG,
Ravi-glione MC, Dye C (2003) The growing burden of tuberculosis: global trends and interactions with the HIV epidemic. Arch Intern
Med 163:1009–1021
4. Stenger S, Modlin RL (1999) T cell mediated immunity to
Myco-bacterium tuberculosis. Curr Opin Microbiol 2:89–93
5. Lykouras D, Sampsonas F, Kaparianos A, Karkoulias K, Tsoukalas G, Spiropoulos K (2008) Human genes in TB infection: their role
in immune response. Monaldi Arch Chest Dis 69(1):24–31
6. Bellamy R (2003) Susceptibility to mycobacterial infections: the
importance of host genetics. Genes Immun 4:4–11
7. Berrington WR, Hawn TR (2007) Mycobacterium tuberculosis, macrophages, and the innate immune response: does common
variation matter? Immunol Rev 219:167–186
8. Comstock GW (1978) Tuberculosis in twins: a re-analysis of the
Prophit study. Am Rev Respir Dis 117:621–624
9. Stead WW, Senner JW, Reddick WT, Lofgren JP (1990) Racial
differences in susceptibility to infection byMycobacterium
tuber-culosis. N Engl J Med 322:422–427
10. Brasil. Ministério da Saúde (2010) Manual de Recomendações para o Controle da Tuberculose no Brasil. Brasília. p 186 11. Lio D, Marino V, Serauto A, Gioia V, Scola L, Crivello A, Forte
GI, Colonna-Romano G, Candore G, Caruso C (2002) Genotype
frequencies of the _874T→A single nucleotide polymorphism in
the first intron of the interferon-gamma gene in a sample of Sicilian
patients affected by tuberculosis. Eur J Immunogenet 29:371–374
12. Cooke GS, Campbell SJ, Sillah J, Gustafson P, Bah B, Sirugo G, Bennett S, Mcadam KP, Sow O, Lienhardt C, Hill AV (2006) Polymorphism within the interferon-gamma/receptor complex is associated with pulmonary tuberculosis. Am J Crit Care Med 174
(3):339–343
13. Vidyarani M, Selvaraj P, PrabhuAnand S, Jawahar MS, Adhilakshmi AR, Narayanan PR (2006) Interferon gamma (ifngamma) & interleukin-4 (IL-4) gene variants & cytokine levels in pulmonary
tuberculosis. Ind J Med Res 124(4):403–441
14. Pravica V, Perrey C, Stevens A, Lee JH, Hutchinson IV (2000) A single nucleotide polymorphism in the first intron of the human IFN-gamma gene: absolute correlation with a polymorphic CA microsatellite marker of high IFN-gamma production. Hum Immunol
61:863–866
15. Pacheco AG, Cardoso CC, Moraes MO (2008) IFNG +874T/A, IL10 21082G/A and TNF 2308G/A polymorphisms in association with tuberculosis susceptibility: a meta-analysis study. Hum Genet
123:477–484
16. Luiz AJB (2002) Meta-Análise: definição, aplicações E sinergia
com dados especiais. Cadernos de Ciência Tecnologia 19(3):407–
428
17. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JPA (2009) The PRISMA statement for reporting sys-tematic reviews and meta-analyses of studies that evaluate health
care interventions: explanation and elaboration. PLoS Med 6:1–28
18. Downs SH, Black N (1998) The feasibility of creating a checklist for the assessment of the methodological quality both of
randomised and non-randomised studies of health care
interven-tions. J Epidemiol Community Health 52:377–384
19. Etokebe GE, Bulat-Kardum L, Johansen MS, Knezevic J, Balen S, Matakovic-Mileusnic N, Matanic D, Flego V, Pavelic J, Beg-Zec Z, Dembic Z (2006) Interferon-gamma gene (T874A and G2109A) polymorphisms are associatedwithmicroscopy-positive
tuberculo-sis. Scand J Immunol 63(2):136–141
20. Amim LH, Pacheco AG, Fonseca-Costa J, Loredo CS, Rabahi MF, Melo MH, Ribeiro FC, Mello FC, Oliveira MM, Lapa e Silva JR, Ottenhoff TH, Kristski AL, Santos AR (2008) Role of IFN-gamma +874T/A single nucleotide polymorphism in the tuberculosis out-come among Brazilians subjects. Mol Biol Rep Rio de Janeiro 35
(4):563–566
21. Larcombe L, Nickerson P, Dembinski I, Lodge A, Larcombe E, Milligan L, Martin B, Orr P (2008) Functional gene polymor-phisms in canadian aboriginal populations with high rates of
tu-berculosis. J Infect Dis 198(8):1175–1179
22. Moran A, Ma X, Reich RA, Graviss EA (2007) No association between the +874T/A single nucleotide polymorphism in the
IFN-gamma gene and susceptibility to TB. Int J Tuber Lung Dis 11(1):113–
115
23. Abhimanyu, Mangangcha IR, Jha P, Aroraa K, Mukerji M, Banavaliker JN, Consortium IGV, Brahmachari V, Bose M (2011) Differential serum cytokine levels are associated with cytokine gene polymorphisms in north Indians with active pulmonary tuberculosis.
Infect Genet Evol (11):1015–1022
24. Fitness J, Floyd S, Warndorv DK, Sichali L, Malema S, Crampin AC, Fine PE, Hill AV (2004) Large-scale candidate gene study of tuberculosis susceptibility in the Karonga district of northern
Malawi. Am J Trop Med Hyg 71:341–349
25. Onay H, Ekmekci A, Durmaz B, Sayin E, Cosar H, Bayram N, Can D, Akin H, Ozkinay C, Ozkinay F (2010) Interferon-g gene and interferon-g receptor-1 gene polymorphisms in children with
tu-berculosis from Turkey. Scand J Infect Dis 42:39–42
26. Mosaad YM, Soliman OE, Tawhid ZEE, Sherif DM (2010)
Interferon-gamma +874T⁄A and interleukin-10 -1082 A⁄G single
nucleotide polymorphism in Egyptian children with tuberculosis.
Scand J Immunol 72(4):358–364
27. Hwang JH, Kim EJ, Kim SY, Lee SH, Suh GY, Kwon OJ, JI Y, Kang M, Kim DH, Koh WJ (2007) Polymorphisms of interferon-g and interferon-g receptor 1 genes and pulmonary tuberculosis in
Koreans. Respirology 12:906–910
28. Zhang M, Lin Y, Iyer DV, Gong J, Abrams JS, Barners PF (1995) T cell cytokine responses in human infection with Mycobacterium
tuberculosis. Infect Immun 63:3231–3234
29. Sallakci N, Coskun M, Berber Z, Gürkan F, Kocamaz H, Uysal G, Bhuju S, Yavuzer U, Singh M, Yefin O (2006) Interferon-gamma gene+874T-A polymorphism is associated with tuberculosis and
gamma interferon response. Tuberculosis 87(3):225–230
30. Hashemi M, Sharifi-Mood B, Nezamdoost M, Moazeni-Roodi A, Naderi M, Kouhpayeh H, Taheri M, Ghavami S (2011) Functional
polymorphism of interferon-γ(IFN-γ) gene +874T/A
polymor-phism is associated with pulmonary tuberculosis in Zahedan,
Southeast Iran. Prague Med Rep 1(11):38–43
31. Rossouw M, Nel HJ, Cooke GS, van Helden PD, Hoal EG (2003) Association between tuberculosis and a polymorphic NFkappaB
binding site in the interferon gamma gene. Lancet 361(9372):1871–
1872
32. Lopez-Maderuelo D, Arnalich F, Serantes R, Gonzalez A, Codoceo R, Madero R, Vazquez JJ, Montiel C (2003) Interferon-gamma and interleukin-10 gene polymorphisms in pulmonary tuberculosis. Am J Respir Crit Care Med Madri 167:970
33. Tso HW, Ip WK, Chong WP, Tam CM, Chiang AK, Lau YL (2005) Association of interferon gamma and interleukin 10 genes
with tuberculosis in Hong Kong Chinese. Genes Immun 6:358–
34. Ansari A, Talat N, Jamil B, Hasan Z, Razzaki T, Dawood G, Hussain R (2009) Cytokine gene polymorphisms across tubercu-losis clinical spectrum in Pakistani patients. PLoS One 4:4778 35. Vallinoto AC, Graça ES, Araújo MS, Azavedo VN,
Cayres-Vallinoto I, Machado LF, Ishak MO, Ishaj R (2010) IFNG +874T/A polymorphism and cytokine plasma levels are associated
with susceptibility to Mycobacterium tuberculosisinfection and
clinical manifestation of tuberculosis. Hum Immunol 71:692–696
36. Selma WB, Harizi H, Bougmiza I, Hannachi N, Kahla IB, Zaieni R, Boukadida J (2011) Interferon gamma +874t/A polymorphism is associated with susceptibility to active pul-monary tuberculosis development in Tunisian patients. DNA
Cell Biol 30(6):379–387
37. Ding S, Li L, Zhu X (2008) Polymorphism of the interferon-gamma gene and risk of tuberculosis in a southeastern Chinese
![Table 1 Studies of the association of polymorphism +874 A/T of interferon-γ and susceptibility to tuberculosis Reference Year Place Description of cases Description of controls Result [11] 2002 Italy 45 patients, the Health Unit](https://thumb-eu.123doks.com/thumbv2/123dok_br/15359473.564235/4.892.74.813.101.1076/association-polymorphism-interferon-susceptibility-tuberculosis-reference-description-description.webp)