BrazJOtorhinolaryngol.2017;83(6):677---682
www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Nasal
polyposis
in
cystic
fibrosis:
follow-up
of
children
and
adolescents
for
a
3-year
period
夽
Silke
Anna
Theresa
Weber
a,∗,
Renata
Mizusaki
Iyomasa
a,
Camila
de
Castro
Corrêa
a,
Wellington
Novais
Mafra
Florentino
a,
Giesela
Fleischer
Ferrari
baUniversidadeEstadualPaulista‘‘JúliodeMesquitaFilho’’,FaculdadedeMedicinadeBotucatu,DepartamentodeOftalmologia,
OtorrinolaringologiaeCirurgiadeCabec¸aePescoc¸o,Botucatu,SP,Brazil
bUniversidadeEstadualPaulista‘‘JúliodeMesquitaFilho’’,FaculdadedeMedicinadeBotucatu,DepartamentodePediatria,
Botucatu,SP,Brazil
Received21February2016;accepted16September2016 Availableonline17October2016
KEYWORDS
Polyposis; Cysticfibrosis; Diagnosis; Endoscopy; Therapy
Abstract
Introduction:Nasalpolyposisisoftenfoundinpatientswithcysticfibrosis.
Objective: Toassesstheincidenceofnasalpolyposis,theresponsetomedicaltreatment, recur-renceandtheneedfor surgicalinterventioninchildren andadolescentswith cysticfibrosis duringathree-yearfollow-up.
Methods:Clinicalsymptoms(pulmonary,pancreaticinsufficiency,malnutrition,nasal obstruc-tion),twopositivesweatchloridetests,andgenotypefindingsin23patientswithcysticfibrosis were analyzed.Allpatients underwentnasalendoscopyevery 12monthsfromJanuary 2005 toDecember 2007,toassessthepresenceandgradeofNasalPolyps.Nasal polyposis,when present,weretreatedwithtopicalcorticosteroidsfor6---12months,withprogressbeing eval-uatedwithinthe3yearsoffollow-up.
Results:Inthefirstevaluation,nasalpolyposiswasdiagnosedin30.43%ofpatients(3bilateral and4unilateral),recurrentpneumoniain82.6%,pancreaticinsufficiencyin87%,and malnu-tritionin74%.Thepresenceofnasalpolyposiswasnotassociatedwithchloridevaluesinthe sweat,genotype,clinicalsignsofseverityofcysticfibrosis,ornasalsymptoms.Inthethree-year periodoffollowup,13patients(56.52%)hadatleastoneeventofpolyposis,withtheyoungest beingdiagnosedat32monthsofage.Onlyonepatientunderwentsurgery(polypectomy),and therewasonediagnosisofnasopharyngealcarcinoma.
夽
Pleasecitethisarticleas:WeberSA,IyomasaRM,CorrêaCC,FlorentinoWN,FerrariGF.Nasalpolyposisincysticfibrosis:follow-upof
childrenandadolescentsfora3-yearperiod.BrazJOtorhinolaryngol.2017;83:677---82.
∗Correspondingauthor.
E-mail:[email protected](S.A.Weber).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.09.005
1808-8694/©2016Associac¸˜aoBrasileiradeOtorrinolaringologiaeCirurgiaC´ervico-Facial.PublishedbyElsevierEditoraLtda.Thisisanopen
Conclusion:Thestudyshowedahighincidenceofnasalpolyposis.Monitoringthroughroutine endoscopyinpatientswithcysticfibrosis,evenintheabsenceofnasalsymptoms,ishighly rec-ommended.Thetherapywithtopicalcorticosteroidsachievedgoodresults.Thus,aninteraction betweenpediatriciansandotolaryngologistsisnecessary.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Polipose; Fibrosecística; Diagnóstico; Endoscopia; Terapia
Poliposenasalemfibrosecística:seguimentoemcrianc¸aseadolescentesduranteum períodode3anos
Resumo
Introduc¸ão:Apoliposenasaléfrequentementeencontradaempacientesportadoresdefibrose cística.
Objetivo:Avaliaraincidênciadepoliposenasal,arespostaaotratamentoclínico,arecorrência eanecessidadedeintervenc¸ãocirúrgicaemcrianc¸aseadolescentescomfibrosecísticadurante umseguimentode3anos.
Método: Os sintomas clínicos (pulmonar, insuficiência pancreática, desnutric¸ão, obstruc¸ão nasal),duaspesquisasdecloronosuorpositivasegenótipode23pacientescomfibrose cís-ticaforamdescritos.Todosospacientesforamsubmetidosàendoscopianasalacada12meses duranteoperíododejaneirode2005adezembrode2007,paraavaliac¸ãodepresenc¸aegrau depoliposenasal.Apoliposenasal,quandopresente,foitratadacomcorticosteroidetópico de6a12meses,eavaliadaaevoluc¸ãonos3anosdeseguimento.
Resultados: Naprimeiraavaliac¸ão,apoliposenasalfoidiagnosticadaem30,43%dospacientes (3bilateraise4unilaterais),pneumoniarecorrenteem82,6%,insuficiênciapancreáticaem87% eadesnutric¸ãoem74%.Apresenc¸adepoliposenasalnãoseassociouaosvaloresdeclorono suor,genótipo,sinaisclínicosdegravidadedafibrosecísticaousintomasnasais.Nos3anosde seguimento,13pacientes(56,52%)apresentarampelomenosumeventodePolipose,sendoo maisjovemdiagnosticadoaos32mesesdeidade.Apenasumpacientefoisubmetidoàcirurgia (polipectomia),ehouveumdiagnósticodecarcinomadanasofaringe.
Conclusão:Oestudomostroualtaincidênciadepoliposenasal.Oacompanhamentopormeio deexamesendoscópicosderotinaempacientesfibrocisticos,mesmonaausênciadesintomas nasais,éaltamenterecomendado.Aterapiacomcorticoidetópicomostroubonsresultados. Sendoassim,faz-senecessáriaainterac¸ãoentrepediatraseotorrinolaringologistas.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Cysticfibrosis (CF) is an autosomal recessive diseasethat affectstheexocrineglands,involving multiple organsand progressingchronicallyandprogressively.Itisthemost com-monlethalgeneticdiseaseinCaucasians,withanaverage frequency of 1:2000 live births.1,2 In Brazil, studies have
revealedan incidenceof1:9500livebirthsinthestate of Parana,3 1:8700 inSanta Catarina4 and.1:10,000in Minas
Gerais.5
Respiratory infections leading to ultimate respiratory failurearetheleadingcausesofdeathinCFpatients. How-ever, mortality has been reduced in recent years due to earlierdiagnosis,greaterattentiontoprophylaxisof recur-rent airway infections, and better control of patients in specializedservices.1,2
CF diagnosis is based on clinical and laboratorial criteria: family history of CF, pancreatic insufficient/
pancreatic sufficient, chronic obstructive suppurative lungdisease,andtwohighsweatchloridetests(>60mEq/L) and/or detection of genetic mutations described in CF. Other clinical data that suggest the disease are: meconium ileus and/or intestinal atresia, hyponatremic dehydration, edema and hypoalbuminemia, chronic panrhinosinusitis, nasal polyposis (NP), volvulus, intus-susception, bronchiectasis of unknown etiology, and azoospermia.6,7
Upper airway (UAW) impairment such as recurrent rinorhinosinusitis, rhinitisand/or NPoccursin over90% of patients.8---16 The incidence of NP, in particular, has been
reportedin6---48%patients,17,18andissymptomaticinabout
4% patients at diagnosis of CF.8,10,11,19 The literature
esti-mates that 14% of patients require surgical treatment of NP.8,10,11,19
Todate,thepathophysiologyofNPisstillunknown.20,21
Three-yearfollow-upofnasalpolyposiswithcysticfibrosis 679
NP, buttheprevalenceof atopyinpatientswithCFis not higherthaninthegeneralpopulation.22
According to data from the literature and the study previously conducted in our service,23 a need for better
characterization of the evolution of UAW involvement in thesepatientswasidentified.
Thus, the aim of this study was to evaluate, in the mediumterm,theincidenceofNP,theresponsetomedical treatment,therateofrecurrence,andtheneedfor surgi-calinterventioninchildrenandadolescentswithCFduring a3-yearfollowupperiod.
Casuistics
and
methods
TheprospectivecohortstudywasapprovedbytheResearch EthicsCommitteeoftheinstitutioninvolvedinthisresearch. Parents/caregiversandchildrenover10yearssignedafree andinformedconsent.
The initial sample consisted of 23patients (20 males), aged 1 year and 9 months to 22 years and 8 months, followed at the Cystic FibrosisReference Center of Pedi-atricsPneumologyDepartmentoftheinstitutionconcerned. Epidemiological data(age, gender) and clinical symptoms of CF were obtained, such as meconium ileus, malnutri-tion,pancreaticinsufficiency,recurrentpneumoniaand/or other respiratory symptoms, as well as the confirmation of CF through sweat chloride test7 and genetic studies.
All patients were investigated for complaints of nasal obstruction, mouth breathing, asthma and rhinosinusitis, andunderwentnasalendoscopyevery12monthsfor3years. Nasofibroscopic procedures wereperformed undertopical anesthesiawithlidocainespraywithnovasoconstrictor.In childrenunder3yearsofagetheflexiblepediatric nasofi-broscopewasused(KarlStorz,diameter2.4mm),andinthe otherstherigidnasalendoscope(KarlStorz,30◦,diameter of2.4or4mm)wasused.
Thepresenceorabsenceofpolypswasdescribed, accord-ingtotheclassificationsuggestedbyLundandKennedy,24in
Grade0---nopolyp,GradeI---polypinthemiddlemeatus, GradeII ---polypthroughthemiddleturbinate,GradeIII ---polypfillingtheentirenasalcavity. Duringendoscopy, the presenceand colorof secretion,andnasalmucosaaspect (coloration,edema,degeneration)wereevaluated.
Patients diagnosed with NP underwent treatment with nasaltopiccorticosteroidforsixmonths,andwere reeval-uatedbyendoscopyafterthisperiod.Incaseofpersistent Polyposis,patientswereevaluatedwithcomputed tomogra-phyoftheparanasalsinusesforapossiblesurgicalschedule. In the statistical analysis, demographic and symptoms datawereregisteredasmeanandstandarddeviation.The association betweenthe presenceof polypsand age,sex, clinical symptoms and geneticmutations was assessedby Fisher’sexacttest,consideringsignificantp<0.05.
Results
CF diagnosis was confirmed in all subjects through the sweat test. Genetic mutations, using a panel containing 12 mutations, were investigated in all patients, and in 8 patients mutations were detected: F 508/other, three F508/ F508, one F508/G 542X, one G542X/other,
Figure1 ImageofendoscopyofagradeIpolypintheright nasalcavityofpatientno.12(P,polyp;CM,middleturbinate).
oneR1162X/R1162X,andin9patients themutationcould not be determined. A significant proportion of patients hadclinicalmanifestations,includingrecurrentpneumonia (82.6%),pancreaticinsufficiency (87%),malnutrition(74%) andmeconiumileus(13%).
The reported respiratory complaints at baseline were asthmain35%ofpatients,rhinosinusitisin22%,and preva-lenceoforalbreathingfoundin22%.
In the first evaluation through nasal endoscopy, Nasal Polypswere foundin 7patients(30.43%). Ofthese,3had bilateral,and 4 unilateral NP, with Grade Iin 3 patients, GradeIIin1patient,andGradeIIIin3patients.No associa-tionwasfound between NP,gender, age, clinicalseverity, or genetic mutation. Fig. 1 illustrates the results of the endoscopicevaluation(Table1).
During the 3 years of follow up, 13 patients (56.52%) experienced at least one event of NP, withthe youngest beingdiagnosedat32monthsofage.Inthesesubjectsthe presenceof nasalpolyposiswas notassociatedwithnasal symptoms,suchasnasalobstruction, rhinorrheaor mouth breathing.Atthefinalendoscopy,sixpatientshad polypo-sis.In all patients, the staging of polyposis was Grade I, indicatinglesserseverity(p<0.05).
The treatment of NP wasnasal topic corticosteroid at theusualdose,and57.14%ofpatientsrespondedto medi-cal therapy in the subsequent evaluation, with only one patientwhohadbilateralNPGradeIIInotshowing satisfac-toryimprovement,andforwhomnasalendoscopicsurgery wasrecommended.Inthesethreeyears,twopatientsdied, andonedevelopednasopharyngealcarcinoma, undergoing chemotherapyandradiotherapywithagoodresponse.The findings regarding the 3 years of follow-up are shown in
Table2.
Discussion
W
eber
SA
et
al.
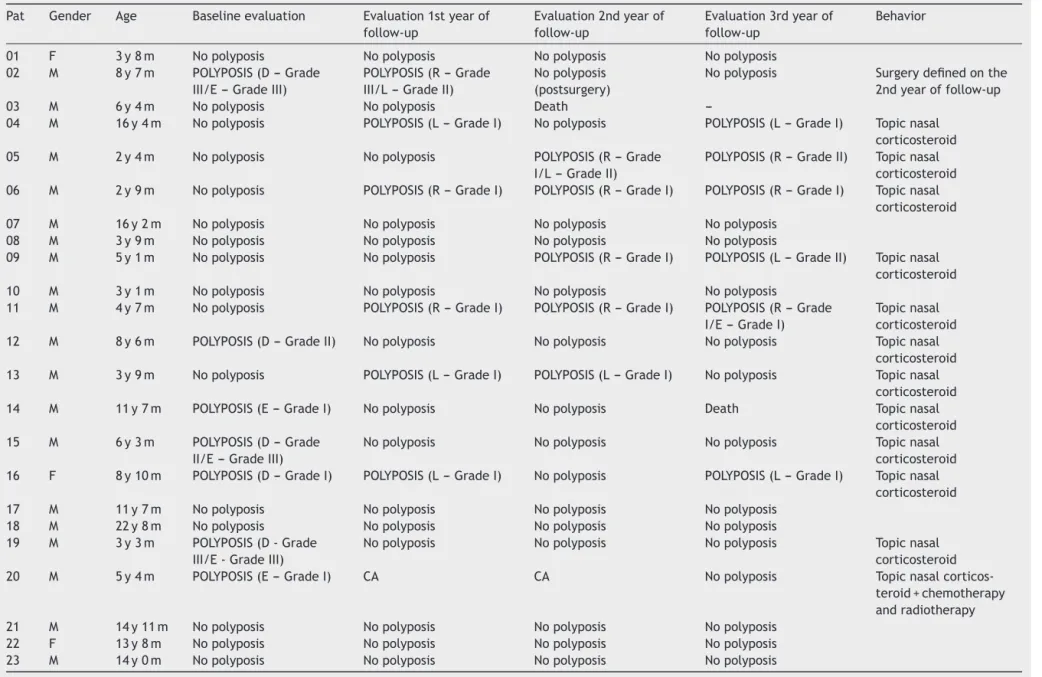
Table1 Resultsofendoscopyinpatientswithcysticfibrosisandnasalpolyposisatbaselineevaluation,first,secondandthirdyearoffollow-up. Pat Gender Age Baselineevaluation Evaluation1styearof
follow-up
Evaluation2ndyearof follow-up
Evaluation3rdyearof follow-up
Behavior
01 F 3y8m Nopolyposis Nopolyposis Nopolyposis Nopolyposis 02 M 8y7m POLYPOSIS(D---Grade
III/E---GradeIII)
POLYPOSIS(R---Grade III/L---GradeII)
Nopolyposis (postsurgery)
Nopolyposis Surgerydefinedonthe 2ndyearoffollow-up 03 M 6y4m Nopolyposis Nopolyposis Death
---04 M 16y4m Nopolyposis POLYPOSIS(L---GradeI) Nopolyposis POLYPOSIS(L---GradeI) Topicnasal corticosteroid 05 M 2y4m Nopolyposis Nopolyposis POLYPOSIS(R---Grade
I/L---GradeII)
POLYPOSIS(R---GradeII) Topicnasal corticosteroid 06 M 2y9m Nopolyposis POLYPOSIS(R---GradeI) POLYPOSIS(R---GradeI) POLYPOSIS(R---GradeI) Topicnasal
corticosteroid 07 M 16y2m Nopolyposis Nopolyposis Nopolyposis Nopolyposis
08 M 3y9m Nopolyposis Nopolyposis Nopolyposis Nopolyposis
09 M 5y1m Nopolyposis Nopolyposis POLYPOSIS(R---GradeI) POLYPOSIS(L---GradeII) Topicnasal corticosteroid 10 M 3y1m Nopolyposis Nopolyposis Nopolyposis Nopolyposis
11 M 4y7m Nopolyposis POLYPOSIS(R---GradeI) POLYPOSIS(R---GradeI) POLYPOSIS(R---Grade I/E---GradeI)
Topicnasal corticosteroid 12 M 8y6m POLYPOSIS(D---GradeII) Nopolyposis Nopolyposis Nopolyposis Topicnasal
corticosteroid 13 M 3y9m Nopolyposis POLYPOSIS(L---GradeI) POLYPOSIS(L---GradeI) Nopolyposis Topicnasal
corticosteroid 14 M 11y7m POLYPOSIS(E---GradeI) Nopolyposis Nopolyposis Death Topicnasal
corticosteroid 15 M 6y3m POLYPOSIS(D---Grade
II/E---GradeIII)
Nopolyposis Nopolyposis Nopolyposis Topicnasal corticosteroid 16 F 8y10m POLYPOSIS(D---GradeI) POLYPOSIS(L---GradeI) Nopolyposis POLYPOSIS(L---GradeI) Topicnasal
corticosteroid 17 M 11y7m Nopolyposis Nopolyposis Nopolyposis Nopolyposis
18 M 22y8m Nopolyposis Nopolyposis Nopolyposis Nopolyposis 19 M 3y3m POLYPOSIS(D-Grade
III/E-GradeIII)
Nopolyposis Nopolyposis Nopolyposis Topicnasal corticosteroid 20 M 5y4m POLYPOSIS(E---GradeI) CA CA Nopolyposis Topicnasal
corticos-teroid+chemotherapy andradiotherapy 21 M 14y11m Nopolyposis Nopolyposis Nopolyposis Nopolyposis
22 F 13y8m Nopolyposis Nopolyposis Nopolyposis Nopolyposis 23 M 14y0m Nopolyposis Nopolyposis Nopolyposis Nopolyposis
Three-yearfollow-upofnasalpolyposiswithcysticfibrosis 681
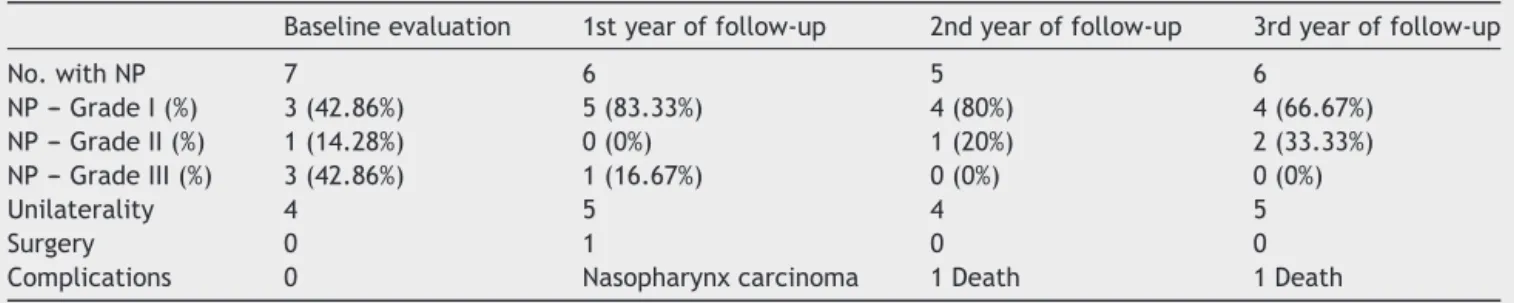
Table2 Comparisonbetweenyoungeragewithnasalpolyposis,numberofpatientswithnasalpolyposis,gradeofpolyposis, unilaterality,presenceofsurgicalindicationsandcomplicationsinthebaselineevaluation,inthefirst,secondandthirdyearof follow-up.
Baselineevaluation 1styearoffollow-up 2ndyearoffollow-up 3rdyearoffollow-up
No.withNP 7 6 5 6
NP---GradeI(%) 3(42.86%) 5(83.33%) 4(80%) 4(66.67%) NP---GradeII(%) 1(14.28%) 0(0%) 1(20%) 2(33.33%) NP---GradeIII(%) 3(42.86%) 1(16.67%) 0(0%) 0(0%)
Unilaterality 4 5 4 5
Surgery 0 1 0 0
Complications 0 Nasopharynxcarcinoma 1Death 1Death
NP,nasalpolyposis;No.,numberofpatients;%,percentage.
Allpatients haddiagnosticconfirmation supported bytwo abnormalchloridedosagesinsweat,accordingtoastandard methodthatissupportedbyliterature.7
Regarding theresult ofthe detectionof genetic muta-tions, in 52.17% the F508 mutationwas present, a high
percentageofpatientswithCFinBrazil,despitethe hetero-geneityofthispopulation;thiscorroboratestheliterature thatidentifiestheassociationofthismutationwithCF.19 It
shouldbenotedthattherewasnocorrelationbetweenthe presenceorseverityofNPandthegenotype.
Intheliterature,NPhasbeenreportedwithanincidence of6---48%inCFpatients10,11,25Inthisstudy,theincidencewas
30.43%;itwashigherthantheonepresentedinanational study thatreportedthe incidencetobe15.2% inchildren withameanageof9.5years.26Inaddition,whenmonitoring
CFpatientsovera3-yearfollow-up,wemadethediagnosis ofNPinachildof2yearsand8months,anageyoungerthan reportedintheliterature,whichdescribestheoccurrence ofNPonlyafter5yearsofage.27
Even with this study population being predominantly composed of children, there was a high incidence of NP, given that of the 13 cases, 12 were children (less than 12 years) and only one wasa teenager of 16 years. The literature brings the incidence of NP of 5% and 15.2% in children.26,28
Therewasincidenceofrhinosinusitisandmouth breath-ing in 22% of patients, similar to that found in the literature.9,10,18,29ThepresenceofNPdidnotcorrelatewith
nasalobstructionorsecretion.18
Among patients withNP, 3patients hadNP at baseline (42.86%), 5 in 1 year of follow-up (83.33%); 4 in the 2nd (80%),and4patientsinthe3rdyearoffollow-up(66.67%) had smallpolyps, Grade I,highlighting the importanceof routineendoscopic examination.11 Thesedata exceed the
percentage found in literature of 68% of identification of smallpolyps.18
Onlyonepatientrequiredsurgery(4.35%),withno recur-renceinthesubsequenttwoyears;theliteratureestimates the need for surgery in patients with NP to be 20%8,9,11
throughoutlife.Becauseofareportofpolyprecurrencewith aneedforsurgeryin28.57---58%,30,31thesepatientsrequire
continuedmonitoring.
Regarding the use of topical corticosteroids, it was observedthat57.14%ofpatientsrespondedsatisfactorilyto theinitialclinicaltreatment,andinasubsequentevaluation therewascomplete involutionoftheNP, whichresembles
theinformationthatthereisimprovementin56%ofpatients withNPwithtopicalcorticosteroidstherapy.8Forthe
pop-ulationwithCF,there isno evaluationdata reportingthe evolutionofNPwithclinicaltreatmentforlongperiods.
Webelievethattheprotocolproposedby thisresearch groupofannualendoscopicfollow-upofCFpatients,in addi-tiontoclinicaltreatment,maybeatleastpartlyresponsible forthe low need forsurgical indication. CFis acommon, seriousgeneticdisease, butwhen thereis early diagnosis andtreatment, comorbidities are reduced,and the qual-ityoflifeoftheseindividualsimprove.Thelimitednumber of patients in this study ledto difficulties in the statisti-cal analysis, emphasizing the importance of other Cystic FibrosisReferenceCentersalsofollowingthisprotocoland publishingtheirresultsinscientificsettings.
Conclusion
Theincidenceofnasalpolyposisinpatientswithcystic fibro-sisishigh, evenamongchildren,andisnotrelatedtothe clinicalseverityof cysticfibrosis or nasalsymptoms. Rou-tineannualnasalendoscopyallowsearlydiagnosisofnasal polyps at an early stage (Grade I polyposis),and the ini-tiation of clinical treatment with satisfactory control of thecondition.Therefore,the interactionbetween pulmo-nologistsandotolaryngologistsiscrucialfor thediagnosis, treatmentindication,andfollow-upofthesepatients.
Funding
ThisstudywasfundedbytheSãoPauloResearchFoundation ---FAPESP(2010/11064---1).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.CysticFibrosisFoundation.Clinicalpracticeguidelinesforcystic fibrosis.Atlanta:CysticFibrosisFoundation;1997.
2.RatjenF,DöringG.Cysticfibrosis.Lancet.2003;361:681---9.
Paraná:avaliac¸ãoapós30mesesdesuaimplantac¸ão.JPediatr. 2005;81:240---4.
4.Honório LFO, Ludwig Neto N, Barbosa E, Perin N, Gastaldi LA, Ferreira JE, et al. Avaliac¸ão da triagem neonatal para fibrosecísticanoEstado deSantaCatarina.JBrasPneumol. 2006;32:S1.
5.ReisF,MeloSO,VergaraAA.Programadetriagemneonatalpara fibrosecísticadeMinasGerais(PETN-FC):aspectosclínicose laboratoriais.JBrasPneumol.2006;32:S1.
6.RosensteinBJ,CuttingGR. Thediagnosis ofcysticfibrosis:a consensusstatement.JPediatr.1998;132:589---95.
7.Gibson LEG,Cooke RE.Testfor concentrationofeletrolytes insweatincysticfibrosisofthepancreasutilizingpilocarpin iontophoresis.Pediatrics.1959;23:545---9.
8.Cepero R, Smith RJH, Cathin FI, Bressler KL, Furuta GT, SandesaKC.CysticFibrosis---anotolaryngologic perspective. OtolaryngolHeadNeckSurg.1987;97:356---60.
9.PiltcherOB,ZucattoAE,RosaDD,PreisslerLC,HentschelEL, PaixãoLQ.Rinossinusitenafibrosecística.RevBras Otorrino-laringol.1997;63:469---78.
10.BastasakisJG, El-NaggarAK.Cysticfibrosisand thesinonasal tract.AnnOtolRhinolLaryngol.1996;105:329---30.
11.RamseyB,RichardsonMA.Impactofsinusitisincysticfibrosis. JAllergyClinImmunol.1992;90:547---52.
12.Graf PM. Rhinitis medicamentosa. Clin Allergy Immunol. 2007;19:295---304.
13.HadfieldPJ,Rowe-JonesJM,MackayIS.Aprospectivetreatment trialofnasal polyps inadultswithcysticfibrosis. Rhinology. 2000;38:63---5.
14.CeperoR,SmithRJ,CatlinFI,BresslerKL,FurutaGT,Shandera KC.Cysticfibrosisanotolaryngologicperspective.Otolaryngol HeadNeckSurg.1987;97:356---60.
15.Morris P, Leach A. Antibiotics for persistent nasal discharge (rhinosinusitis)inchildren.CochraneDatabaseSystRev.2002. CD001094.
16.VidelerWJ,vanDrunenCM,ReitsmaJB,FokkensWJ.Nebulized bacitracin/colimycin:atreatmentoptioninrecalcitrantchronic rhi-nosinusitiswithStaphylococcusaureus?Adouble-blind, ran-domized,placebo-controlled,cross-overpilotstudy.Rhinology. 2008;46:92---8.
17.Schwachman H, Kulczyckii LL, Mueller HL, Flake CJ. Nasal polyposis in patients with cystic fibrosis. Pediatrics. 1962;30:389---401.
18.HenrikssonG,HestrinKM,KarpatiF,WikstroemAC,StiernaP, HjelteL.Nasalpolypsincysticfibrosis.Chest.2002;121:40---7.
19.KingdomTT,LeeKC,FirsimmonsSC,CroppGJ.Clinical charac-teristicsand genotypeanalysisofpatientswithcysticfibrosis and nasalpolyposisrequiring surgery. ArchOtolaryngol Head NeckSurg.1996;122:1209---13.
20.Konstan MW, Schluchter MD, Xue W, Davis PB. Clinical use of ibuprofen is associated with slower FEV1 decline in children with cystic fibrosis. Am J Respir Crit Care Med. 2007;176:1084---9.
21.LindstromDR,ConleySF,SplaingardML,GershanWM. Ibupro-fen therapy and nasal polyposisin cysticfibrosispatients. J Otolaryngol.2007;36:309---14.
22.RamseyB,RichardsonM.Impactofsinusitisincysticfibrosis.J AllergyClinImmunol.1992;90:547---52.
23.WeberSAT,FerrariGF.Incidênciaeevoluc¸ãodapoliposenasal emcrianc¸aseadolescentescomfibrosecística.RevBras Oto-rrinolaringol.2008;74:16---20.
24.JohanssonL,AkerlundA,HolmbergK,MelenI,StierneP,Bende M.Evaluationofmethodsforendoscopicstagingofnasal poly-posis.ActaOtolaryngol.2000;120:72---6.
25.CimminoM, CavaliereM, NordoneM, PlantulliA, OreficeA, EspositoV,et al. Clinicalcharacteristicsand genotype anal-ysisof patientswithcystic fibrosisand nasal polyposis. Clin Otolaryngol.2003;28:125---32.
26.ThoméDC,TomikowaSO,RomanoF,PaderaF,AddeFV,Voegels RL,etal.Manifestac¸õesnasossinusaisempacientescomfibrose cística(FC).JBrasPneumol.2006;32:5.
27.SternR,BoatT,WoodR,LeRoyW,DoershukC.Treatmentand prognosis of nasal polyps in cystic fibrosis. Am J Dis Child. 1982;136:1067---70.
28.SchmittEJ,NeavilleW,PougdeeT.Prevalenceofcystic fibro-sisinchildrenwhopresentwithnasalpolyposis.JAllergyClin Immunol.2005;115:516.
29.ShapiroED,MilmoeGJ,WaldER,RodnanJB,BowenA. Bacteri-ologyofthemaxillarysinusesinpatientswithcysticfibrosis.J InterDis.1982;146:589---93.
30.YungMW,GouldJ,UptonGJ.Nasalpolyposisinchildrenwith cysticfibrosis: a long-term follow-upstudy. Ann OtolRhinol Laryngol.2002;111:1081---6.