www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Speech
nasality
and
nasometry
in
cleft
lip
and
palate
夽
Fabiane
Rodrigues
Larangeira
a,∗,
Jeniffer
de
Cássia
Rillo
Dutka
b,
Melina
Evangelista
Whitaker
c,
Olívia
Mesquita
Vieira
de
Souza
b,
José
Roberto
Pereira
Lauris
b,
Mariana
Jales
Felix
da
Silva
d,
Maria
Inês
Pegoraro-Krook
baMaster’sDegreePrograminSciences,DepartmentofSpeech/LanguagePathologyandAudiology,FaculdadedeOdontologiade
Bauru,UniversidadedeSãoPaulo(USP),Bauru,SP,Brazil
bDepartmentofSpeech/LanguagePathologyandAudiology,FaculdadedeOdontologiadeBauru,UniversidadedeSãoPaulo
(USP),Bauru,SP,Brazil
cSpeechAidProsthesisService,HospitaldeReabilitac¸ãodeAnomaliasCraniofaciais,UniversidadedeSãoPaulo(USP),Bauru,SP,
Brazil
dMaster’sDegreePrograminRehabilitationSciences,HospitaldeReabilitac¸ãodeAnomaliasCraniofaciais,UniversidadedeSão
Paulo(USP),Bauru,SP,Brazil
Received13January2015;accepted26May2015 Availableonline18December2015
KEYWORDS
Cleftpalate; Speech;
Speechproduction measurement; Diagnosis; Velopharyngeal insufficiency
Abstract
Introduction:Perceptualevaluationisconsideredthegoldstandardtoevaluatespeechnasality. Severalproceduresareusedtocollectandanalyzeperceptualdata,whichmakesitsusceptible toerrors.Therefore,therehasbeenanincreasingdesiretofindmethodsthatcanimprovethe assessment.
Objective:Todescribeandcomparetheresultsofspeechnasalityobtainedbyassessmentsof livespeech,theTestofHypernasality(THYPER),assessmentsofaudiorecordedspeech,and nasometry.
Methods:Aretrospectivestudyconsistingof331patientswithoperatedunilateralcleftlipand palate.Speechnasalitywasassessedbyfourmethodsofassessment:liveperceptualjudgement, THYPER,audio-recordedspeechsamplejudgementbymultiplejudges,andnasometry.Alldata were collectedfrommedical recordsofpatients, withtheexception ofthespeech sample recordingassessment,whichwascarriedoutbymultiplejudges.
夽 Pleasecitethisarticleas:LarangeiraFR,DutkaJCR,WhitakerME,deSouzaOMV,LaurisJRP,daSilvaMJF,etal.Speechnasalityand
nasometryincleftlipandpalate.BrazJOtorhinolaryngol.2016;82:326---33.
∗Correspondingauthor.
E-mail:fa2frodrigues@yahoo.com.br(F.R.Larangeira). http://dx.doi.org/10.1016/j.bjorl.2015.05.017
Results:The resultsshowed thatthehighest percentagesofabsence ofhypernasalitywere obtainedfromjudgementsperformedliveandfromtheTHYPER,withequalresultsbetween them(79%).Lowerpercentageswereobtainedfromtherecordingsbyjudges(66%)andfrom nasometry(57%).
Conclusion: Thebestresultsamongthefourspeechnasalityevaluationmethodswereobtained fortheonesperformedlive(livenasalityjudgementbyaspeechpathologistandTHYPER). © 2015Associac¸˜aoBrasileira de Otorrinolaringologiae CirurgiaC´ervico-Facial.Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Fissurapalatina; Fala;
Medidadaproduc¸ão dafala;
Diagnóstico; Insuficiência velofaríngea
Nasalidadedefalaenasometrianasfissuraslabiopalatinas
Resumen
Introduc¸ão: A avaliac¸ão perceptivaéconsiderada padrão-ouro para avaliaranasalidadede fala.Váriosprocedimentossãoutilizadosparacoletareanalisarosdadospercebidos,oquea tornasuscetívelaerros.Porisso,háumapreocupac¸ãocrescentenaprocurademétodosque possamaperfeic¸oá-la.
Objetivo: Descreverecompararosresultadosdanasalidadedefalaobtidospormeiode jul-gamento ao vivo,TestedeHipernasalidade (THIPER), julgamentodegravac¸ões porjuízese nasometria.
Método: Estudoretrospectivode331pacientescomfissuralabiopalatinaunilateraloperada.Foi realizadaaanálisedosresultadosdojulgamentodanasalidadeaovivoepormeiodegravac¸ões porjuízes,doTHIPERedanasometria.Osdadosforamcoletadosdoprontuáriodospacientes, comexcec¸ãodojulgamentodasgravac¸õesdasamostrasdefala,quefoirealizadoporjuízes múltiplos.
Resultados: Foramobtidasporcentagensmaisaltasdeausênciadehipernasalidadeno julga-mentoaovivoenoTHIPER,comresultadosiguaisentreambas(79%).Porcentagensmenores deausênciadehipernasalidadeforamobtidasnojulgamentodasgravac¸õesporjuízes(66%)e paraanasometria(57%).
Conclusão:Osmelhoresresultadosentreasquatromodalidadesdeavaliac¸ãodanasalidadede falaforamobtidosparaasrealizadasaovivo(julgamentoporumfonoaudiólogoeTHIPER). ©2015Associac¸˜aoBrasileiradeOtorrinolaringologiaeCirurgiaC´ervico-Facial.Publicado por ElsevierEditoraLtda.Todoslosderechosreservados.
Introduction
Oneofthegreatchallenges forachild bornwithcleftlip and palate is to develop the resonance and articulation for normal speechproduction. A cleft palate is the most commoncauseofvelopharyngealdysfunction(VPD),and pri-mary palatoplasty should aimto establish the anatomical andfunctionalconditionsforproperclosureofthe velopha-ryngeal mechanism during speech.1,2 In general, speech disordersrelatedtoVPDarehypernasality,airemissionand compensatoryarticulation.3
The diagnosis of speech disorders resulting from VPD should be carried out through clinical and instrumental assessment.Theauditory-perceptualassessment is consid-ered thegold standard toassessspeech disordersrelated toVPDand cleft palate. Itis the method thatallows the identificationofthesealterations,theassessmentof their severity aswell as the evaluation of the effectivenessof performedtreatments.4,5 However,severalproceduresare usedtocollectandanalyzedataoftheperceptual assess-ment, making it difficult tocompare different studies,1,6
inadditiontothefactthatthisassessmentis subjective.7 As the auditory-perceptual assessment is susceptible to errorsduetoitssubjectivity,therehasbeenanincreasing desire to seek methods that could improve this evalua-tion.
Forinstance, the instrumentalacoustic analysisof the speechsignal, suchasthenasometry, wasdevelopedasa meansofcorroboratingtheperceptualtestsofspeech reso-nance.Thenasometerprovidesthedegreeof‘‘nasalance’’, whichis the average ratioof nasal/total(nasal plus oral) acoustic energy converted to a percentage value.8 The nasalancevaluereflectstherelativeamountofnasal acous-tic energy in an individual’s speech. The validity of the nasometertomeasurehypernasalityhasbeendemonstrated bymanyresearchers,9,10resultinginacceptanceanduseof nasometryinboth clinicalandresearchsettings.11,12 How-ever, somevariables mayhinderthe judgmentofnasality andinterferewiththeobtainedresults.
auditory-perceptualjudgmentbasedonrecordings;(3)Test ofHypernasality(THYPER);and(4)nasometry.
Methods
This wasa retrospective study thatused datafrom three typesofauditory-perceptualassessment:judgmentof nasal-ityperformed live andby judges, THYPER andnasometry of 331 patients (132 girls and 199 boys) with operated unilateral cleft lip and palate, submitted to these three evaluationsbetween5and13yearsofage.The studywas approvedbytheEthicsCommitteeinResearchwithHuman Beingson25March2014(Opinionnumber569,720).
The data were collected according to the following inclusion criteria: (a) the selected judgement of nasality performedlive,THYPERandnasometryhadtobeperformed duringthe patient’s same visit to the institution andhad tobe available in each patient’s medical record; (b) the selectedspeechrecordingsshouldalsohavebeenperformed onthepatient’ssamevisittotheinstitutionwhenheorshe wassubmittedtothejudgementofnasalityperformedlive and tonasometry. Only thoseassessments containing the followingfivesentenceswithlowpressureconsonantswere selected:Olouroiaolharalua(Theparrotwasgoingtosee themoon),Lauraliaaoluar(Laurareadbythemoonlight),
Aleoaé leal(The lionessis loyal),Lili eraloira (Lili was blond),Luluolhaaarara(Lululooksthemacaw).
Auditory-perceptualassessmentofspeechnasality performedlive
This judgment was carried out by an experienced speech/languagepathologistduringspontaneousspeechand repetition of words and phrases by the patients, using a four-pointscale(0=nohypernasality,1=mildhypernasality, 2=moderatehypernasalityand3=severehypernasality).
TestofHypernasality(THYPER)
Thistest involves therepetitionof 10two-syllable words, composedonlybytheconsonant[b]andoralvowels(babá,
bebê,bibi,bobó,bubu,baba,bebe,bobi,boba,buba),each repeatedtwice, one performed in the usualmanner with opennostrilsandanotherwithoccludednostrils.The ratio-naleforthetestinterpretationistheassumptionthatifthe patienthasvelopharyngealclosureduringwordutterance, thereis noperceptual change in resonancewith or with-outnostrilocclusion.However,ifthepatientdoesnothave velopharyngealclosure,thesoundproducedwillbedirected tothenasalcavity,causinghypernasality.Inthiscasethere will be noticeable change in the production of the same word when comparingutterance with and without nostril occlusion.
The final test scoreconsidersthe numberof words for whichthe evaluator heard thenoticeablechange in reso-nance.Scoresmayrangefrom0to10,indicatingthatthere wasnovariationintheresonanceofanyofthepairsofthe10 words,to10---10,indicatingresonancevariationinallpairs (Fig.1).
Figure1 PerformingtheTestofHypernasality.
Auditory-perceptualassessmentofspeechnasality throughrecordings
Speechsampleswerereadorrepeatedaftertheevaluator and recorded on audio simultaneously tonasometry. The recordings were made in a silent, sound-treated environ-ment, usingan AKGC420headset microphone,positioned 5cm from the mouth, and an Intel Pentium 4 computer (256MB15RAM),consistingofaCreativeAudigyIIsoundcard andusingSonySoundForgeprogram(2003),withasampling rateof44,100Hz,inasinglechannel,16bits.Theselected recordingswereeditedusingtheSonySoundForgePro10.0 softwareandrecordedintoaCD.
Totesttheintrajudgereliability,50(15%)sampleswere duplicated and inserted randomly into a file containing a totalof381sentences(331+50).Thesampleswerejudged bythreespeech/languagepathologists (judges)withmore than10yearsofexperienceinthediagnosisandtreatment ofVPDandcleftlipandpalate.Beforethejudgement,the judgeswentthroughatrainingsessionsotheycouldbecome familiarized withthe procedureandscale use.The recor-dingswereheardusingtheWindowsMediaPlayerprogram (MicrosoftWindows)andheadphones.
Thejudgeswereseatedinaquietroomandcompleted taskspresentedwithWindowsMediaPlayer(Microsoft Win-dows)overheadphones(AKGK414P)connectedtoastereo splitter. They should judge the recorded samples until a consensuswasreached.
Nasometricassessment
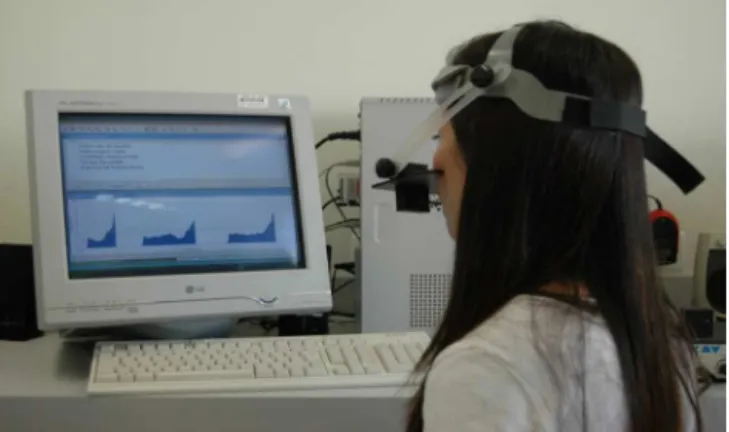
This assessment was performed by experienced speech/language pathologists, using a 6200-2 Pentium ByteOnnasometer,manufacturedbyKayElemetrics(1992). Theequipmentconsistsofamicrocomputer-basedsystem, in which the acoustic, oral and nasal speech energy is picked up by two microphones directed to the individ-ual’s mouth and nose, separated by a horizontal metal plate positioned above the upper lip during the speech sample recording. The setis held in positionby ahelmet (Fig.2).
Table1 Distributionofthenumberandpercentageofpatientsaccordingtotheoccurrenceofhypernasalityinthefourtypes ofassessment.
Methodsofassessment Occurrenceofhypernasality
Absentn(%) Presentn(%)
Liveperceptualjudgement 262(79%) 69(21%)
Judgmentbymultiplejudges 217(66%) 114(34%)
TestofHypernasalitya 263(79%) 68(21%)
Nasometry(cutoff=27%)b 188(57%) 143(43%)
a Scores(0---2),nohypernasality;scores(
≥3),withhypernasality.
b Scores(
≤27%),nohypernasality;scores(>27%),withhypernasality.
wereobtainedaftertherepetitionofthesamelowpressure phrasesdescribedabove.
Dataanalysis
Intrajudge agreement of the recorded samples was cal-culated using kappa statistics.13 To obtain the indices of sensitivity,specificityandoverallnasometerefficiency,the cut-offvalueof27%wasused.Theagreementpercentages ofthefourtypesofassessmentwerepresentedinpairs,by combiningtwo methods, usingkappa statistics.The com-parisonbetweentheresultsofthefourmodalitiesregarding theabsenceandpresenceofhypernasalitywascarriedout inpairs,usingtheMcNemartest,withasignificancelevelof
p<0.05.
Results
Theresultsregardingtheoccurrenceofhypernasalityinthe fourmodalitiesofassessmentareshowninTable1.
Theresultsofthenasalityjudgmentperformedliveare showninFig.3;theresultsofTHYPERscoreinterpretation areshowninTable2;theauditory-perceptualjudgmentof speechnasalitybyjudgesisshowninFig.4;thepercentage ofagreementlevel()betweenthefourtypesofassessment aredescribedinTable3;thecomparisonofthefour eval-uationmethodsisshowninTable4(comparedinsixpairs:
Figure2 Patientundergoingnasometry.
79%
12% 8%
1%
No hyper Mild hyper Moderate hyper Severe hyper
Live judgement classification in the four-point scale
Figure3 Distributioninpercentageoflivejudgement classi-ficationinthefour-pointscale.
Table2 DistributionofTHYPERscores withbinary inter-pretationofthefindingsandcalculationofthepercentage indicating absence (without hypernasality) and presence (withhypernasality).
THYPERscore Interpretation n(%)
0---2 Totalwithouthyper 263(79%)
3---10 Totalwithhyper 68(21%)
Scores(0---2),withouthypernasality;scores(3or>),with hyper-nasality.
livevs.THYPER;livevs.judges;livevs.nasometry;judges vs.nasometry;judgesvs.THYPER;THYPERvs.nasometry). Theresultsofsensitivity,specificityandoverall nasome-terefficiencyindiceswere62%,87%and76%,respectively.
66%
25%
8%
1% No hyper Mild hyper Moderate hyper Severe hyper
Recorded sample judgement by judges in the four-point scale
Table3 Percentagesofagreement(%)andvalueamong thefourtypesofassessment.
Nasalityassessment(%)
Modalities Live THYPER Judges
THYPER 95%(0.84)c ---
---Judges 79%(0.48)b 78%(0.45)b ---Nasometry 72%(0.40)a 73%(0.40)a 76%(0.50)b
aRegularagreement. b Moderateagreement. c Almostperfectagreement.
Discussion
Theresultsshowedthatthehighestpercentagesof hyper-nasality absence in the four modalities were obtained in the live judgement and THYPER, with equal results for both (79%). Lower percentages of hypernasality absence wereobtainedinjudgementof recordingsbyjudges(66%) andevenlowerresultswereobtainedinnasometry(57%). Padilha14 found 69% of hypernasality absence at the live judgement,72%inTHYPER,62%inthejudgementbyjudges and58%innasometry.
BothinthisstudyandinthestudybyPadilha,14theresults showedhighlevelofagreementbetweenthelivejudgement andTHYPER,contrarytotheagreementbetweentheother methodsofassessment,whichwasregularormoderate.In thepresent study,thissame paired comparison showeda significant difference, indicating that a larger number of patientswasidentifiedtohavehypernasalitybythe nasom-etrythanthroughthejudgementbyjudges.
Thesameoccurredwhenthefindingsofthelive judge-ment and THYPER were compared to results from the judgement by judges and nasometry, withthe number of patientsidentifiedwithhypernasalitybeingalwayslowerat thelivejudgementandTHYPER.Itwasalsoobservedthat thelivejudgementbyasingleevaluatorusingthefour-point scale and the THYPER scores had similarresults, but sig-nificantlydifferfromtheotherstudiednasalityassessment modalities.
Severalfactorsmayexplainthefindingsofthisstudy,such asthestimulususedtoobtainthespeechsamples,the eval-uator’sandthejudges’experienceandtraining,inaddition tothespeechvariablessuchascompensatoryarticulation, nasalsnort,dysphonia, amongothers.Lohmander etal.15
claim that the perceptual judgment of nasality is not an easytaskandreportthatthevariablesrelatedtothespeech material,theindividualcharacteristicsoftheevaluatorsand theirtimeofclinical experience,aswellasthequalityof recordings,forinstance,arethefactorsthatmostinterfere withresultreliability.
Henningssonetal.1affirmthatspeechsamplesmust con-sist of sentences containing pressure consonants and all kinds ofvowels, including highvowels. KuehnandMoon16 and Sweeney and Sell10 reportthat hypernasality is more likely to occur in the production of high vowels, due to theneed for greatereffort inthevelopharyngeal closure, andthatspeechsamplesdevoidofnasalconsonantsarenot representativeofspontaneousspeech,representingonlya partialsampleofhypernasality.
The qualityof the evaluator selected tocarry out the nasality judgment,both live andthrough recordings, is a factorthatdeservestobediscussed.Theevaluator’s expe-rienceinthediagnosisandevaluationofVPDfacilitatesthe performanceof theperceptualjudgment,whichincreases the study’s reliability and credibility.1,4,5,17 However, one mustconsiderthatevenexperiencedevaluatorsaresubject tointernal(lapsesofmemoryandattention,sleep,fatigue) andexternalvariables(relatedtotheenvironmentortothe sampleitself),whichmayinterferewithjudgment.18
EadieandBaylor19 suggestatheoreticalmodelofvoice qualityperception,emphasizingthatitiscommonfor listen-ers,whenjudgingvoicedimensions,toalsocomparethem withtheirinternal standard,suchashabits(or strategies) andindividualperceptualbiases,overallsensitivityforthe qualitytobejudged,fatigue,lapsesofattention, transcrip-tion errors,etc. The first threefactors canbe shaped by trainingorthelistener’sexperience,whileothersmustbe consideredasrandomerrors.
Some factors can interact with factors related to the judgmenttask.One,forinstance,istheabilityoflistenersto differentiateandinterpretdifferentpointsandintervalsin thesameclassificationscale.19Amongtheseseveralfactors, thoserelatedtolisteners’internalstandardshavereceived increasedattentioninvoiceresearch.
The literature in the voice area currently reports no significant association between demographic variables (age,level ofclinical experiencerelatedtovoice,speech pathology) and the listeners’ judgement of dysphonic voices.20,21Bodtetal.22claimthattheprofessionalspecialty (for instance, otorhinolaryngologists vs. speech/language pathologists)hasagreaterinfluenceontheperceptualvoice
Table4 Numberandpercentageofpatientswithhypernasality,accordingtothefourmethodsofassessmentanddifference betweenfindingsandpvalue.
Methodofassessmentn(%) Methodofassessmentn(%) Difference(%) p-Value
Live---69(21%) THYPER---68(21%) 1(0%) 1.000
Live---69(21%) Judges---114(34%) 45(13%) <0.001a
Live---69(21%) Nasometry---143(43%) 74(22%) <0.001a
THYPER---68(21%) Nasometry---143(43%) 75(22%) <0.001a
THYPER---68(21%) Judges---114(34%) 46(13%) <0.001a
Judges---114(34%) Nasometry---143(43%) 29(9%) <0.001a
judgmentthanthenumberofyearsofclinicalexperience, concludingthattheevaluator’sinexperiencehasno signif-icant impactoninterjudge reliability, providedtheyhave sometrainingpriortotheauditory-perceptualvoice judg-ment.
Several authors suggest that to improve the listeners’ reliability, the hypernasality judgement should be per-formed bya groupof evaluators(andnotjust one),after specific training to adjust the internal scale. During this training,theevaluatorsmustjudgereferencespeech sam-ples with varying degrees of nasality until they reach a consensus.15 It is presumed that internal standards for hypernasalityrepresentationareestablishedafterexposure tospeechsamples23andthattheymayvaryduetothe eval-uator’slevelofexperience.
Lewis,WattersonandHoughton,24forinstance,observed that experienced evaluators demonstrate better reliabil-itythan inexperiencedones, unlikesome reportsof voice studies in which experienced evaluators exhibited worse reliability than the inexperienced ones. The authors24 explainthatthisdiscrepancymayberelatedtothefactthat experiencedevaluatorsparticipatinginhypernasality stud-ies usually work together and, for this reason,may have developeda‘‘commonear’’overtime.
In the present study,the speech sampleswere judged by threespeech/languagepathologists withmore than 10 years’experienceinthediagnosisandtreatmentofspeech disordersinpatientswithcleftlipandpalate.Training ses-sionswerecarriedoutwithrecordedreferencesamplesfor the evaluators to identify the occurrence of hypernasal-ity and classify itspresence asmild, moderate or severe by consensus. As in the study by Padilha,14 the speech sample ofthisstudy consistedof continuouslyedited sen-tences, to form a single judgment block. Although the evaluators’training used the referencesamples from the study by Padilha,14 it wasobserved that the judgmentof hypernasalityabsence throughrecordingsproduced worse scores.
Theauditory-perceptualassessmentnotonlyassessesthe stateofspeechofanindividual,butalsoindirectlyprovides informationon velopharyngeal functionin the absenceof palatalfistula inthe populationwithcleft palate.25 Thus, itis necessarytohave areliableandvalidcomprehensive protocoltoassessspeech.Althoughitisacknowledgedthat theauditory-perceptual assessmentisconsidered thegold standard for the evaluation of speech disorders resulting fromcleft palate andVPD, it is alsorecognized that this approach maybe somewhat confusing.17 Sell5 states that a speech sample must contain the repetition of syllables andphrases,theproductionofdecoratedandspontaneous speech and a conversation sample, agreeing with Hut-tersandHenningsson,26 whoemphasizedthatthephonetic contentofthespeechsamplecaninfluencethe hypernasal-ityperceptionbylisteners.
Silva27 reported the importance of controlling some speech variables, such as the presence of compensatory articulationsandaudiblenasalsnort,asthesecaninterfere and hinder the auditory-perceptual judgment of nasality. Compensatoryarticulationsandnasalsnortseldomoccurin speechsamplesconsistingoflowpressureconsonants,most oftenoccurringwithhigh-pressuresamples.28
Thepresenceofdysphoniamayalsohinderthe auditory-perceptualassessment,asitmaydistorttheevaluationof thedegreeofhypernasalityandfurtherimpairthejudgment of speechintelligibility.29 As dysphoniaand compensatory articulationswerenotcontrolledvariablesinthisstudy,itis difficulttoaffirmwhethertheirpresenceinanypatienthad anyinfluenceontheresults.Therefore,itissuggestedthat futurestudiescontrolforthepresenceofthesealterations, astheymayactuallyinterferewithhypernasalityjudgment. As an alternative to solve the limitations of live auditory-perceptual evaluation, Lohmander and Olsson,6 Sell5andHenningssonetal.1allproposedthatthe auditory-perceptual judgement be carriedout by multiple judges, based onrecorded speech samples. They emphasize that therecordingisaresourcethatalwayscanbeonhandtobe usedwhenandasoftenasnecessary,aswellaseditedand presentedfortheauditory-perceptualjudgmentbymultiple judges,whichallowsvalidatingtheclinicalfindingsobtained duringtheliveassessment.
Lohmanderetal.6stressthattheuseofrecordingsallows obtaining intra- and interjudge reliability measurements, whichcontributestoincreasedscientific credibilityofthe results. This type of assessment, however, also has some disadvantagesthatshouldbeconsidered.Oneofthem con-cernsthetechnicalqualityofthespeechsamplerecording, whichcancaptureambientnoiseormightnotdetectenough acousticinformationtoallowthejudgetoidentifythe pres-enceofweakintraoralpressure,inaudibleairleakageand errorsrelatedtospeechproduction.26Anotheristhatduring theauditory-perceptualjudgment,thejudgecannotusethe patient’sexpressiontohelpclarifydoubtsorobserveother visualcluesavailableintheliveassessment.
Inthepresent study,theauditory-perceptualjudgment ofhypernasality,bothliveandinaudiorecordings,was car-riedoutusingthesamefour-pointscale usedbyPadilha.14 Theresultsofbothstudiesshowedthepredominanceofmild hypernasality in most judged patients with hypernasality speech.
According to Padilha,14 the auditory-perceptual judg-mentofmildhypernasalityisveryclosetothejudgement of absenceof hypernasalityon the scale, and the choice betweenoneandtheothermayhavebeenadifficulttask, especially in those patients likely to have fluctuations in nasality speech. Identifying the nasality at the extremes of the range (normal vs. severe hypernasality) has been mentioned by Sommerlad et al.7 as an easier task than identifyingsmallalterations.Inthisregard,theuseof instru-mental assessment has been recommended as a way to corroboratetheperceptualfindings.
Sweeney and Sell10 report the occurrence of a strong correlationbetweentheperceptualevaluationsofnasality andnasalance scores duetothe use ofcontrolled speech samplesandscalestoclassifyhypernasality.However, cor-relationsbetweennasalancescoresandauditory-perceptual judgmentsshouldbeinterpretedwithcaution.10
tomoderatebetweennasometryandtheotherthreetypes ofassessment,similartothefindingsofPadilha.14
Watterson,McFarlane andWright31 affirmthatthe fac-torthatcaninterfereinthecorrelationbetweennasalance scoresandlistener’sjudgmentsisassociatedwiththespeech stimuliusedinaudiorecordingsandnasometry.Brunnegård, Lohmanderand VanDoorn32 found a goodor moderate to goodcorrelationbetweennasalancescoresandperceptual judgmentamongtrainedspeechlanguagepathologistsand regulartomoderate amonguntrainedlisteners, and men-tionedthatother speechparameters,suchasarticulation andvoice,caninadequatelyinterferewiththehypernasality judgement.
Inthepresentstudy,thesensitivity,specificityand over-allefficiencyof thenasometerwereestablishedusingthe cut-offof 27% andmaintainingthe liveassessmentasthe gold standard. The results weresimilar tothose of Bran-camp,LewisandWatterson33andlowerregardingsensitivity whencomparedtothosefoundbyHardinetal.,30Watterson, LewisandDeutsch34andSweeneyandSell.10
Nevertheless, in ordertoobtain more informationand understandingofhypernasalityanditsevaluationintheVPD diagnosisafterprimarypalatoplasty,itis suggestedthata study be carried out with a large number of patients at differentagegroups,usingdifferentspeechsamples.
Conclusion
Weconcludethattheabsenceofspeechhypernasalitycan bebetterperceivedthroughtheauditory-perceptual judg-ment performed live and through THYPER, than by the perceptual judgement through recordings of speech sam-plesandnasometry.Althougheachmethodhasadvantages anddisadvantages,thebiggestadvantageofthelive assess-ment,whichisthegoldstandardfordetectingtheslightest occurrence of hypernasality, is the fact that it is easy to implementandthatitcanberepeatedwhenevernecessary. However,itsdisadvantageisthatthedatacannotbe repro-duced, or quantified, or shared by other members of the team,or comparedwith datafrom other centers. Future studies with greater control of the phonetic context of speechsamples arerequired toimprove the reliabilityof theauditory-perceptualjudgementofspeechnasality.
Funding
sources
ThisstudywassupportedbyFAPESP(Fundac¸ãodeAmparoà PesquisadoEstadodeSãoPaulo).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.HenningssonG,KuehnD,SellD,SweeneyT,Trost-Cardamone J,WhitehillT.Universalparametersforreportingspeech out-comesinindividualswithcleftpalate.CleftPalateCraniofacJ. 2008;45:1---17.
2.AgrawalK. Cleft palate repairand variations. IndianJPlast Surg.2009;42Suppl:102---9.
3.Kummer AW, Clark SL, Redle EE, Thomsen LL, Billmire DA. Currentpracticeinassessing andreportingspeechoutcomes ofcleftpalateand velopharyngealsurgery: asurvey ofcleft palate/craniofacial professionals. Cleft Palate Craniofac J. 2012;49:146---52.
4.SmithB,GuyetteTW.Evaluationofcleftpalatespeech.Clin PlastSurg.2004;31:251---60.
5.Sell D. Issues in perceptual speech analysis in cleft palate and relateddisorders: a review. IntJLang Commun Disord. 2005;40:103---21.
6.LohmanderA,OlssonM.Methodologyforperceptualassessment ofspeechinpatientswithcleftpalate:acriticalreviewofthe literature.CleftPalateCraniofacJ.2004;41:64---70.
7.SommerladBC,MehendaleFV,BirchMJ,SellD,HatteeC, Har-land K. Palate re-repair revisited. Cleft Palate Craniofac J. 2002;39:295---307.
8.SweeneyT, SellD,O’Regan M.Nasalance scoresfor normal-speaking Irish children. Cleft Palate Craniofac J. 2004;41: 168---74.
9.Whitehill TL. Nasalance measures in Cantonese-speaking women.CleftPalateCraniofacJ.2001;38:119---25.
10.Sweeney T, Sell D. Relationship between perceptual ratings ofnasality and nasometryinchildren/adolescents withcleft palateand/orvelopharyngealdysfunction.IntJLangCommun Disord.2008;43:265---82.
11.Genaro KF, Yamashita RP, Trindade IEK. Avaliac¸ão clínica e instrumental na fissura labiopalatina. In: Fernandes FDM, MendesBCA,NavasALPGP,editors.TratadodeFonoaudiologia. 2nded.SãoPaulo:Roca;2010.p.488---503.
12.Fukushiro AP, Trindade IE. Nasometric and aerodynamic outcome analysis of pharyngeal flap surgery for the man-agement of velopharyngeal insufficiency. J Craniofac Surg. 2011;22:1647---51.
13.LandisJR,KochG.Themeasurementofobserveragreementfor categoricaldata.Biometrics.1977;33:159---74.
14.Padilha EZ. Nasalidade e nasalância de fala na fissura labiopalatinaDissertac¸ão.Bauru:FaculdadedeOdontologiade Bauru,UniversidadedeSãoPaulo;2013.
15.LohmanderA,WilladsenE,PerssonC,HenningssonG,Bowden M,HuttersB.Methodologyforspeechassessmentinthe Scand-cleftproject---aninternationalrandomizedclinicaljudgement onpalatalsurgery:experiencesfromapilotstudy.CleftPalate CraniofacJ.2009;46:347---62.
16.KuehnDP,MoonJB.Velopharyngealclosureforceandlevator velipalatiniactivationlevelsinvaryingphoneticcontexts.J SpeechLangHearRes.1998;41:51---62.
17.JohnA,SellD,SweeneyT,Harding-BellA,WilliamsA.Thecleft auditingprotocolforspeech-augmented:avalidatedand reli-ablemeasureforauditingcleftspeech.CleftPalateCraniofac J.2006;43:272---88.
18.BaylisAL, Munson B,Moller KT.Perceptions ofaudiblenasal emissioninspeakerswithcleftpalate:acomparativestudyof listenerjudgments.CleftPalateCraniofacJ.2011;48:399---411. 19.EadieTL,BaylorCR.Theeffectofperceptualtrainingon inex-perienced listeners’ judgments ofdysphonic voice. J Voice. 2006;20:527---44.
20.EadieTL,KapsnerM,RosenzweigJ,WaughP,HillelA,Merati A.Theroleofexperienceonjudgmentsofdysphonia.JVoice. 2010;24:564---73.
21.Fang-lingL,MattesonS.Speechtasksandinterraterreliability inperceptualvoiceevaluation.JVoice.2014;28:725---32. 22.BodtMS,WuytsFL,VandeHeyningPH,CrouxC.Test-retest
studyoftheGRBASscale:influenceofexperienceand profes-sionalbackgroundonperceptualratingofvoicequality.JVoice. 1997;11:74---80.
24.LewisKE, Watterson TL, Houghton SM.The influence of lis-tenerexperienceandacademictrainingonratingsofnasality. JCommunDisord.2003;36:49---58.
25.Moon JB. Evaluation of velopharyngeal function. In: Moller KT,StarrCD,editors.Cleftpalateinterdisciplinaryissuesand treatment:forcliniciansbyclinicians.Austin:Pro-ed;1993.p. 251---306.
26.Hutters B, Henningsson G. Speech outcome following treatment in cross-linguistic cleft palate studies: method-ological implications. Cleft Palate Craniofac J. 2004;41: 544---9.
27.Silva L. Medidas de nasalância da fala de crianc¸as com fissura labiopalatina e sua correlac¸ão com o julgamento perceptivo-auditivoda nasalidade Dissertac¸ão.Bauru: Facul-dade de Odontologia de Bauru, Universidade de São Paulo; 2007.
28.PrandiniEL,Pegoraro-KrookMI,DutkaJCR,MarinoVCC. Occur-rence of consonant production errors inliquid phonemes in childrenwithoperated cleft lipandpalate. JApplOralSci. 2011;19:579---85.
29.NagarajanR,SavithaVH,SubramaniyanB.Communication dis-orders inindividuals with cleftlip and palate: an overview. IndianJPlastSurg.2009;42:137---43.
30.Hardin MA, Van Demark DR, Morris HL, Payne MM. Corre-spondencebetween nasalancescoresand listenerjudgments of hypernasality and hyponasality. Cleft Palate Craniofac J. 1992;29:346---51.
31.WattersonT,MCFarlaneSC,WrightDS.Therelationshipbetween nasalanceandnasalityinchildrenwithcleftpalate.JCommun Disord.1993;26:13---28.
32.BrunnegårdK,LohmanderA,VanDoornJ.Comparisonbetween perceptualassessmentsofnasalityandnasalancescores.IntJ LangCommunDisord.2012;47:556---66.
33.BrancampTU,LewisKE,WattersonT.Therelationshipbetween nasalance scores and nasality ratings obtained with equal appearing interval and direct magnitude estimation scaling methods.CleftPalateCraniofacJ.2010;47:631---7.