Brazilian
Journal
of
OTORHINOLARYNGOLOGY
www.bjorl.org
ORIGINAL
ARTICLE
Auditory-perceptual
analysis
of
voice
in
abused
children
and
adolescents
夽
,
夽夽
Luciene
Stivanin
a,∗,
Fernanda
Pontes
dos
Santos
a,
Christian
César
Cândido
de
Oliveira
a,
Bernardo
dos
Santos
b,c,
Simone
Tozzini
Ribeiro
a,
Sandra
Scivoletto
aaDepartmentandInstituteofPsychiatry,HospitaldasClínicas,FaculdadedeMedicina,UniversidadedeSãoPaulo(FM-USP),São
Paulo,SP,Brazil
bInstituteofMathematicsandStatistics,UniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
cInstituteofPsychiatry,HospitaldasClínicas,FaculdadedeMedicina,UniversidadedeSãoPaulo(FM-USP),SãoPaulo,SP,Brazil
Received2September2013;accepted5August2014 Availableonline25November2014
KEYWORDS Childabuse; Voice;
Communication disorders; Childhealth
Abstract
Introduction:Abusedchildrenandadolescentsareexposed tofactorsthatcantrigger vocal changes.
Objective: Thisstudy aimedtoanalyze theprevalenceofvocalchanges inabusedchildren andadolescents,throughauditory-perceptualanalysisofvoiceandthestudyoftheassociation betweenvocalchanges,communicationdisorders,psychiatricdisorders,andglobalfunctioning.
Methods:This was anobservational and transversal study of136 children and adolescents (meanage10.2years,78 male)who wereassessedby amultidisciplinaryteamspecializing inabused populations.Speechevaluationwas performed(involving theaspects oforal and writtencommunication,aswellasauditory-perceptualanalysisofvoice,throughtheGRBASI scale).PsychiatricdiagnosiswasperformedinaccordancewiththeDSM-IVdiagnosticcriteria andbyapplyingtheK-SADS;globalfunctioningwasevaluatedbymeansoftheC-GASscale.
Results:Theprevalenceofvocalchangewas67.6%;ofthepatientswithvocalchanges,92.3% hadothercommunicationdisorders.Voicechangeswereassociatedwithalossofsevenpoints in global functioning,and therewas noassociation between vocalchanges andpsychiatric diagnosis.
夽 Pleasecitethisarticleas:StivaninL,dosSantosFP,deOliveiraCC,dosSantosB,RibeiroST,ScivolettoS.Auditory-perceptualanalysis
ofvoiceinabusedchildrenandadolescents.BrazJOtorhinolaryngol.2015;81:71---8.
夽夽
Institution:ProgramaEquilíbrio,DepartamentoeInstitutodePsiquiatriadoHospitaldasClinicas,FaculdadedeMedicinadaUniversidade deSãoPaulo(FM-USP),SãoPaulo,SP,Brazil.
∗Correspondingauthor.
E-mail:stivanin@usp.br(L.Stivanin). http://dx.doi.org/10.1016/j.bjorl.2014.11.006
Conclusion:Theprevalenceofvocalchangewasgreaterthanthatobservedinthegeneral pop-ulation,withsignificantassociationswithcommunicationdisordersandglobalfunctioning.The resultsdemonstratethatthesituationsthesechildrenexperiencecanintensifythetriggering ofabusivevocalbehaviorsandconsequently,ofvocalchanges.
© 2014Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE Maustratosinfantis; Voz;
Transtornosda comunicac¸ão; Saúdeinfantil
Análiseperceptivo-auditivadavozdecrianc¸aseadolescentesvítimasdemaustratos
Resumo
Introduc¸ão:Crianc¸aseadolescentesvítimasdemaustratosestãoexpostasafatoresquepodem desencadearalterac¸õesvocais.
Objetivo:Analisar a prevalência de alterac¸ão vocal nesta populac¸ão realizando análise perceptivo-auditiva da voz e estudar a associac¸ão entre alterac¸ão vocal, transtornos da comunicac¸ão,transtornopsiquiátricoefuncionamentoglobal.
Método: Estudoobservacionaletransversal.Participaram136sujeitos,comidademédiade 10,2anos,atendidosporequipemultidisciplinarespecializadanotratamentoambulatorialde vítimasdemaustratos.Foirealizadaavaliac¸ãofonoaudiologia(aspectosdacomunicac¸ãooral eescritaeanáliseperceptivo-auditivadavozaqualfoifeitapormeiodaescalaGRBASI).O diagnósticopsiquiátricofoidadodeacordocomoscritériosdiagnósticosdaCID-10eaplicac¸ão doK-SADS;ofuncionamentoglobalfoiavaliadopormeiodaescalaC-GAS.
Resultados: Aprevalênciadealterac¸ãovocalfoide67,6%,dospacientescomalterac¸ãovocal, 92,3%apresentaramoutrostranstornosdacomunicac¸ão.Aalterac¸ãovocalestáassociadaaum prejuízodesetepontosnofuncionamentoglobalenãoapresentouassociac¸ãocomtranstorno psiquiátrico.
Conclusão:A prevalênciade alterac¸õesvocaisencontrada foi maiordoqueaobservadana populac¸ãogeral, comassociac¸õessignificantescomtranstornos dacomunicac¸ãoe funciona-mentoglobal.Assituac¸õesqueestascrianc¸asvivempodemintensificarodesencadeamentode comportamentosvocaisabusivoseconsequentementedealterac¸õesvocais.
©2014Associac¸ãoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Violence against children and adolescents is considered to be a public health problem due to the many nega-tiveconsequencestobiopsychosocialdevelopment,1suchas
internalizingandexternalizing problems,2,3 belowaverage
intellectual function,3 academic and school performance
impairment,4,5 aswell asoral andwritten communication
disorders.6,7
Orallanguage,oneofthemostelaborateformsofhuman
communication,allowsthechildtoorganizehis/her
percep-tions,acquireknowledge,andbuildmemories.Itprovides
notonlysocialinteraction,butalsothelearninganduseof
rulestoregulateone’sownbehaviorandemotionalstate.8
Orallanguageacquisitiondisorderscanimpairlearning9and
causesocial,emotional,andbehavioralproblems.10,11
Successful communication depends not only on the
content of what is said, but also on the manner and
attitudethat thespeaker assumes duringthe interaction.
Specifically,facialexpressionsandvocalmodulationsduring
oral emission convey the speaker’s emotional state and
intention.12Thus,theproductionandrecognitionofspecific
characteristics of the speaker contribute to effective
communication.
The voice is an innate neurophysiological function,
resultingfromasophisticatedmuscularprocessing.Through
itsflexibility,itactsasasensitiveindicatorofthespeaker’s
emotions, attitudes, physical condition, and sociocultural
role.13
Anydifficulty or alteration in vocal emission that
pre-vents natural voice production characterizes dysphonia,14
an increasinglycommonobservation,withaprevalence of
6%---37%.15---17
Genetic and environmental components influence the
onset of vocal symptoms in different ways: the genetic
effectismoderate,whiletheenvironmentaleffectsarethe
moreimportantfactorsintheonsetofdysphonia.18
The causes of dysphonia include premature birth;19
nasal obstruction;20 allergic pulmonary reactions, such as
asthma and bronchitis; gastroesophageal reflux; auditory
symptoms;16 and sleeping problems.21 The main cause,
however,isvocalabusebychildren,asindicatedbystudies
with dysphonic children (90.3%,22 45.2%,23 and 54.67%24).
Therapidandcontinuouscollisionofthevocalfoldsduring
phonationcausestraumatothemucosalcapillaries,edema,
andinitiatestheprocessofnoduleformation.Lesionssuch
as cysts, sulci, paralysis, and papillomatosis may also
Knowing that voicechanges in childhood can interfere
withemotionaldevelopmentandsocializationofchildren,25
the identification and care of these disorders are
impor-tanttoallowfor thechild’sglobal functioning,helpingto
promotephysicalandemotionalhealth.
Childhoodvictimsofabuseareexposedtosomefactors
relatedtodysphonia,astheygrowinenvironmentswhere
yelling is very common among adults. The street
experi-encealsobecomesanaggravatingfactor.Yellingveryoften
becomesawayofstandingupforoneselfinthefaceof
dif-ficulties,inadditiontothefactthat theseindividualsare
directlyexposedtoenvironmentalaggressions(from
pollu-tion toclimate aspects) and drug use. It is, therefore, a
populationmorelikelytoshowchangesinvocalpatterns.
The aim of this study was to assess the prevalence
of voice disorders in this population and the
associa-tionofthesechangeswithothercommunicationdisorders,
psychiatric disorders, and global functioning through the
auditory-perceptual analysisof voicein childrenand
ado-lescentsvictimsofabuse.
Methods
Across-sectional observational studywasconducted after
the approval of the Research EthicsCommittee, protocol
number4353.
The participants were 136 children and adolescents
treatedbetweenJanuary2010andJuly2012bya
multidisci-plinaryteamspecializinginoutpatienttreatmentofvictims
ofabuse.Thesechildrenarereferredtothisservicebythe
technicalstaffofthe shelterswhere theyliveor byChild
ProtectiveServices.Themeanageofparticipantswas10.2
years,and78%weremales.The criteriafor patient
inclu-sioninthestudy wereage6---18 years;at leastonesocial
diagnosis(Z55---Z65---Personswithpotentialhealthhazards
relatedtosocioeconomicandpsychosocialcircumstances),
accordingtotheInternationalClassificationofDiseases
(ICD-10),26andconsentfromtheguardianforparticipationinthe
research.
Thosewithneurologicalproblemsandpsychiatric
symp-tomsthatcouldimpairtheunderstandingoftheevaluation,
such as patients with delusions, were excluded. Patients
who were already undergoing speech therapy were also
excluded.
Forthespeechtherapy assessment,specific testswere
usedintheareasoforallanguage,27,28 writtenlanguage,29
andspeech.30Thediagnoseswereclassifiedasphonological
disorders, alteration of semantic-syntactic skills, changes
inpragmaticcapacities,receptive-expressivelanguage
dis-order,writtenlanguagedisorder,articulationdisorder,and
dysfluency.
Forvoiceanalysis,samplesofspontaneousspeechwere
collected,aswellasofconnectedspeech,vocalemissions,
andsingingvoice,recordedonadigitalrecorder;oralmotor
assessmentwasalsoperformed.Clearandsimplelanguage
wasusedtoassessthechild/adolescent,andtheprocedure
wasexemplifiedtofacilitatethetestunderstanding.
Several times, more than one speech sample was
col-lected,toensurethesubsequentanalysis.Speechsamples
were submitted to auditory-perceptual analysis by
audi-ologists using the GRBAS31 scale, which characterizes the
patternofchange,tobeclassifiedas0(nodysphonia)and
1,2,and3(presenceofdysphonia).TheJapaneseGRBASI
scale,usedinternationally,isacompactandreliablemethod
ofassessingtheglobaldegreeofdysphonia(G)by
identify-ingkeyfactorswhendefiningadysphonicvoice:roughness
(R),breathiness(B),asthenia(A),strain(S),andinstability
(I).Forgreater data reliability,two other speech
pathol-ogistsspecializedinvoicewereaskedtoparticipate.After
listeningtotherecordedmaterial,theycompletedthesame
evaluation protocol. Samples whose analyses showed no
agreementwereexcludedfromthesample.
Psychiatric diagnoses were made by psychiatrists
spe-cializedin child and adolescent psychiatry. The Schedule
for Affective Disorders and Schizophrenia for School-Age
Children/Present and Lifetime Version (K-SADS-PL)32 was
appliedanddisorderswereclassifiedaccordingtothe
DSM-IV.
TheChildren’sGlobalAssessmentScale(C-GAS)involves
clinicalappraisalofthegenerallevelofpatientfunctioning
basedontheirbehaviorathome,withthefamily,atschool,
withfriends andduringleisure activities in thelast three
months.The scores range from1 to 100, and scores >70
indicatenormality.33
Data
treatment
Adescriptiveanalysisoftheresultsregardingthe
percent-age of patients with voice disorders was performed, by
gender and age. Analyses of associations between vocal
changeandthepresenceofpsychiatricandcommunication
disordersweremeasuredthroughFisher’sexacttest.34
Com-parisonofmeasuresofglobalfunctioning(C-GAS)between
groups wasperformed usingtheKruskal---Wallis,35 andthe
posthocwasperformedusingtheWilcoxon-Mann---Whitney
testwithBonferronicorrectionformultiplecomparisons.All
analyseswereperformedusingSPSS,release14.36
Results
According to the auditory-perceptual analysis of voice,
67.6% (n=92) of the patients had vocal changes, 79.3%
(n=72)wereyoungerthan12years,and56.5%weremales.
Therewasnostatisticaldifferencebetweenthegroups of
malesandfemales(p=0.423).
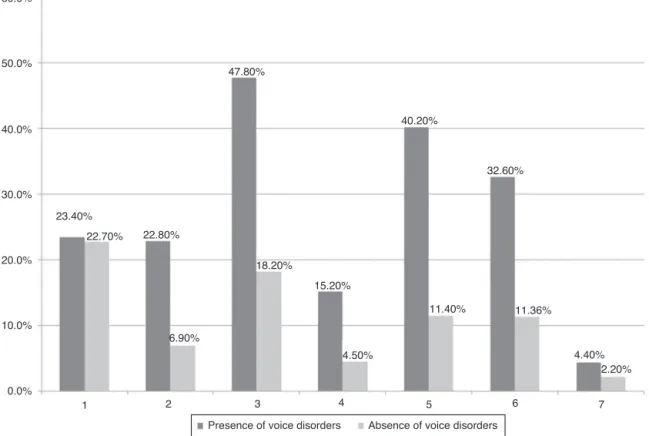
Mostsubjectswithvoicechanges(92.3%)alsohadother
communicationdisorders,asshowninFig.1.Theassociation
betweenthepresenceofvocalchange andcommunication
disorder was statistically significant in pragmatic
disor-ders(p=0.001), articulationdisorders(p=0.011),changes
insemantic-syntacticskills(p=0.029),receptive-expressive
language disorders (p=0.005), and written language
dis-order (p=0.000), indicating that individuals with these
disordersshowedahigherprevalenceofvoicechanges.The
pragmaticdisorder may increase the occurrence of vocal
changeby3.6-fold(p=0.004)andthephoneticdisorder,by
3.1-fold(p=0.034).
Fig.2showsthepercentageofpresenceandabsenceof
vocal disordersin psychiatricdisorders,distributedin the
most prevalent DSM-IV diagnostic categories in this
sam-ple. Although a higher proportion of voice changes was
1 2 3 4 5 6 7
11.40% 11.36%
4.40% 2.20% 4.50%
15.20%
32.60% 40.20%
18.20%
6.90% 22.80% 22.70%
23.40%
10.0% 20.0% 30.0% 40.0% 50.0% 60.0%
47.80%
0.0%
Absence of voice disorders Presence of voice disorders
Figure1 Associationbetweenvoicedisordersandotherdisordersoforalcommunicationin136childrenandadolescentvictimsof abuse(1,Phonologicaldisorder;2,Alterationinsemantic-syntacticskills;3,Alterationinpragmaticskill;4,Receptive-expressive languagedisorder;5,Writtenlanguagedisorder;6,Articulationdisorder;7,Speechdisfluency).
50.0%
45.0%
40.0%
35.0%
30.0%
25.0%
20.0%
15.0%
10.0%
5.0%
0.0%
F30 - F39 F70 - F79 F90 F91 F92 F98.0 - F98.1
14.10%
6.81%
20.50% 33.70%
14.10%
9.10%
4.30%
0%
10,90% 18,20% 36.40%
31.50%
Presence of voice disorders Absence of voice disorders
60.73
57.23
55.21
46.7 70
60
50
40
30
20
10
0
Without dysphonia and psychiatric disorder (n=15)
Only dysphonia (n=22)
Only psychiatric disorder (n=29)
Dysphonia + psychiatric disorder (n=70)
Figure3 Globalfunctioning(CGAS)ingroupsofchildrenwithvoiceand/orpsychiatricdisorders(n=136).
retardation,therewasnostatisticallysignificantassociation
between thesevariables (mood disorders,p=0.697;
men-talretardation,p=0.266;hyperkineticdisorders,p=0.159;
disordersofconduct,0.581;mixeddisordersofconductand
emotions,p=0.304;enuresisandencopresis ofnonorganic
origin,p=0.282).
To verify the subjects’ global functioning, they were
divided into four groups according to the presence or
absenceofvocalandpsychiatricdisorders.Themeanglobal
functioning(C-CGAS)foreachgroupwasbelowthelevelof
normalityandcanbeseeninFig.3.
The global functioning scoresof participants without a
disorder and in groups with vocal changes or psychiatric
disorderswerefoundtobebetween51and60,which
cor-responds to children with some problems in more than
one area. Participants who have voice changes and
psy-chiatric disorders have a global functioning in the range
41---50, which corresponds to children with obvious
prob-lems, deficits in most areas, or severe deficits in one
area. Statistical analysis showed no association between
voicechangesandpsychiatricdisorders(p=0.289)forglobal
functioning. However, the presence of voice change was
associatedwithalossofsevenpointsintheCGAS(p=0.002),
whereasthepresenceofapsychiatricdisorderwas
associ-atedwithalossof8.6points(p<0.001).
Discussion
The aimofthisstudy wastodetermine theprevalenceof
vocalchangesinchildrenandadolescentvictimsofabuse,
andto study theassociation between voicedisorders and
communicationandpsychiatricdisorders,aswellasglobal
functioning.
The results indicate a prevalence of voice disorders
higher than that observed in the general population;
higher prevalence of voice disorders in individuals with
communicationdisorders(significantassociation);no
signif-icant association between voicedisorders and psychiatric
disorders;andassociationbetween voicechangesandloss
ofsevenpointsinglobalfunctioning.
Weobservedahigherprevalenceofvoicedisordersthan
thatdescribedinstudiesonchildhooddysphonia,wherethe
prevalencerangesfrom6%to37%15---17;thissuggeststhatthe
factorstowhichchildrenandadolescentvictimsofabuseare
exposedmayincreasetheriskforthedevelopmentofvocal
disorders.
Deviantvocal behaviorisaformofinteraction,
aggres-sion,leadership,andawaytobecomeacceptedbyagroup,
andrepresentstheresultoftheinteractionofanatomical,
physiological,social,emotional,orenvironmentalfactors.37
One of the factors that couldtrigger voicechanges in
thisstudy populationwasthedisorganizedenvironmentin
whichtheylivedorstilllive.Familieswithtroubled
dynam-ics,crowded sheltersandlack ofindividualizedattention,
or even the streets, where the most efficient
communi-cationis notalways thesociallyaccepted type,arethree
riskfactorsfortheonsetofvocaldisorders.Theindividual
producesvocalmodulations thatarespecificforeachtype
of situation experienced (happiness, sadness, and anger,
amongothers)and environmentalfactors can causethem
tomake motor adjustments andchange the physiological
mechanisms,sothatthevoicemeetstheir needs.Studies
indicate that factors such as divorce, separation,
abnor-mal life conditions, too many adults in the environment,
impaired parent---child relationships, and unusual kinship
relationswereassociatedwiththeincidenceofdysphoniain
42%oftheassessedchildren.13 Childrenborntodepressed
mothersarelessresponsivetofacesandvoiceandinteract
lesswiththeirmothers.38
Ifthesechildren andadolescences need tochange the
vocal pattern tomeet their communication needs, it can
beinferredthatan impediment(whetherorganicor
func-tional)insomeaspectofmessagetransmissioncanworsen
thevocaldisorderandintensifyvoicechanges.Distortionsin
theproductionofspeechsoundsduetochangesinthe
posi-tionoftheteethinthedentalbite,inthetoneofthelips,
ofthephonoarticulatorytract,andcanalsocausevocal
dis-orders. Similarly, children with fewer language resources
tounderstand the environment and work out their needs
throughanefficientspeech,makeuseofothermeanssuch
asyelling, interrupting, crying, talking excessively,which
characterizesan abusive vocal behavior that alsotriggers
voicealterations.
Other disordersofcommunication, notassessed inthis
study,suchashearinglossandauditoryprocessing
difficul-ties,aremorecommoninchildrenandadolescentvictimsof
abuse,39whichpreventstheauditoryfeedbackoftheirown
speechandcausesdisordersinthevocalfoldmovement.
Althoughnoassociationwasobservedbetweenvocaland
psychiatricdisordersinthisstudy,itisknownthatabused
individualsexhibitcertaincharacteristics,suchaslow
self-esteem;lowtolerancetofrustration;difficultyestablishing
trustandattachment;andbehavioral,communication,and
interpersonal skill problems. Behaviors such as agitation,
motorrestlessness,impulsiveness,inattention,anxiety,and
insecuritylead toabusive and prolonged vocal behaviors,
suchastalkingtoomuchoratanincreasedspeechvelocity,
raisingthevocalintensity,yelling,andsuddenvocalattack,
whichoverloadstheapparatus.
For instance, a high-pitched voice may in some cases
reflecttensionintheintrinsicmusclesofthelarynx
result-ingfromanxietystates. Moreinsecureindividuals tend to
usea higher-pitched voiceand lowerintensity, word
pro-nunciationtendstobeimprecise,andtheynormallyusea
morerestricted voicemodulation, which cangive amore
monotonousspeech.40,41
Changesinbehavior,withphysicalandverbalaggression,
often appear to substitute the socially structured
behav-iorandcommunicationinchildrenandadolescentsatsocial
risk.Thisformofexpressionisessentialinthestreets,and
isoftenrelatedtosurvivalandanimportantpossibilityto
demonstratethefeelingsofbeingignoredbysociety---itis
awaytobeseenandheardin relationtotheirneedsand
desires.Moreover,inshelters,episodesofpsychomotor
agi-tation can beinterpreted asa clear sign of the need for
individualizedattention.Thus,onemustconsiderthatthis
typeofbehaviorandexpression,bothphysicalandverbal,
ispartoftheinteractionprocessofthesechildrenwiththe
worldaroundthemandthatithasitsrole.42
Therewasnodifferencebetweengendersforvoice
alter-ations, which differs from other studies that indicated a
prevalenceofvoicedisordersinboys.22---24,43,44 Researchers
highlight thatthe behavior of boysis more impulsiveand
aggressive than that of girls, who more typically exhibit
hyperactivity,anxiety,andleadership;themalebehaviour
when translated to the phonation mechanisms results in
vocalabuse.However,amongthepopulation ofvictimsof
abuse,girlsalsoneedtheabusiveuseofvoiceto
communi-cateandmeettheirneeds,whichcouldexplaintheabsence
ofgenderdifferencesinthisstudy.
Difficultiesin communication and behavioral and
emo-tional problems cause impairment of social skill,45,46 as
well as academic achievement and school engagement
limitations,47whichcharacterizesaglobalfunctioningthat
is below expectations. Although the vocal change has an
impact on overall health, on communication efficiency,
oneducationaland socialdevelopment,self-esteem,
self-image,andparticipationingroupactivities,48inthepresent
study a causal association between voice disorders and
globalfunctioningcouldnotbeinferred,giventhe
complex-ityoftheinvolvedfactors.
Anotherlimitationreferstothevocalassessmentused.
The scale used in the present study for the
auditory-perceptualanalysisofvoicewasemployedinother recent
studies andconsidered tobean excellent means ofvocal
assessment.16,49 However,theresearcherssuggestthe
per-formance of otorhinolaryngological examinationstoverify
thepresenceofvocalfoldlesions.
Martinsetal.24 identified57.5%ofvocal nodulesatthe
videolaryngoscopicassessment.Inthisstudy,patientswere
initiallyreferredtotheotorhinolaryngologyserviceof the
city health care network for examination and treatment,
ifnecessary.However,theauthorsdonothave theresults
of these evaluationsyet, which theyintendtoaddress in
afuturestudy.Anothersalientpointis thatthechildren’s
attitudesandthoseoftheirinterlocutorswerenotassessed
inthephysical, social/emotional,andfunctionaldomains.
Theauthorsindicatetheinclusionofsubjectivevoice
analy-sisthroughinterviewswithparents/tutorsandthechildren
themselves,inordertoincludespecifictechniquestoreduce
theabusivevocalbehavior.50
Conclusion
Childrenvictimsof abusehavea highprevalence ofvoice
disorders,mainlyassociatedwithcommunicationdisorders
and impaired global functioning. Characteristics of this
population, such as living in unsanitary places, disturbed
interpersonalrelationships,behavioralandemotional
prob-lems, and communication difficulties can constitute a
complex picture associated with abusive vocal behavior.
Otorhinolaryngologicalevaluation,aswellastheassessment
oftheattitudesofchildrenandcaregivers, shouldbe
con-sidered inordertocomplementthevocal assessment and
improvethemanagementofthispopulation.
Funding
This study was supported by Research Grant --- Fundac¸ão
FaculdadedeMedicina.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Gilbert R, Widom CS, Browne K, Fergusson DM, Elspeth W, Janson S. Child maltreatment 1: burden and consequences of child maltreatment in high-income countries. Lancet. 2009;373:68---81.
2.TerrLC.Childhoodtraumas:anoutlineandoverview.JLifelong LearnPsychiatry.2013;1:323---33.
4.Sullivan PM, Knuston JF. The prevalence of disabilities and maltreatment among runaway children. Child Maltreatment Neglect.2000;24:1275---88.
5.PerlmanS,FantuzzoJ.Timingand influenceofearly experi-encesof child maltreatmentand homelessness onchildren’s educationalwell-being.ChildYouthServRev.2010;32:874---83. 6.EigstiIM, Cicchetti D.The impactof child maltreatment on
expressivesyntaxat60months.DevSci.2004;7:88---102. 7.StivaninL,OliveiraCCC,ScivolettoS.Levantamentopreliminar
de patologias na comunicac¸ão oral em crianc¸as e adoles-centesemsituac¸ãodevulnerabilidadesocial.In:16◦Congresso
BrasileirodeFonoaudiologia,CamposdoJordão,SP, Anaisdo congressoemCDR.2008.
8.Bolter NI, Cohen NJ. Language impairment and psychiatric comorbidities.PediatrClinNorthAm.2007;54:525---42. 9.BüttnerG,HasselhornM.Learningdisabilities:debateson
def-initions,causes,subtypes,andresponses.IntJDisDevEduc. 2011;58:75---87.
10.TommerdahlJ.Whatteachersofstudents withSEBDneedto knowaboutspeechandlanguagedifficulties.EmotBehav Diffi-cult.2009;14:19---31.
11.KreismanNV,JohnAB,KreismanBM,HallJW,CrandellCC. Psy-chosocialstatusofchildrenwithauditoryprocessingdisorder.J AmAcadAudiol.2012;23:222---33.
12.MostT,AmirN,DotanG,WeiselA.Auditoryandvisualaspects ofemotionproductionbychildrenandadults.JSpeechLang Pathol.2008;2:24---31.
13.Maia AA, Gama ACC, Michalick-Triginelli MF. Reac¸ão entre transtorno do déficit de atenc¸ão/hiperatividade, dinâmica familiar,disfoniaenódulovocalemcrianc¸as.RevCiênc Médi-cas.2006;15:379---89.
14.LeHucheF,AllaliAA.Voz:patologiavocaldeorigemfuncional. 2nded.PortoAlegre:ArtmedEditora;2005.
15.Carding PN, Roulstone S, Northstone K. The prevalence of childhood dysphonia: a cross-sectional study. J Voice. 2006;20:623---30.
16.TavaresELM, BrasolottoA, Santana MF, Padovan CA,Martins RHG.Epidemiologicalstudyofdysphoniain4---12year-old chil-dren.BrazJOtorhinolaryngol.2011;77:736---46.
17.TavaresELM,LabioRB,MartinsRHG.Normativestudyofvocal acousticparametersfromchildrenfrom4to12yearsofage withoutvocalsymptoms:apilotstudy.BrazJOtorhinolaryngol. 2010;76:485---90.
18.Nybacka I, Simberg S, Santtila P, Sala E, Sandnabba NK. Genetic and environmental effects on vocal symptoms and their intercorrelations. J Speech Lang Hear Res. 2012;55: 541---53.
19.GartenL,SalmA,RosenfeldJ,WalchE,BührerC,HüsemanD. Dysphoniaat12monthscorrectedageinvery low-birth-weight-bornchildren.EurJPediatr.2011;170:469---75.
20.LabioRB,TavaresELM,AlvaradoRC,MartinsRLG.Consequences of chronic nasal obstruction on the laryngeal mucosa and voicequalityof4-to12-year-old children.JVoice.2012;26: 488---92.
21.BagnallAD,Dorrian J,FletcherA. Somevocal consequences ofsleepdeprivationandthepossibilityof‘‘fatigueproofing’’ the voice with voicecraft voice training. J Voice. 2011;25: 447---61.
22.AngelilloN,DiCostanzoB,AngelilloM,CostaG,BarillariMR, BarillariU.Epidemiologicalstudyonvocaldisordersinpediatric age.JPrevMedHyg.2008;49:1---5.
23.ConnellyA,ClementeWA,KubbaH.Managementofdysphonia inchildren.JLaryngolOtol.2009;123:642---7.
24.MartinsRHG,RibeiroH,MelloFMZ,BrancoA,TavaresELM. Dys-phoniainchildren.JVoice.2012;26:670---4.
25.MarkhamC,DeanT.Parents’andprofessionals’perceptionof qualityoflifeinchildrenwithspeechandlanguagedifficulty. IntJLangCommDis.2006;41:189---212.
26.Organizac¸ãoMundial daSaúdeClassificac¸ãointernacionaldas doenc¸as.10threv.PortoAlegre:ArtesMédicas;1992. 27.Andrade CRF, Béfi-Lopes DM, Fernandes FDM, Wertzner H.
ABFW: teste de linguagem infantil nas áreas de fonologia, vocabulário,fluênciaepragmática.Carapicuiba,SP:Pró-Fono; 2000.
28.Norbury C, Bishop D. Narrative skills of children with communication impairments.Int JLangComm Dis. 2003;38: 287---313.
29.SallesJF,ParenteMAMP.Relac¸ãoentreosprocessoscognitivos envolvidos na leitura de palavras e as habilidades de con-sciência fonológica em escolares.Pró-Fono RevAtual Cient. 2002;14:175---86.
30.BehlauM,PontesP.Avaliac¸ãoetratamentodasdisfonias.São Paulo:Lovise;1995.
31.FexS.Perceptualevaluation.JVoice.1992;6:155---8.
32.KaufmanJ,BirmaherB,BrentD,RaoU,FlynnC,MoreciP,etal. Scheduleforaffectivedisordersandschizophreniafor school-agechildren---presentandlifetimeversion(k-sads-pl):initial reliabilityandvaliditydata.JAmAcadChildAdolescPsychiatry. 1997;36:980---8.
33.ShafferD,Gould MS,BrasicJ,AmbrosiniP,Fisher P,Bird H, etal.Achildren’sGlobalAssessmentScale(CGAS).ArchGen Psychiatry.1983;40:1228---31.
34.AgrestiA. Categoricaldataanalysis.2nded.NewYork:John Wiley&Sons;2002.
35.ConoverWJ. Practicalnonparametric statistics.3rded.New York:JohnWiley&Sons;1999.
36.SPSSInc.SPSSforWindows.Version14.0.Chicago,IL:SPSSInc.; 2005.
37.HersanRCGP.Avaliac¸ãodevozemcrianc¸as.Pró-FonoRevAtual Cient.1991;3:3---9.
38.FieldT,DiegoM,Hernandez-ReifM.Depressedmothers’infants are less responsive to faces and voices. Infant Behav Dev. 2009;32:239---44.
39.ScarpariGK, Pontes F, OliveiraPA, Stivanin L, OliveiraCCC. Funcionamentoglobal,desempenhoneuropsicológicoe proces-samento auditivo em crianc¸as e adolescentes submetidas a maustratos.In:8◦ CongressoBrasileirodeCérebro,
Compor-tamentoeEmoc¸ões.2012.
40.Roy N, Holt KI, Redmond S, Muntz H. Behavioral character-istics of childrenwith vocalfold nodules. JVoice. 2007;21: 157---68.
41.Takeshita TK, Ricz LA, Isaac ML, Ricz H, Lima WA. Com-portamento vocal de crianc¸as em idadepré-escolar. Arq Int Otorrinolaringol.2009;13:252---8.
42.Scivoletto S, Stivanin L, Ribeiro ST, Oliveira CCC. Avaliac¸ão diagnósticadecrianc¸aseadolescentesemsituac¸ãode vulner-abilidadeeriscosocial:transtornodeconduta,transtornosde comunicac¸ãooutranstornosdoambiente?RevPsiquiatrClín. 2009;36:206---7.
43.Martins RHG, Trindade SHK. A crianc¸a disfônica: diagnós-tico,tratamentoeevoluc¸ãoclínica.RevBrasOtorrinolaringol. 2003;69:801---6.
44.KiliMA,OkurE,YildirimI,GuzelsoyS.Theprevalenceofvocal foldnodulesinschoolagechildren.IntJPediatr Otorhinolaryn-gol.2004;68:409---12.
45.CarlinoFC, Del PretteA, Abramides DVM.Avaliac¸ãodo grau deinteligibilidadedefaladecrianc¸ascomdesviofonológico: implicac¸ões nas habilidades sociais. Rev CEFAC. 2011: 1---7.
46.DelPretteZAP,RochaMM,SilvaresEFM,DelPretteA.Socialskills and psychologicaldisorders: convergingand criterion-related validityforYSRandIHSA-Del-Pretteinadolescentsatrisk.Univ Psychol.2012;11:941---55.
48.Connor NP, Cohen SB, Theis SM, Thibeault SL, Heatley DG, Bless DM. Attitudes of children with dysphonia. J Voice. 2008;22:197---209.
49.Simões-Zenari M,NemrK, Behlau M.Voicedisordersin chil-dren and its relationship with auditory, acoustic and vocal
behaviorparameter. IntJPediatr Otorhinolaryngol.2012;76: 896---900.