w w w . r b o . o r g . b r
Case
report
Arthroscopic
treatment
of
synovial
osteochondromatosis
of
the
elbow.
Case
report
and
literature
review
夽
Bernardo
Barcellos
Terra
∗,
Eduardo
Wanzenboeck
Moraes,
Alceuleir
Cardoso
de
Souza,
José
Maria
Cavatte,
João
Carlos
de
Medeiros
Teixeira,
Anderson
De
Nadai
HospitalSantaCasadeMisericórdiadeVitória,Vitória,ES,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received14August2014 Accepted1September2014 Availableonline8September2015
Keywords:
Synovialchondromatosis Arthroscopy
Elbow Synovitis
a
b
s
t
r
a
c
t
Synovialosteochondromatosisisabenignproliferativedisorderwithmetaplasiaofthe syno-vialmembranethataffectsthefibroblastsofthesynovialjoints,tendonsandbursae.In literature,therearefewdescriptionsofsynovialosteochondromatosisoftheelbow.The objectiveofthisarticlewastoreportacaseofsynovialosteochondromatosisoftheelbow inapatientaged32,basketballathlete,inwhichsurgicaltreatmentwaschosenbecauseof thepainandfunctionallimitationandstageofdiseasewithmultipleloosebodies.Patient 32,male,presentedwithpainandlimitationofmotionoftheelbow.Therangeof pas-sivemotionwas100◦offlexionand30◦extension.Therangeofactivemotionwas40–90◦.
Magneticresonanceobservedmanyloosebodiesmainlyintheposteriorcompartmentin theolecranonfossaplussomechondrallesionsinthecapitellum.Thearthroscopic treat-mentwaschosenwithtwoanteriorsportals(medialandlateral)andtwoposteriorportals (standardposteriorandposterolateral)foreasingloosebodiesandosteoplastyofthe olecra-nonfossa.Thevisualanalogscalepainwas9–3anditsarcofactivemotionwas110◦to
−20◦ offlexionandextension.OnascaleofperformancefromMayoClinicpatientswas65points preoperativelyto90postoperativelywith9monthsfollow-upandthepatientwassatisfied withthetreatmentoutcome.Arthroscopictreatmentofsynovialosteochondromatosisof theelbowisaneffectiveandsafetherapeuticmanagementwithlowmorbidityandearly returntoactivities.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkperformedintheDepartmentofOrthopedicsandTraumatology,HospitalSantaCasadeMisericórdiadeVitória,Vitória,ES, Brazil.
∗ Correspondingauthor.
E-mail:[email protected](B.B.Terra). http://dx.doi.org/10.1016/j.rboe.2015.08.014
Tratamento
artroscópico
da
osteocondromatose
sinovial
do
cotovelo.
Relato
de
caso
e
revisão
da
literatura
Palavras-chave:
Osteocondromatosesinovial Artroscopia
Cotovelo Sinovite
r
e
s
u
m
o
Aosteocondromatosesinovialéumapatologiaproliferativacommetaplasiabenignada membranasinovialqueafetaosfibroblastosdasarticulac¸õessinoviais,dostendõesedas bursas.Naliteratura,existempoucasdescric¸õesdeosteocondromatosesinovialdocotovelo. Oobjetivodesteartigofoirelatarumcasodeosteocondromatosesinovialdecotoveloem umpacientede32anos,sexomasculino,atletadebasquete,noqualseoptoupelo trata-mentocirúrgicodevidoaoquadroclínicocomdorelimitac¸ãofuncionaleaoestágioda doenc¸acommúltiploscorposlivres.Pacienteapresentoudorelimitac¸ãodoarcode movi-mentodocotovelo.Oarcodemovimentopassivoerade100◦deflexãoe−30◦deextensão.
Naressonânciamagnéticaobservaram-sediversoscorposlivres,principalmenteno com-partimentoposteriornafossadoolecrano,alémdealgumaslesõescondraisnocapítulo. Optou-sepelotratamentoartroscópicocomafeituradedoisportaisanteriores(mediale lateral)edoisposteriores(posteriorpadrãoeposterolateral)pararemoc¸ãodoscorposlivres eosteoplastiadafossaolecraniana.Aescalavisualanalógicadadorfoide9para3eseuarco demovimentoativofoipara110◦deflexãoe−20◦deextensão.Naescaladedesempenho
daClínicaMayoopacientefoide65pontosnopré-operatóriopara90nopós-operatório comnovemesesdeseguimentoesatisfeitocomoresultado.Otratamentoartroscópico daosteocondromatosesinovialdocotovelomostra-secomumaopc¸ãoterapêuticaeficaze seguranomanejoterapêuticodessapatologia,apresentabaixamorbidadeeretornoprecoce àsatividades.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Synovialosteochondromatosisisaproliferativepathological conditionwithbenignmetaplasiaofthesynovialmembrane thataffectsthefibroblastsofthesynovialjoints,tendonsand bursas.Thefirstdescriptionintheliteratureofthis patholog-icalconditionwasinrelationtothekneejoint,byAmbrose Páréin1958,apudHoandChoueka.1
Osteochondromatosiscan affect anyjoint,but the great majorityofthecasesinvolvethe knee.Inthe upperlimbs, thejointmostaffectedistheelbow,buttheshoulder,wrist, acromioclavicularandeventheinterphalangealjointsmaybe involved.2,3Thefirstcaseintheelbowwasreportedby
Hender-sonin1918,citedbyMusseyandHenderson.4Intheliterature,
therearefewdescriptionsofsynovialosteochondromatosisof theelbow,mainlyconcerningsurgicalresults.5
Synovial osteochondromatosis can be classified as pri-marywhenthecartilaginoustissueoriginatesdirectlyfrom the metaplasia of the synovial tissue or the bursa; or as secondary synovial osteochondromatosis when freebodies originatedirectlyfromthehyalinecartilageandaredeposited inthejointspaceorinthetendonsheath,duetodegenerative diseases,traumaorneuropathicarthropathy.6
Synovial osteochondromatosis can be subdivided into intra-articular synovial and tenosynovial (extra-articular) types.Intra-articularosteochondromatosisismorecommon and is usually monoarticular. Tenosynovial osteochondro-matosisisextra-articularand morecommonlyinvolvesthe flexortendonsofthefingers,wristsandfeet.Histologically, theyarethesameentities,butitisimportanttodifferentiate
them, since there is a greater chance that extra-articular tenosynovialosteochondromatosismightreoccur.7,8
Theobjectiveofthispaperwastoreportonacaseof syno-vialosteochondromatosisoftheelbowina32-year-oldpatient whowasabasketballplayer,forwhomsurgicaltreatmentwas chosen because ofhisclinical condition ofpain and func-tionallimitationandthestageofthedisease,withmanyfree bodies.
Case
report
Thepatientwasa32-year-oldmanwhocametothe outpa-tientclinic3monthsbeforethesurgery,presentingpainand limitationofelbowrangeofmotionthathadbegun8months earlier.Hesaidthathehadnotfallen;hehad nothad any systemicdiseasesorprevioussurgery;andhedidnotprovide anyotherinformationofrelevancetothecase.Oninspection, itwasnotedthatoneelbowpresentedslightedema,but with-out phlogisticsigns.Hecomplainedofpainonpalpationin thefossaoftheolecranonandintheregionoftheinsertion oftheextensorsandsupinatorsoftheforearm.Thepassive rangeofmotionwasfrom40◦ to100◦ offlexion.Theactive rangeofmotionwasfrom50◦ to90◦,pronationwas90◦ and supinationwas85◦.Neurologicalandvascularexaminations showednormalfindings.
RL 90 left RL 93 left R 2 cm
P
2 cm P
F Sc 9 F F
TSE/M SI 12
Sc 9 TSE/M SI 11
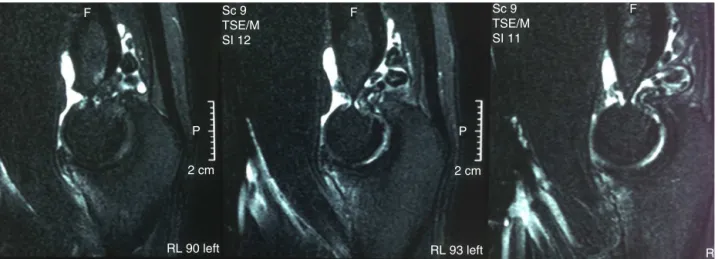
Fig.1– T2-weightedsagittalmagneticresonanceimagingshowingmanyfreebodiesinthefossaoftheolecranon.
capitellum(Figs.1–3),andtheradiologist’sdiagnostic hypoth-esiswasthatthiswasintra-articularsynovial osteochondro-matosis.Theresultsfromtheserumtestswerenegativefor rheumatologicaldiseasesorinfectiousprocesses.
Because of the severity of the case, it was decided to usearthroscopictreatment.Twoanteriorportals(medialand lateral)wereopened(for partialsynovectomy,anterior cap-sulotomy to gain extension and microperforations in the capitellum because of the osteochondral lesions) and two posterior portals (standard posterior and posterolateral) in ordertoremovethefreebodiesandperformosteoplastyon thefossaoftheolecranon becauseofthelocalosteophytes (Figs.4–7).Atthetimeofthesurgery,materialfor histopatho-logical examinationwascollected (free bodyand fragment fromthesynovialmembrane),whichsubsequentlyconfirmed thediagnosis.
Thepatient was immobilized bymeans ofcompressive bandaging.Passivemovementwasallowedduringthe imme-diate postoperativeperiod and activemovement according tothetoleranceofpain.Physiotherapeuticrehabilitationwas startedonthetenthpostoperativeday.
Inthesecondweekaftertheoperation,thepatientreturned to the outpatient clinic practically without pain and pre-sentedanactiverangeofmovementof20–100◦(Figs.8and9).
Eighteenmonthsaftertheoperation,thescoreonthevisual analogscalehaddecreasedfrom9to1andthepatient’sactive rangeofmotionwasnow10–130◦.OntheMayoClinic perfor-mancescale,thepatientwentfrom65pointsto90afterthe operationandhewasextremelysatisfiedwiththeresultfrom thetreatment. TheMayoClinicfunctionalscale9takesinto
considerationfourcriteria(pain,rangeofmotion,stabilityand function)andrangesfrom10to100points.Resultantscores higherthan90areexcellent;75to89good;60to74fair;and lowerthan60poor.
Discussion
Synovialosteochondromatosisofthejointsisararecondition forwhichthedefinitionanddiagnostic criteriaareunclear. Thereisstilllittleknowledgeaboutthiscondition.10Clinically,
thesignsandsymptomsarenonspecificandmaysuggest sev-eral pathological conditions. Inmost cases, the symptoms comprisepainand/orlossofrangeofmotion.Incapacityto performcompleteextensionisoneofthefirstsymptoms, fol-lowedinsomecasesbylockingofthejoint.Stiffnessisnota markedcharacteristic.Inourcase,thepatienthadapainful
RL 90 left RL 93 left RL 96 left
2 cm P
2 cm P
2 cm P
F Sc 8 F F
TSE/M SI 12
Sc 8 TSE/M SI 11
AP 89 post
AP 85 post
AP 82 post
3 cm
R
3 cm
R
3 cm
R
F
F
F
Sc 6
TSE/M
SI 11
Sc 6
TSE/M
SI 10
Sc 6
TSE/M
SI 9
Fig.3–T2-weightedcoronalmagneticresonanceimagingshowingmanyfreebodiesinthefossaoftheolecranonandin thelateralcompartment,alongwithachondrallesioninthecapitellum.
rangeofmotion,withoutanysigns andsymptomsof com-pressionoftheulnarnerve.
MilgramandPease11described30casesofsynovial
osteo-chondromatosisandidentifiedthreedistinctstages:disease withintrasynovialactivity,butwithoutthepresenceoffree bodies;transitionallesionswithsynovialactivityandfree bod-ies;and multiplefreebodies, but without synovialactivity. Ourpatientwasinstage3,sincehepresentedmultiple intra-articular free bodies. From arthroscopy, we observed only slightfociofsynovitis.
Fig.4–Intraoperativearthroscopicimageshowingfree bodiesinthefossaoftheolecranon.
Bothconservativetreatmentandsurgerycanbeusedas therapyforosteochondromatosis.Painreliefcanbeachieved through nonsurgicaltreatment. Surgicaltreatmentis advo-catedinphasesIIandIIIbythegreatmajorityofauthors.It shouldbeperformedinassociationwithsynovectomy,since theremayberecurrenceofthelesionafterremovalofthefree bodyalone.However,somestudieshavequestionedtreatment involving synovectomy.12,13 In the casepresentedhere, we
chosetoperformsynovectomyoftheanteriorandposterior compartments.
Fig.6–Freebodiesremoved.
In the literature, recurrence of this disease has been reported in up to 22% of the cases.14 The cause is
gener-ally attributed to incomplete removal of free bodies or to the synovial disease.Itis believed that recurrence implies thatthereisa greater chanceofmalignant transformation tochondrosarcoma,althoughthistransformationofsynovial osteochondromatosis is rare.15,16 The possibility of
malig-nanttransformationneedstobeconsideredwhenperiosteal reactionandcorticalerosionareobserved.Onanalyzing his-tologicalslides,thedifferentialdiagnosestobeconsideredare periosteal chondroma, giant-cell tumor, calcifying aponeu-roticfibroma,tumoralcalcinosis,hydroxyapatitedeposition, free bodies and inflammatory arthritis. The results from histopathologicalanalysisonthefreebodyandonafragment fromthecapsuleshowedalterationscompatiblewithsynovial osteochondromatosiswithmoderatediseaseactivity.
Intheupperlimbs,thelocationmostaffectedbysynovial osteochondromatosisistheelbow,followedinsecondplace bytheshoulder.Paimetal.16reportedtheresultfrom
arthro-scopictreatmentofacaseofsynovialosteochondromatosis oftheshoulder,inwhich44freebodieswereremoved.Over a1-yearfollow-up,almostcompleterecoveryoftherangeof motion,withoutpain,wasshown.Lasmaretal.17reporteda
caseofsynovialosteochondromatosisinaknee,inwhichover an8-monthfollow-up,excellentrecoverywasobtained.These authorsdrewattentiontothedifferentialdiagnosiswith pig-mented villonodular synovitis and noted that in standard radiographicexaminations,thediagnosismightgounnoticed,
Fig.7–Arthroscopicportalsconstructed(proximal anteromedial,proximalanterolateral,standardposterior andposterolateral).
given that the freebodies mightnot becalcified. Polesello etal.18reportedtheresultfromarthroscopictreatmentofsix
casesofhiposteochondromatosis,fromwhichgoodresults wereshown,withimprovementontheHarrisscaleas modi-fiedbyByrd,from54pointsbeforetheoperationto90points aftertheoperation.
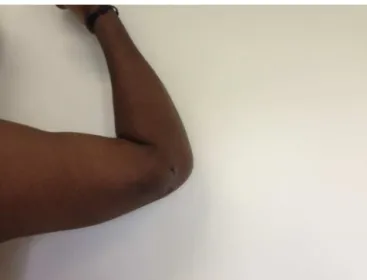
Fig.8–Twoweeksaftertheoperation,with−20◦ofactive
Fig.9–Twoweeksaftertheoperation,with100◦ofactive flexion.
Thecasereportedinthepresentstudyhasbeenfollowed upfor16monthsandsofarthepatientremainsfreefrompain andwithoutanysignsofrecurrence.
Conclusion
Arthroscopictreatment ofsynovialosteochondromatosis of theshoulderwasshowntobeaneffectiveandsafemeansof therapeuticmanagementforthispathologicalcondition,with lowmorbidityandanearlyreturntoactivities.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. HoYY,ChouekaJ.Synovialchondromatosisoftheupper extremity.JHandSurg.2013;38(4):804–10.
2. Bui-MansfieldLT,RohiniD,BaggM.Tenosynovial chondromatosisoftheringfinger.AJRAmJRoentgenol. 2005;184(4):1223–4.
3.GalliaGL,WeissN,CampbellJN,McCarthyEF,TufaroAP, GokaslanZL.Vertebralsynovialchondromatosis.Reportof twocasesandreviewoftheliterature.JNeurosurgSpine. 2004;1(2):211–8.
4.MusseyRDJr,HendersonMS.Osteochondromatosis.JBone JointSurgAm.1949;31(3):619–27.
5.MatsumotoK,HukudaS,FujitaM,KakimotoA,TachibanaS. Cubitalbursitiscausedbylocalizedsynovialchondromatosis oftheelbow.Acasereport.JBoneJointSurgAm.
1996;78(2):275–7.
6.OzcelikIB,KuvatSV,MersaB,PilanciO.Synovial
chondromatosisofthemetacarpophalangealjointofthering finger.ActaOrthopTraumatolTurc.2010;44(4):337–9. 7.MilgramJW,AddisonRG.Synovialosteochondromatosisof
theknee.Chondromatousrecurrencewithpossible chondrosarcomatousdegeneration.JBoneJointSurgAm. 1976;58(2):264–6.
8.MilgramJW.Synovialosteochondromatosis:a
histopathologicalstudyofthirtycases.JBoneJointSurgAm. 1977;59(6):792–801.
9.MorreyBF,AnKN,ChaoEY.Functionalevaluationofthe elbow.In:MorreyBF,editor.Theelbowanditsdisorders.2nd ed.Philadelphia:WBSaunders;1993.p.95.
10.KamineniS,O’DriscollSW,MorreyBF.Synovial osteochondromatosisoftheelbow.JBoneJointSurgBr. 2002;84(7):961–6.
11.MilgramJW,PeaseCN.Synovialosteochondromatosisina youngchild.Acasereport.JBoneJointSurgAm.
1980;62(6):1021–3.
12.ShpitzerT,GanelA,EngelbergS.Surgeryforsynovial chondromatosis.26casesfollowedupfor6years.Acta OrthopScand.1990;61(6):567–9.
13.RanallettaM,BongiovanniS,CalvoJM,GallucciG,MaignonG. Arthroscopictreatmentofsynovialchondromatosisofthe shoulder:reportofthreepatients.JShoulderElbowSurg. 2009;18(3):e4–8.
14.MauriceH,CroneM,WattI.Synovialchondromatosis.JBone JointSurgBr.1988;70(5):807–11.
15.DavisRI,HamiltonA,BiggartJD.Primarysynovial
chondromatosis:aclinicopathologicreviewandassessment ofmalignantpotential.HumPathol.1998;29(7):683–8. 16.PaimAE,FerreiraDC,PaimA,AlmeidaRM.Tratamento
artroscópicodaosteocondromatosesinovialdoombro:relato decaso.RevBrasOrtop.2008;43(4):146–9.
17.LasmarNP,VieiraRB,RosaJO,LasmarRCP,ScarpaAC. Osteocondromatosesinovial.RevBrasOrtop.2010;45(5):490–2. 18.PoleselloGC,OnoNK,HondaEK,GuimarãesRP,RicioliJunior