ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Idiopathic
musculoskeletal
pain
in
Indian
children–Prevalence
and
impact
on
daily
routine
Ganesh
Kumar,
Amieleena
Chhabra,
Vivek
Dewan,
Tribhuvan
Pal
Yadav
∗Dr.RamManoharLohiaHospitalandPostGraduateInstituteofMedicalEducationandResearch,DepartamentofPediatrics,NewDelhi, India
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received1August2014 Accepted1March2015
Availableonline4September2015
Keywords:
Idiopathicmusculoskeletalpain Prevalence
Impact
a
b
s
t
r
a
c
t
Objectives:Tostudytheprevalenceofidiopathicmusculoskeletalpain(IMSP)inschoolgoing childrenanditsimpactondailylife.
Methods:Onethousandeighteenapparentlyhealthyschoolchildrenaged5–16yearswere assessedandanalysedforIMSPanditsassociatedproblems.Standardtestsforsignificance wereapplied.
Results:Onehundredandsixty-five(16.2%)childrenmostlymales(55.2%)reportedIMSP. Lowerlimbs(52.1%)werethemostcommonlocationofpain.Morethan1yearofpain his-torywaspresentin15%.Thirty-sevenpercentchildrencomplainedofdiscomfortduring walking,30.9%,hadpainduringphysicalexercise,29.2%haddifficultyattendinglessons and4.2%hadinterferenceinpursuinghobbies.Thechildrenwerealsofurthersubgrouped intopreadolescentsandadolescents.Therewassignificantdifferenceinpaindurationand durationofeachpainepisodeinthetwogroups(p=0.01).Asignificantnumberofchildren (21.2%)withIMSPreportedschoolabsenteeism(p<0.001).Asignificantnumberof adoles-centshadhistorypositiveforcontactsports(p=0.001).Sleepdisturbanceswerealsoreported tobehigherinchildrenwithIMSP(29%vs.5.7%,p=0.001).Otherassociatedproblemsin chil-drenwithIMSPfoundweredaytimetiredness(51.1%),headache(47.3%)andabdominalpain (24.8%).
Conclusions:PrevalenceofIMSPinschoolchildrenaged5–16yrswasfoundtobe16.2% andasignificantpercentageofthesechildrenexperienceinterferencewithdailyactivities includingschoolabsenteeism.
©2015ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](T.P.Yadav). http://dx.doi.org/10.1016/j.rbre.2015.07.015
Prevalência
e
impacto
nas
atividades
diárias
da
dor
musculoesquelética
idiopática
em
crianc¸as
da
Índia
Palavras-chave:
Dormusculoesquelética idiopática
Prevalência Impacto
r
e
s
u
m
o
Objetivos: Estudaraprevalênciadedormusculoesqueléticaidiopática(DMEI)emcrianc¸as emidadeescolareseuimpactonasatividadesdiárias.
Métodos: Foramavaliadas eanalisadas1.018crianc¸asemidadeescolar aparentemente saudáveisentrecincoe16anosquantoàpresenc¸adeDMEIeseusproblemasassociados. Foramaplicadosostestesdesignificânciapadrão.
Resultados: RelataramDMEI165(16,2%)crianc¸as,emsuamaiorpartedosexomasculino (55,2%).Osmembrosinferiores(52,1%)foramalocalizac¸ãomaiscomumdador.Ahistória dedor presentehaviamaisdeumanofoiencontradaem15%dascrianc¸as;37%delas queixaram-sededesconfortoduranteacaminhada,30,9%,tinhamdorduranteo exercí-ciofísico,29,2%tinhamdificuldadedefrequentarasaulase4,2%sofriaminterferênciana participac¸ãoempassatempos.Ascrianc¸asforamaindasubagrupadasempré-adolescentes e adolescentes. Houve diferenc¸aestatisticamentesignificativa nadurac¸ão da dor e na durac¸ãodecadaepisódiodedornosdoisgrupos(p=0,01).Umaquantidadesignificativa decrianc¸ascomDMEI(21,2%)relatouabsentismoescolar(p<0,001).Umaquantidade signi-ficativadeadolescentestinhahistóriapositivadepráticadeesportesdecontato(p=0,001). Osdistúrbiosdosonotambémforamrelatadoscomomaioresemcrianc¸ascomDMEI(29%
vs.5,7%,p=0,001).Outrosproblemasassociadosencontradosemcrianc¸ascomDMEIforam ocansac¸oduranteodia(51,1%),acefaleia(47,3%)eadorabdominal(24,8%).
Conclusões:AprevalênciadeDMEIencontradaemcrianc¸asentrecincoe16anosfoide16,2%. Umapercentagemsignificativadessascrianc¸asrelatainterferêncianasatividadesdiárias, incluindoabsentismoescolar.
©2015ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Amongstchildren presentingwithchronic musculoskeletal pain(MSP),painwithoutanyidentifiablecausein appendic-ular or axial locations of the body constitute a significant proportionofthesecases(5–15%)andiscalledasidiopathic musculoskeletalpain(IMSP).1 Avariableduration(<6weeks
to3months)andfrequency(once/weekto3times/week)have beentakentodefineIMSPbyvariousauthors.2,3
Thoughconsideredbenign,inliteraturemostlyfromwest, IMSP hasbeen reportedto have significant effect on daily activity;psychosocialfunctioningandhealthrelatedquality oflife.4–8
IMSPhasbeenaneglectedareaofresearchinIndiaand thereispaucityofdataonitsvariousaspectsincluding preva-lence.
Weconductedthisstudywith,aprimaryobjectiveof find-ingouttheprevalenceofidiopathicmusculoskeletalpainin schoolchildrenandasecondaryobjectivetofinditsimpact ondailylivesofthesechildren.
Materials
and
methods
Studydesign
CrosssectionalStudy.
Studyduration
FromMarch2010toDecember2011.
Samplesizecalculation
SamplesizewascalculatedtakingmeanprevalenceofIMSP as10%,withan˛errorof2%andconfidenceintervalof95,it
wasrequiredtoinclude864subjectsforthestudy.
Enrolmentanddatacollection
For the purposeofthisstudy,any appendicular/axial mus-culoskeletal pain of ≥6 weeks, and frequency of at least once/week,withoutanyidentifiablecauseondetailedhistory andexaminationwereconsideredasIMSP.
Table1–ProfileofchildrenwithandwithoutIMSP.
NoIMSP(n=853) IMSP(n=165) p-Value
Mean± SD Min–Max 95%CI Mean± SD Min–Max 95%CI
Age(yrs) 11.43± 3.177 5–16 11.21–11.64 11.04± 3.013 5–16 10.57–11.50 0.389
Height(cm) 140.95± 18.072 96–187 139.7–142.17 140.61± 16.068 112–173 138.1–143.0 0.805 Weight(kg) 39.83± 13.540 16–66 38.92–40.74 35.72± 12.477 17–68 33.80–37.63 <0.001 BMI(kg/sq.m) 19.37± 3.22 10.2–31.72 19.15–19.58 17.55± 3.37 9.36–31.22 17.03–18.07 <0.001
fallingasleep,wakingupduringnightduetopain)andschool absenteeism(definedasmorethan10percentabsenteeismof totalschooldays)wastaken.Theinformationobtainedwas verifiedfromtheparents.
Sleepdisturbanceswereassessedusingsleepdisturbance scaleforchildren.9,10Allchildrenwereinquiredabout
indul-gence in contact sports like football, wrestling, kabaddi, martial arts, etc. If yes, then the type and frequency of thegameplayedwasobtained.Otherinformationrecorded foreachcasewere;parentaleducation,parentaloccupation, socioeconomicstatus,11familyhistoryofMSP,age(years),sex,
height(cm),andweight(kg)andhypermobilityofjointsasper Beightonscriteria.12
Clinicalexaminationwasdonetofindoutspecificcauses like arthritis, myositis, growing pains, fibromyalgia, reflex muscular dystrophy, trauma, connective tissue disorders, osteochondritis.Childrensuspectedofsufferingfromanyof theseknowncauseswerereferredforfurtherevaluationand excludedfromanalysis.Childrenwithmusculoskeletalpain, whohadclinicalevidenceofchronicsystemicdiseaseslike tuberculosis, heart disease, kidney disease, malabsorption, etc., and those who had takenvitamin D,calcium supple-ments,steroidsoranticonvulsantsinlast6months,werealso excluded.
ThestudywasapprovedbytheInstitutionalEthics Com-mittee.
Statisticalanalysis
Continuousvariableswerepresentedasmean±SD,and cat-egoricalvariableswere presentedasabsolutenumbersand percentage. The comparison of normally distributed con-tinuousvariablesbetweenthegroupswasperformedusing Student’st-test.Nominalcategoricaldatabetweenthegroups werecomparedusingChi-squaredtestorFisher’sexacttest asappropriate.Forallstatisticaltests,p-value≤0.05was con-sideredtobestatisticallysignificant.Statisticalanalysiswas performedby theSPSS programfor Windows,version 17.0 (SPSS,Chicago,Illinois).
Results
Atotalof1026schoolgoingchildrenaged5–16 yearswere evaluatedforMSP.Oftheseeightwereexcluded(oneeachof arthritis,myositis,osteochondritisandfiveofMSPlessthan 6weeksduration).Rest1018schoolchildrenwereincluded forfinalanalysis.Ofthese165(16.2%)hadIMSP,withmean ageof11.04(±3.01)years.Ninety-one(55.2%)wereboysand
74 (44.8%)were girls.Meanage, weight, heightandBMIof childrenwithandwithoutIMSParedepictedinTable1.
Most(38.2%)caseswereaged13–16years,33.9%were9–12 yearsold,and27.9%werebetween5and8yearsofage.
LowerlimbswerethemostcommonsiteofIMSP(52.1%) followed by upper limb (31.5%), neck (29.1%), lower back (26.7%), chest(17.6%),and upperback (10.9%).Painat mul-tiple sites (54.5%) was more common than at single site (45.5%).
Historyofpainofmorethan1yearand6monthsto1year waspresentin15%ofchildreneach,28.5%forpast3–6months and41.2%for6weeksto3months.Thehistoryofdurationof painwassimilaringirlsandboys(p=0.436).
Forty percent (40%) caseshad pain episodes lastingfor >30minwhile60%hadpainlastingfor<30min.Therewasno significantdifferenceinthedurationofpainepisodesbetween boysandgirlsandalsobetweenpreadolescentsand adoles-cents(p=0.430and0.130).
Almost daily pain episodes, 2–4 episodes per week, 1–3 episodes per week and once a weekwere found in28.4%, 23.1%,25.4%and23.1%,respectively.Differencebetween fre-quency of pain among boys and girls was not significant (p=0.869).
WedividedthechildrenwithIMSPintotwogroupsfor fur-theranalysis-childrenlessthan10yearsage(preadolescent) andmorethan10yearsofage(adolescent).Adolescentshad a longer duration of pain history. Most ofthe adolescents had ahistory ofpainduration ofmorethan threemonths whereasmostpreadolescentshadpaindurationoflessthan3 months.Similarlythefrequencyofpainwashigherin adoles-centsthoughthedifferencewasnotstatisticallysignificant. Pain episodestendedtolast longerinadolescents as com-paredtopreadolescentsandsignificantlyhighernumberof adolescentscomplainedofseverepainascomparedto pread-olescents(13.7%vs.1.3%,p<0.01)(Table2).
Lowerlimbswerethemostcommonsiteofpainin adoles-cents(44.3%)ascomparedtopreadolescents(29.9%).
AgoodproportionofchildrenwithIMSPhadreported dif-ficulties indailyactivitieslike walking,exerciseand sitting duringlessonsduetopain.Howevertherewasnodifference whenthedifficultieswerecomparedbetweenpreadolescents andadolescents(Table3).
Table2–Descriptionofpaininchildren&adolescents.
Paindescription Total <10years
n=77
>10years n=88
p-Value
Painduration
>1year 25(15.1) 6(7.8) 19(21.6) 0.010
6monthsto1 year
25(15.1) 9(11.7) 16(18.1) 0.010
3–6months 44(26.6) 20(26) 24(27.3) 0.004
3months–6 weeks
71(43.2) 42(54.5) 29(33) 0.017
Painfrequency
Almostdaily 47(28.4) 22(28.6) 25(28.4) 0.303
Onceperweek 38(23.1) 15(19.5) 23(26.2) 0.300
1–2perweek 42(25.4) 24(31.2) 18(20.4) 0.308
2–4perweek 38(23.1) 16(20.7) 22(25) 0.101
Durationofpain
<30min 100(60) 45(58.4) 55(62.5) 0.011
>30min 65(40) 32(41.6) 33(37.5) 0.061
Descriptionofpain
Mild 90(54.6) 53(68.8) 37(42) 0.053
Moderate 62(37.6) 23(29.9) 39(44.3) 0.071
Severe 13(7.8) 1(1.3) 12(13.7) 0.001
Table3–ImpactofIMSPonroutineactivitybetweenadolescents(>10yrs)andpreadolescents(<10yrs).
Activity n(%)
ChildrenwithIMSP
<10yrs >10yrs p-Value
Difficultywhile sittingduring lessons 49(29.2)
22(28.6) 27(30.7) 0.767
Painduringwalking 66(37.5)
34(44.2) 32(36.4) 0.308
PainduringPhysical exercise
51(30.9)
20(29.9) 31(35.2) 0.464
Interferencewith hobbies 7(4.2)
2(2.6) 5(5.7) 0.451
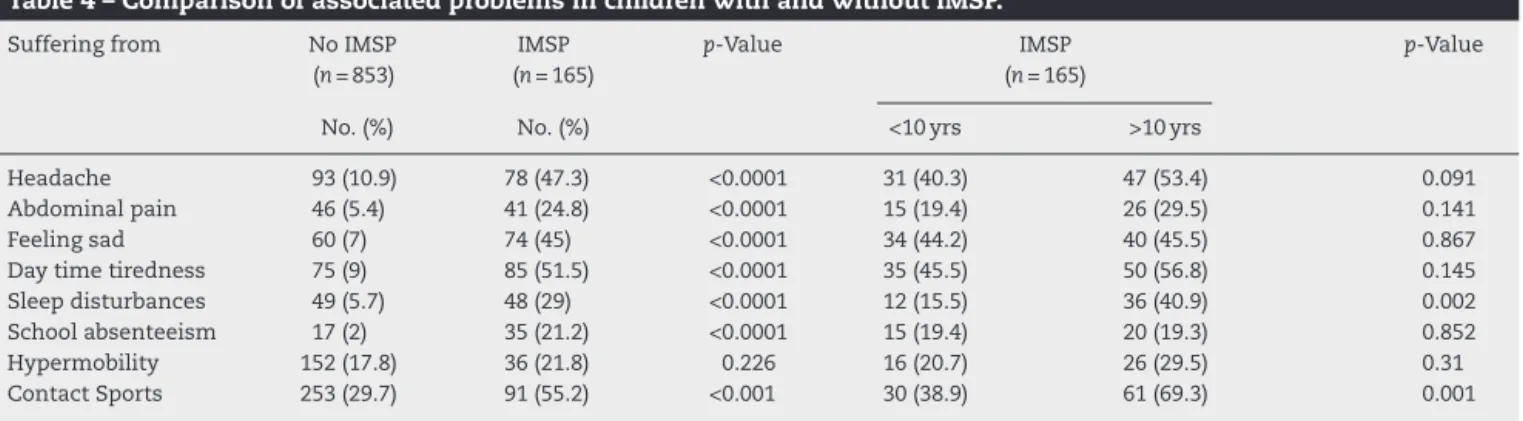
Table4–ComparisonofassociatedproblemsinchildrenwithandwithoutIMSP.
Sufferingfrom NoIMSP
(n=853)
IMSP (n=165)
p-Value IMSP
(n=165)
p-Value
No.(%) No.(%) <10yrs >10yrs
Headache 93(10.9) 78(47.3) <0.0001 31(40.3) 47(53.4) 0.091
Abdominalpain 46(5.4) 41(24.8) <0.0001 15(19.4) 26(29.5) 0.141
Feelingsad 60(7) 74(45) <0.0001 34(44.2) 40(45.5) 0.867
Daytimetiredness 75(9) 85(51.5) <0.0001 35(45.5) 50(56.8) 0.145
Sleepdisturbances 49(5.7) 48(29) <0.0001 12(15.5) 36(40.9) 0.002
Schoolabsenteeism 17(2) 35(21.2) <0.0001 15(19.4) 20(19.3) 0.852
Hypermobility 152(17.8) 36(21.8) 0.226 16(20.7) 26(29.5) 0.31
Twenty-onepercent(21.2%)childrenwithIMSPreported school absenteeism as compared to 2% without IMSP and the difference was significant (p≤0.0001). However, school absenteeismwasfoundtobesimilarinpreadolescentsand adolescents(p=0.852).
Historyofplayingcontactsportswaspresentinsignificant (p<0.001)numberofchildrenwithIMSP(55.2%)ascompared tochildren without (29.7%). Duration ofplay reportedwas 30minto1h.Thechildrenusedtoplaythesesportsfor1–5 daysinaweekwithanaverage of3daysper week.There wasalsosignificantlyhighernumberofadolescentwith his-tory of playing contact sports (69.3% vs. 38.9%, p=0.001). Thirty-threepercentofchildrenplayedfootball,20.9%played kabaddi and wrestling each, 14.3% were involved in box-ingwhile11%learnedmartialarts.Therewasnosignificant differenceinthedurationofgameplayedineachgroup (chil-drenwithIMSPandwithoutIMSP)(p=0.50).However,there wassignificant difference inthe numberofdays playedin aweekin thesetwo groups(p=0.007). Onfurther analysis ofhistory of contactsports in preadolescents and adoles-cents,nosignificant differencewasfoundbetweenthe two groupsindurationandfrequencyofsportsplayed(p=0.165 and0.162).
Sleepdisturbanceswereassessedusingsleepdisturbance scale for children. There was significant difference in the meanscoreinthechildrenwithandwithoutIMSP(mean±SD (range),38.29±9.61(7–56)vs.23.18±7.13(8–38),p<0.001).The mostcommondisturbancesnotedinchildrenwithIMSPwere disordersofinitiatingandmaintainingsleepandsleepwake transitiondisorders.
Hypermobilitywasfoundin21.8%ofIMSPcasesas com-paredto17.8%withoutbutthedifferencewasnotsignificant (p=0.226). Alsothe occurrenceofhypermobility in preado-lescentsand adolescents was notfoundtobe significantly different(p=0.31).
Almost half of (50.2%) children with IMSP belonged to lowersocioeconomicclass,31.5%belongedtomiddleclassand 16.7%toupperclass.IMSPsignificantlyoccurredmoreinlower socioeconomicclassincomparisontoupperandmiddleclass (p=0.032and0.004).
IMSP was significantly more prevalent in children with lowermaternaleducation(73.3%vs.26.7%,p<0.0001)while father’s education status showed no significant difference (53.3%vs.46.7%,p=0.226).
InchildrenwithIMSPpresenceofhistoryofbodyaches inbothparentswas significantlyhigherinparentsof chil-drenwith IMSPthan that ofchildrenwithout IMSP(father 3%vs.0.6%,p<0.0001,mother23.6%vs.3.8%,p<0.004).A sig-nificantnumberofparentsofadolescentsrevealedahistory ofbodyachesascomparedtopreadolescents(43.2%vs.13%,
p=0.001).
Discussion
MostchildrenwithIMSPwereintheagegroupof13–16years (38.2%)followedby9–12yearsand 5–8yearsagegroup.On sub grouping the children furtherinto preadolescents and adolescents,55.3% were adolescents Previousstudies have alsoshownthattheprevalenceincreasewithincreasingage
andwasmostcommonamongtheadolescentagegroup.4,5
The cause for higher prevalence in adolescents could be increaseinactivityandstressorswithincreasingage.Other factors playing a role could be organisationof health ser-vices,economy,culturaldifferencesorsomeotherunknown factors.13,14However,theexactreasonbehindsuchtrendisnot
known.
ChildrenwithIMSPhadalowerBMIinourstudywhichis contrarytothefindingsbyStovitzetal.15whofoundpainto
beassociatedmoreinobeseandoverweightchildren.However fewstudieshavefoundnosuchassociation.16Whychildren
with lowBMIhave increasedincidenceofpain syndromes mightbeasubjectrequiringexploration.
Aslightmale(55.2%)predominanceinourstudyissimilar toastudyonadolescentAmericanchildren17andcontraryto
others.Thisishypothesisedtobeduetogenetic,hormonal andenvironmentalfactors.7,18,19HoweverZapataetal.have
reportednosexpredilectionintheirstudyinadolescentswith musculoskeletalpain.20Theexactreasonofgenderdisparity
incaseswithIMSP,indifferent studieshasnotbeen eluci-dated.
MostcommonsiteofIMSPwaslowerlimbs(52.1%)followed byupperlimb(31.5%).Lowerlimbswerethemostcommon siteinadolescentsaswell(44.3%).Thisisinaccordancewith previous studies onidiopathic musculoskeletal pain byDe Inocencio4andPaladinoetal.18OnthecontraryZapataetal.
havereportedthemostcommonsitetobelowerbackintheir study onadolescents.20Thehigherincidenceoflowerlimb
paincouldbeduetoincreaseinphysicalactivitywith increas-ingage.
Inourstudy56.8%childrenhadpainpersistingformore than 3monthsand 43.2%hadpainhistory of6weeksto3 months. Onfurtheranalysisofpain inpreadolescents and adolescentsitwasseenthat21.6%adolescentscomplainedof ahistoryofmorethanyearwhilemostofthepreadolescents (54.5%)hadpainlastingforlessthan3months.Eighty-two per-centchildrenwithidiopathicmusculoskeletalpainhadmore thanoneepisodeofpainperweekandtheremaininghadat leastonepainepisodeperweek.Thisisinaccordancewith previousstudiesbyKonijnenbergetal.5andEl-Metwallyetal.7
Dailypainepisodeswereseenin28.4%ofchildren(both ado-lescentsandpreadolescents)inourstudyandthisishigher thanthosereportedinearlierstudies.18,19
Pain experienced during walking was the most preva-lentassociatedproblemspresentin44.2%ofpreadolescents and 36.4% adolescents. A little more than one third also reporteddifficultyinsittingduringlessonsandinterference with hobbies, which may affect the attention and con-centration span thereby leading to deterioration in school performance.
Wealsoanalysedthepainintensityusingvisualanalogue scaleforpain.Majorityofpreadolescentsreportedmildpain whilemoderatepainwasmorecommonintheadolescents withsignificantdifferencebetweenthetwoagegroups.We usedself-reportingtoolsfordescriptionofpainastheyare appropriateforchildrenabove4yearsandprovideareliable andvalidapproachofmeasuringpain.7
comparedbetweenpreadolescentsandadolescentsmoreof adolescents reported day time tiredness (56.8%) and sleep disturbances(40.9%).Thedifferencewasnotfoundtobe sta-tisticallysignificant.Suchassociationsmaynotonlydecrease theproductivityintheseyoungadultsbutmightevenaffect severalareasoflife.Earlierstudieshavealsoreported simi-larassociationswithpain.Converselymoodchangeandsleep disturbances may influence pain modulations resulting in aviscouscycleofchronicpain.3,13 Psychologicalstresscan
amplifyassociationbetweenpainandsleep.Theassociation withfeelingsad,stressandsleepdisturbancesislikelytobe strongerin adolescents who are stilldeveloping their abil-itytoregulateemotion,attentionandemotionalresponseto stress.21
Other pains like headache and abdominal pain were significantlyassociatedwithIMSP;however,therewasno sig-nificantdifferencebetweenpreadolescents andadolescents withIMSP. We did notanalyse these associated pain syn-dromes/stressorindetailinourchildren,howeveritisknown bypreviousstudies thatchildrenwithidiopathicpain syn-dromeshaveothersomaticpains.3,8
We found statistically significant higher school absen-teeisminallchildrenwithIMSP,whichisinaccordancewith previousstudies.2,22Thisprobablyisduetosleepdisturbances
anddifficultyinsittingthroughlesionsduetopainresultingin deteriorationinschoolperformanceandhigherratesofschool absenteeism.
Similartoprevious studies23,24 apositivehistoryof
con-tact sports was significantly higher in children with IMSP (p<0.001). Also significantly higher number of adolescents indulgedincontactsports (p<0.001).Indulgence incontact sportscouldincreasethechancesofsubtleinjuriesand per-hapschancesofMSP.
TherewasnosignificantassociationfoundbetweenIMSP andpositivehypermobilitytestinourstudywhichisin accor-dancewithpreviousstudies,7,25whereasafewstudieshave
shown a positive correlation19,26 This disparity in various
studieswarrantstheneedofmorelargerstudiestoestablish suchassociation.
IMSP in our study was found more prevalent in lower socioeconomicgroupwithlowermaternaleducationand pos-itive family history ofbody aches,which isin accordance withpreviousstudies.24,25Thetransmissionofpaininfamilies
couldoccurthroughbiologicaland/orpsychologicalfactors. Also some families may have a tendency to express feel-ingsthroughsomaticsymptoms;thusmusculoskeletalpain could be an expression of emotional stress in susceptible children.20,27
Inourstudy,sincethedatawascollectedbyrecall,acertain amountofrecallbiascannotberuledout,whichcouldbea limitation.
Toconclude,theoverallprevalenceofIMSPinschool chil-drenaged5–16yearswasfoundtobe16%andithadsignificant interferenceondailyactivitiesofthesechildren.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.MallesonPN,ConnellH,BennettSM,EcclestoneC.Chronic musculoskeletalpainandotheridiopathicpainsyndromes. ArchDisChild.2001;84:189–92.
2.MikkelssonM,SalminenJJ,KautiainenH.Non-specific musculoskeletalpaininpreadolescents.Prevalenceand 1-yearpersistence.Pain.1997;73:29–35.
3.O’SullivanP,BealesD,JensenL,MurrayK,MyersT.
Characteristicsofchronicnon-specificmusculoskeletalpain inchildrenandadolescentsattendingarheumatology outpatientsclinic:across-sectionalstudy.PediatrRheumatol. 2011;9:1–9.
4.DeInocencio.Epidemiologyofmusculoskeletalpainin primarycare.ArchDisChild.2004;89:431–4.
5.KonijnenbergAY,UiterwaalCSPM,KimpenJLL,vander HoevenJ,BuitelaarJK,deGraeff-MeederER.Childrenwith unexplainedchronicpain:substantialimpairmentin everydaylife.ArchDisChild.2005;90:680–6.
6.AaslandA,FlatoB,VandvikIH.Psychologicalfactorsin childrenwithidiopathicmusculoskeletalpain:aprospective longitudinalstudy.ActaPediatr.1997;86:740–6.
7.El-MetwallyA,SalminenJJ,AuvinenA,MacfarlaneG, MikkelssonM.Riskfactorsfordevelopmentofnon-specific musculoskeletalpaininpreteensandearlyadolescents:a prospective1-yearfollow-upstudy.BMCMusculoskelet Disord.2007;8:1–8.
8.KingS,ChambersCT,HuguotA,MacNevinRC,MacGrathPJ, ParkerL,etal.Theepidemiologyofchronicpaininchildhood andadolescentsrevisited:asystematicreview.Pain.
2011;152:2729–38.
9.BruniO,OttavianoS,GuidettiV,RomoliM,InnocenziM, CortesiF,etal.Thesleepdisturbancescaleforchildren. Constructionandvalidationofaninstrumenttoevaluate sleepdisturbanceinchildrenandadolescents.JSleepRes. 1996;5:251–61.
10.FerreiraVR,LucaineCarvalhoBC,RuotoloF,FaustodeMorias J,PradoLB,PradoGF.Sleepdisturbancescaleforchildren: translation,cultureadaptation,andvalidation.SleepMed. 2009;10:457–63.
11.KumarN,ShekharC,KumarP,KunduAS.Kuppuswamy’s socioeconomicstatusscale–updatingfor2007.IndianJ Pediatr.2007;74:1131–2.
12.BeightonP,SolomonL,SoskolneC.Articularmobilityinan Africanpopulation.AnnRheumDis.1973;32:413–8. 13.HoftunGB,RomundstadPR,ZwartJA,RyaggM.Chronic
idiopathicpaininadolescence-highprevalenceand disability:theyoungHuntstudy2008.Pain.2011;152: 2259–66.
14.SherryDD,MallesonPN.Idiopathicmusculoskeletalpainin childhood.RheumDisClinNorthAm.2002;28:669–85. 15.StovitzSD,PardeePE,VazquezG,DuvalS,SchwimmerJB.
Musculoskeletalpaininobesechildrenandadolescents.Acta Pediatr.2008;97:489–93.
16.FairbankJC,PynsentPB,VanPoortvlietJA,PhilipsH.Influence ofanthropometricfactorsandjointlaxityintheincidenceof adolescentbackpain.Spine.1984;9:461–4.
17.RheeH,MilesMS,HalpernCT,Holditch-DavisD.Prevalenceof recurrentphysicalsymptomsinUSadolescents.PediatrNurs. 2005;31:314–50.
18.PaladinoC,EymannA,LleraJ,DeCuntoCL.Estimated prevalenceofmusculoskeletalpaininchildrenwhoattenda communityhospital.ArchArgentPediatr.2009;107: 515–9.
20.ZapataAL,MoraesAP,LeoneC,FilhoUD,SilvaCA.Painand musculoskeletalpainsyndromesinadolescents.JAdolesc Health.2006;8:769–71.
21.MolinaJ,DosSantosFH,TeresaRA,TerrariM,FragaMM, GuerraSilvaS,etal.Sleep,stress,neurocognitiveprofile,and healthrelatedqualityoflifeinadolescentswithidiopathic musculoskeletalpain.Clinic(Paris).2012;67:1139–44. 22.Roth-IsigkeitA,ThyenU,StövenH,SchwarzenbergerJ,
SchmuckerP.Painamongchildrenandadolescents: restrictionsindailylivingandtriggeringfactors.Pediatrics. 2005;115:e152–62.
23.SubramanyamV,JanakiKV.Jointhypermobilityinsouth Indianchildren.IndianPediatr.1996;33:771–2.
24.MacfarlaneGJ,NorrieG,AthertonK,PowerC,JonesGT.The influenceofsocioeconomicstatusonthereportingof regionalandwidespreadmusculoskeletalpain:resultsfrom the1958BritishBirthCohortStudy.AnnRheumDis.2009;68: 1591–5.
25.MikkelssonM,SalminenJJ,KautiainenH.Jointhypermobility isnotacontributingfactortomusculoskeletalpainin pre-adolescents.JRheumatol.1996;23:1963–7. 26.GedaliaA,PressJ.Articularsymptomsinhypermobile
schoolchildren;aprospectivestudy.JPediatr.1991;119: 944–6.