www.revportpneumol.org
REVIEW
Prevention
of
ventilator-associated
pneumonia
J.
Oliveira
a,b,
C.
Zagalo
a,c,
P.
Cavaco-Silva
a,b,∗aCIIEM,InstitutoSuperiordeCiênciasdaSaúdeEgasMoniz,MontedeCaparica,Portugal bTechnoPhageS.A.,Lisbon,Portugal
cInstitutoPortuguêsdeOncologiadeLisboaFranciscoGentil,Lisbon,Portugal
Received9September2013;accepted8January2014
Availableonline24March2014
KEYWORDS Ventilator-associated pneumonia; Mechanical ventilation; Prevention
Abstract Invasivemechanicalventilation(IMV)representsariskfactorforthedevelopmentof
ventilator-associatedpneumonia(VAP),whichdevelopsatleast48hafteradmissioninpatients
ventilatedthroughtracheostomyorendotrachealintubation.VAPisthemostfrequent
intensive-care-unit(ICU)-acquiredinfectionamongpatientsreceivingIMV.Itcontributestoanincrease
inhospitalmortality,durationofMVandICUandlengthofhospitalstay.Therefore,it
wors-enstheconditionofthecriticalpatientandincreasesthetotalcostofhospitalization. The
introductionofpreventivemeasureshasbecomeimperative,toensurecontrolandtoreduce
theincidenceofVAP.Preventivemeasuresfocusonmodifiableriskfactors,mediatedby
non-pharmacologicalandpharmacologicalevidencebasedstrategiesrecommendedbyguidelines.
Thesemeasuresareintendedtoreducetheriskassociatedwithendotrachealintubationand
topreventmicroaspirationofpathogenstothelowerairways.
©2013Sociedade Portuguesade Pneumologia. PublishedbyElsevier España, S.L.All rights
reserved. PALAVRAS-CHAVE Pneumoniaassociada aoventilador; Ventilac¸ãomecânica; Prevenc¸ão
Prevenc¸ãodepneumoniaassociadaaousodoventilador
Resumo Aventilac¸ãomecânicainvasivarepresentaumfatorderiscoparaodesenvolvimento
dapneumoniaassociadaaoventilador(PAV),quesedesenvolve48horasoumaisapósa
admis-sãohospitalar,em doentesventiladosatravésdetraqueostomiaouintubac¸ãoendotraqueal.
A PAVé a infec¸ãoadquirida naunidade de cuidadosintensivos (UCI)mais frequente entre
osdoentessubmetidosaventilac¸ãomecânicainvasiva.Contribuiparaoaumentoda
mortal-idadehospitalar, dadurac¸ão daventilac¸ãomecânicaedotempo deinternamentonaUCI e
nohospital.Porconseguinte,agravaoestadodesaúdedodoentecríticoeaumentaocusto
totaldahospitalizac¸ão.Aadoc¸ãodemedidaspreventivaséimprescindível,demodoa
garan-tirocontroloeadiminuic¸ãodaincidênciadaPAV.Asmedidaspreventivasincidemsobreos
fatoresderiscomodificáveis,sendoaplicadasestratégiasnãofarmacológicasefarmacológicas
baseadas na evidência e recomendadas por guidelines. As medidas preventivas têm como
∗Correspondingauthor.
E-mailaddresses:[email protected],[email protected](P.Cavaco-Silva).
0873-2159/$–seefrontmatter©2013SociedadePortuguesadePneumologia.PublishedbyElsevierEspaña,S.L.Allrightsreserved. http://dx.doi.org/10.1016/j.rppneu.2014.01.002
finalidadediminuiroriscoassociadoàintubac¸ãoendotraquealepreveniramicroaspirac¸ãode
microrganismospatogénicosparaasviasaéreasinferiores.
©2013SociedadePortuguesa dePneumologia.Publicado porElsevier España,S.L.Todosos
direitosreservados.
Introduction
Invasivemechanicalventilationisariskfactorforthe devel-opment of pneumonia,1,2 being the ventilator-associated pneumonia(VAP)apublichealthproblem.VAPisa hospital-acquired pneumonia which occurs in patients who were subjected to invasive mechanical ventilation, whether throughtracheostomyor endotrachealintubation,atleast 48hoursbeforetheonsetofinfectionandthatwere ven-tilatedattheonsetofthepneumonia.3Thisdiseaseisalso classifiedaccordingtothetimeelapsedfromthebeginning ofthemechanicalventilation(MV)totheonsetof pneumo-nia;itisconsideredasearly-onsetifitoccurswithin4days ofthestartofMV,andlate-onsetifitoccursafter5ormore daysofMV onset.4,5However,not allthestudies consider early-andlate-onsetVAPwithinthesametimerangeframe (Table1).
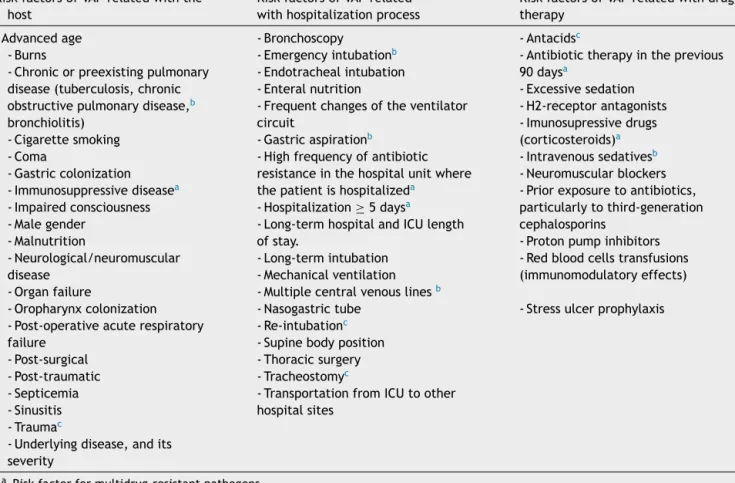
VAPoccursprimarilyinintensivecareunits(ICU),6where themostdebilitatedpatientsarehospitalized,often requir-ingventilatorysupport.Itisestimated thatfrom8to28% ofthepatientsreceivingMVdeveloppneumonia,theriskis between3and10 timeshighercomparedtopatients who donotreceiveMV.7Furthermore,almost90%ofepisodesof nosocomialpneumoniaregisteredin ICUoccurduring MV.5 Thepredisposingriskfactorsforthedevelopmentofthe dis-easeareinnumerableandaredividedintothreegroupsas schematizedinTable2:relatedwiththehost,the hospital-izationprocessandwithdrugtherapy.
AnepisodeofVAPmaybeduetoasinglepathogenorcan havepolymicrobialorigin.5,8,9The etiology ofVAPis quite diverse:bacterial,fungalandviral;fungiandviruses repre-sentagreaterrolewhentheimmunesystemofthepatients is weakened.8,10 The most common bacteria are listed in Table3.
VAPisoneofthemajorfactorscontributingto morbid-ityandmortalityin theICU.11 A meta-analysisfoundthat the average attributable mortalityto VAP is 32.5% in the ICU,12 supported by another study13 that found 33%. VAP increases the ICU and hospital length of stay, as well as thetimethepatientrequiresventilatorysupport.13,14 This pathologyisalsoresponsibleformorethanhalfofthe pre-scribed antibiotics in the ICU5 and for the increased cost ofhospitalinternment,registering awiderangeof values forthe average costattributabletothedisease(between
Table1 Differentdefinitionsofearlyandlate-onsetVAP.
Citation Early-onsetVAP Late-onsetVAP
Park,200510 ≤4---7days >7days
Olaecheaetal.,201085 ≤7days >7days
Erbayetal.,200416 ≤3---5days >3---5days
2089.13D and>29431.70D).14---18Duetoallthis,thesearch for preventive measures in order toreduce these param-eters,aswell astopreventthe onsetofthe disease,has becomeimperative.19,20
Pathogenesis
There are several sources of VAP pathogens that can be classified asexogenousand endogenousin relation tothe patient (Fig. 1). The exogenous sources are mostly from aerosolsofthecontaminatedair,medicaldevices (humidi-fier,ventilatorycircuit,catheterandbronchoscope),health professionals and other patients. The endogenoussources arerepresentedbytheoral,pharyngealandgastricfloraof thepatient.21,22
Microorganismsreachthelowerrespiratorytractmainly by microaspiration of oropharyngeal secretions or secret-ions that areaspirated tothe oropharynxthrough gastric reflux; and secondarily by direct extension of a contigu-ous infection, inhalation of contaminated aerosols or by hematogenousspreadofmicroorganismsfromothersitesof infection.21,23
The defense mechanisms against lung infection in a healthynonsmokerinclude:theanatomyofairways,cough reflex, mucus production, mucociliary clearance, lacto-ferrin, basement membrane and the immune system.21,24 Not all defense mechanisms are operational in critically ill patients due to underlying diseases, sedative medica-tion, poor nutrition and medical devices,22 such as the endotrachealtube(ETT)whichisusedintheMVand com-promises the cough reflex and the mucociliary clearance (ETTincreasesmucoussecretionandstagnationof secret-ions) and causes lesions on the surface of the tracheal epithelium.21,25TheETTcuffpreventstheaspirationoflarge volume secretions;however, it is not completelyairtight, sincethereisthepossibilityofestablishingmicrochannels between thetrachealmucous andthecuff whenit is dis-tended,whichincreasestheprobabilityofmicroaspiration of the accumulated secretions above the cuff (subglottic secretions) tothe lowerairways.25 Inaddition, pathogens that reach the ETT cuff areable to colonize the interior ofthetube,ensuringaccesstothedistalairwayswiththe aidoftheinspiratoryflowfromtheMV,establishing posteri-orlythelunginfection.24Previoussurgeriesandmedication, particularlyantibiotherapy,mayalsopredisposethepatient tothedisease.5
Preventionofventilator-associatedpneumonia
VAP prevention is performed through pharmacological and non-pharmacological measures that mainly focus on modifiable riskfactors.Withthisreview ourintentionwas to approach the most consensual preventive measures
Table2 RiskfactorsofVAP5,65,86---89
RiskfactorsofVAPrelatedwiththe
host
RiskfactorsofVAPrelated
withhospitalizationprocess
RiskfactorsofVAPrelatedwithdrug
therapy
-Advancedage
-Burns
-Chronicorpreexistingpulmonary
disease(tuberculosis,chronic
obstructivepulmonarydisease,b
bronchiolitis) -Cigarettesmoking -Coma -Gastriccolonization -Immunosuppressivediseasea -Impairedconsciousness -Malegender -Malnutrition -Neurological/neuromuscular disease -Organfailure -Oropharynxcolonization
-Post-operativeacuterespiratory
failure -Post-surgical -Post-traumatic -Septicemia -Sinusitis -Traumac
-Underlyingdisease,andits
severity
-Bronchoscopy
-Emergencyintubationb
-Endotrachealintubation
-Enteralnutrition
-Frequentchangesoftheventilator
circuit
-Gastricaspirationb
-Highfrequencyofantibiotic
resistanceinthehospitalunitwhere
thepatientishospitalizeda
-Hospitalization≥5daysa
-Long-termhospitalandICUlength
ofstay.
-Long-termintubation
-Mechanicalventilation
-Multiplecentralvenouslinesb
-Nasogastrictube
-Re-intubationc
-Supinebodyposition
-Thoracicsurgery
-Tracheostomyc
-TransportationfromICUtoother
hospitalsites
-Antacidsc
-Antibiotictherapyintheprevious
90daysa -Excessivesedation -H2-receptorantagonists -Imunosupressivedrugs (corticosteroids)a -Intravenoussedativesb -Neuromuscularblockers
-Priorexposuretoantibiotics,
particularlytothird-generation
cephalosporins
-Protonpumpinhibitors
-Redbloodcellstransfusions
(immunomodulatoryeffects)
-Stressulcerprophylaxis
a Riskfactorformultidrug-resistantpathogens. b Specificriskfactorsofearly-onsetVAP. c Specificriskfactorsoflate-onsetVAP.
A B C D E F
Figure1 Routesofcolonization/infectioninmechanicallyventilatedpatients21A---oralandpharyngealcolonization;B---gastric
colonization;C---infectedpatients;D---handlingofrespiratoryequipment;E---useofrespiratorydevices;andF---aerosolsfrom
Table 3 Predominant bacteria in ventilator-associated
pneumonia.10,85,90
Gram-positivecocci
Methicillin-sensitiveStaphylococcusaureus(MSSA)
Methicillin-resistantStaphylococcusaureus(MRSA)
Streptococcuspneumoniae
AerobicGram-negativebacilli
Haemophilusinfluenzae
LactosefermentingGram-negativebacilli Enterobacteriaceae Enterobacterspp. Escherichiacoli Klebsiellapneumonia Proteusspp. Serratiaspp.
Non-lactosefermentingGram-negativebacilli Pseudomonasaeruginosa
Acinetobacterbaumannii
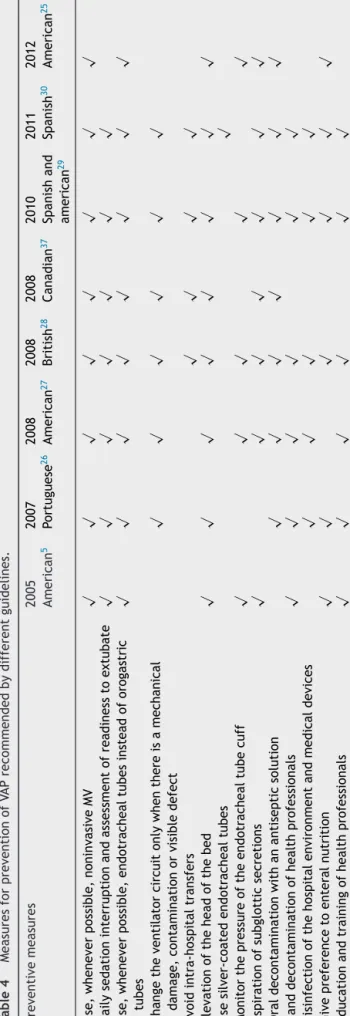
thataredescribedin guidelinesdrawn upbynationaland internationalscientificmedicalsocieties(Table4indicates thepreventivemeasuresthateachguidelinerecommends).
Noninvasivemechanicalventilation
The first step in the prevention of VAP is the patient evaluation in order to determine the need for invasive mechanical ventilation. MV should be avoided whenever possible,5,21,25---30since,byusingintubation,theriskof noso-comialpneumoniaisincreased6---21times.5
AlthoughnoninvasiveMVisconsideredafeasible alterna-tivetoinvasiveMVinsomeclinicalsituations,itisimportant to perceive that it is not applicable in all patients, and therefore it cannot replace MV and endotracheal intuba-tion in all situations. Noninvasive MV has been employed withfavorableclinical resultsincasesof:exacerbationof chronicobstructivepulmonarydisease(COPD),cardiogenic pulmonaryedema,acutehypoxemicrespiratoryfailureand in some immunosuppressed patients withpulmonary infil-trates and respiratory failure.5,31 A meta-analysis of 12 studies,inwhichthetargetpopulationhadCOPDasthe pre-vailingdisease,concludedthatnoninvasivepositivepressure MV, compared with invasive positive pressure MV, signifi-cantlydecreased mortalityand incidence of VAP, andthe ICUandhospitallengthofstay.32
The useof noninvasiveMVafterextubation inorderto preventre-intubationandtoreducethetimeofMV(invasive andnoninvasive)hasbeeninvestigatedandtheresultsare nowpromising.33However,morestudiesareneededinorder togetabetterunderstandingofitsroleinVAPprevention. Untilnow,theefficacyofthismeasurehasonlybeenproven inpatientswithCOPD.31
Weaningfrominvasivemechanicalventilation
TheweaningfrominvasiveMV involvesaclosemonitoring of the patient, not only because it usually occurs in an intensivecareenvironment,butalsobecausethe monitor-ingofsignsandsymptomsisessentialinidentificationofa Table
4 Measures for prevention of VAP recommended by different guidelines. Preventive measures 2005 American 5 2007 Portuguese 26 2008 American 27 2008 British 28 2008 Canadian 37 2010 Spanish and american 29 2011 Spanish 30 2012 American 25 Use, whenever possible, noninvasive MV √ √ √ √ √ √ √ √ Daily sedation interruption and assessment of readiness to extubate √ √ √ √ √ √ √ Use, whenever possible, endotracheal tubes instead of orogastric tubes √ √ √ √ √ √ √ √ Change the ventilator circuit only when there is a mechanical damage, contamination or visible defect √√ √ √ √√ Avoid intra-hospital transfers √√ √ √ Elevation of the head of the bed √√ √√ √√ √ √ Use silver-coated endotracheal tubes √ Monitor the pressure of the endotracheal tube cuff √ √√ √ √ Aspiration of subglottic secretions √√ √ √ √ √ √ Oral decontamination with an antiseptic solution √ √√ √√ √ √ Hand decontamination of health professionals √ √ √√ √ √ Disinfection of the hospital environment and medical devices √ √√ √ √ Give preference to enteral nutrition √√ √ √ √ √ Education and training of health professionals √√ √√ √ √
possiblefailureoftheweaningprocess:increasedshortness of breath, tachycardia, diaphoresis, oxygen desaturation, hypertensionandincreasedanxiety.34
Currently,themost widelyusedweaningmethodisthe spontaneousbreathingtrial (SBT),whichallowsthe obser-vationforsignsofrespiratoryfailure.DuringSBTthepatient breathesspontaneouslythroughtheETT,whichisconnected toaT-piece.TheT-piececanprovideasourceofhumidified oxygen (withoutmechanical ventilator), reducedlevelsof continuouspositiveairwaypressureand/orpressuresupport ventilationforshortperiodsoftime(30min---2h).34,35
Since it is difficult topredict the duration of MV, the current guidelines recommend the use of protocols for implementing theweaningprocess withdailyassessments of the patient, in order toassess whether there are the necessaryconditionstobegintheweaningprocess.5,26---30
Ideally,protocolsofinvasiveMVweaninginclude wean-ingfromsedatives,sinceitwasfoundthat thisprocedure contributes to the reduction of the duration of MV and the ICU length of stay and, consequently, to reduce the risk ofVAP.5,26---30,36 Indeed,theoveruseof sedativesisnot beneficial to the weaning process, as it can inhibit the patient’s breathingcapacity,which isindispensabletothe discontinuationofMV.
Endotrachealintubation
Guidelinesrecommendthatintubationshouldpreferablybe applied with orotrachealand orogastric tubes, instead of usingnasotrachealor nasogastrictubes,sinceoral intuba-tionisassociatedwithalowerincidenceofVAP.5,25---29,37
Frequencyofchangesoftheventilatorcircuit
One of the risk factors related with increased hospital-ization is the frequent change of the ventilator circuit. Currently it is consensual that one circuit only should be used in each patient,and that it shouldonly be changed when there is a mechanical damage or contamination (blood, vomit, or purulent secretions).26,27,29,30,37,38 This recommendation is based on the evidence that frequent changes in the ventilator circuit do not contribute to a decreasedincidenceofVAP.39
Avoidunnecessaryintra-hospitaltransfers
Bercault et al. found that an episode of transport from theICU toanotherplaceinthehospitalincreasestherisk of development of VAP.40 It is thought that the patient’s positioning in supine position, and the frequent handling of the ventilator tubing during the transfers, may facili-tatetheaspirationofcontaminatedsecretions.29Nowadays, when an intra-hospital transfer is needed the patient should be in an inclined position and enteral nutrition (EN)shouldbesuspended4hbeforethetransfer.28---30
Specificpreventionofmicroaspiration
a) Elevationoftheheadofthebed
Elevationof the headof thebed hasthe purposeof avoiding positioningthe patient in supineposition --- a
position whose leaning is 0◦ and is a risk factor for
the development of VAP, in order to prevent gastroe-sophagealrefluxandsubsequentaspirationtothelower airways. In fact, elevation of the head of the bed is associatedwithareducedriskofaspiration.27,29A meta-analysis concluded that a head elevation of 15---30◦ is
not sufficient topreventthe developmentof VAP.41 At present, elevationoftheheadof thebedbetween30◦
and 45◦5,25---30 is recommended, but there are already some studies and guidelines that would only consider elevationoftheheadofthebedat45◦.37,41 Theuseof thehorizontal---lateralpositionwithanelevationof45◦
hasshownpromisingresults,becausecomparedwiththe semi-recumbentposition,ithashadalowerincidenceof VAP(4/10 versus1/10).42 However,thismeasureis not yetincludedinguidelinesastherearestillsomedoubts remaintobecleared.
b) Modificationsinendotrachealtubes
ModificationsinETTareintended toprevent mecha-nisms throughwhich endotrachealintubation increases theriskofVAP:1)aspirationofsecretionsintothelower airways, 2) mucosal injury and decreased mucociliary clearance of secretions, 3) microaspiration of secreti-onsaroundtheinflatedcuffand4)biofilmformationand bacterialcolonizationintheETTlumen.43
In order to replace the traditional ETT, which have polyvinylchloride in their constitution, antibacterial-coated ETT have been developed; the most studied compound issilver, which hasbactericidal activity and is able to prevent biofilm formation.44 A prospective study found that intubation with silver-coated ETT is safe, delays the ETT colonization, reduces the biofilm formation anddecreases themaximalbacterialburden intrachealsecretionsfor7days.45 Anotherprospective study concluded that patients intubated with silver-coated ETT showed lower incidence of VAP, delay in disease onset (with higher impact in the first 10 days ofintubation)46anddecreasedmortality.47Upuntilnow, nostudyhasreachedaconclusionabouttheinfluenceof thispreventivemeasureinthedurationofMV,andinICU and hospitallength of stay. Therefore,this preventive measureisstillnotconsensualamongthescientific com-munity; sofar only the Spanish guidelines recommend it.30However,itisworthnotingthatacost-effectiveness study of silver-coated ETT confirmed that, although silver-coated ETT are much more expensive (60.22D) thanconventionaltubes(1.47D),theyreducedthe hos-pitalcostsfrombetween7085.68D and12034.60D per preventedcaseofVAP.48
TheimprovementoftheETTcuffhasalsobeentried out, both in terms of shape as well as its inflation characteristics, in order toprevent microaspiration of subglottic secretions. The studies which analyzed ETT withpolyurethane cuffs have shown goodresults, sug-gestingthattheymaybeeffectiveinthepreventionof microaspirationof secretionstothe lowerairways.49---52 However, to date, none of the studies predicted the actionofthesetubesinthedurationofMVandICUand hospitallengthofstay.
Anotherrecommendationmadebysomeguidelinesis relatedtothecuffpressure.Itshouldbecheckeddaily,at regularintervals,andmaintainedbetween20and30cm
H2O:belowthisvalue theriskof pneumoniaincreases,
and above it tracheal mucosal injuries can occur.25,29 However,theBritishguidelinesrecommendsanarrower rangeofpressure(>25and<30cmH2O)28andthe
Amer-ican guidelines only recommend a minimum value of 20cmH2O.5,27
c) Aspirationofsubglotticsecretions
Currently,aspirationofsubglotticsecretionsis recom-mended by almost all guidelines,sincestudies show a reductionintheincidenceofVAPwhenthispreventive measureis used.5,25,27---30,37 The meta-analysisof Dezfu-lian ital. concluded that subglottic secretion drainage reducedtheincidenceofVAPbyalmostahalf,andthatin patientswithanestimatedMVtimeofmorethan72hthis measuredecreased,onaverage,thedurationofMVby2 days,theICUlengthofstayby3days,anddelayedthe onsetofpneumoniaby6.8days.53Therecommendations concerningtheuseofaspirationofsubglotticsecretions differ between guidelines.Canadian guidelines recom-menditinpatientswhoareexpectedtorequireMVfor morethan72h,37buttheSpanishhavereducedthetime to48h,30andtheBritishrecommendtheimplementation ofthismeasureregardlessoftheexpectedMVduration.28 Possiblythelatterapproachisthemostsensible,because itisverydifficulttopredictthedurationofMV.54
There is no doubt that the use of this technique, continuously or intermittently, is effective in the pre-vention of VAP,55---58 but to date none of the forms of aspirationhavebeenhighlightedasthebest.Currently, both are implementedin order topreventand reduce microaspirationand,forthispurpose,specificETThave beendeveloped.TheseETThaveasecondlumen (aspi-ration lumen), which has an evacuation orifice in the edgeofthecuffconnectedtoasuctionsystem,allowing continuous or intermittent aspiration of the subglottic secretions.25,30,59
Controlofthecolonizationoftheoropharynxand
thedigestivetract
A major aim of VAP prevention consists in reducing the colonization of the oropharynx and the digestive tract, sincetheyrepresentanincreasedriskofmicroaspirationof pathogenstothelowerairways.21
a) Oralantiseptics
PatientswhoareintubatedwithETTcannotperform theirdaily oral hygiene, whichcarriesa riskof biofilm colonizationbypathogenicmicroorganisms.60 Oral anti-septicshavebeen usedinordertoreduce andprevent oropharyngealcolonizationbybacterialpathogens,and hencethisisaviablealternativesinceitcanbe imple-mentedbyhealthcareproviders.
The use of oral antiseptics significantly reduces the incidence and the relativerisk (RR=0.56) of VAP, sug-gestingthatthismeasureisefficientinitsprevention.61 Duetoitsverybroadspectrumofaction, whichcovers microorganismssuchasPseudomonasaeruginosa, Acine-tobacter spp., andmethicillin-resistantStaphylococcus aureus,62 some of the most common pathogens impli-cated in VAP, chlorhexidine (CHX) is the most studied
antiseptic,anditsefficacyinthepreventionofVAPhas beenproven.63,64Infact,themostrecentguidelines rec-ommendoraldecontaminationwithCHXasapreventive measureofVAP.25---27,30,37However,noguidelines recom-mend a posology for this preventive measure. Studies usedconcentrationsof0.12%,0.2%and2%ofCHX admin-istered 2, 3 or 4 times daily.62 A more recent study suggeststheuseof15mlofanoralsolutionof0.12%of CHXtwiceadayuntil24hafterextubation.65
The Canadianguideline isthe onlyonethat, besides recommendingtheuseofCHXasanoralantiseptic,also recommendsthattheuseofiodopovidoneshouldbe con-sideredinpatientswithsevereheadinjury,basedona singlestudyperformedinthispatientpopulation.37 b) Antibiotic prophylaxis: Selective oropharyngeal
decon-tamination(SOD)andselective digestive decontamina-tion(SDD)
SODconsistsofenteraladministrationofantimicrobial agents,while inSDDthe parenteralroute isalsoused. Thesedecontaminations areselectivebecausethe aim istopreventtheoropharyngealandgastriccolonization by aerobic Gram-negative bacilli, S. aureus and fungi specieslikeCandida,without affectingthe commensal flora.65 Antimicrobialregimensstudieddonotvaryvery much.Theyconsistessentiallyintheadministrationfour timesadayofantibioticsthatactonlyinthe gastroin-testinaltract,i.e.whicharenotabsorbed(e.g.,colistin, polymyxin E, tobramycin and/or amphotericin B), and antibioticsadministeredintravenously(e.g.cefotaxime orciprofloxacin)inthecaseofSDD.54,62
de Smet et al. have conducted the largest study concerning SOD and SDD to date, they confirmed a 2.9% decrease in the mortality rate with SOD, and a 3.5% decrease withSDD. Bothdecontamination proce-dures reduced the duration of MV, ICU and hospital length of stay, daily doses of antimicrobials and the incidence of ICU-acquired bacteremia caused by S. aureus,P.aeruginosaandEnterobacteriaceae.Moreover, isolationofGram-negativebacteriadecreased consider-ably in patients who were treated withSOD and SDD. Authors defend the administration of DSO because it does notincludewidespreadsystemic prophylaxiswith cephalosporins,andsoavoidstheincreaseofantibiotic resistanceinICU.66However,thisstudyhasa characteris-ticthathaspreventedthegeneralizedrecommendation of SOD and SDD: antibiotic resistance recorded in the studiedICU(Holland)isconsideredlow(<5%)when com-pared to the rates of antibiotic resistance in other countries such as the USA.54,65 Studies in different locations,withdifferent rates ofantibiotic resistance, are needed in order to obtain a better and more widespreadperceptionofthelong-termeffectofthese measures.
Alaterstudy,carriedoutinthesameICU,evaluated theimpact of SODand SDD onantibiotic resistance in Gram-negative bacteria,concluding that although SOD and SDD reduced mortality, both measures were asso-ciatedwithagradualincrease in antibioticresistance, primarily to ceftazidime.67 Thus, American guidelines andother morerecentonesdonotrecommendroutine useofprophylacticantibioticsandSDD,duetoconcerns abouttherisingproblemofantibioticresistance.5,30,37
c) Probiotics
Probioticsareviablemicroorganismspresentin suffi-cientnumbersothattheycanhaveabeneficialeffecton thehealthofthehost,whichisachievedbycolonization andchangesofthemicroflorainacompartmentofthe host(e.g.oralcavity,gut),wheretheyremain temporar-ily,favoringthegrowthofbacterialspeciesbeneficialto theorganism,anddecreasingthepresenceofpotential pathogens.68,69
A meta-analysis includingfive studies that analyzed theeffectofprobioticsinventilatedpatients,concluded that itsimplementation reducedthe incidence of VAP, ICU length of stay and colonization of the respiratory tract by P. aeruginosa; however, no differences were observedinmortalityratesandMVduration.70Twoother studiesthatwerenotincludedinthementioned analy-sisalsoprovedtheefficacy(reductionofVAPincidence and antibiotics use) and safety of probiotics adminis-tration in the prevention of VAP.69,71 It is a fact that probioticsadministrationhasbeenshowntobepromising inpreventingVAP,possiblyrepresentinganalternativeto antibioticprophylaxis,duetotheincreasingproblemof resistance.However,todate,noguidelinesrecommend theiruse.Morestudiesareneeded,withmore represen-tative patientpopulations,in ordertoextrapolate the results.
Disinfectionandantisepsis
BesidesallspecificmeasurestopreventVAP,guidelinesalso recommendoneofthemostbasicandcommonpreventive measures of nosocomial infections: hygiene and disinfec-tionof thehospitalenvironment,healthcareprofessionals andmedicaldevices.5,26---30Regardingthelatter,disinfection of the respiratory equipment, removalof thecondensate withtheventilatorcircuitclosedduringtheprocedure,and use ofsterilewaterwhenrinsingthereusable devicesare recommended.
Adherencetohand hygieneprogramsis consideredone of themost importantpreventivemeasuresof healthcare-associatedinfections,72andalsohastheadvantageofbeing cheap. The CDC Guideline for Hand Hygiene in Health-Care Settings analyzed data from observational studies concludingthatthepercentageofhealthprofessionalswho implementtherecommendedproceduresforhandhygieneis highlyvariable,withanoverallaverageof40%.73Inorderto reducepooradherence,trainingofhealthprofessionalsand assessmentoftheirperformance,distributionofinformation leafletsandlecturesaresuggested.74
Enteral
nutrition
ENisconsideredariskfactorforthedevelopmentof pneu-monia, because it increases the risk of aspiration of the gastric contenttothe lowerairways.5,75 However,in ven-tilated patients who have a critical condition, its use is unavoidableandnecessary,becauseitavoidsthe develop-mentofacatabolicstate28 anddecreasestheincidenceof infectious complications and hospitalizationcosts.76 Addi-tionally,ventilation timeis greaterwhen patientsarefed by parenteral route.77 Alarge-scalestudy determinedthe impact ofearly (administered withinthe first48h of MV)
versuslateENonICUandhospitalmortalityofmechanically ventilatedpatients.Authorsconcludedthatearly adminis-tration of EN wasassociated withlower rates of ICU and hospitalmortality,especiallyinthosepatientswithaworse health condition; however it increased the risk of devel-opment of VAP. Since the increased risk of VAP was not associatedwithanincreasedmortality,authorsrecommend early administrationof EN,mainly in patients whoareat highriskofdeath.78
The UK guidelines recommend that the rate and vol-ume of ENshould be adjusted to avoid gastric distension in order to prevent aspiration of gastric content to the lowerairways.28 As the semi-recumbent position(30---45◦)
has been associated with the prevention of aspiration of gastric content, guidelinesconsider it essential when the patientisfedbyEN,whichshouldbeadministeredassoon aspossible.5,25,26,29,30
Educationandtrainingforhealthprofessionals
Some guidelinesemphasize theimportance ofVAP educa-tion and training programs for health professionals who are directly involved in providing health care topatients underMV,5,26---30 sinceit isassociated withprovenefficacy inreducingtheincidenceofVAPby50%.79 Aquestionnaire carried out with 1200 USA nurses revealed that only 82% adhere to hand-washing practices, 77% use gloves, 52% raisetheheadof thebedto30---45◦ duringtheentireday
and36%aspiratethesubgloticsecretions;italsorevealed that nurses who used a protocol of oral hygiene were associatedwitha greaterknowledge ofthe diseaseanda higher compliance with good service practices to reduce theriskofVAP.80Therearereasonsfornon-compliancewith guidelines by health professionals, such as disagreement withtheresultsofthestudies,patientdiscomfort,fearof adverseeffects,lackofresourcesandtheassociatedcosts withpreventivemeasures.29
Bundles
A bundle consists of a small set of preventive measures withprovenefficacy,whichensuresmoreefficient preven-tionofthedisease,comparedtothesumoftheirindividual implementation.25,54,81
Mostofthehospitalteamsthathaveevaluated preven-tivemeasuresforVAP,haveimplementedthebundle devel-opedbytheInstituteforHealthcareImprovementwhichis composed of: elevation of the head of the bed between 30◦ and45◦,dailysedationinterruptionandassessmentof
readinesstoextubate,dailyoralcarewithCHX,pepticulcer diseaseprophylaxisanddeepveinthrombosisprophylaxis.82 A3-yearstudyanalyzedtheimpactofaslight modifica-tiontothisbundle(withoutdailyoralcarewithCHX), veri-fyingthedecreaseofhospitalizationchargesandtherateof VAP.83Aliteraturereviewthatincludesseveralstudiesthat haveimplementedbundles topreventVAPconcludedthat thebundlesdecreasetheincidenceofVAP,durationofMV, ICUlengthofstay,mortalityandassociatedcosts.84
There is no complete concordance between the pre-ventive measures included in the studied bundles and the recommendations of the most recent guidelines. In fact, deep vein thrombosis prophylaxis is not indicated
in any guidelines as a preventive measure of VAP and, althoughpepticulcerdiseaseprophylaxisispresentinsome guidelines, it is not recommended on a routine basis.5,28 Therefore,studiesareneededtoassessbundlesthatinclude measures recommended by the most recent guidelines, in order to evaluate if they have a synergistic effect on patient’sclinicaloutcomesandinthedecreaseofVAP inci-dence,whenimplementedtogether.
Conclusion
Overthelastfewyearstherehasbeenanoticeableeffort todevelopandimprovepreventivemeasurestoreducethe incidence of VAP. It is crucial that this effort continues because,althoughthestrategiesdevelopedinrecentyears arepromising,VAPremainsanosocomialproblemwhichis difficulttocontrol,withhighratesofmortality,morbidity andhospitalcosts.
The preventive strategy of VAP focuses on modifiable risk factors, with several pharmacological and non-pharmacologicalmeasures available, whichaim toreduce therisk associated withendotracheal intubation and pre-ventthemicroaspirationofpathogenstothelowerairways. Preventivemeasuresincludeavoidanceofendotracheal intubation and use of noninvasive MV wheneverpossible, preferenceoforotrachealandorogastrictubes,weaningof ventilation combinedwithweaning of sedatives,use of a singleventilator circuit per patient,use of antibacterial-coatedETTpreferablywithapolyurethanecuff,aspiration of subglottic secretions,patient positioning,avoidanceof unnecessaryintra-hospitaltransfers,preferenceforenteral nutrition,useoforalantiseptics,goodhygienepracticesby health professionals, and disinfection of hospital settings andmedicaldevices.
Administrationofprobioticshasshownpromisingresults, although, to date, noguidelines recommend its use. The mostpromisingpreventivemeasuresinthenearfutureare thedevelopmentofnewETTandbundles.However, devel-opmentofabundlethatcontainsthecurrentrecommended preventivemeasures,inguidelinesissuedbyscientific medi-calsocieties,isstilllacking.
Ethical
disclosures
Protection of human and animal subjects.The authors declarethatnoexperimentswereperformedonhumansor animalsforthisstudy.
Confidentialityofdata.Theauthorsdeclarethatnopatient dataappearinthisarticle.
Right to privacy and informed consent.The authors declarethatnopatientdataappearinthisarticle.
Conflicts
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
References
1. Vincent JL, Rello J, Marshall J, Silva E, Anzueto A, Martin CD,etal.InternationalStudyofthePrevalenceOutcomesof InfectioninIntensiveCareUnits.JAMA.2009;302:2323---9.
2.Klompas M, Khan Y, Kleinman K, Evans RS, Lloyd JF, Stevenson K, et al. Multicenter evaluation of a novel surveillanceparadigmfor complicationsofmechanical venti-lation.PLoSOne. 2011;6:e18062,http://dx.doi.org/10.1371/ journal.pone.0018062.
3.Centers for Disease Control and Prevention. CDC/NHSN Pro-tocol Corrections, Clarification, and Additions, April; 2013. Available from: http://www.cdc.gov/nhsn/PDFs/pscManual/ 6pscVAPcurrent.pdf[accessedon02.05.13].
4.CravenDE.Epidemiologyofventilator-associatedpneumonia. Chest.2000;117:S186---7.
5.AmericanThoracicSocietyInfectiousDiseasesSocietyof Amer-ica.Guidelines for the managementof adultswith hospital-acquired, ventilator-associated, and healthcare-associated pneumonia.AmJRespirCritCare.2005;171:388---416. 6.Amin A. Clinical and economic consequences of
ventilator-associatedpneumonia.ClinInfectDis.2009;49:S36---43. 7.ChastreJ, Fagon JY.Ventilator-associated pneumonia. Am J
RespirCritCare.2002;165:867---903.
8.File TM. Epidemiology pathogenesis, microbiology, and diagnosis of hospital-acquired, ventilator-associated, and healthcare-associated pneumonia in adults; 2013. Available from: http://www.uptodate.com/contents/ epidemiology-pathogenesismicrobiology-and-diagnosis-of-hospital-acquired-ventilator-associated-and-healthcare associated-pneumonia-in-adults [last updated on 17.05.013; accessedonJune4].
9.CombesA,FiglioliniC,TrouilletJL,KassisN,WolffM,Gibert C,etal. Incidenceand outcome ofpolymicrobial ventilator-associatedpneumonia.Chest.2002;121:1618---23.
10.ParkDR.Themicrobiologyofventilator-associatedpneumonia. RespirCare.2005;50:742---63.
11.Martin SJ, Yost RJ. Infectious diseases in the critically ill patients.JPharmPract.2011;24:35---43.
12.AgrafiotisM,SiemposII,NtaidouTK,FalagasME.Attributable mortalityofventilator-associatedpneumonia:ameta-analysis. IntJTuberLungD.2011;15:1154---63.
13.MuscedereJG,DayA,HeylandDK.Mortalityattributable mor-tality,and clinicalevents as endpoints for clinicaltrials of ventilator-associatedpneumoniaand hospital-acquired pneu-monia.ClinInfecDis.2010;5:S120---5.
14.Rello J, Ollendorf DA, Oster G, Montserrat VL, Bellm L, Redman R, et al. Epidemiology and outcomes of ventilator-associatedpneumoniainalargeUSdatabase.Chest.2002;122: 2115---21.
15.Warren DK, Shukla SJ, Olsen M, Kollef MH, Hollenbeak CS, CoxMJ,et al. Outcome and attributable costof ventilator-associated pneumonia among intensive care unit patients in a suburban medical center. Crit Care Med. 2003;31: 1312---7.
16.ErbayRH,YalcinAN,ZencirM,SerinS,AtalayH.Costsandrisk factorsforventilator-associatedpneumoniainaTurkish Univer-sityHospital’sIntensiveCareUnit:a case-controlstudy.BMC PulmonMed.2004:4.
17.SafdarN,DezfulianC,CollardHR,SaintS.Clinicalandeconomic consequencesofventilator-associatedpneumonia:asystematic review.CritCareMed.2005;33:2184---93.
18.MuscedereJ,MartinCM,HeylandDK.Theimpactof ventilator-associated pneumonia on the Canadian health care system. JCritCare.2008;23:5---10.
19.KlompasM. Theparadox ofventilator-associated pneumonia preventionmeasures. CritCare. 2009:13, http://dx.doi.org/ 10.1186/cc8036.
20.Bonten MJ. Ventilator-associated pneumonia: preventing the inevitable.ClinInfectDis.2011;52:115---21.
21.SafdarN,CrnichCJ,MakiDG.Thepathogenesisof ventilator-associated pneumonia: itsrelevance to developing effective strategiesforprevention.RespirCare.2005;50:725---39.
22.Joseph NM, Sistla S, Dutta TK, Badhe AS, Parija SC. Ventilator-associatedpneumonia:areview.EurJInternMed. 2010;21:360---8.
23.Prescott HC, O’Brien JM. Prevention of ventilator-associated pneumonia in adults. F1000 MedRep. 2010:2, http://dx.doi.org/10.3410/M2-15.
24.HunterJD. Ventilatorassociatedpneumonia.PostgradMedJ. 2006;82:172---8.
25.GrapMJ,MunroCL,UnokiT,HamiltonVA,WardKR. Ventilator-associatedpneumonia:thepotentialcriticalroleofemergency medicineinprevention.JEmergMed.2012;42:353---62. 26.FroesF,PaivaJA,AmaroP,BaptistaJP,BrumG,BentoH,etal.
Consensusdocumentonnosocomialpneumonia.RevPort Pneu-mol.2007;13:419---86.
27.CoffinSE,KlompasM,ClassenD,AriasKM,PodgornyK,Anderson DJ,etal.Strategiestopreventventilator-associated pneumo-niainacutecarehospitals.InfectControlHospitalEpidemiol. 2008;29:S31---40.
28.MastertonRG,GallowayA, FrenchG,StreetM,ArmstrongJ, Brown E,et al. Guidelines for the management of hospital-acquiredpneumonia in theUK: report ofthe WorkingParty on Hospital-Acquired Pneumonia of the British Society for AntimicrobialChemotherapy.JAntimicrobChemother.2008;62: 5---34.
29.DíazLA,LlauradóM,RelloJ,RestrepoMI.Non-pharmacological prevention of ventilator associated pneumonia. Arch Bron-coneumol.2010;46:188---95.
30.BlanquerJ,AspaJ,AnzuetoA,FerrerM,GallegoM,RajasO, etal.SEPARguidelinesfornosocomialpneumonia.Arch Bron-coneumol.2011;47:510---20.
31.BrochardL.Mechanicalventilation:invasiveversusnoninvasive. EurRespirJ.2003;22:S31---7.
32.BurnsKE,AdhikariNK,KeenanSP,MeadeMO.Noninvasive pos-itivepressureventilationasaweaningstrategyforintubated adultswith respiratoryfailure. Cochrane DatabaseSyst Rev. 2010.
33.Thille AW, Richard JC, Brochard L. The decision to extu-bate in the intensive care unit. Am J Respir Crit Care. 2013;187:1294---302.
34.CawleyMJ.Mechanicalventilation:introductionforthe phar-macypractitioner.JPharmPract.2011;24:7---16.
35.Gali B, Goyal DG. Positive pressure mechanical ventilation. EmergMedClinNAm.2003;21:453---73.
36.KressJP,PohlmanAS,O’ConnorMF,HallJB.Dailyinterruption of sedative infusions in critically ill patients undergo-ing mechanical ventilation. New Engl J Med. 2000;342: 1471---7.
37.MuscedereJG,DodekP,KeenanS,FowlerR,CookD,Heyland DK.Comprehensiveevidence-basedclinicalpracticeguidelines forventilator-associatedpneumonia:Prevention.JCritCare. 2008;23:126---37.
38.Hesse DR, Kallstrom TJ, Mottram CD, Myers TR, Sorenson HM, Vines DL. Care of the ventilator circuit and its rela-tiontoventilator-associatedpneumonia.RespirCare.2003;48: 869---79.
39.Branson RD. The ventilator circuitand ventilator-associated pneumonia.RespirCare.2005;50:774---85.
40.BercaultN,WolfM,RungeI,FleuryJC,BoulainT.Intrahospital transportofcriticallyillventilatedpatients:ariskfactorfor ventilator-associatedpneumonia---amatchedcohortstudy.Crit CareMed.2005;33:2471---8.
41.AlexiouVG,IerodiakonouV,DimopoulosG,FalagasME.Impact ofpatient position onthe incidence ofventilator-associated pneumonia:ameta-analysisofrandomizedcontrolledtrials.J CritCare.2009;24:515---22.
42.MauriT,BerraL,KumwilaisakK,PiviS,UfbergJW,KueppersF, etal.Lateral-horizontalpatientpositionandhorizontal orien-tationoftheendotrachealtubetopreventaspirationinadult
surgicalintensivecareunitpatients:afeasibilitystudy.Respir Care.2010;55:294---302.
43.Deem S, TreggiariMM. New endotrachealtubes designed to preventventilator-associatedpneumonia:dotheymakea dif-ference?RespirCare.2010;55:1046---55.
44.RuppME,FitzgeraldT,MarionN,HelgetV,PuumalaS,Anderson JR, et al.Effect of silver-coatedurinarycatheters: efficacy, cost-effectiveness, andantimicrobial resistance.AmJInfect Control.2004;32:445---50.
45.Rello J, Kollef MH, Diaz E, Sandiumenge A, del Castillo Y, Corbella X, et al. Reduced burden of bacterial airway col-onization witha novel silver-coatedendotracheal tube in a randomized multiple-center feasibility study.Crit CareMed. 2006;34:2766---72.
46.KollefMH,AfessaB,AnzuetoA,VeremakisC,KerrKM, Margo-lisBD,etal.Silver-CoatedEndotrachealTubesandIncidence ofVentilator-AssociatedPneumonia:TheNASCENTRandomized Trial.JAMA.2008;300:805---13.
47.AfessaB,ShorrAF,AnzuetoAR,CravenDE,SchinnerR,Kollef MH.Associationbetweenasilver-coatedendotrachealtubeand reducedmortalityinpatientswithventilator-associated pneu-monia.Chest.2010;137:1015---21.
48.ShorrAF,ZilberbergMD,KollefMH.Cost-effectivenessanalysis ofasilver-coatedendotrachealtubetoreducetheincidenceof ventilator-associated pneumonia.InfectControl Hospital Epi-demiol.2009;30:759---63.
49.YoungPJ,BurchettK,HarveyI,BluntMC.Thepreventionof pul-monaryaspirationwithcontroloftrachealwallpressureusing asiliconecuff.AnaesthIntensCare.2000;28:660---5.
50.Dullenkopf A,GerberA,WeissM.Fluidleakagepasttracheal tubecuffs:evaluationofthenewmicrocuffendotrachealtube. IntensCareMed.2003;29:1849---53.
51.Young PJ, Pakeerathan S, Blunt MC, Subramanya S. A low-volume, low-pressure tracheal tube cuff reduces pulmonary aspiration.CritCareMed.2006;34:632---9.
52.Lucangelo U, Zin WA, Antonaglia V, Petrucci L, Viviani M, Buscema G,et al.Effect ofpositiveexpiratory pressureand typeoftrachealcuffontheincidenceofaspirationin mechan-icallyventilatedpatientsinanintensive careunit.CritCare Med.2008;36:409---13.
53.Dezfulian C, Shojania K, Collard HR, Kim HM, Matthay MA, Saint S. Subglottic secretion drainage for preventing ventilator-associatedpneumonia:ameta-analysis.AmJMed. 2005;118:11---8.
54.Klompas M. Prevention of ventilator-associated pneumonia. ExpertRevAntiInfectTher.2010;8:791---800.
55.KollefMH,SkubasNJ,SundtTM.Arandomizedclinicaltrialof continuousaspirationofsubglotticsecretionsincardiacsurgery patients.Chest.1999;116:1339---46.
56.SmuldersK,vanderHoevenH,Weers-PothoffI, Vandenbroucke-GraulsC.Arandomizedclinicaltrialofintermittentsubglottic secretiondrainageinpatientsreceivingmechanicalventilation. Chest.2002;121:858---62.
57.BouzaE,PérezMJ,Mu˜nozP,RincónC,BarrioJM,HortalJ. Con-tinuousaspirationofsubglotticsecretionsinthepreventionof ventilator-associatedpneumoniainthepostoperativeperiodof majorheartsurgery.Chest.2008;134:938---46.
58.Lacherade JC, JongheBD, GuezennecP,Debbat K,HayonJ, Monsel A, et al. Intermittent subglottic secretion drainage ventilator-associated pneumonia: a multicenter trial. Am J RespirCritCare.2010;182:910---7.
59.BouzaE, BurilloA.Advancesin thepreventionand manage-mentofventilator-associatedpneumonia.CurrOpinInfectDis. 2009;22:345---51.
60.ShiZ,XieH,WangP,WuY,ChenE,NgL,etal.Oralhygiene care for critically ill patients to prevent ventilator associ-ated pneumonia (Protocol). Cochrane Database of SystRev. 2010.
61.ChanEY,RuestA,MeadeMO,CookDJ.Oraldecontamination forpreventionofpneumoniainmechanicallyventilatedadults: systematicreviewandmeta-analysis.BritMedJ.2007:334. 62.MicekST,SkrupkyLP.Currentconceptsinthepreventionand
treatmentofventilator-associatedpneumonia.JPharmPract. 2010;23:25---32.
63.KoemanM,vanderVenA,HakE,JooreH,KaasjagerK,deSmet A,etal.Oraldecontaminationwithchlorhexidinereducesthe incidenceofventilator-associatedpneumonia.AmJRespirCrit Care.2006;173:1348---55.
64.TantipongH,MorkchareonpongC,JaiyindeeS,ThamlikitkulV. Randomizedcontrolledtrialandmeta-analysis oforal decon-taminationwith2%chlorhexidinesolutionforthepreventionof ventilator-associatedpneumonia. InfectControl Hospital Epi-demiol.2008;29:131---6.
65.File TM. Risk factors and prevention of hospital-acquired, ventilator-associated, and healthcare-associated pneumonia in adults; 2013. Available from: http://www.uptodate.com/ contents/risk-factors-and-prevention-ofhospital-acquired-ventilator-associated-and-healthcare-associated-pneumonia-in -adults[lastupdatedon21.02.13;accessedon26.04.13]. 66.deSmetA,KluytmansJ,CooperBS,MasciniEM,BenusR,van
derWerfTS,etal.Decontaminationofthedigestivetractand oropharynxinICUpatients.NewEnglJMed.2009;360:20---31. 67.OostdijkE,deSmetA,BlokH,GroenE,vanAsseltG,Benus
R, et al. Ecologicaleffects ofselective decontamination on resistantGram-negativebacterialcolonization.AmJRespirCrit Care.2010;181:452---7.
68.Schrezenmeir J, de Vrese M. Probiotics, prebiotics, and synbiotics --- approaching a definition. Am J Clin Nutr. 2001;73:S361---4.
69.Morrow LE, Kollef MH, Casale TB. Probiotic prophylaxis of ventilator-associatedpneumonia:ablinded,randomized con-trolledtrial.AmJRespirCritCare.2010;182:1058---64. 70.SiemposII,NtaidouTK,FalagasME.Impactoftheadministration
ofprobioticsontheincidenceofventilator-associated pneumo-nia:ameta-analysisofrandomizedcontrolledtrials.CritCare Med.2010;38:954---62.
71.Giamarellos-Bourboulis EJ, Bengmark S, Kanellakopoulou K, Kotzampassi K. Pro- and synbiotics to control inflammation and infection in patients with multiple injuries. J Trauma. 2009;67:815---21.
72.MathurP.Handhygiene:backtothebasicsofinfectioncontrol. IndianJMedRes.2011;134:611---20.
73.CentersforDiseaseControlandPreventionGuidelineforHand Hygiene in Health-Care Settings: Recommendations of the HealthcareInfectionControlPracticesAdvisoryCommitteeand theHICPAC/SHEA/APIC/IDSAHandHygieneTaskForce.MMWR RecommRep.2002:51.
74.ManiA,ShubangiAM,SainiR.Handhygieneamonghealthcare workers.IndianJDentRes.2010;21:115---8.
75.MethenyNA,ClouseRE,ChangY,StewartBJ,OliverDA,Kollef MH.Tracheobronchialaspirationofgastriccontentsincritically
illtube-fedpatients:frequency,outcomes,andriskfactors.Crit CareMed.2006;34:1007---15.
76.GramlichL,KichianK,PinillaJ,RodychNJ,DhaliwalR,Heyland DK.Does enteral nutritioncompared to parenteral nutrition resultinbetteroutcomesincriticallyilladultpatients?A sys-tematicreviewoftheliterature.Nutrition.2004;20:843---8. 77.AltintasND,AydinK,Türko˘gluMA,Abbaso˘gluO,TopeliA.Effect
of enteral versus parenteral nutrition on outcome of medi-calpatientsrequiringmechanicalventilation.NutrClinPract. 2011;26:322---9.
78.Artinian V, Krayem H, DiGiovine B. Effects of early enteral feedingontheoutcomeofcriticallyillmechanicallyventilated medicalpatients.Chest.2006;129:960---7.
79.Baxter AD, Allan J, Bedard J, Malone-Tucker S, Slivar S, LangillM,etal.Adherencetosimpleandeffectivemeasures reducestheincidenceofventilator-associatedpneumonia.Can JAnaesth.2005;52:535---41.
80.CasonCL,TynerT, SaundersS,BroomeL.Nurses’ implemen-tationofguidelinesfor ventilator-associatedpneumoniafrom thecentersfordiseasecontrolandprevention.AmJCritCare. 2007;16:28---36.
81.Institute for Healthcare Improvement. Evidence-Based Care Bundles; 2013. Available from: http://www.ihi.org/ explore/bundles/Pages/default.aspx[accessedon15.05.13]. 82.Institute for Healthcare Improvement. Implement of IHI
VentilatorBundle;2013.Available from:http://www.ihi.org/ knowledge/Pages/Changes/ImplementtheVentilato\rBundle. aspx[accessedon15.05.13].
83.Al-TawfiqJA,AbedMS.Decreasingventilator-associated pneu-monia in adult intensive care units using the Institute for Healthcare Improvement bundle. Am J Infect Control. 2010;38:552---6.
84.O’Keefe-McCarthyS,Santiago C,LauG. Ventilator-associated pneumonia bundled strategies: an evidence-based practice. WorldviewsEvidBasedNurs.2008;5:193---204.
85.OlaecheaPM,InsaustiJ,BlancoA,LuqueP.Epidemiologyand impactofnosocomialinfections.MedIntens.2010;34:256---67. 86.IbrahimEH,TracyL,HillC,FraserVJ,KollefMH.Theoccurrence
ofventilator-associatedpneumonia inacommunity hospital: riskfactorsandclinicaloutcomes.Chest.2001;120:555---61. 87.Tejerina E, Frutos-Vivar F, Restrepo MI, Anzueto A, Abroug
F, Palizas F, et al. Incidence, risk factors, and outcome of ventilator-associated pneumonia. J Crit Care. 2006;21: 56---65.
88.Gillespie R. Prevention and management of ventilator-associatedpneumonia--- theCareBundleapproach.Southern AfrJCritCare.2009;25:44---51.
89.JosephNM,SistlaS,DuttaTK,BadheAS,ParijaSC. Ventilator-associated pneumonia in a tertiary care hospital in India: incidenceandriskfactors.JInfectDevCtries.2009;3:771---7. 90.Jones RN. Microbialetiologies of hospital-acquired bacterial
pneumoniaandventilator-associatedbacterialpneumonia.Clin InfectDis.2010;51:S81---7.