CASE REPORT
Aortic Dissection Repair Using the STABILISE Technique Associated with
Arch Procedures: Report of Two Cases
Alice Lopesa,b,*, Ryan Gouveia Meloa,b,c, Miguel L. Gomesa,b, Pedro Garridoa,b, Nádia Junqueirab,d, Gonçalo Sobrinhoa,b,c, Ruy Fernandes e Fernandesa,b,c, João Leitãob,e, Ângelo Nobreb,c,d, Luís M. Pedroa,b,c a
Vascular Surgery Department, Heart and Vessels Division, Hospital de Santa Maria (CHLN), Lisbon, Portugal
b
Lisbon Academic Medical Centre, Lisbon, Portugal
c
Lisbon School of Medicine, University of Lisbon, Portugal
d
Cardio-Thoracic Surgery Department- Heart and Vessels Division, Hospital de Santa Maria (CHLN), Lisbon, Portugal
e
General Radiology Department, Hospital de Santa Maria (CHLN), Lisbon, Portugal
Introduction:The stent assisted balloon induced intimal disruption and relamination in aortic dissection repair (STABILISE) technique is being increasingly used for the treatment of complicated aortic dissections. However, as it is a fairly recent technique, the scientific information is limited.
Report:In this paper we report two cases of the STABILISE technique associated with procedures in the ascending aorta and supra-aortic trunks, consisting of a“frozen elephant trunk” procedure in one case and in the other, a carotid endarterectomy associated with reimplantation of the vertebral artery and partial arch debranching.
Discussion:In conclusion, while acknowledging the need for longer follow up and greater experience to support the safety and efficacy of this procedure, the two cases reported confirm that the STABILISE technique is a valid endovascular alternative in the treatment of complicated aortic dissections.
Ó 2019 The Authors. Published by Elsevier Ltd on behalf of European Society for Vascular Surgery. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Article history: Received 3 October 2018, Revised 4 December 2018, Accepted 6 January 2019, Keywords:Aortic dissection, STABILISE, Bare stent, Stent graft, Endovascular
INTRODUCTION
Acute aortic dissection is a common catastrophic event affecting the aorta. According to the current therapeutic paradigm for distal dissection, intervention is reserved for complications such as impending rupture, aneurysmal dilatation, uncontrolled pain, or hypertension and obstruc-tion of aortic branches with organ malperfusion.1,2 Endo-vascular techniques, when anatomically feasible, are newer less invasive treatment options for severely ill patients, and have better outcomes than open surgery.3
“Stent assisted balloon induced intimal disruption and relamination in aortic dissection repair” (STABILISE) is a new development of the previously introduced PETTICOAT technique, the goal of which is to achieve an immediate remodelling of the thoraco-abdominal aorta with conse-quent obliteration of the false lumen (FL) through the reapposition of the dissectionflap to the outer layers of the aorta.3 It is usually indicated in a subset of patients with type B dissection (TBAD) but in some cases a proximal
landing zone (PLZ) has to be obtained through interventions in the aortic arch.
The aim of this paper is to report two cases of compli-cated aortic dissection successfully treated with the STA-BILISE technique in combination with arch interventions, and to discuss the technical details of the procedures. CASE 1
A 70 year old male hypertensive patient with ischaemic heart disease presented to the emergency department with pleuritic thoracalgia. The patient reported a previous history of chest pain three months before, although he did not seek medical assistance at the time.
Computed tomography angiography (CTA) revealed a type A aortic dissection (TAAD) with the primary entry tear in the ascending aorta, which was also aneurysmal (6 cm) at that level. Distally, the dissection extended to the left external iliac artery. All the renal and visceral vessels emerged from the true lumen (TL), and the FL was partially thrombosed and causing extreme compression of the TL at lower descending thoracic aorta level (Fig. 1). There was no overt organ ischaemia.
Considering the ascending aortic aneurysm and compression of the TL, a one stage hybrid approach was proposed, consisting of the “frozen elephant trunk” (FET) procedure (Fig. 2) followed by a STABILISE technique (Fig. 3).
* Corresponding author. Hospital de Santa Maria, Serviço de Cirurgia Vascular, Avenida Professor Egas Moniz, 1649-035, Lisboa, Portugal.
E-mail address:[email protected](Alice Lopes).
2405-6553/Ó 2019 The Authors. Published by Elsevier Ltd on behalf of European Society for Vascular Surgery. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
https://doi.org/10.1016/j.ejvssr.2019.01.003
The procedure was performed under general anaesthesia and cerebrospinalfluid (CSF) drainage with pressure moni-toring (<10 mmHg). Initially, a hydrophilic guidewire was introduced via the right femoral artery to the ascending aorta under fluoroscopy and transoesophageal echocardi-ography guidance and its placement in the TL was confirmed by small contrast injections at sequential levels through a 6F sheath. After wire placement in the TL, the open intervention was performed by cardiothoracic sur-geons, with the patient under deep hypothermic circulatory arrest, and consisted in the replacement of the ascending aorta and arch using a hybrid stent graft system (E-vita Open PlusÒ, Jotec GmbHÒ, Hechingen, Germany) over the previously mentioned wire, with an“island” reimplantation of the supra-aortic branches, thus allowing the creation of a FET and a PLZ for the endovascular stage.
After replacing the hydrophilic guidewire with an extra stiff wire (LunderquistÒ, Cook MedicalÒ, Bloomington, IN, USA), a stent graft was deployed (ZTAÒ 34-113, Cook MedicalÒ) with the proximal landing in the FET and aiming to cover the primary entry tear. A Cook Medical Zenith Dissection Endovascular StentÒ(ZDESÒ36-164-2) was then deployed through the visceral aorta and distally 5 cm below the renal arteries. Finally, a 46 mm semi-compliant, poly-urethane balloon (CodaÒ, Cook MedicalÒ) was carefully used to sequentially dilate (craniocaudal direction) the stents in order to obliterate the FL.
The completion angiogram and the post-operative CTA confirmed adequate sealing and complete realignment of the aorta with TL patency and FL obliteration as well as patency of all aortic branches (Fig. 1).
Patient recovery was uneventful.
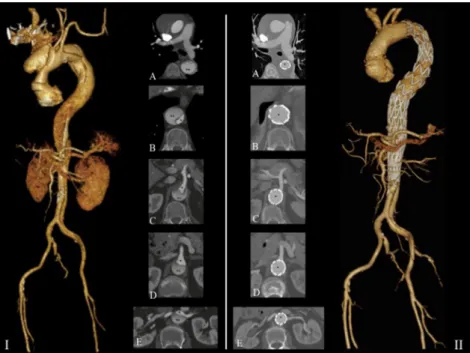
Figure 1. I. Pre-operative computed tomography angiography of a“subacute” type A aortic dissection. Axial scans with the true (*) and false (**) lumens at the level of the descending thoracic aorta (A), thoraco-abdominal junction (B), celiac trunk (C), superior mesenteric artery (D), and renal arteries (E). II. Computed tomography angiography after STABILISE procedure at the same levels with complete remodelling of the thoraco-abdominal aorta.
Figure 2. Ascending aorta and arch replacement using a hybrid stent graft system, over a previously inserted stiff wire, thus allowing the creation of a“frozen elephant trunk” and a proximal landing zone for the endovascular stage (A and B); aortic dissection (C).
CASE 2
A 69 year old male with arterial hypertension and dyslipi-daemia was admitted because due to sudden intense back pain. CTA confirmed TBAD with the primary entry tear located immediately distal to the left subclavian artery (LSA) and extending to the aortic bifurcation. Both the TL and the FL were patent, the TL was severely compressed by the FL and all the renal and visceral arteries emerged from the TL. Moreover, the arch had a bovine morphology and the left vertebral artery (LVA) took origin from the aortic arch.
The patient was managed conservatively and discharged under strict antihypertensive medication. Four months after the initial event he reported severe bilateral lower limb claudication which was attributed to the extreme compression of the TL by the FL in the visceral segment although no evidence of visceral malperfusion was present (Fig. 4). Additionally, the duplex scan evaluation revealed an 80% bilateral carotid stenosis.
The patient was admitted for a staged hybrid procedure with left carotid endarterectomy (CEA) associated with partial arch debranching consisting in re-implantation of the LVA into the CCA and left carotidesubclavian bypass with proximal ligation of the LSA.
One week after thefirst procedure, and after placement of a CSF drain, a STABILISE technique was performed, consisting of TL catheterisation with an extra stiff guidewire (LunderquistÒ; Cook MedicalÒ) and deployment of two stent grafts (ZTAÒP-34-209þ ZTAÒP-34-161, Cook Medi-calÒ) 3 cm above the celiac trunk. A Cook Medical Zenith Dissection Endovascular StentÒ (ZDESÒ 34-180) was then deployed over the visceral aorta and landing distally four cm below the renal arteries. Finally, a 46 mm Coda balloon
(Cook Medical) was used to sequentially dilate (craniocau-dal direction) the stent grafts and the dissection stent aiming to obliterate the FL (Fig. 5). The completion angio-gram and the post-operative CTA confirmed the complete realignment of the aorta with TL patency, FL obliteration, and patency of all aortic branches (Figs. 4 and 6).
There were no complications. DISCUSSION
Two cases of complicated aortic dissections successfully managed by the STABILISE technique are reported, one “subacute” type A and one chronic type B.
Regarding endovascular treatment of TBAD, the focus for some time has been on the covering the entry tear with thoracic endovascular aneurysm repair (TEVAR).4However, as has been shown, the natural history of these conditions leads to further degeneration and complications if the distal aorta is not dealt with.1,2,5The STABILISE technique, like the initial PETTICOAT technique, seeks to solve this conundrum.6,7
As an evolution from the initial PETTICOAT, the STABILISE technique adds balloon dilatation of the entire stented aorta to rupture the lamella and therefore occlude the FL, make the TL diameter return to normal, and recover the normal perfusion of the aortic branches. The main advan-tage is the promotion of a complete remodelling of the aorta through the reapposition of theflap against the aortic wall.6,7
As it is a fairly recent technique, few series have been published. Nevertheless, better long-term results and a lower rate of re-intervention than previous approaches are to be expected.3
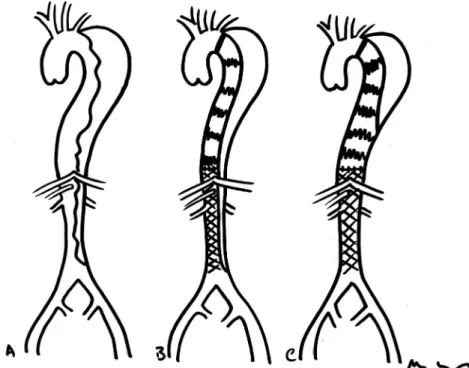
Figure 3. Schematic representation of the STABILISE technique. (A) Type B aortic dissection. (B) After implantation of a proximal covered stent graft and placement of a distal bare metal stent, with residual flow in the false lumen (PETTICOAT technique). (C) Intimal re-apposition after ballooning the stent graft and dissection stent with obliteration of the false lumen (STABILISE technique).
There are, however, some issues that need to be clarified with further experience. One of them is the ideal timing for the procedure. Although it can be performed at any stage of the dissection,6it is assumed that the risk of aortic rupture in the acute phase may be too high and interventions should be limited to emergency cases.3 In thesefirst two weeks, a simple PETTICOAT to fix the malperfusion cases may be safer than to dilate a weak aorta. The subacute phase (2e12 weeks) seems to be a better time target considering the balance between efficacy and the risk of complications. During this phase, the intimal flap remains flexible and the potential for positive aortic remodelling is maximal. For chronic dissection cases, theflap is more rigid
and organised and some degree of aneurysmal degenera-tion may already be present, and therefore complete opening of the TL may be difficult.
The second issue that needs to be addressed is the indication for the procedure. The most common indication in the literature is decreased perfusion of the aortic collateral arteries2 and in both the cases the aim was to aggressively re-open the TL as it had collapsed over the ostia of the visceral vessels. Additionally, in the second case, there was severe malperfusion of the lower limbs causing disabling claudication. However, for some authors, the disruption and reapposition of the lamella to the outer aortic wall may also have a positive impact on later aortic
Figure 4. I. Pre-operative computed tomography angiography of a chronic type B aortic dissection. Axial scans with the true (*) and false (**) lumens at the level of the descending thoracic aorta (A), thoraco-abdominal junction (B), celiac trunk (C), superior mesenteric artery (D), and renal arteries (E). II. CTA after STABILISE procedure at the same levels with complete remodelling of the thoraco-abdominal aorta.
Figure 5. Sequential ballooning of the bare metal stent in a caudal direction with progressive expansion of the stent and consequent reapposition of theflap to the outer aortic wall.
remodelling. Further studies are needed to confirm this hypothesis.1,3,6
The cases reported have another feature related to the need for associated aortic arch procedures. These were necessary to promote an adequate PLZ for the descending aortic interventions. In case 1 an open arch replacement was performed in a single stage procedure, demonstrating that a concomitant approach to these two aortic segments is possible and had no major disadvantages. In case 2, the arch intervention was a typical zone 2 debranching (but promoting a “type zone 1” debranching because of the presence of a bovine arch morphology). The less common procedure was the debranching of the LVA that arose directly from the aorta, the deliberate occlusion of which may be an unpredictable cause of stroke. Therefore, the option to add a left CEA took into account the need to
manipulate the left carotid arteries and also that a bilateral stenosis was present.
CONCLUSION
Whilst acknowledging the need for longer follow up and greater experience to support the safety and efficacy of this procedure, the two cases add to the knowledge that the STABILISE technique is a valid endovascular alternative in the treatment of complicated aortic dissections.6
CONFLICT OF INTEREST None.
FUNDING None. REFERENCES
1 Lombardi JV, Cambria RP, Nienaber CA, Chiesa C, Teebken O,
Lee A, et al. Prospective multicenter clinical trial (STABLE) on the endovascular treatment of complicated type B aortic dissection using a composite device design. J Vasc Surg 2012;55:629e40. 2 Canaud L, Faure E, Ozdemir BA, Alric P, Thompson M. Systematic review of outcomes of combined proximal stent-grafting with distal bare stenting for management of aortic dissection. Ann Cardiothorac Surg 2014;3:223e33.
3 Melissano G, Bertoglio L, Rinaldi E, Mascia D, Kahlberg A,
Loschi D, et al. Satisfactory short-term outcomes of the STABI-LISE technique for type B aortic dissection. J Vasc Surg 2018;68: 966e75.
4 Nienaber CA, Kische S, Rousseau H, Eggebrecht H, Rehders TC, Kundt G, et al. Endovascular repair of type B aortic dissection: long-term results of the randomized investigation of stent grafts in aortic dissection trial. Circ Cardiovasc Interv 2013;6:407e16.
5 De Luccia N. Disruption of membrane to remodel aorta after
type B dissection: the final solution? Eur J Vasc Endovasc Surg 2018;56:216.
6 Hofferberth SC, Nixon IK, Boston RC, McLachlan CS, Mossop PJ. Stent-assisted balloon-induced intimal disruption and relami-nation in aortic dissection repair: the STABILISE concept. J Thorac Cardiovasc Surg 2014;147:1240e5.
7 Faure EM, Batti SE, Rjeili MA, Julia P, Alsac JM. Mid-term out-comes of stent assisted balloon induced intimal disruption and relamination in aortic dissection repair (STABILISE) in acute type B aortic dissection. Eur J Vasc Endovasc Surg 2018;56:209e15. Figure 6. Post-operative computed tomography angiography of a
chronic type B aortic dissection showing a patent left vertebral artery reimplanted in the left common carotid artery.