www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
REVIEW
ARTICLE
Different
clinical
presentation
of
intralabyrinthine
schwannomas
---
a
systematic
review
夽
Thaís
Gomes
Abrahão
Elias,
Adriana
Perez
Neto,
Ana
Tereza
Silveira
Zica,
Marcos
Luiz
Antunes
∗,
Norma
de
Oliveira
Penido
UniversidadeFederaldeSãoPaulo(UNIFESP),DepartamentodeOtorrinolaringologiaeCirurgiadeCabec¸aePescoc¸o,SãoPaulo, SP,Brazil
Received31January2018;accepted17May2018
KEYWORDS
Schwannoma; Neuroma; Neurilemmoma; Intralabyrinthine schwannoma
Abstract
Introduction:Intralabyrinthineschwannomaisarare,benigntumorthataffectsthemost termi-nalportionsofthevestibularandcochlearnerves.Thistumorcanbeclassifiedinto10subtypes, accordingtoitsinnerearlocation.
Objective: Tocarryoutacomprehensivereviewofthemostfrequentauditorymanifestations secondarytotheintralabyrinthineschwannoma,describingthepossibleunderlying pathophy-siologicalmechanisms.
Methods:Systematicreview oftheliteratureuntil October2017usingthePubMed,Web of ScienceandScopusdatabases.Theinclusioncriteriawereclinicalmanifestationsofthe intral-abyrinthineschwannoma.Threeresearchersindependentlyassessedthearticlesandextracted relevantinformation.Thedescriptionofacaseofanintravestibularsubtypeintralabyrinthine schwannomawithmultipleformsofclinicalpresentationswasusedasanexample.
Results:Twenty-sevenstudiesmetourinclusioncriteria.Themostcommonintralabyrinthine schwannomasubtypewastheintracochlear,followedbytheintravestibulartype.Allthecases demonstratedhearingloss,usuallyprogressivehearingloss.
Conclusion: Thediagnosisofintralabyrinthineschwannomasisbasedonhigh-resolution mag-neticresonanceimagingandshouldbeincludedinthedifferentialdiagnosisofpatientswith vestibulocochlearcomplaints.Althoughthereareapproximately600casesintheliterature,we stilllackadetaileddescriptionoftheclinicalevolutionofthepatients,correlatingitwithMRI findingsoftemporalbonesandtumorsubtype.
© 2018 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
夽 Pleasecitethisarticleas:EliasTG,PerezNetoA,ZicaAT,AntunesML,PenidoNO.Differentclinicalpresentationofintralabyrinthine
schwannomas---asystematicreview.BrazJOtorhinolaryngol.2019;85:111---20.
∗Correspondingauthor.
E-mail:[email protected](M.L.Antunes).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
https://doi.org/10.1016/j.bjorl.2018.05.007
PALAVRAS-CHAVE
Schwannoma; Neuroma; Neurilemoma; Schwannoma intralabiríntico
Diferentesapresentac¸õesclínicasdoschwannomaintralabiríntico---umarevisão
sistemática
Resumo
Introduc¸ão:Schwannomaintralabirínticoéumtumorbenigno,raro,queafetaasporc¸õesmais terminaisdosnervosvestibularecoclear.Estetumorpodeserclassificado,deacordocomsua localizac¸ãonaorelhainterna,em10subtipos.
Objetivo:Realizar uma revisão abrangente das manifestac¸ões auditivas mais frequentes secundáriasaoschwannomaintralabirínticoedescreverospossíveismecanismos fisiopatológi-cossubjacentes.
Método: Revisãosistemáticadaliteraturaatéoutubrode2017nasbasesdedadosPubMed, Web ofScience e Scopus.O critériode inclusão foi manifestac¸ões clínicas do schwannoma intralabiríntico.Trêspesquisadores avaliaramdeformaindependente osartigoseextraíram informac¸õesrelevantes.Exemplificamoscomadescric¸ãodeumcasodeschwannoma intral-abirínticosubtipointravestibularcommúltiplasformasdeapresentac¸õesclínicas.
Resultados: Vinteseteestudoscontemplaramnossoscritériosdeinclusão.Osubtipodo schwan-nomaintralabirínticomaiscomumencontradofoiointracoclear,seguidopelointravestibular. Todososcasosapresentaramalterac¸ãoauditiva,normalmenteperdaauditivaprogressiva. Conclusão:Odiagnósticodeschwannomasintralabirínticosbaseia-seemexamesderessonância magnéticadealtaresoluc¸ãoedeveserincluídonodiagnósticodiferencialdepacientescom queixasvestibulococleares.Apesardetermosaproximadamente600casosnaliteratura,ainda nosfaltadescric¸ãodetalhadadaevoluc¸ãoclínicadospacientesemcorrelac¸ãocomachadosna ressonânciamagnéticadeossostemporaiseosubtipotumoral.
© 2018 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Intralabyrinthineschwannomaisarare,benigntumorthat affects the most terminal portions of the vestibular and cochlearnerves.Itcanbelocatedinthevestibule,cochlea or semicircular canals.1 Patients usually have nonspecific symptoms, including hearing loss, tinnitus and vertigo.2 Amongtheresultingsymptoms,themostfrequentishearing loss,whichaffects95%ofthepatients.Mosttimes,thisloss isslowandprogressive,butitmaybesuddenorfluctuating. Lesscommon symptomsinclude tinnitus (51%),imbalance (35%), vertigo (22%) and ear fullness (2%), which may be presentaloneorincombination.3,4
In1972,Karlan etal.5reportedthefirstintraoperative findingsof theintralabyrinthineschwannoma,whichwere complementedin1979 withthe histopathological descrip-tionof a patient’s temporal bone withthe same lesion.6 However,only after 1987 studies were published empha-sizingtheimportanceofmagneticresonanceimaging(MRI) studiesinthediagnosisofthisdisease.7Currently,the gold-standardexaminationforthediagnosisofintralabyrinthine
schwannoma is the temporal bone MRI, which may show
tumorenhancementinpost-gadoliniumT1-weightedimages andfillingdefectsinT2-weightedimages.5,6
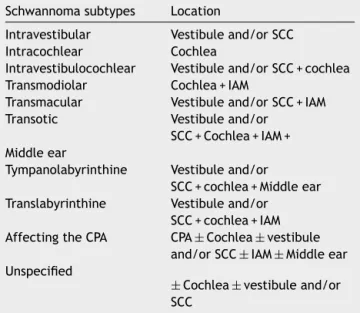
The intralabyrinthine schwannoma can be classified accordingtoitslocationintheinnerear.Initially,seven sub-typeswereidentifiedbyKennedyetal.,andsubsequently,in 2013,VanAbeletal.,aimingatusingamorespecific nomen-clature regarding tumor location, added another three subtypes (Table 1).7,8 The controversy remains regarding whichsubtypeoftheintralabyrinthineschwannomawould
Table1 ModifiedKennedyclassificationsystem.7
Schwannomasubtypes Location
Intravestibular Vestibuleand/orSCC
Intracochlear Cochlea
Intravestibulocochlear Vestibuleand/orSCC+cochlea
Transmodiolar Cochlea+IAM
Transmacular Vestibuleand/orSCC+IAM
Transotic Vestibuleand/or
SCC+Cochlea+IAM+
Middleear
Tympanolabyrinthine Vestibuleand/or
SCC+cochlea+Middleear
Translabyrinthine Vestibuleand/or
SCC+cochlea+IAM
AffectingtheCPA CPA±Cochlea±vestibule
and/orSCC±IAM±Middleear
Unspecified
±Cochlea±vestibuleand/or
SCC
SCC, semicircularcanals;IAM, internalauditorymeatus;CPA, cerebellopontineangle.
be the most common; however, most studies state that the intracochlear location is the most often found, with semicircularcanalsbeingmorerarelyinvolved.9
Articles selected during the data search
( n = 330 )
After title and abstract analysis
After removal of articles in duplicate
After reading the full-text articles ( n = 115 )
( n = 40 )
( n = 27)
Figure1 Flowchartshowingthearticleselectionprocess.
tointralabyrinthineschwannomaanditsassociationwiththe lesionsubtype.Thus,theaimofthisstudyistocarryouta comprehensivereview ofthemostfrequenthearing mani-festationssecondarytotheintralabyrinthineschwannoma, describingthepossibleunderlyingpathophysiological mech-anisms.Atthesametime,wereportthecaseofapatient withhearinglosssecondarytotheintralabyrinthine schwan-nomaoftheintravestibularsubtype.
Methods
Systematicreview
AsystematicreviewwascarriedoutinthePubmed,Webof ScienceandScopusdatabasesuntilOctober2017.The fol-lowingdescriptorswereused,indicated inthePortuguese language Health Sciences Descriptors (DeCS) terminology (Schwannoma,Neurilemoma, Neuroma), aswell as in the Englishlanguage(Schwannoma,Neurilemmoma,Neuroma). Thesearchstrategiesforthedifferentdatabasesareshown inTable2.
The inclusion criteria consisted of studies describing clinical manifestations of intralabyrinthine schwannoma, irrespectiveofitssubtype.Initially, thetitleandabstract inEnglishwereread,andthenthefull-textofstudiesthat mettheinclusioncriteriawerereadintheirentirety.
Three investigatorsindependentlyassessedthe articles andextractedrelevantinformation,anddiscrepancieswere resolvedbymutualagreement.Inacomplementarymanner, we exemplified the literature review findings by describ-ing a clinical case of an intralabyrinthine schwannoma (intravestibular subtype) with multiple forms of clinical presentation.
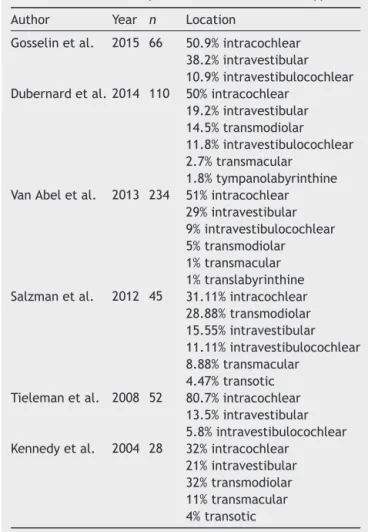
Table3 Mainintralabyrinthineschwannomassubtypes.
Author Year n Location
Gosselinetal. 2015 66 50.9%intracochlear 38.2%intravestibular 10.9%intravestibulocochlear Dubernardetal. 2014 110 50%intracochlear
19.2%intravestibular 14.5%transmodiolar 11.8%intravestibulocochlear 2.7%transmacular
1.8%tympanolabyrinthine VanAbeletal. 2013 234 51%intracochlear
29%intravestibular 9%intravestibulocochlear 5%transmodiolar 1%transmacular 1%translabyrinthine Salzmanetal. 2012 45 31.11%intracochlear
28.88%transmodiolar 15.55%intravestibular 11.11%intravestibulocochlear 8.88%transmacular
4.47%transotic Tielemanetal. 2008 52 80.7%intracochlear
13.5%intravestibular 5.8%intravestibulocochlear Kennedyetal. 2004 28 32%intracochlear
21%intravestibular 32%transmodiolar 11%transmacular 4%transotic
Results
Descriptionofthesystematizedliteraturesearches
Thesearchforarticlesinthedatabasesidentified330 arti-cles,ofwhich27wereincludedinthisreview(Fig.1).
According to the Oxford Center for Evidence-Based Medicineclassificationaboutthelevelsofscientificevidence ofthe27articlesreadasfull-textarticles,5were System-atic Reviews (with homogeneity) of Cohort Studies (level 2A),1wasanArticleonObservationofTherapeuticResults, EcologicalStudy(level2C)and21wereCaseReports(level 4).
Regardingthemaintumorlocation,therewasa consen-susamongthestudiesthattheintracochlearsubtypeinall studies wasthe most frequent, followed by the intraves-tibulartype,excepttheonebySalzmanetal.,whofound thetransmodiolarsubtypeasthesecondmostfrequenttype (Table3).
Table2 Searchstrategy.
Database Searchstrategy Articles
Table4 Mainmanifestationsofintralabyrinthineschwannomas.
Author Year n Clinicalpicture
Plontkeetal. 2017 12 100%hearingloss
Covellietal. 2017 1 Hearingfluctuationandvertigo
Fukushimaetal. 2017 1 Suddenhearingloss
Plontkeetal. 2017 1 Suddenhearingloss
Sabatinoetal. 2017 1 Rapidlyprogressivehearinglossandvertigo
Jerinetal. 2016 5 40%progressivehearingloss
40%suddenhearingloss 20%vertigo
Shupaketal. 2016 7 95%progressivehearingloss
Gosselinetal. 2015 66 Nodescriptionoftheclinicalcase
Leeetal. 2015 1 Suddenhearinglossandvertigo
Dubernardetal. 2014 110 94.5%progressivehearingloss
59.1%vertigo
Bittencourtetal. 2014 1 Hearingfluctuationandtinnitus
Kimetal. 2013 1 Suddenhearingloss
Schuttetal. 2013 1 Hearingfluctuation,earfullnessandvertigo
VanAbeletal. 2013 234 84%progressivehearingloss
3%hearingfluctuation 43%vertigo
Salzmanetal. 2012 45 60%progressivehearingloss
31.11%suddenhearingloss 8.89%hearingfluctuation 35.56%vertigo
Gordtsetal. 2011 1 Hearingfluctuationandtinnitus
Magliuloetal. 2009 1 Suddenhearinglossandvertigo
Brozek-Madryetal. 2009 1 Suddenhearinglossandvertigo
Tielemanetal. 2008 52 83.67%progressivehearingloss
14.28%suddenhearingloss 19.23%vertigo
Jiaetal. 2008 4 75%progressivehearingloss
25%suddenhearingloss 75%vertigo
Nishimuraetal. 2008 1 Suddenhearinglossandtinnitus
Lellaetal. 2007 7 71.42%progressivehearingloss
28.5%suddenhearingloss 57.14%vertigo
Kennedyetal. 2004 28 61%progressivehearingloss
32%suddenhearingloss 7%hearingfluctuation 71%tinnitus
29%vertigo
Greenetal. 1999 4 75%progressivehearingloss
25%suddenhearingloss 75%vertigo
Deuxetal. 1998 3 Progressivehearingloss,tinnitusandvertigo
Weedetal. 1994 1 Progressivehearinglossandtinnitus
DeLozieretal. 1979 2 Progressivehearinglossandvertigo
Regardingthepatients’clinicalpicture,themainclinical manifestations are shown in Table 4 and Fig. 2. Patient management reporting was carried out for 486 patients. In 276 patients (56%), clinical follow-up with serial MRI waschosen. In 210 (44%) patients, the patientchose the surgical management since most of them were patients
51.85% 51.85%
25.93% 25.93%
66.67%
n = 27 articles
7.41% 7.41%
Progressive HL Sudden HL Hearing fluctuation Unspecified HL Vertigo Tinnitus Ear fullness
Figure2 Mainmanifestationsoftheintralabyrinthineschwannomasinthe27articles.
Descriptionofacaseofintralabyrinthine schwannomaoftheintravestibularsubtype accordingtothemodifiedKennedyclassification7
A38-year-oldfemalepatientcametotheoutpatientclinic to have a consultation with an otorhinolaryngologist due todizzinessandimbalance for3 years.Shereported that eachepisodelastedonlyafewseconds,withnotriggering
factorsorsymptomimprovementorworsening.Theevents wereofminimalintensityanddidnothindertheactivities ofdaily living. After afew weeks of the condition onset, thedizzinessbecamerotationalandwastriggeredbyhead movementstotheleft.Thisdizzinesssymptomwithanew characteristic lastedfor minutesand also ceased sponta-neously. When questioned, she denied headaches, visual or auditory symptoms associated withdizziness. She also
RE Audiometry 250
-10 -10
0 0
10 10
20 20
30 30
40 40
50 50
60 60
70 70
80 80
90 90
100 100
110 110
120 120
dB
Logoaudiometry Stapedial reflex dB
250
500 1K 2K 4K 8K Hz 500 1K 2K 4K 8K Hz
LE
I R F
Right afferent pathway Left afferent pathway
S T R I R F
Masking Masking
RE RE
40 00
00 00 00 00
90 80
IPSI CONTRA
85 90 90
45 35 55 55
80 80 85
90 50
75 84 92
CONTRA IPSI
85 85
100
SN
WN,PN,SN, WN,PN,SN,
SN
LE LE
Hz
500 1k 2k 4k dBNA
dbHL dbHL
dbHL dbHL
dbHL dbHL
dbHL Threshold Threshold
dBM'S dBM'S
Mono % Oi % Tri %
B
C
Figure3 (A)Audiometryshowingmoderatesensorineurallossintheleftear.(B)T2-weightedMRIofthetemporalbones,axial
view,withhyposignalintheleftvestibule. (C)T1-weightedMRIofthetemporalbones,axialview,withcontrast,lesion shows
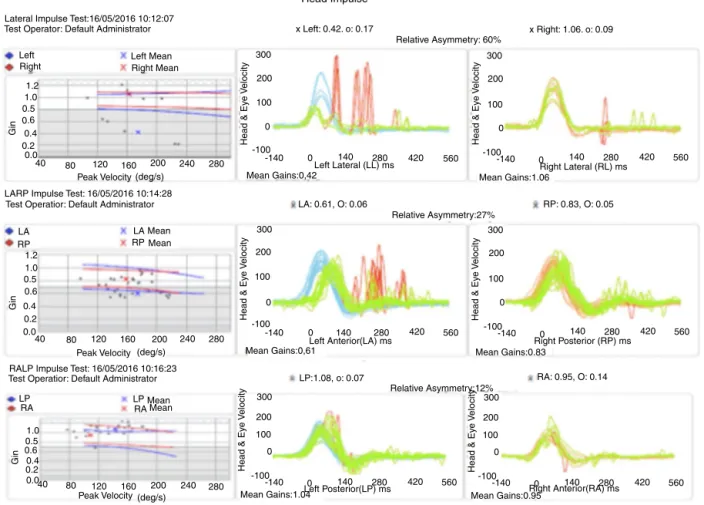
Head Impulse
Lateral Impulse Test:16/05/2016 10:12:07
Left LA LP LP LA RP RP RA RA Left Mean Mean Mean Mean Mean 1.2 1.0 0.5 0.6 0.4 0.2 0.0
40 80 120 160 200 240 280
1.2 1.0 0.5 0.6 0.4 0.2 0.0
40 80 120 160 200 240 280
LARP Impulse Test: 16/05/2016 10:14:28
RALP Impulse Test: 16/05/2016 10:16:23 Test Operatior: Default Administrator
Test Operatior: Default Administrator Peak Velocity
Peak Velocity Right Mean Right
Test Operator: Default Administrator x Left: 0.42. o: 0.17
LA: 0.61, O: 0.06
LP:1.08, o: 0.07
x Right: 1.06. o: 0.09 Relative Asymmetry: 60%
300 300 300 200 200 200 100 100 100 0 0 0 0 0 0 -100 -100 -100 -140 -140 -140 140 140 140 280 280 280 420 420 420 560 300 200 100 0 0 -100
-140 140 280 420 560
300 200 100 0 0 -100
-140 140 280 420 560
300 200 100 0 0 -100
-140 140 280 420 560
560 560 Mean Gains:1.06 Mean Gains:0,42 Mean Gains:0,61 Relative Asymmetry:27% Relative Asymmetry:12% Mean Gains:0.83 Mean Gains:0.95 Mean Gains:1.04
Right Lateral (RL) ms
Right Posterior (RP) ms
Right Anterior(RA) ms Left Anterior(LA) ms
Left Posterior(LP) ms
RP: 0.83, O: 0.05
RA: 0.95, O: 0.14 Left Lateral (LL) ms
Head & Ey
e
V
elocity
Head & Ey
e
V
elocity
Head & Ey
e
V
elocity
Head & Ey
e
V
elocity
Head & Ey
e
V
elocity
Head & Ey
e V elocity (deg/s) (deg/s) Gin Gin Gin 1.0 0.5 0.6 0.4 0.2
0.040 80 120 160 200 240 280 Peak Velocity (deg/s)
Figure4 Head-impulsetestshowingleftvestibularhypofunction.
deniedcomorbidities or continuous intakeof medications foranydisease.
The general physical examination, otorhinolaryngolog-ical evaluation and neurological tests did not show any alterations, nor did the auditory assessment (audiometry and immittance audiometry). The patient was also sub-mittedtovideo-electronystagmography,whichshowedleft hypofunctiononthecalorictest.Consideringtheresultsof thephysical, audiometricandvestibularfunctiontests, -histaminetherapywasstarted,ofwhichdosewasgradually increasedinthefirst60 daysuntilreachingthemaximum recommendeddose (216mg/day)inadditiontomeclizine. However,thepatientdid notshow improvementwiththe useofthemedications.
Four months afterthe initial consultation, the patient noticedaworseninginthefrequencyandintensityof rota-tionaldizziness when exposedto specific sounds, such as alarmsandsirens;thedizzinessceasedassoonasthesound triggeringitwasinterrupted.Sixmonthsafterthecondition onset,shealsonoticed earfullnessinthe leftear associ-atedwithahissing-typetinnitus,inadditiontodifficultyin understandingsoundsinthatear.
These symptoms (ear fullness, tinnitus and alterations of comprehension) showed fluctuation, with moments of worseningandspontaneousimprovement;inthemoments ofhearingworsening, shealsonoticedrotationaldizziness worsening. Considering the worsening of the symptoms, the patient was evaluated by new serial audiometries,
which showed fluctuationof auditory thresholds compati-blewithclinicalworsening. Shethenunderwentan MRIof thetemporalbones,whichdisclosedaleftvestibularlesion (Fig.3).
Whensheunderwentvestibularfunctionexaminationby vestibulo-ocular reflexdetection throughthe hadimpulse test,sheshowedanormalvestibular-ocularreflexinallright semicircularcanalsassessed.Ontheotherhand,regarding the left canals, there was a decreased vestibulo-ocular reflexgaininthelateralandanteriorcanals,withcovered anduncoveredcorrectivesaccades;however,the vestibulo-ocular reflex gain of the left posterior canal was normal (Fig.4).Basedonthisexamination,vestibularhypofunction wasidentifiedintheleftsuperiorvestibularnerve topogra-phy.
Becauseit wasa millimetric lesion, withlittle impact fromtheauditorypointofview,itwasdecidedtofollowthe patientbyrepeatingtheMRIandtheaudiometryannually (Fig.5).
Inthethirdyearof follow-up,thepatientshowed sud-den hearingloss inthe leftear,without worseningof the vestibularcomplaints. Anewaudiometryshowedprofound hearingloss inthe leftear,compatiblewiththediagnosis of sudden sensorineural hearing loss, or sudden deafness (Fig.5).
At this time, treatment with oral prednisolone
A
B C
RE
RE RE
250 -10
0
10
20
30
40
50 60
70
80
90
100
110
120
dB
40 50 100
20 100
SN
WN,PN,SN WN,PN,SN
05
Masking Masking
I R F S T R
S D T Logoaudiometry
dBNA
dBNA Mono %
Tri % Di %
dBNA
dBNA
dBNA
-10
0
10
20
30
40
50 60
70
80
90
100
110
120
dB 250
500 1K 2K 4K 8K Hz 500 1K 2K 4K 8K Hz
RE
RE RE
Audiometry
Figure5 (A)Audiometryshowingmildsensorineurallossintheleftear.(B)T2-weightedMRIoftemporalbones,axialview,with
hyposignalintheleftvestibule.(C)T1-weightedMRIoftemporalbones,axialview,withcontrast,lesionshowshyperuptakeinthe
leftvestibule.
(Fig. 6). The MRI showed tumor growth of approximately 1mm in comparisonto the last examination performed 2 yearsearlier(Fig.5).Theaudiometryshowedconsiderable worseningofauditorythresholdsintheleftear(Fig.6).
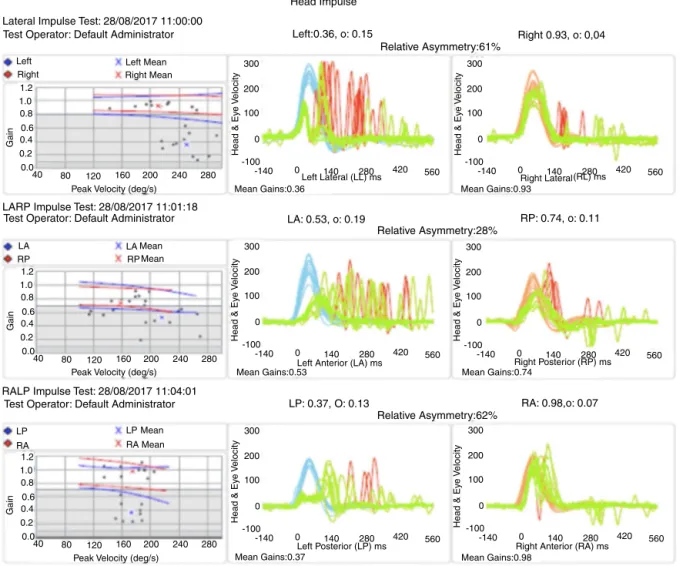
Repeatingthevestibularfunctionexaminationby detec-ting the vestibulo-ocular reflex throughthe head impulse test at that moment showed that the previously inves-tigated right semicircular canals remainednormal. There was a significant decrease in gain at the left in all assessed semicircular canals with compensatory saccades (Fig.7).
After21daysoftreatment,thepatientdidnotshowany improvementfromthepointofviewofhearingfunctionor bodybalance.Therefore,translabyrinthinesurgerywas cho-sen,asthepatienthadnohearingtobepreservedasshehad before.
Discussion
Itisstilldifficulttoestimatetherealprevalenceof
intral-abyrinthine schwannomas, due to the small number of
A
B
C
RE Audiometry LE
-10 250 500 1K 2K 4K 8K Hz 250 500 1K
2K 4K 8K Hz
0
10
20
30
40 50
60
70
80
90
100
120 110
dB
-10
0
10
20
30
40 50
60
70
80
90 100
120 110
dB
Logoaudiometry
I R F S T R
Right afferent pathway
Threshold Hz Threshold
500 1k 2k 4k
Left afferent pathway
S D T
Masking Masking
40 100
WN,PN,SN WN,PN,SN
05
SN
00 00 00 10
IPSI CONTRA IPSI CONTRA AUS
95
120
85 85 90 90
120 105 LE
LE RE
RE
Stapedial reflex
dbHL
dbHL dbHL
dbHL dbHL dbHL dbHL
dbHL Mono % Di % Tri %
dBNA
dBNP´S dBNP´S
Figure6 (A)Audiometryshowingdeepsensorineurallossintheleftear.(B)T2-weightedMRIoftemporalbones,coronalview,
withhyposignalintheleftvestibule.(C)T1-weightedMRIoftemporalbones,axialview,T1withcontrast,lesionshowshyperuptake
intheleftvestibule.
Anothertopicstilldebatedinseveralstudiesisthetumor origin. Although some studies suggest that it is not pos-sible toclearly identify the tumor origin,11 Neff et al.,12 ina reviewof 55cases (23intracochlear, 25 intravestibu-lar and7 involving the cochlea andvestibule), concluded that there seems to be no difference between the inci-denceoftumorgenesisinthecochlearnerveorvestibular nerve.
As for the clinical picture of the patients with intral-abyrinthineschwannoma,therehavebeen nostudiesthat correlatedtumorlocationwithpatientcomplaint.Moreover, studiesdescribinglong-termfollow-up,changesinthe clin-icalpictureduringtumor evolutionandtumorradiological evolutionarescarceanddocumentlimitedsamples. There-fore,ourstudyseemstobethefirstone intheliterature tocorrelate, based on a case report, the tumor subtype withthe clinical manifestations,in addition todescribing
the clinical evolution and results ofauditory and imaging testsinalong-termfollow-up.
Inourreview,themain clinicalmanifestation observed in patientswithintralabyrinthineschwannoma, regardless ofthesubtype,ishearingloss,beingusuallysensorineural, progressive, with low speech discrimination.12 It is esti-mated that 15%---32%of patients havesudden hearing loss astheinitialmanifestationofthecondition,withrarecases of hearing loss fluctuation.13,14 The second most frequent complaintisvertigo,whichmayoccursecondarytoall intral-abyrinthineschwannomasubtypes.
Head Impulse
Lateral Impulse Test: 28/08/2017 11:00:00
LARP Impulse Test: 28/08/2017 11:01:18
RALP Impulse Test: 28/08/2017 11:04:01 Test Operator: Default Administrator
Test Operator: Default Administrator
Test Operator: Default Administrator
Right 0.93, o: 0,04 Relative Asymmetry:61%
Relative Asymmetry:28%
Relative Asymmetry:62% Left:0.36, o: 0.15
Left Mean Right Mean
Peak Velocity (deg/s)
Peak Velocity (deg/s)
Peak Velocity (deg/s)
Mean Gains:0.36
Mean Gains:0.53
Mean Gains:0.37
Left Lateral (LL) ms
Head & Ey
e
V
elocity
Head & Ey
e
V
elocity
Head & Ey
e
V
elocity
Head & Ey
e
V
elocity
Head & Ey
e
V
elocity
Head & Ey
e V elocity Gain Gain Gain Right Lateral
Right Posterior (RP) ms
Left Posterior (LP) ms
LP: 0.37, O: 0.13 RA: 0.98,o: 0.07
RP: 0.74, o: 0.11 LA: 0.53, o: 0.19
Right Anterior (RA) ms Left Anterior (LA) ms
Mean Gains:0.93 Mean Gains:0.74 Mean Gains:0.98 200 100 0 -100
-140 0 140 280 420 560
300
200
100
0
-100
-140 0 140 280 420 560
300 200
100
0
-100
-140 0 140 280 420 560
300
200
100
0
-100
-140 0 140 280 420 560
300 200
100
0
-100
-140 0 140 280 420 560
300
200
100
0
-100
-140 0 140 280 420 560
300 Left Right (RL) ms LA LP LA LP RP RA RP RA Mean Mean Mean Mean 1.2 1.0 0.8 0.6 0.4 0.2 0.0
40 80 120 160 200 240 280
1.2 1.0 0.8 0.6 0.4 0.2 0.0
40 80 120 160 200 240 280
1.2 1.0 0.8 0.6 0.4 0.2 0.0
40 80 120 160 200 240 280
Figure7 Head-impulsetestshowingleftvestibularhypofunctioninallassessedsemicircularcanals.
whichwouldcausecompressionoftheadjacentstructures.15 In both cases,the tumor can also cause metabolic alter-ations in the inner earfluids, leading tohearing loss and imbalance.16
Althoughnotlimitedtoit,thecomplaintofvertigooccurs more frequently in the intravestibular schwannoma.17,18 Regardingthetreatmentofintralabyrinthineschwannomas, inmostofthecasesreportedintheselectedstudies, clini-calandserialradiologicalfollow-upwaschosen,considering the low percentage (15%) of patients that showed tumor growth withina 5-year evolution period.18 In some situa-tions,itispossibletochoosesurgicalexcisionofthetumor, withthemainindicationsbeing(1)evidenceoftumorgrowth leadingtoinvolvementofthecerebellopontineangle, inter-nal auditory meatusor middle ear;(2) totalhearing loss; (3) vestibular symptoms that do not improve with clini-caltreatment;or(4)diagnosticdoubt.1Areviewpublished by Van Abel et al.2 including 14 patients diagnosed with labyrinthineschwannomawhounderwentclinicalfollow-up, estimatedthatonly3%requiredsurgicaltreatment. Consid-ering thehighrisk ofcomplications duringthesurgeryfor thelabyrinthineschwannomaremoval(includingdeafness, dizzinessandfacialparalysis)andthelowgrowthpotential ofthesetumors,studiessuggestthattheclinicalfollow-up isbest,withsurgerybeingreservedforspecificsituationsor signsofuntreatablesymptoms.
Conclusion
The main clinical manifestation of patients with
intral-abyrinthine schwannoma is hearing loss, present in
approximately100%ofthereportedcases.19,20Themost fre-quenttypeofhearinglossisthesensorineuraltype,whichis characteristicallyprogressive; suddenor fluctuatinglosses arelessfrequent. Althoughtherearealmost 600 casesof intralabyrinthine schwannoma reported in the literature, detaileddescriptionsofthepatients’clinicalevolutionand thecorrespondingradiologicalcorrelationsarescarce.The embryologicalandpathophysiologicalmechanismsinvolved in the genesis of the tumor and its consequent auditory sequelaeareyettobecompletelyelucidated.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
2.VanAbelKM,CarlsonML,LinkMJ,NeBA,BeattyCW,LohseCM, etal.Primaryinnerearschwannomas:acaseseriesand system-aticreviewoftheliterature.Laryngoscope.2013;123:1957---66. 3.Ebmeyer J, Lautermann J, Scholtz LU, Sudhoff H.
Intral-abyrinthineschwannomas.HNO.2011;59:168---72.
4.KnippingS, Fabricius A, KöslingS, BlochingM. Intracochlear schwannoma as a cause ofa deafness: a case report.HNO. 2007;55:641---3.
5.KarlanMS,BasekM,PotterGB.Intracochlearneurilemoma.Arch Otolaryngol.1972;96:573---5.
6.MayerO.EinfallvonmultiplenTumoreninden Endausbreitun-gendesAkustikas.ZOhrenheilkd.1917:95---113.
7.Mafee MF, LachenauerCS, Kumar A, ArnoldPM,Buckingham RA, Valvassori GE. CT and MR imaging of intralabyrinthine schwannoma:reportoftwocasesandreviewoftheliterature. Radiology.1990;174:395---400.
8.Jackson LE, Hoffmann KK, Rosenberg SI. Intralabyrinthine schwannoma:subtledifferentiatingsymptomatology. Otolaryn-gologyHeadNeck.2003;129:439---40.
9.GordtsF,VanDerVekenP,TopsakalV.Apilotwithan intrav-estibular schwannoma: to fly or not to fly? Otol Neurotol. 2011;32:326---9.
10.Tieleman A, Casselman JW, Somers T. Imaging of intral-abyrinthine schwannomas: a retrospective study of 52cases withemphasison lesiongrowth.AmJNeuroradiol. 2008;29: 898---905.
11.O’KeeffeLJ,CamilleriAE,GillespieJE,CairnsA,RamsdenRT. Primarytumoursofthevestibuleandinnerear.JLaryngolOtol. 1997;111:709---14.
12.NeffBA,WillcoxTOJr,SataloffRT.Intralabyrinthine schwanno-mas.OtolNeurotol.2003;24:299---307.
13.KennedyRJ,SheltonC,SalzmanKL.Intralabyrinthine schwan-nomas: diagnosis, management, and a new classification system.OtolNeurotol.2004;25:160---7.
14.VanAbelKM,CarlsonML,LinkMJ.Primaryinnerear schwan-nomas:acaseseriesandsystematicreviewoftheliterature. Laryngoscope.2013;123:1957---66.
15.RosahlS.Acousticneuroma:treatmentorobservation?Dtsch ArzteblInt.2009;106:505---6.
16.Jiang ZY, Kutz JWJr, Roland PS, Isaacson B. Intracochlear schwannomas confined to the otic capsule. Otol Neurotol. 2011;32:1175---9.
17.GrayeliAB,FondC,KalamaridesM.Diagnosisandmanagement ofintracochlearschwannomas.OtolNeurotol.2007;28:951---7. 18.Saltzman KL, Childs AM, Davidson HC, Kennedy RJ, Shelton
C, Harnsberger HR. Intralabyrinthine schwannomas: imaging diagnosisandclassification.AJNRAmJNeuroradiol.2012;33: 104---9.
19.WeedDT,TeagueMW,StewartR.Intralabyrinthineschwannoma: acasereport.OtolaryngolHeadNeck.1994;111:137---42. 20.DeLozierHL,GacekRR,DanaST.Intralabyrinthineschwannoma.