SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Comparative
study
of
topical
vs.
intravenous
tranexamic
acid
regarding
blood
loss
in
total
knee
arthroplasty
夽
Ari
Zekcer
a,∗,
Ricardo
Del
Priori
b,
Clauber
Tieppo
c,
Ricardo
Soares
da
Silva
a,
Nilson
Roberto
Severino
daClínicaOrtopédicaTatuapé,GrupodeCirurgiadeJoelho,SãoPaulo,SP,Brazil bClínicaSantaMaria,SãoPaulo,SP,Brazil
cInstitutodeOrtopediaCampoBelo,SãoPaulo,SP,Brazil
dFaculdadedeCiênciasMédicas,SantaCasadeMisericórdiadeSãoPaulo,DepartamentodeOrtopediaeTraumatologia,SãoPaulo,SP,
Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received13August2016 Accepted20September2016 Availableonline30August2017
Keywords:
Tranexamicacid Arthroplasty
Replacementarthroplasty Knee
Fibrinmodulatingagents Antifibrinolytic
a
b
s
t
r
a
c
t
Objective:Tocomparetopicalvs.intravenoustranexamicacid(TA)intotalkneearthroplasty regardingbloodlossandtransfusion.
Methods:NinetypatientswererandomizedtoreceiveTAintravenously(20mg/kgin100mL ofsaline;groupIV),topically(1.5gin50mLofsaline,sprayedovertheoperatedsite,before releaseofthetourniquet;topicalgroup),orintravenoussaline(100mL withanesthesia; controlgroup).Thevolumeofdrainedbloodin48h,theamountoftransfusedblood,and theserumlevelsofhemoglobinandhematocritbeforeandaftersurgerywereevaluated.
Results:The groups were similar for gender, age, weight, laterality, and preoperative hemoglobinandhematocritlevels (p>0.2).Thehemoglobinlevel droppedinallgroups whencomparingthepreoperativeandthe48-hevaluations:thecontrolgroupdecreased 3.8mg/dLonaverage,whiletheIVgrouphadadecreaseof3.0,andthetopicalgroup,of3.2 (p=0.019).ThedifferencebetweenthecontrolandIVgroupswasconfirmedbyBonferroni test(p=0.020).Thedifferencebetweenthecontrolgroupandthetopicalgroupwasnot sig-nificant(p=0.130),althoughtherewaslessreductioninhemoglobininthetopicalgroup;the comparisonbetweentheIVgroupandthetopicalgroupwasalsonotsignificant(p=1.000).
Conclusion: UsingtopicandIVtranexamicaciddecreasedbloodlossandtheneedfor transfu-sionintotalkneearthroplasty.TopicalapplicationshowedresultssimilartoIVuseregarding theneedforbloodtransfusion,butwithoutthepossiblesideeffectsofIVadministration.
©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
夽
PaperdevelopedatAACD,SãoPaulo,SP,Brazil;andFaculdadedeCiênciasMédicas,SantaCasadeMisericórdiadeSãoPaulo,SãoPaulo, SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](A.Zekcer).
http://dx.doi.org/10.1016/j.rboe.2017.08.005
Estudo
comparativo
com
uso
do
ácido
tranexâmico
tópico
e
intravenoso
em
relac¸ão
à
perda
sanguínea
na
artroplastia
total
do
joelho
Palavras-chave:
Ácidotranexâmico Artroplastia
Artroplastiadesubstituic¸ão Joelho
Moduladoresdefibrina Antifibrinolíticos
r
e
s
u
m
o
Objetivo: Compararousodeácidotranexâmico(AT)tópicoeintravenosonaartroplastia totaldejoelhocomrelac¸ãoàperdadesangueenecessidadedetransfusão.
Métodos: Foramrandomizados90pacientesparareceberATporviaintravenosa(20mg/kg em100mLdesoluc¸ãosalina;grupoIV),tópico(1,5gem50mLdesoluc¸ãosalina,antes desoltarotorniquete;grupotópico)ousoluc¸ãosalinaintravenosa(100mLcomanestesia; grupocontrole).Ovolumedesanguedrenadoem48horas,aquantidadedesangue trans-fundidoeasconcentrac¸õessériasdehemoglobinaehematócritoforamavaliadosantese depoisdacirurgia.
Resultados: Osgruposeramsemelhantesquantoasexo,idade,lateralidadeeconcentrac¸ões pré-operatóriasdehemoglobinaehematócrito(p>0,2).Aconcentrac¸ãodehemoglobina diminuiuemtodososgruposquandoasavaliac¸õespré-operatóriaeem48horasforam comparadas:ogrupocontroletevereduc¸ãomédiade3,8mg/dL,enquantoogrupoIVteve diminuic¸ãode3,0eogrupotópico,de3,2(p=0,019).Adiferenc¸aentreosgruposcontrole eIVfoiconfirmadapelotestedeBonferroni(p=0,020).Adiferenc¸aentreosgrupos con-troleetópiconãofoisignificativa(p=0,130),apesardehaverumamenordiminuic¸ãoda hemoglobinanogrupotópico;acomparac¸ãoentreosgruposIVetópicotambémnãofoi significativa(p=1,000).
Conclusão: OusodeATtópicoeIVreduziuasperdassanguíneaseanecessidadede trans-fusãonaartroplastiatotaldojoelho.OusotópicomostrouresultadosemelhanteaousoIV emrelac¸ãoànecessidadedetransfusãosanguínea,porémsemospossíveisefeitoscolaterais daadministrac¸ãoIV.
©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Totalkneearthroplastyisamajororthopedicoperation involv-ing considerablelossofblood.Despite the commonuse of tourniquets,itisestimatedthatthevolumeofbloodloss dur-ingthissurgeryisbetween800and1200mL.1–5
Bleedingduringsurgicaltraumainducesactivationofthe coagulationcascade3,6andthenfibrinolysis.1,7–9Tranexamic acid,anantifibrinolytic agent,has demonstrated inhaving the abilityofreducing blood loss, but there isstill contro-versyregardingthe dosageandthe typeofadministration. Tranexamicacidinhibitsfibrinolysisbycompeting withthe lysinemolecule atfibrinogen binding sites.7,10,11 Itis used successfullyinheartsurgery,organtransplantsand gyneco-logicalsurgery,proceduresinvolvingalargeamountofblood loss.10–14 In kneearthroplasty, intravenoustranexamicacid hasbeenshowntoreducebloodlossandtheneedforblood transfusion.1,15–19However,thedosageandtypeof adminis-trationare stillcontroversial,andpossiblesideeffectssuch as nausea, headache and hypercoagulation, although rare, may occur.18,20–22 A study measuring the plasma levels of plasminogeninperipheralbloodsuggests thattheeffectof tranexamicacidisgreateratthesiteofthesurgicalwound thanintheperipheralblood.7
Wedesignedthisrandomizedcontrolledtrialtoobserveif therewasanydifferencebetweenthetopicalandintravenous administration of tranexamic acid in total knee arthro-plastyregardingthevolumeofbloodlossand theneedfor
transfusion.Thehypothesestestedherewere:(1)the blood losswouldbehigherinthecontrolgroupwhencomparedto theothers;(2)topicalandintravenousadministrationsofthe drugshouldbeequallyeffectiveinreducingbloodlossandthe needforbloodtransfusion.
Material
and
methods
Studydesignandscenario
Thisisarandomized,single-blind,simulation-controlled clin-ical study performedin alargehospital betweenJune and November 2014. The Research Ethics Committeeapproved the study protocol (number 27270814.0.0000.0085) and the patients signedthe freeandinformed consentformbefore schedulingthedateofsurgery,afterbeingfullyinformedabout theproceduresanddesignofthestudy.Thestudyisenrolled inclinicaltrials.gov(protocolregisterNCT02323373).
Participantsandsurgicaltechnique
patientwassubmittedtolateralreleaseofthepatella. Exclu-sioncriteriawere:historyor identifiedriskofdeepvenous thrombosisor pulmonary embolism or history of coagula-tionorcardiovasculardisorders;vasculardiseasesorcurrent useofanticoagulantdrugs;orthopedicsurgeryinthelower limbs.
Thesame prosthesis was used in all cases (Genesys 2, Smith&Nephew,Memphis,USA).Tourniquetswereusedin all patients. All patientsreceived intravenousbolus hydra-tion(8mL/kg)immediatelypriortosurgeryand4mL/kg/hof salineduringtheoperation.Thesameanesthesiateam par-ticipatedinallsurgeries.Thesamekneesurgeryteam,with experiencedsurgeons(thatis,therewasnoresidentsurgeon orinteamtraining)performedalltheoperations.Hemostasis wasdoneaftertourniquetreleasebeforetissueclosure.A suc-tiondrainagedevicewasinstalledandusedfor48h(3.2mm, Portovac,Zammi),thedrainedvolumewasrecordedeverysix hours.
Patients received either regional (double-block) or gen-eral (when lumbarpuncture was not possible) anesthesia. The regional anesthesia protocol included spinal anesthe-sia(4mLof0.5%bupivacaine)andplacementofanepidural catheter.Apatient-controlledanalgesiapump(PAC)allowed paincontrolfor48haftersurgery,with165mLofsaline(0.9%), fentanyl(15mL)andropivacaine (20mL,1%)with adminis-trationof4mLperhour,6mLbolus,20-minrepeatinterval, andmaximumdoseof60mLin24h.Generalanesthesiawas performed withpropofol, fentanyl and cisatracurium besi-latefortrachealintubation.Intravenousinfusionpumpswere maintainedwithpropofol andopioids. PACforintravenous analgesia includedsaline solution(0.9%, 95mL,),morphine (50mL,1–2mL/h,bolusof1mgevery15min)andamaximum doseof6mL/h.
All patients of the three groups received the same postoperative care protocol, including physiotherapy with continuous passive movement equipment (for 1h, 3times a day), withgradual increase offlexion, initiatedwith 60◦
ofkneeflexion;preventionofvenousthrombosiswith elas-ticstockingsandsodiumenoxiparin(Clexane®,Sanofi)given subcutaneouslyoncedailyfor10days.
Outcomes
Theprimaryoutcomeanalyzedinthisstudywasthevolume ofbloodlossintotalkneearthroplasty.Thiswasdetermined by the suction drain, with recording of the total volume inmilliliters,measured48hafterthe endofsurgery,when drainagesystemswereremoved.Secondaryoutcomeswere: needfortransfusion(patientreceivedtwounitsofpackedred bloodcellseverytimehemoglobinlevelswerebelow8.0g/dL). Onemonthbeforesurgeryand24and48haftersurgery,all patientsunderwenthemoglobinandhematocritserum lev-els,and thenormalizedinternationalratioand coagulation timewere calculated.Theageandsexofthepatientswere alsorecorded.Therefore,thevariablesanalyzedinthisstudy were:hemoglobin level, hematocrit, partialthromboplastin time(PTT), internationalnormalized ratio (INR),volume of bloodlossthroughtheportovacdrainandneedfor transfu-sion.
Samplesize
Weusedtheprimaryparameterstodetectthedifferencesand toassumethestandarddeviationswithvalueof˛=0.05and withpowerof80%;thesamplesizeforeachgroupwas cal-culatedtobe26(Table1).Expectingwithdrawalandexitsof about10%,wedecidedtoenroll30patientsineachgroup.
Randomization,allocationandinterventions
Randomizationwasperformedbytheanesthesiologist draw-inglotsofsealedenvelopes,previouslyplacedinacontainer with 90 similar envelopes (30 in each group) prepared in advancewithanallocationratioof1:1:1.
Each patient was allocated to one of three groups: the topical group consisted ofpatients receiving a solution of 1.5gtranexamicacid(50gmg/mL,Transamin®,ZydusNikkho) diluted in50mL saline (at 0.9%),which coveredthe entire operatedarea,andmaintainedfor5minforabsorptionbefore tourniquetrelease.Theintravenousgroupreceived20mg/kg oftranexamicaciddilutedin100mLat0.9%salinesolution, administeredwithanesthesiain10min.Finally,thecontrol consistedofpatientswhoreceivedonly100mLofsaline,also administeredatthetimeofanesthesiarunningin10min.
Statisticalanalysis
Forstatisticalanalysis,SPSSsoftwareversion13.0wasused. Significance was set at 5%. We used the t-test for the pairedanalyses,theChi-squaretestandthenon-parametric Kruskal–Wallis and Mann–Whitneytests. Wealsoused the analysis of variance (Anova) with the Bonferroni multiple comparisonsmethod.
Results
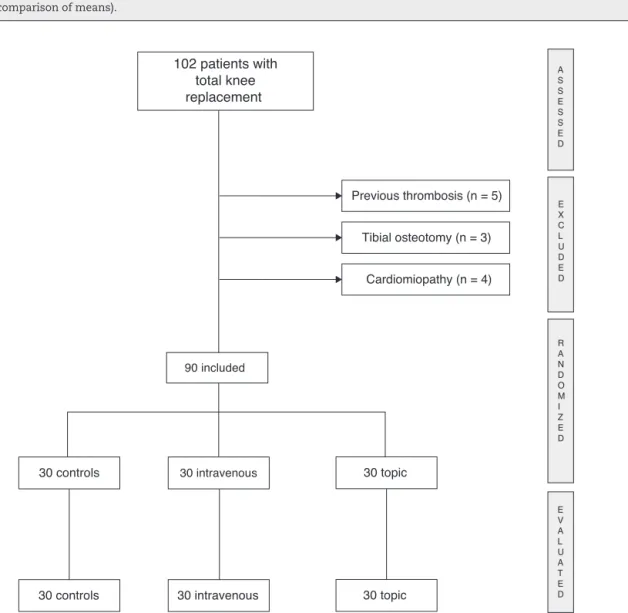
During the study period, 102 patients were invited to par-ticipate. However,we had to excludefour patients due to cardiomyopathy,fiveduetopreviouseventsof thromboem-bolism,andthreepreviouslysubmittedtotibialosteotomies (Fig. 1). Therefore, we concluded the evaluations with 90 patients,30ineachgroup.Ofthesepatients,80wereoperated with regional anesthesia (double block) and 10 with gen-eral anesthesia (duetoprevious spinearthrodesisorother anatomicalproblemsthathinderedtheperformanceofanew puncture).Therewerenosurgicalcomplications,nolesionsor sideeffects,andnopatientperishednorwherethereareany withdrawals.
Table1–Parametersforcalculatingsamplesize.
Parameters Hb Ht PTT INR
Difference 1 10 3.5 0.06
Deviation 1.2 4 6 0.10
Alpha 5% 5% 5% 5%
Testpower 80% 80% 80% 80%
Sample 14 4 26 24
Hb,hemoglobin;Ht,hematocrit;INR,normalizedinternationalratio;PTT,partialthromboplastintime. Pairtedttest(comparisonofmeans).
30 topic 30 controls
30 intravenous 30 topic
30 intravenous
R A N D O M I Z E D
90 included
Previous thrombosis (n = 5)
Cardiomiopathy (n = 4)
30 controls
102 patients with
total knee
replacement
Tibial osteotomy (n = 3)
E X C L U D E D A S S E S S E D
E V A L U A T E D
Fig.1–Flowchartforpatientenrolment.Onehundredandtwopatientswithtotalkneeprosthesiswereevaluated.
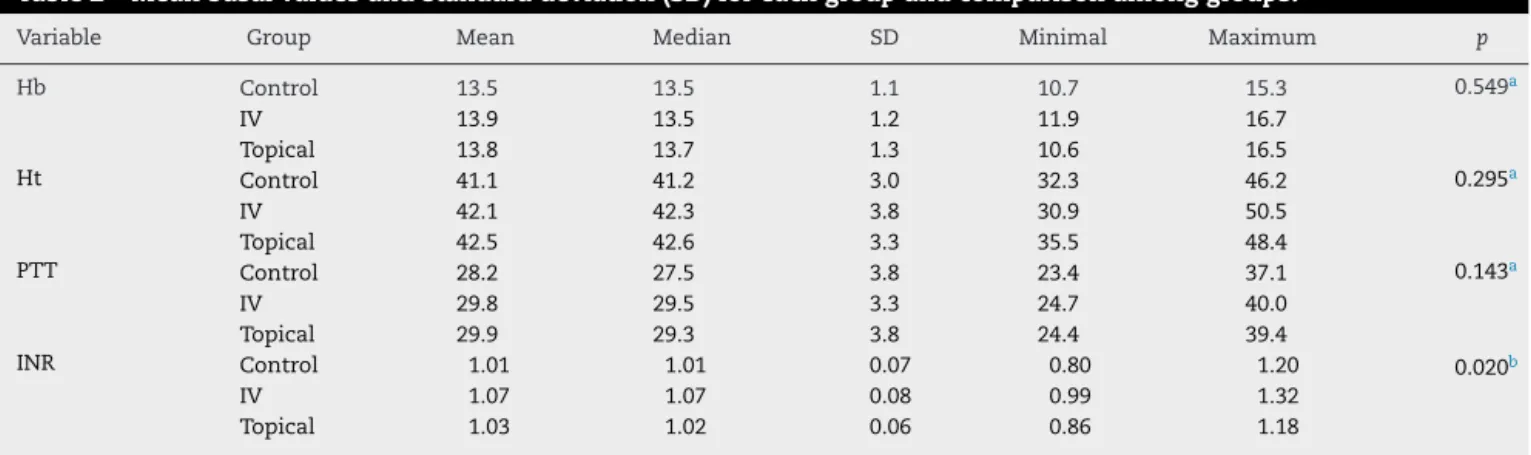
international ratio was significantly different between the controland intravenousgroups(p=0.008)and betweenthe intravenousandtopicalgroups(p=0.042),butitwassimilar incomparisontothe topicaland controlgroups (p=0.470). HematocritandPTTwerenotsignificantlydifferentbetween groups.Table2showsthemeanvaluesatthebeginningofthe studyandthestandarddeviationsineachgroup.
Hemoglobinconcentrationdecreasedinall groupswhen thepreoperativeevaluationswerecompared,andin48hours: therewasareductionof27.40%inthecontrolgroup,23.18% inthe topical group, and 22.30% inthe intravenousgroup (p=0.001 for all). The difference between the groups was
significant:thecontrolgroupdecreasedby3.8mg/dLon aver-age,whiletheintravenousgrouphadareductionof3.0andthe topicalgroup,3.2(p=0.019).AnotherBonferronicomparison showedthattherewasasignificantdifferencebetweenthe controlandintravenousgroups(p=0.020),whereastherewas nodifferencebetweencontrolandtopicalgroups(p=0.130), andintravenousandtopicalgroups(p=1.000).Fig.2showsa boxdiagramwithsuchcomparisons.
Table2–Meanbasalvaluesandstandarddeviation(SD)foreachgroupandcomparisonamonggroups.
Variable Group Mean Median SD Minimal Maximum p
Hb Control 13.5 13.5 1.1 10.7 15.3 0.549a
IV 13.9 13.5 1.2 11.9 16.7
Topical 13.8 13.7 1.3 10.6 16.5
Ht Control 41.1 41.2 3.0 32.3 46.2 0.295a
IV 42.1 42.3 3.8 30.9 50.5
Topical 42.5 42.6 3.3 35.5 48.4
PTT Control 28.2 27.5 3.8 23.4 37.1 0.143a
IV 29.8 29.5 3.3 24.7 40.0
Topical 29.9 29.3 3.8 24.4 39.4
INR Control 1.01 1.01 0.07 0.80 1.20 0.020b
IV 1.07 1.07 0.08 0.99 1.32
Topical 1.03 1.02 0.06 0.86 1.18
INR,normalizedinternationalratio;IV,intravenousgroup;Hb,hemoglobin;Ht,hematocrit;PTT,partialthromboplastintime. a Varianceanalysis–Anova.
b Kruskall–Wallistest.
Table3–Meanvolumeofblooddrainedandstandarddeviation(SD)foreachgroupandcomparisonamongthegroups (varianceanalysisandBonferronimultiplecomparisonstest).
Test Group Mean Median SD Minimal Maximum p
Anova Control 609 595 203 260 1.000 0.001
IV 421 340 246 150 990
Topical 409 400 213 70 850
Bonferroni Controlvs.IV 0.004
Controlvs.topical 0.004
IV vs.topical 1.000
IV,intravenousgroup.
18
16
14
12
10
8
6
Control IV Topic
Hb (dl/g)
Hb PRE Hb 48h
Fig.2–Graphshowsthecomparisonofhemoglobinlevels preoperatively(blueboxes)and48haftersurgery(green boxes).
1000
800
600
400
200
0
Control IV Topic
Drain (ml)
Fig.3–Graphshowingthecomparisonofdraineffective outputinthethreegroups.
intravenous groups, and between the control and topical groupswassignificant,butthedifferencebetweenthetopical andintravenousgroupswasnotsignificant.Thisisillustrated inFig.3.
Discussion
Most bleeding after total knee arthroplasty occurs after tourniquetremoval.9,23–26Despitethecontroversiesregarding postoperativeoutcomes,suchasfunctionandpain, tourni-quetsarewidelyusedintotalkneearthroplastyandactually reducebloodlossbyhalf.27Buttheystillcarryrisksofnerve damageandoptionsforreducingbloodlossarebeing investi-gated.
Weconductedarandomized,controlledstudyinaBrazilian populationstudygroupthatcomparedthetopicaland intra-venousadministrationofanantifibrinolyticagent,tranexamic acid,whichinsomestudiesisadministeredpriorto tourni-quet application to slow the onset of fibrinolysis,17 and has been shown to reduce postoperative blood loss in orthopedicsurgerywithoutthromboemboliceventsorother complications.17,28–31ThedrugwasalsostudiedintheCrash seriesofmulticenterstudieswithtraumapatients;itreduced the risk of death due to hemorrhage when administered withinthreehoursofthetrauma.17,29,32,33
In this study, we were able to confirm the hypothesis that blood loss would begreater inthe control group, not treatedwithtranexamicacid,comparedtotwoothergroups that usedthe drug. Thisfinding is consistentwith the lit-erature, confirmingthe antifibrinolyticeffectoftranexamic acid.1,15–19,30,34,35 In addition, we also confirm the second hypothesis: we haverevealed that topicaland intravenous administrationsofthedrugareequallyeffectiveinreducing bloodloss.
Thetopicaladministrationoftranexamicacid hassome advantages,themainonebeingthepossibilityofusinglower dosage.36Inaddition,itavoidstherisksassociatedwiththe systemic absorption of the medication, with the possible riskofhypercoagulation,37withtheuseonlyoflocalaction, andalsoslowstheonsetoffibrinolysis.9,21Theycanalsobe administeredbyintra-articularinjectionthrough thedrain, shortly afterclosure, withclear effects on totalblood loss and knee joint edema.38 However,our study isone ofthe firsttodirectlycompareintravenousdrugadministrationwith localadministrationintotalkneearthroplastyinaBrazilian populationgroup. Ourstudy demonstratedthat the topical dose of 1.5g was as effective as the intravenous dose of 20gmg/kgoftranexamicacidinrelationtotheneedforblood transfusion.
Maniaretal.22 conductedarandomized,controlledtrial comparing various tranexamic acid dosage schedules and included a group receiving a single local dose application of 3g/100mL saline solution in patients undergoing total kneearthroplasty.Theauthorscomparedlocalvs.intravenous administrationofthedrug,butitwasadosagestudyinwhich variousintravenousadministrationschemeswerecompared withonlyonelocaladministrationregimenanddosage.The resultofthisstudy reportedthattobeeffective,the useof IVtranexamicacidshouldbegiveninoneinitialdoseatleast duringanestheticinduction.Asinourstudy,theyfound signif-icantdifferencesbetweenlocaladministrationoftranexamic acidandcontrols.
Options for minimizing bleeding in total knee arthro-plasties are described inthe literature, amongthem: local
adrenalineuse,theuseofanavigationsystemforbonecuts and/ortheuseofhemostaticagents(Floseal®,Baxter).39
One of the limitations of our study is that it was not double-blind.Anotherlimitationwasthepreoperative evalu-ationsperformedbydifferentlaboratories,butwiththesame methodology.
Conclusions
Thisrandomizedandcontrolledclinicalstudydemonstrated thattheIVuseoftranexamicacidhadthelowestbloodloss regardingtopicalandcontrolgroups,butthetopicalusewas sufficienttoreducetheneedforbloodtransfusions,without thepossiblesideeffectsoftheIVuseinthetotalknee arthro-plasty.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.BenoniG,FredinH.Fibrinolyticinhibitionwithtranexamic
acidreducesbloodlossandbloodtransfusionafterknee
arthroplasty:aprospective,randomised,double-blindstudy
of86patients.JBoneJointSurgBr.1996;178(3):434–40.
2.CushnerFD,FriedmanRJ.Bloodlossintotalknee
arthroplasty.ClinOrthopRelatRes.1991;(269):98–101.
3.HiippalaS,StridL,WennerstrandM,ArvelaV,MäntyläS,
YlinenJ,etal.Tranexamicacid(Cyklokapron)reduces
perioperativebloodlossassociatedwithtotalknee
arthroplasty.BrJAnaesth.1995;74(5):534–7.
4.LotkePA,FaralliVJ,OrensteinEM,EckerML.Bloodlossafter
totalkneereplacement.Effectsoftourniquetreleaseand
continuouspassivemotion.JBoneJointSurgAm.
1991;73(7):1037–40.
5.SehatKR,EvansR,NewmanJH.Howmuchbloodisreallylost
intotalkneearthroplasty?Correctbloodlossmanagement
shouldtakehiddenlossintoaccount.Knee.2000;7(3):151–5.
6.ZoharE,FredmanB,EllisM,LubanI,SternA,JedeikinR.A
comparativestudyofthepostoperativeallogeneic
blood-sparingeffectoftranexamicacidversusacute
normovolemichemodilutionaftertotalkneereplacement.
AnesthAnalg.1999;89(6):1382–7.
7.BenoniG,LethagenS,FredinH.Theeffectoftranexamicacid
onlocalandplasmafibrinolysisduringtotalknee
arthroplasty.ThrombRes.1997;85(3):195–206.
8.KambayashiJ,SakonM,YokotaM,ShibaE,KawasakiT,Mori
T.Activationofcoagulationandfibrinolysisduringsurgery,
analyzedbymolecularmarkers.ThrombRes.
1990;60(2):157–67.
9.PetäjäJ,MyllynenP,MyllyläG,VahteraE.Fibrinolysisafter
applicationofapneumatictourniquet.ActaChirScand.
1987;153(11–12):647–51.
10.DunnCJ,GoaKL.Tranexamicacid:areviewofitsusein
surgeryandotherindications.Drugs.1999;57(6):1005–32.
11.EubanksJD.Antifibrinolyticsinmajororthopaedicsurgery.J
AmAcadOrthopSurg.2010;18(3):132–8.
12.MonganPD,BrownRS,ThwaitesBK.Tranexamicacidand
aprotininreducepostoperativebleedingandtransfusions
duringprimarycoronaryrevascularization.AnesthAnalg.
13.BoylanJF,KlinckJR,SandlerAN,ArellanoR,GreigPD,
NierenbergH,etal.Tranexamicacidreducesbloodloss,
transfusionrequirements,andcoagulationfactorusein
primaryorthotopiclivertransplantation.Anesthesiology.
1996;85(5):1043–8,discussion30A–31A.
14.WellingtonK,WagstaffAJ.Tranexamicacid:areviewofits
useinthemanagementofmenorrhagia.Drugs.
2003;63(13):1417–33.
15.CamarasaMA,OlléG,Serra-PratM,MartinA,SánchezM,
RicósP,etal.Efficacyofaminocaproic,tranexamicacidsin
thecontrolofbleedingduringtotalkneereplacement:a
randomizedclinicaltrial.BrJAnaesth.2006;96(5):576–82.
16.GoodL,PetersonE,LisanderB.Tranexamicaciddecreases
externalbloodlossbutnothiddenbloodlossintotalknee
replacement.BrJAnaesth.2003;90(5):596–9.
17.JansenAJ,AndreicaS,ClaeysM,D’HaeseJ,CamuF,Jochmans
K.Useoftranexamicacidforaneffectivebloodconservation
strategyaftertotalkneearthroplasty.BrJAnaesth.
1999;83(4):596–601.
18.TanakaN,SakahashiH,SatoE,HiroseK,IshimaT,IshiiS.
Timingoftheadministrationoftranexamicacidfor
maximumreductioninbloodlossinarthroplastyoftheknee.
JBoneJointSurgBr.2001;83(5):702–5.
19.RalleyFE,BertaD,BinnsV,HowardJ,NaudieDD.One
intraoperativedoseoftranexamicAcidforpatientshaving
primaryhiporkneearthroplasty.ClinOrthopRelatRes.
2010;468(7):1905–11.
20.EngelJM,HohausT,RuwoldtR,MengesT,JürgensenI,
HempelmannG.Regionalhemostaticstatusandblood
requirementsaftertotalkneearthroplastywithandwithout
tranexamicacidoraprotinin.AnesthAnalg.2001;92(3):775–80.
21.WongJ,AbrishamiA,ElBeheiryH,MahomedNN,Roderick
DaveyJ,GandhiR,etal.Topicalapplicationoftranexamic
acidreducespostoperativebloodlossintotalknee
arthroplasty:arandomized,controlledtrial.JBoneJointSurg
Am.2010;92(15):2503–13.
22.ManiarRN,KumarG,SinghiT,NayakRM,ManiarPR.Most
effectiveregimenoftranexamicacidinkneearthroplasty:a
prospectiverandomizedcontrolledstudyin240patients.Clin
OrthopRelatRes.2012;470(9):2605–12.
23.FahmyNR,PatelDG.Hemostaticchangesandpostoperative
deep-veinthrombosisassociatedwithuseofapneumatic
tourniquet.JBoneJointSurgAm.1981;63(3):461–5.
24.KlenermanL,ChakrabartiR,MackieI,BrozovicM,StirlingY.
Changesinhaemostaticsystemafterapplicationofa
tourniquet.Lancet.1977;1(8019):970–2.
25.NakaharaM,SakahashiH.Effectofapplicationofa
tourniquetonbleedingfactorsindogs.JBoneJointSurgAm.
1967;49(7):1345–51.
26.TsumaraN,YoshiyaS,ChinT,ShibaR,KohsoK,DoitaM.A
prospectivecomparisonofclampingthedrainor
post-operativesalvageofbloodinreducingbloodlossafter
totalkneearthroplasty.JBoneJointSurgBr.2006;88(1):
49–53.
27.EjazA,LaursenAC,KappelA,LaursenMB,JakobsenT,
RasmussenS,etal.Fasterrecoverywithouttheuseofa
tourniquetintotalkneearthroplasty.ActaOrthop.
2014;85(4):422–6.
28.WangQ,LiuJ,FanR,ChenY,YuH,BiY,etal.Tranexamicacid
reducespostoperativebloodlossofdegenerativelumbar
instabilitywithstenosisinposteriorapproachlumbar
surgery:arandomizedcontrolledtrial.EurSpineJ.
2013;22(9):2035–8.
29.RobertsI,PerelP,Prieto-MerinoD,ShakurH,CoatsT,HuntBJ,
etal.Effectoftranexamicacidonmortalityinpatientswith
traumaticbleeding:prespecifiedanalysisofdatafrom
randomisedcontrolledtrial.BMJ.2012;345:e5839.
30.CharoencholvanichK,SiriwattanasakulP.Tranexamicacid
reducesbloodlossandbloodtransfusionafterTKA:a
prospectiverandomizedcontrolledtrial.ClinOrthopRelat
Res.2011;469(10):2874–80.
31.LinPC,HsuCH,ChenWS,WangJW.Doestranexamicacid
savebloodinminimallyinvasivetotalkneearthroplasty?Clin
OrthopRelatRes.2011;469(7):1995–2002.
32.RobertsI,ShakurH,CoatsT,HuntB,BalogunE,BarnetsonL,
etal.TheCRASH-2trial:arandomisedcontrolledtrialand
economicevaluationoftheeffectsoftranexamicacidon
death,vascularocclusiveeventsandtransfusionrequirement
inbleedingtraumapatients.HealthTechnolAssess.
2013;17(10):1–79.
33.KerK,KiriyaJ,PerelP,EdwardsP,ShakurH,RobertsI.
Avoidablemortalityfromgivingtranexamicacidtobleeding
traumapatients:anestimationbasedonWHOmortality
data,asystematicliteraturereviewanddatafromthe
CRASH-2trial.BMCEmergMed.2012;12:3.
34.SinghJ,BallalMS,MitchellP,DennPG.Effectsoftranexamic
acidonbloodlossduringtotalhiparthroplasty.JOrthopSurg
(HongKong).2010;18(3):282–6.
35.HynesMC,CalderP,RosenfeldP,ScottG.Theuseof
tranexamicacidtoreducebloodlossduringtotalhip
arthroplasty:anobservationalstudy.AnnRCollSurgEngl.
2005;87(2):99–101.
36.Sa-NgasoongsongP,WongsakS,ChanplakornP,Woratanarat
P,WechmongkolgornS,WibulpolprasertB,etal.Efficacyof
low-doseintra-articulartranexamicacidintotalknee
replacement;aprospectivetriple-blindedrandomized
controlledtrial.BMCMusculoskeletDisord.2013;14:340.
37.ZuffereyPJ,MiquetM,QuenetS,MartinP,AdamP,Albaladejo
P,etal.Tranexamicacidinhipfracturesurgery:arandomized
controlledtrial.BrJAnaesth.2010;104(1):23–30.
38.IshidaK,TsumuraN,KitagawaA,HamamuraS,FukudaK,
DogakiY,etal.Intra-articularinjectionoftranexamicacid
reducesnotonlybloodlossbutalsokneejointswellingafter
totalkneearthroplasty.IntOrthop.2011;35(11):1639–45.
39.HelitoCP,GobbiRG,CastrillonLM,HinkelBB,PécoraJR,
CamanhoGL.ComparisonofFloseal®andelectrocauteryin
hemostasisaftertotalkneearthroplasty.ActaOrtopBras.