NASOPHARYNGEAL COLONI ZATI ON W I TH METHI CI LLI N- RESI STANT STAPHYLOCOCCUS
AUREUS AND MORTALI TY AMONG PATI ENTS I N AN I NTENSI VE CARE UNI T
Cr ist ian e Rav agn an i For t aleza1 Edson Car v alho de Melo2 Car los Magno Cast elo Br anco For t aleza3
For t aleza CR, Melo EC, For t aleza CMCB. Nasophar y ngeal colonizat ion w it h m et hicillin- r esist ant st aphy lococcus au r eu s an d m or t alit y am on g pat ien t s in an in t en siv e car e u n it . Rev Lat in am En fer m agem 2 0 0 9 set em br o-out ubr o; 1 7 ( 5 ) : 6 7 7 - 8 2 .
Nasophar y ngeal colonizat ion w it h Met hicillin- r esist ant St aphy lococcus aur eus ( MRSA) is com m on in cr it ically ill pat ient s, but it s effect on pat ient pr ognosis is not fully elucidat ed. A r et r ospect ive cohor t st udy w as car r ied out enr olling 122 pat ient s fr om an int ensiv e car e unit w ho w er e scr eened w eek ly for nasophar y ngeal colonizat ion w it h MRSA. Th e ou t com es of in t er est w er e: gen er al m or t alit y an d m or t alit y by in f ect ion . Sev er al ex posu r e v ar iables ( sev er it y of illness, pr ocedur es, int er cur r ences and MRSA nasophar y ngeal colonizat ion) w er e analy zed t hr ough univar iat e and m ult ivar iable m odels. Fact or s significant ly associat ed w it h m or t alit y in gener al or due t o infect ion w er e: APACHE I I and lung disease. The per for m ance of sur ger y pr edict ed fav or able out com es. MRSA colonizat ion did not pr edict m or t alit y in gener al ( OR= 1.02; 95% CI = 0.35- 3.00; p= 0.97) or by infect ious causes ( OR= 0.96; 95% CI = 0.33- 2.89; p= 0.96) . The r esult s suggest t hat , in t he absence of sev er it y of illness fact or s, colonizat ion w it h MRSA is not associat ed w it h unfav or able out com es.
DESCRI PTORS: St aphy lococcus aur eus; int ensiv e car e unit s; m or t alit y
COLON I ZACI ÓN N ASAL POR EL STAPHYLOCOCCUS AUREUS RESI STEN TE A LA
METI CI LI NA Y MORTALI DAD EN PACI ENTES DE UNA UNI DAD DE TERAPI A I NTENSI VA
La colonización nasofar íngea por el St aphylococcus aur eus r esist ent e a la m et icilina ( Met hicillin- r esist ant S.aur eus - MRSA) es com ún en pacient es cr ít icam ent e enfer m os, per o su efect o sobr e el pr onóst ico no est á com plet am ent e esclar ecido. Fu e r ealizado u n est u dio de Coh or t e r et r ospect iv o con 1 2 2 pacien t es de u n a Un idad de Ter apia I n t en siv a q u e r ealiza sem an alm en t e ex ám en es p ar a con st at ar la colon ización n asof ar ín g ea p or MRSA. Lo en con t r ad o d e in t er és f u e: m or t alid ad g en er al y m or t alid ad p or cau sas in f ecciosas. Div er sas v ar iab les d e ex posición ( gr av edad, pr ocedim ien t os ocu r r en cias y colon ización n asof ar ín gea por MRSA) f u er an an alizadas en m odelos univ ar iados y m ult iv ar iados. Los fact or es asociados significat iv am ent e a la m or t alidad en gener al o por causas infecciosas fuer an: APACHE I I y enfer m edad pulm onar . La r ealización de cir ugía pr edij o m ej or el pr onóst ico. La colonización por MRSA no pr edij o la m or t alidad en gener al ( OR= 1.02; I C95% = 0.35- 3.00; p= 0.97) o por causas infecciosas ( OR= 0. 96; I C95% = 0. 33- 2. 89; p= 0. 96) . Los r esult ados sugier en que, en la ausencia de fact or es de gr av edad, la colonización por MRSA no se asocia al peor pr onóst ico.
DESCRI PTORES: St aphy lococcus aur eus; unidades de t er apia int ensiv a; m or t alidad
COLON I ZAÇÃO N ASAL POR STAPHYLOCOCCUS AUREUS RESI STEN TE À METI CI LI N A E
MORTALI DADE EM PACI ENTES DE UMA UNI DADE DE TERAPI A I NTENSI VA
A colonização de nasofar inge por St aphy lococcus aur eus, r esist ent e à m et icilina ( Met hicillin- r esist ant S. aur eus - MRSA) , é com u m em pacien t es cr it icam en t e doen t es, m as seu sign if icado pr ogn óst ico n ão é in t eir am en t e conhecido. Realizou- se est udo de coor t e r et r ospect iv o com 122 pacient es de um a unidade de t er apia int ensiv a qu e r ealizar am t r iagem sem an al par a colon ização por MRSA. Os desf ech os de in t er esse f or am : m or t alidade ger al e m or t alidade por infecção. Div er sas v ar iáv eis de ex posição ( gr av idade, pr ocedim ent os, int er cor r ências e colon ização n asof ar ín g ea p or MRSA) f or am an alisad as em m od elos u n iv ar iad os e m u lt iv ar iad os. Fat or es sign if icat iv am en t e associados à m or t alidade ger al ou por in f ecção f or am : APACHE I I e doen ça pu lm on ar . A colonização por MRSA não foi pr edit or a de m or t alidade ger al ( OR= 1,02; I C95% = 0,35- 3; p= 0,97) ou por infecção ( OR= 0 , 9 6 ; I C9 5 % = 0 , 3 3 - 2 , 8 9 ; p= 0 , 9 6 ) . Os r esult ados suger em que, na ausência de fat or es de gr av idade, a colonização por MRSA não car act er iza pior pr ognóst ico.
DESCRI TORES: St aphy lococcus aur eus; unidades de t er apia int ensiv a; m or t alidade
Faculdade de Medicina de Bot ucat u, Univer sidade Est adual Paulist a “ Júlio de Mesquit a Filho”, Brazil: 1RN, e- m ail: cr ysravagnani@bol.com .br ; 2Phy sician, Hospit al Est adual de Baur u, Mast er ’s St udent , e- m ail: edcar @uol.com .br ; 3Ph.D., Assist ant Pr ofessor, e- m ail: cm for t aleza@uol.com .br.
I NTRODUCTI ON
H
o s p i t a l - a c q u i r e d i n f e c t i o n s ( H A I ) a r e a m o n g t h e m a i n a d v e r se o ccu r r e n ce s r e l a t e d t ot h e car e of p at ien t s in I n t en siv e Car e Un it s ( I CUs)( 1 ).
A p r e d o m i n a n c e o f m u l t i d r u g - r e s i s t a n t ( M D R)
m icr oor g an ism s h as b een sh ow n in t h e et iolog y of
t h e se i n f e ct i o n s( 2 ) i n se v e r a l co u n t r i e s, i n cl u d i n g
Br a zi l . MD R m i cr o o r g a n i sm s a r e d ef i n ed a s t h o se
t h a t a r e r e s i s t a n t t o o n e o r m o r e c l a s s e s o f
an t im icr ob ials r ou t in ely u sed in t h eir t r eat m en t s( 3 ).
Th e m e t h i c i l l i n - r e s i s t a n t s t a p h y l o c o c c u s a u r e u s
( MRSA) st a n d s o u t a m o n g t h e m . Th i s b a ct e r i u m
w a s f i r s t d e s c r i b e d i n Eu r o p e i n 1 9 6 1 a n d w a s
g l o b a l l y d i s s e m i n a t e d i n f o l l o w i n g d e c a d e s( 4 ).
St r a i n s o f MRSA a r e r e si st a n t t o a l l b e t a - l a ct a m
d r u g s ( p e n i c i l l i n s , c e p h a l o s p o r i n s a n d
c a r b a p e n e m s ) a n d s e v e r a l o t h e r c l a s s e s o f
a n t i m i cr o b i a l s ( cl i n d a m y ci n , q u i n o l o n es)( 5 ).
Dat a fr om t he Nat ional Nosocom ial I nfect ion
Su r v e i l l a n ce Sy st e m ( NNI S) i n t h e Un i t e d St a t e s
r eveal t hat MRSA cor r esponded t o 59.5% of S.aureus
st rains isolat ed fr om I CUs( 6). Brazilian dat a point t o a
sim ilar scen ar io. A r ep or t f r om t h e Ep id em iolog ical
Su r v eillan ce Cen t er of t h e st at e of Sao Pau lo h as
i d e n t i f i e d S. a u r e u s a s t h e se co n d m o st f r e q u e n t
bact er ium found in blood cult ur es collect ed in I CUs,
cor r esp on d in g t o 2 6 . 7 % of p osit iv e ex am s; am on g
t he isolat ed st r ains, 58.8% w er e MRSA( 7).
N a s o p h a r y n g e a l c o l o n i z a t i o n g e n e r a l l y
p r eced es t h e em er g en ce of in f ect ion b y MRSA. I n
addit ion, colonized pat ient s can spr ead t his agent in
I CU s , c o n t r i b u t i n g t o i n c r e a s e d m o r b i d i t y a n d
m o r t a l i t y( 8 ). Th e i d e n t i f i c a t i o n a n d i s o l a t i o n o f
in d iv id u als in f ect ed b y MRSA, ev en w h en t h ese d o
n ot p r esen t sig n s of act iv e in f ect ion , con t r ib u t e t o
r e d u ce t h e ci r cu l a t i o n o f t h i s a g e n t a n d a l so i t s
par t icipat ion in t he HAI et iology. A com m on pr act ice
u s e d t o i d e n t i f y c o l o n i z e d i n d i v i d u a l s i s t h e
p er f o r m an ce o f “ act i v e su r v ei l l an ce cu l t u r es”( 9 ), a
p e r i o d i c co l l e ct i o n o f cu l t u r e s o f n a so p h a r y n g e a l
secr et ion s u sin g sw abs.
A l t h o u g h t h e e p i d e m i o l o g i c a l u t i l i t y o f
sur v eillance cult ur es has been pr ov en, t he im pact of
nasal colonizat ion in pat ient s’ prognosis has not been
est ablished( 9). This st udy ’s obj ect iv e w as t w ofold: t o
a n a l y z e t h e e f f e c t o f MRSA c o l o n i z a t i o n o n t h e
pr ogn osis of pat ien t s h ospit alized in I n t en siv e Car e
Unit s and t o ident ify ot her pr edict or s of m or t alit y for
t he pat ient s of t his st udy.
METHOD
St udy sit e
Th i s st u d y w a s ca r r i e d o u t i n t h e Ad u l t s’
I nt ensive Car e Unit ( AI CU) of t he Baur u St at e Hospit al
( BSH) . This is a t eaching hospit al link ed t o Bot ucat u
S c h o o l o f Me d i c i n e , S a o Pa u l o S t a t e Un i v e r s i t y
( UNESP) . The hospit al cur r ent ly has 280 beds in use
and four I CUs. The AI CU has 11 beds and car es for
m edical and sur gical pat ient s.
St u dy Design
This is a ret rospect ive cohort st udy, enrolling
122 pat ient s adm it t ed t o t he AI CU bet ween May 2005
an d Mar ch 2 0 0 6 . Th ese pat ien t s w er e scr een ed f or
MRSA t hr ough sur v eillance cult ur es ( nasophar y ngeal
swabs) at t he t im e of t heir adm ission and weekly during
t h eir h osp it alizat ion . Pr oced u r es f or m icr ob iolog ical
analysis and ant im icr obial suscept ibilit y t est s follow ed
st an d ar d s r eco m m en d ed b y t h e l i t er at u r e( 1 0 ). Tw o
out com es w er e consider ed: ( 1) deat h and ( 2) deat h
caused by or relat ed t o infect ion.
Th e f o l l o w i n g v a r i a b l es w er e st u d i ed : ( 1 )
dem ogr aphic dat a; ( 2) com or bidit ies and sev er it y of
i l l n e s s a t t h e t i m e o f a d m i s s i o n ; ( 3 ) i n v a s i v e
p r o ced u r es, d ev i ces a n d u se o f i m u n o ssu p r essi v e
m edicat ion; ( 4) HAI diagnosis; ( 5) MRSA colonizat ion.
These dat a w er e ev aluat ed in r elat ion t o t he ov er all
chance of dy ing ( St udy 1 ) and t o deat h caused by /
r elat ed t o infect ion ( St udy 2) . The sever it y of pat ient s’
condit ions w as det er m ined by scor es obt ained in t he
Acu t e Ph y siolog y an d Ch r on ic Healt h Ev alu at ion I I
( APACHE I I ) , com put ed at t he t im e of adm ission( 11).
Definit ions of HAI follow ed guidelines provided by t he
Cen t er s for Disease Con t r ol an d Pr ev en t ion( 1 2 ).
St at ist ical an aly sis
Data were entered in the EPI I NFO v.3.2. (©DC,
USA) a n d a n a l y ze d t h r o u g h t h e SPSS st a t i st i ca l
soft w ar e v. 1 5 . 0 (©SPSS I nc. ) .
Un iv ar iat e an aly sis
D i c h o t o m o u s v a r i a b l e s w e r e a n a l y z e d
t hr ough t he Chi- Squar e Test or Fischer ’s Ex act Test ,
w hen appr opr iat e. Age w as evaluat ed by t he St udent ’s
T-Test , w hile APACHE I I scores w ere evaluat ed t hrough
Mu lt iv ar iable an aly sis
Va r i a b l e s w e r e i n c l u d e d i n h i e r a r c h i c a l
m o d e l s o f l o g i s t i c r e g r e s s i o n . T h e o r d e r o f
i n t r o d u ct i o n w a s: 1st g r o u p – d e m o g r a p h i c d a t a ;
2n d g r ou p – com or b id it ies an d sev er it y of illn ess at
t h e t i m e o f a d m i s s i o n ; 3r d g r o u p – i n v a s i v e
p r oced u r es, u se of d ev ices an d im m u n osu p p r essiv e
m ed icat ion ; 4t h g r ou p – HAI d iag n osis. A sig n if ican ce
lev el of 0 . 0 5 w as r eq u ir ed f or v ar iab les t o b e k ep t
in t h e m od els. How ev er, b ecau se MSRA colon izat ion
w as t h e var iab le of p r im ar y in t er est in t h is st u d y,
it w as f or ced in t o all m od els, ev en w h en it d id n ot
r each t h e r eq u ir ed st at ist ical sig n if ican ce. Th e lim it
u sed t o d ef in e sig n if ican ce in t h e f in al m od el w as
0 . 0 5 .
Et h ical aspect s
Th i s s t u d y w a s a p p r o v e d b y t h e Et h i c s
Com m it t ee for Resear ch w it h hum an subj ect s and is
included in t he proj ect : Risk fact ors for t he acquisit ion
of isolat ed m ult ir esist ant St aphy lococcus aur eus an d
Pseu d om on as aer u g in osa i n p at i en t s at t h e Bau r u
St at e Hospit al.
RESULTS
MRSA co l o n i za t i o n w a s d e t e ct e d t h r o u g h
sur v eillance cult ur es in t hir t y of t he st udied pat ient s.
Mor t alit y in t he follow ed cohor t w as high: 94 deat hs
( 7 7 % ) , 6 7 of w h ich w er e r elat ed t o or cau sed b y
h ospit al- acqu ir ed in f ect ion .
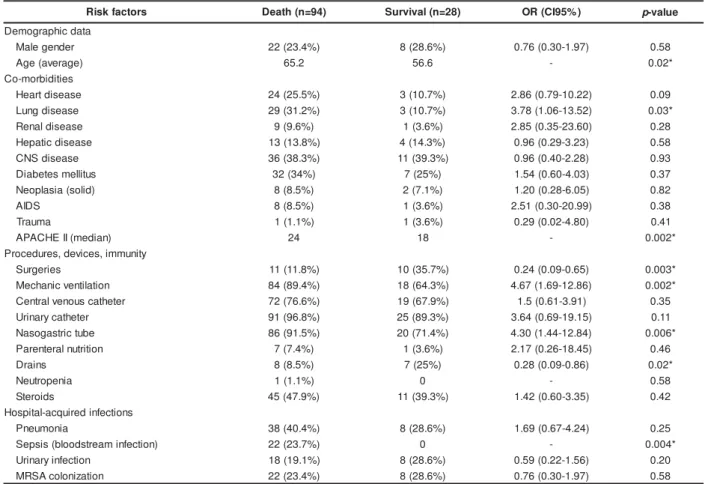
I n St udy 1, w hich inv est igat ed pr edict or s for
g e n e r a l m o r t a l i t y, u n i v a r i a t e a n a l y s i s ( Ta b l e 1 )
iden t ified age, lu n g disease, APACHE I I , m ech an ical
v en t ilat ion , t h e p r esen ce of n asog ast r ic t u b es an d
diagnosis of sepsis as risk fact ors for deat h. Surgeries
and dr ains, on t he ot her hand, w er e associat ed w it h
a bet t er prognosis. I n t he m ult ivariable analysis ( Table
3) , only APACHE I I and lung disease w er e im plicat ed
i n a h i g h e r d e a t h r i s k . Th e p r a c t i c e o f s u r g e r y
present ed a negat ive associat ion w it h m ort alit y. MSRA
colonizat ion w as not associat ed w it h a w or se out com e
( OR= 0. 76; CI 95% = 0. 30- 1, 97; p= 0, 58) .
Table 1 – Mor t alit y r isk fact or s in pat ient s in t he I nt ensiv e Car e Unit at t he Baur u St at e Hospit al ( univar iat e
an aly sis)
Dat a in num ber and per cent age, except w hen indicat ed * St at ist ically significant variables
OR= Odds Rat io. CNS = Cent r al Ner vous Syst em . APACHE= Acut e Physiology and Chr onic Healt h Evaluat ion ( sever it y scor ing syst em for pat ient s in I CU) . MRSA= Met hicillin- r esist ant St aphylococcus aur eus
s r o t c a f k s i
R Death(n=94) Survival(n=28) OR(CI95%) p-value
a t a d c i h p a r g o m e D r e d n e g e l a
M 22(23.4%) 8(28.6%) 0.76(0.30-1.97) 0.58 ) e g a r e v a ( e g
A 65.2 56.6 - 0.02*
s e i t i d i b r o m -o C e s a e s i d t r a e
H 24(25.5%) 3(10.7%) 2.86(0.79-10.22) 0.09 e s a e s i d g n u
L 29(31.2%) 3(10.7%) 3.78(1.06-13.52) 0.03* e s a e s i d l a n e
R 9(9.6%) 1(3.6%) 2.85(0.35-23.60) 0.28
e s a e s i d c i t a p e
H 13(13.8%) 4(14.3%) 0.96(0.29-3.23) 0.58 e s a e s i d S N
C 36(38.3%) 11(39.3%) 0.96(0.40-2.28) 0.93 s u t il l e m s e t e b a i
D 32(34%) 7(25%) 1.54(0.60-4.03) 0.37
) d il o s ( a i s a l p o e
N 8(8.5%) 2(7.1%) 1.20(0.28-6.05) 0.82
S D I
A 8(8.5%) 1(3.6%) 2.51(0.30-20.99) 0.38
a m u a r
T 1(1.1%) 1(3.6%) 0.29(0.02-4.80) 0.41
) n a i d e m ( II E H C A P
A 24 18 - 0.002*
y t i n u m m i , s e c i v e d , s e r u d e c o r P s e i r e g r u
S 11(11.8%) 10(35.7%) 0.24(0.09-0.65) 0.003* n o i t a l i t n e v c i n a h c e
M 84(89.4%) 18(64.3%) 4.67(1.69-12.86) 0.002* r e t e h t a c s u o n e v l a r t n e
C 72(76.6%) 19(67.9%) 1.5(0.61-3.91) 0.35 r e t e h t a c y r a n i r
U 91(96.8%) 25(89.3%) 3.64(0.69-19.15) 0.11 e b u t c i r t s a g o s a
N 86(91.5%) 20(71.4%) 4.30(1.44-12.84) 0.006* n o i t i r t u n l a r e t n e r a
P 7(7.4%) 1(3.6%) 2.17(0.26-18.45) 0.46
s n i a r
D 8(8.5%) 7(25%) 0.28(0.09-0.86) 0.02*
a i n e p o r t u e
N 1(1.1%) 0 - 0.58
s d i o r e t
S 45(47.9%) 11(39.3%) 1.42(0.60-3.35) 0.42 s n o i t c e f n i d e r i u q c a -l a t i p s o H a i n o m u e n
P 38(40.4%) 8(28.6%) 1.69(0.67-4.24) 0.25 ) n o i t c e f n i m a e r t s d o o l b ( s i s p e
S 22(23.7%) 0 - 0.004*
n o i t c e f n i y r a n i r
U 18(19.1%) 8(28.6%) 0.59(0.22-1.56) 0.20 n o i t a z i n o l o c A S R
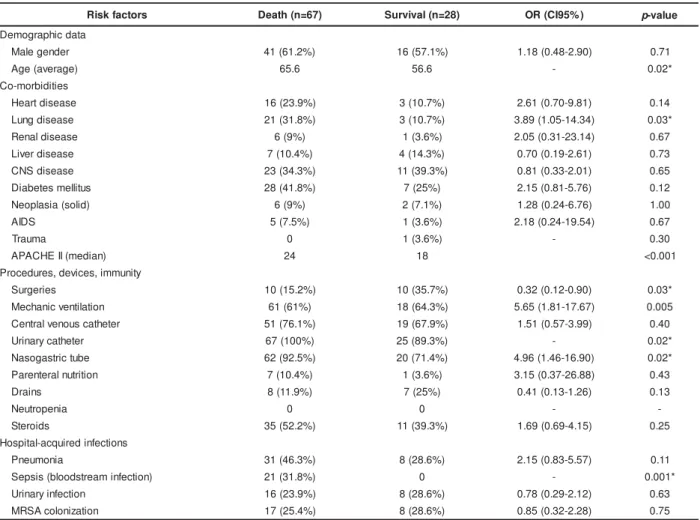
St udy 2 ( pr edict or s for m or t alit y by infect ion)
ident ified t he sam e risk fact ors found in t he univariat e
analysis car r ied out in St udy 1 ( Table 2) . I n t he st age
of m ult ivariable analysis, APACHE I I and lung disease
w er e pr edict or s of a w or se pr ognosis ( Table 3) . Once
again , MSRA colon izat ion w as n ot associat ed w it h a
higher r isk of deat h caused by or r elat ed t o infect ion
( OR= 0 . 9 6 ; CI 9 5 % = 0 . 3 3 - 2 . 8 9 ; p= 0 . 9 6 ) .
Table 2 – Mor t alit y r isk fact or s r elat ed t o or caused by hospit al- acquir ed infect ion in pat ient s in t he I nt ensive
Car e Unit at t he Baur u St at e Hospit al ( univ ar iat e analy sis)
* St at ist ically significant variables
OR= odds r at io. CNS = Cent r al Ner vous Syst em . APACHE= Acut e Physiology and Chr onic Healt h Evaluat ion ( sever it y scor ing syst em for pat ient s in I CU) MRSA= Met hicillin- r esist ant St aphylococcus aur eus
Table 3 – Mult ivariable analysis of risk fact ors relat ed
t o gener al m or t alit y and m or t alit y r elat ed t o or caused
b y h o sp i t a l - a cq u i r e d i n f e ct i o n i n p a t i e n t s i n t h e
I nt ensiv e Car e Unit at t he Baur u St at e Hospit al
s r o t c a F k s i
R OR(CI95%) p-value
y t il a t r o m l a r e n e G II E H C A P
A 1.10(1.04-1.18) 0.003
e s a e s i d g n u
L 5.72(1.37-23.93) 0.02
y r e g r u
S 0.42(0.11-0.95) 0.04
n o it a z i n o l o c A S R
M 1.02(0.35-3.00) 0.97
n o it c e f n i o t e u d y t il a t r o M II E H C A P
A 1.11(1.04-1.19) 0.002
e s a e s i d g n u
L 6.02(1.43-25.46) 0.02
n o it a z i n o l o c A S R
M 0.96(0.33-2.89) 0.96
OR= odds r at io. APACHE= Acut e Physiology and Chr onic Healt h Evaluat ion ( sever it y scor ing syst em for pat ient s in I CU) . MRSA= Met hicillin- r esist ant
St aphylococcus aur eus
DI SCUSSI ON
I nfect ion cont r ol pr act ices should be seen as
an im por t ant par t of a lar ger cont ex t : t he pr om ot ion
of qualit y and safe car e t o pat ient s( 13). That is w hy a
cr it ical ev alu at ion of r isk s r elat ed t o h ealt h car e is
e s s e n t i a l a n d a p p l i e s t o t h e c o n t r o l o f M D R
m icr oor gan ism s. Th is st u dy aim s t o con t r ibu t e t o a
b e t t e r u n d e r s t a n d i n g o f t h e r i s k s p o s e d b y t h e
acquisit ion of MRSA in cr it ical pat ient s.
Som e r ecent st udies ev aluat ed m or t alit y due
t o MSRA in hospit alized pat ient s. The m aj or it y involved
p a t i e n t s w i t h b l o o d c u l t u r e s p o s i t i v e f o r M RS A
( bact er em ia) . On e of t h ese st u dies car r ied ou t in a
s r o t c a f k s i
R Death(n=67) Survival(n=28) OR(CI95%) p-value
a t a d c i h p a r g o m e D r e d n e g e l a
M 41(61.2%) 16(57.1%) 1.18(0.48-2.90) 0.71
) e g a r e v a ( e g
A 65.6 56.6 - 0.02*
s e it i d i b r o m -o C e s a e s i d t r a e
H 16(23.9%) 3(10.7%) 2.61(0.70-9.81) 0.14
e s a e s i d g n u
L 21(31.8%) 3(10.7%) 3.89(1.05-14.34) 0.03*
e s a e s i d l a n e
R 6(9%) 1(3.6%) 2.05(0.31-23.14) 0.67
e s a e s i d r e v i
L 7(10.4%) 4(14.3%) 0.70(0.19-2.61) 0.73
e s a e s i d S N
C 23(34.3%) 11(39.3%) 0.81(0.33-2.01) 0.65
s u t il l e m s e t e b a i
D 28(41.8%) 7(25%) 2.15(0.81-5.76) 0.12
) d il o s ( a i s a l p o e
N 6(9%) 2(7.1%) 1.28(0.24-6.76) 1.00
S D I
A 5(7.5%) 1(3.6%) 2.18(0.24-19.54) 0.67
a m u a r
T 0 1(3.6%) - 0.30
) n a i d e m ( II E H C A P
A 24 18 <0.001
y t i n u m m i , s e c i v e d , s e r u d e c o r P s e i r e g r u
S 10(15.2%) 10(35.7%) 0.32(0.12-0.90) 0.03*
n o it a li t n e v c i n a h c e
M 61(61%) 18(64.3%) 5.65(1.81-17.67) 0.005
r e t e h t a c s u o n e v l a r t n e
C 51(76.1%) 19(67.9%) 1.51(0.57-3.99) 0.40
r e t e h t a c y r a n i r
U 67(100%) 25(89.3%) - 0.02*
e b u t c i r t s a g o s a
N 62(92.5%) 20(71.4%) 4.96(1.46-16.90) 0.02*
n o it i r t u n l a r e t n e r a
P 7(10.4%) 1(3.6%) 3.15(0.37-26.88) 0.43
s n i a r
D 8(11.9%) 7(25%) 0.41(0.13-1.26) 0.13
a i n e p o r t u e
N 0 0 -
-s d i o r e t
S 35(52.2%) 11(39.3%) 1.69(0.69-4.15) 0.25
s n o it c e f n i d e r i u q c a -l a t i p s o H a i n o m u e n
P 31(46.3%) 8(28.6%) 2.15(0.83-5.57) 0.11
) n o it c e f n i m a e r t s d o o l b ( s i s p e
S 21(31.8%) 0 - 0.001*
n o it c e f n i y r a n i r
U 16(23.9%) 8(28.6%) 0.78(0.29-2.12) 0.63
n o it a z i n o l o c A S R
Br a zi l i a n t ea ch i n g h o sp i t a l co m p a r ed m o r t a l i t y i n
p a t i e n t s w i t h cu l t u r e s p o si t i v e f o r MSRA a n d f o r
m et hicillin- suscept ible S. aur eus ( MSSA) . The aut hor s
concluded t hat t he r isk w as higher for pat ient s affect ed
by MRSA( 1 4 ). On e st u dy f r om t h e Un it ed St at es, on
t h e ot h er h an d , com p ar ed sim ilar g r ou p s, car ef u lly
m at ching cases accor ding t o t he sever it y of illness( 15)
and t heir r esult s did not find differ ences in m or t alit y
b e t w e e n MRSA a n d MSSA p a t i e n t s. Pa t i e n t s w i t h
MRSA, t h ou gh , w er e h ospit alized f or lon ger per iods
and incurred higher cost s for t he hospit al. Ot her st udies
a d d r e s s i n g p a t i e n t s w i t h b a c t e r e m i a o b t a i n e d
conflict ing r esult s( 16- 17).
S t u d i e s t h a t f o l l o w c o h o r t s o f p a t i e n t s
c o l o n i z e d b y M RSA a r e r a r e r. Th e f o l l o w u p o f
t r an sp l an t ed p at i en t s an d / or p at i en t s aw ai t i n g f or
h epat ic t r an splan t at ion r ev ealed t h at n asal car r iage
incr eased t he r isk of infect ion by 15 fold but had no
i m p act o n m o r t al i t y( 1 8 ). I n an o t h er st u d y, au t h o r s
f ollow ed in div idu als ch r on ically in f ect ed by MRSA( 1 9 )
an d , o f t h e 2 8 1 p er si st en t car r i er s, 9 6 p r esen t ed
infect ions and 14 died.
I n t he casuist ic of t his st udy, asy m pt om at ic
carriage of MRSA did not increase t he risk of general
m or t alit y nor of m or t alit y caused by infect ion. I nst ead,
t he usual m ort alit y predict ors in pat ient s in I CUs w ere
id en t if ied . Th e APACHE I I is a scor in g sy st em t h at
h a s t h e p r eci se f u n ct i o n o f p r ed i ct i n g d ea t h r i sk .
Ther efor e, it s st at ist ical significance is not sur pr ising.
The pr esence of lung disease incr eases t he need for
v ent ilat or y suppor t and t he r isk of hospit al- acquir ed
pneum onia. Sur gical pat ient s, on t he ot her hand, ar e
know n t o be t he gr oup w it h t he best pr ognosis( 11).
Alt hough t hese findings ar e int er est ing, t hey
should be int er pr et ed w it h caut ion. The fact t hat MRSA
colonizat ion by it self does not det er m ine deat h does
not m ean t hat infect ions by t his agent ar e associat ed
w it h a good pr ognosis. One should t ak e int o account
t h at m or t alit y in t h e st u d ied coh or t w as v er y h ig h
( 7 7 % ) . I n ot h er w or d s, MRSA colon izat ion d id n ot
in cr ease t h e r isk of deat h in a gr ou p of sev er ely ill
pat ient s. What w ould have been t he r esult s if w e had
st u d i ed i n d i v i d u al s w h o se p r i m ar y d i seases h ad a
b e t t e r p r o g n o si s? Fu r t h e r r e se a r ch i s n e e d e d t o
answ er t his quest ion.
An ot h er qu est ion ar ises. Will t h e r esu lt s of
t his st udy be used as a r at ionale against t he need for
a ct i v e su r v ei l l a n ce cu l t u r es? I t i s a f a ct t h a t t h e
collect ion of t hese cult ures increases laborat orial cost s
and t he w orkload of professionals from infect ion cont rol
com m it t ees( 8- 9). How ever, w e believe t hat a conclusive
an sw er f or t h e r eal n eed f o r su r v ei l l an ce cu l t u r es
r equ ir es clar if icat ion of ot h er f act or s. Am on g t h em ,
t he im pact of MRSA colonizat ion on t he incidence of
infect ions, pat ient s’ lengt h of st ay at t he hospit al and
hospit al cost s. This is an open field for r esear ch.
We know t hat MRSA is an im port ant agent of
HAI s in I CUs. A r igid im plem ent at ion of pr ot ocols t o
pr event HAI s, isolat ion pr ecaut ions and hand hygiene
is r ecom m ended for it s cont r ol. I nt er v ent ion st udies
h a v e s h o w n t h a t i n c r e a s e d a d h e r e n c e t o t h e s e
m easur es r educes HAI and m or t alit y r at es( 20). This is
a challenge for healt h pr ofessionals, on w hose hands
lay ( lit erally) t he responsibilit y for cont rolling infect ions.
We con clu d e t h at MRSA colon izat ion in t h e
st u d ied p op u lat ion w as n ot associat ed w it h h ig h er
m or t alit y r at es. Ot her st udies – focusing on m or bidit y
indicat or s and hospit al cost s – ar e necessar y t o bet t er
assess t he im pact of t his agent in pat ient s adm it t ed
t o I CUs.
REFERENCES
1. For st er AJ, Ky er em ant eng K, Hooper J, Shoj ania KG, v an Walr av en C. Th e im pact of adv er se ev en t s in t h e in t en siv e car e unit on hospit al m or t alit y and lengt h of st ay. BMC Healt h Ser v Res 2 0 0 8 Decem b er ; 8 ( 1 2 ) : 2 5 9 - 6 7 .
2. Rosent hal VD, Maki DG, Salom ao R, Mor eno CA, Meht a Y, Higu er a F, Cu ellar LE, Ar ik an OA, Abou qal R, Leblebicioglu H; I n t er n at ion al Nosocom ial I n f ect ion Con t r ol Con sor t iu m . Dev ice- associat ed nosocom ial infect ions in 55 int ensiv e car e u n i t s o f 8 d e v e l o p i n g co u n t r i e s. An n I n t e r n Me d 2 0 0 6 ; 1 4 5 ( 8 ) : 5 8 2 - 9 1 .
3. Siegel JD, Rhinehar t E, Jackson M, Chiar ello L, Healt hcar e I n f e c t i o n Co n t r o l Pr a c t i c e s A d v i s o r y Co m m i t t e e . Managem ent of m ult idr ug- r esist ant or ganism s in healt h car e se t t i n g s, 2 0 0 6 . Am J I n f e ct Co n t r o l 2 0 0 7 ; 3 5 ( 1 0 Su p p l
2 ) : S1 6 5 - 9 3 .
4. Kr eisw ir t h B, Kor nblum J, Ar beit RD, Eisner W, Maslow JN, McGeer A, Low DE, Novick RP. Evidence for a clonal or igin of m e t h i ci l l i n r e si st a n ce i n St a p h y l o co ccu s a u r e u s. Sci e n ce 1 9 9 3 ; 2 5 9 ( 5 0 9 2 ) : 2 2 7 - 3 0 .
5 . Ch a m b e r s H F. Th e c h a n g i n g e p i d e m i o l o g y o f St aphy lococcus aur eus? Em er g I nfect Dis 2001 Mar ch- Apr il; 7 ( 2 ) : 1 7 8 - 8 2 .
6 . Na t i o n a l No so co m i a l I n f e ct i o n s Su r v e i l l a n ce . Na t i o n a l Nosocom ial I n f ect ion s Su r v eillan ce ( NNI S) Sy st em Rep or t , dat a sum m ar y fr om Januar y 1992 t hr ough June 2004, issued O c t o b e r 2 0 0 4 . A m J I n f e c t Co n t r o l 2 0 0 4 D e c e m b e r ; 3 2 ( 8 ) : 4 7 0 - 8 5 .
( BEPA) 2 0 0 8 ; 5 ( 5 3 ) : 1 2 - 2 3 .
8. Jar vis WR. The epidem iology of colonizat ion. I nfect Cont r ol Hosp Ep id em iol 1 9 9 6 ; 1 7 ( 1 ) : 4 7 - 5 2 .
9. McGinigle KL, Gour lay ML, Buchanan I B. The use of act ive sur v eillance cult ur es in adult int ensiv e car e unit s t o r educe m e t h i c i l l i n - r e s i s t a n t S t a p h y l o c o c c u s a u r e u s - r e l a t e d m or bidit y, m or t alit y, and cost s: a sy st em at ic r eview. Clin I nfect D i s 2 0 0 8 ; 4 6 ( 1 1 ) : 1 7 1 7 - 2 5 .
1 0 . Nat ion al Com m it t ee on Clin ical Lab or at or y St an d ar d s. Per f or m an ce st an dar ds f or An t im icr obial Disk Su scept ibilit y Test s; Appr ov ed St andar d—Eight h Edit ion. NCCLS docum ent M2 - A8 . Pen n sy l v an i a ( EUA) : NCCLS; 2 0 0 3 .
1 1 . Kn a u s WA, D r a p e r EA, Wa g n e r D P, Z i m m e r m a n JE. APACHE I I : a sev er it y of disease classificat ion sy st em . Cr it Car e Med 1 9 8 5 Oct ob er ; 1 3 ( 1 0 ) : 8 1 8 - 2 9 .
1 2 . H o r a n T C, A n d r u s M , D u d e c k M A . CD C/ N H S N su r v eillan ce d ef in it ion of h ealt h car e– associat ed in f ect ion and cr it er ia for specific t y pes of infect ions in t he acut e car e set t in g. Am J I n f ect Con t r ol 2 0 0 8 Ju n e; 3 6 ( 5 ) : 3 0 9 - 3 2 . 1 3 . Lacer da RA. Pr odu ção cien t íf ica in f ecção h ospit alar e a cont r ibuição da enfer m agem : ont em , hoj e e per spect ivas. Rev Lat in o- am En f er m ag em 2 0 0 2 ; 1 0 ( 1 ) : 5 5 - 6 3 .
14. Cont er no LO, Wey SB, Cast elo A. Risk fact or s for m or t alit y in St aph y lococcu s au r eu s bact er em ia. I n f ec. Con t r ol Hosp.
Ep id em iol 1 9 9 8 ; 1 9 ( 1 ) : 3 2 - 7 .
15. Cosgr ov e SE, Qi Y, Kay e KS, Har bar t h S, Kar chm er AW, Ca r m e l i Y. T h e i m p a c t o f m e t h i c i l l i n r e s i s t a n c e i n St a p h y l o co ccu s a u r eu s b a ct er em i a o n p a t i en t o u t co m es: m or t alit y, lengt h of st ay, and hospit al char ges. I nfect Cont r ol Hosp Ep i d em i ol 2 0 0 5 ; 2 6 ( 2 ) : 1 6 6 - 7 4 .
16. Laupland KB, Ross T, Gr egson DB. St aphylococcus aur eus b l o o d st r e a m i n f e ct i o n s: r i sk f a ct o r s, o u t co m e s, a n d t h e influence of Met hicillin r esist ance in Calgar y, Canada, 2000-2 0 0 6 . J I n f ect Dis 2000-2 0 0 8 Au g u st ; 1 9 8 ( 3 ) : 3 3 6 - 4 3 .
1 7 . Wan g FD, Ch en YY, Ch en TL, Liu CY. Risk f act or s an d m or t alit y in pat ient s w it h nosocom ial St aphy lococcus aur eus bact er em ia. Am J I nfect Cont r ol 2008 Mar ch; 32( 2) : 118- 22. 1 8 . Ru ssell DL, Flood A, Z ar od a TE, Acost a C, Riley MM, Busut t il RW et al. Out com es of Colonizat ion w it h MRSA and VRE Am ong Liver Tr ansplant Candidat es and Recipient s. Am J Tr an sp lan t . 2 0 0 8 ; 8 ( 8 ) : 1 7 3 7 - 4 3 .
1 9 . Dat t a R, Hu an g SS. Risk of in fect ion an d deat h du e t o m e t h i ci l l i n - r e si st a n t St a p h y l o co ccu s a u r e u s i n l o n g - t e r m car r ier s. Clin I n f ect Dis 2 0 0 8 Au g u st ; 4 7 ( 2 ) : 1 7 6 - 8 1 . 2 0 . Mor eir a M, Fr eit as MR, Mar t in s ST, Cast elo A, Medeir os EA. Ef f i ca cy o f a p r o g r a m o f p r e v e n t i o n a n d co n t r o l f o r Met h icillin - Resist an t St aph y lococcu s au r eu s in f ect ion s in an I n t en siv e- Car e Un it . Br az J I n f ect Dis 2 0 0 7 ; 1 1 ( 1 ) : 5 7 - 6 2 .