FAMI LY MEMBERS’ NEEDS AT I NTENSI VE CARE UNI TS: COMPARATI VE ANALYSI S
BETW EEN A PUBLI C AND A PRI VATE HOSPI TAL
1Kát ia Sant ana Fr eit as2 Miak o Kim u r a3 Kar in e Azev edo São Leão Fer r eir a4
Fr eit as KS, Kim u r a M, Fer r eir a KASL. Fam ily m em ber s’ n eeds at in t en siv e car e u n it s: com par at iv e an aly sis bet w een a public and a pr iv at e hospit al. Rev Lat ino- am Enfer m agem 2007 j aneir o- fev er eir o; 15( 1) : 84- 92.
This cr oss- sect ional st udy pr oposed t o analy ze t he needs of adult I CU pat ient s’ fam ily m em ber s at a public and a pr iv at e hospit al, r egar ding t heir lev el of im por t ance and sat isfact ion. Ninet y - one fam ily m em ber s w er e int er view ed, 47 fr om t he public hospit al and 44 fr om t he pr ivat e one, using t he Br azilian adapt at ion of t he Cr it ical Car e Fam ily Need I nv ent or y ( I NEFTI ) . Ther e w as no significant differ ence bet w een t he gr oups in t he t ot al scor e of im por t ance at t r ibut ed t o t he needs ( p= 0. 410) . The sat isfact ion scor e w as higher in t he pr iv at e hospit al t han in t he public one ( p= 0.002) . Mult iple linear r egr ession analysis allow ed us t o est ablish a hier ar chy of im por t ance and sat isfact ion of t he fam ily m em ber s’ needs in each gr oup. The differ ences obser ved bet w een t he gr oups suggest t hat t he fulfillm ent of t heir needs r equir es int er v ent ions dir ect ed at t he specificit y of each t y pe of hospit al.
DESCRI PTORS: fam ily ; fam ily nur sing; needs assessm ent ; int ensiv e car e unit s
NECESI DADES DE LOS FAMI LI ARES DE PACI ENTES EN UNI DADES DE TERAPI A
I NTENSI VA: ANÁLI SI S COMPARATI VO ENTRE HOSPI TAL PÚBLI CO Y PRI VADO
Se t r at a de un est udio t r ansver sal, con obj et o de analizar y com par ar las necesidades de los fam iliar es de pacient es adult os int er nados en UTI s de un hospit al público y un pr ivado, r espect o al gr ado de im por t ancia y sat isfacción. Se les ent r evist ar on a 91 fam iliar es, 47 de la inst it ución pública y 44 de la pr ivada, ut ilizándose el I n v en t ar io de Necesidades y Est r esor es de Fam iliar es en Ter apia I n t en siv a ( I NEFTI ) . No h u bo dif er en cia significat iv a ent r e los gr upos en la punt uación t ot al de im por t ancia at r ibuida a las necesidades ( p= 0, 410) . El gr ado de sat isfacción fue m ayor en el hospit al pr ivado con r elación al público ( p= 0,002) . El análisis de r egr esión lin ear m ú lt ipla per m it ió est ablecer u n a j er ar qu ía de im por t an cia y de sat isfacción de las n ecesidades de los f am iliar es de cada gr u po. Las dif er en cias obser v adas en t r e los gr u pos su gier en qu e el at en dim ien t o de su s necesidades r equier e int er v enciones dir eccionadas a la especificidad de cada t ipo de inst it ución.
DESCRI PTORES: fam ilia; enfer m er ía de la fam ilia; ev aluación de necesidades; unidades de t er apia int ensiv a
NECESSI DADES DE FAMI LI ARES DE PACI ENTES EM UNI DADES DE TERAPI A I NTENSI VA:
ANÁLI SE COMPARATI VA ENTRE HOSPI TAL PÚBLI CO E PRI VADO
Tr at a- se de est u do t r an sv er sal qu e t ev e com o pr opost a an alisar com par at iv am en t e as n ecessidades de fam iliar es de pacient es adult os, int er nados em UTI s de hospit al público e pr iv ado, quant o ao seu gr au de im por t ância e sat isfação. For am ent r evist ados 91 fam iliar es, sendo 47 de inst it uição pública e 44 de par t icular , u t ilizan do- se o I n v en t ár io de Necessidades e Est r essor es de Fam iliar es em Ter apia I n t en siv a ( I NEFTI ) . Não houve difer ença significat iva ent r e os gr upos no escor e t ot al de im por t ância at r ibuído às necessidades ( p= 0,410) . O gr au de sat isfação foi m aior no hospit al pr iv ado ( p= 0, 002) . A análise de r egr essão linear m últ ipla per m it iu est abelecer um a hier ar quia de im por t ância e de sat isfação das necessidades dos fam iliar es de cada gr upo. As difer enças obser v adas ent r e os gr upos suger em que o at endim ent o de suas necessidades r equer int er v enções dir ecionadas à especificidade de cada t ipo de inst it uição.
DESCRI TORES: fam ília; enfer m agem fam iliar ; det er m inação de necessidades de cuidados de saúde; unidades
de t er apia int ensiv a
1 St udy ext r act ed fr om Mast er ’s Thesis; 2 RN, M.Sc., I nt ensive Therapy Specialist , e- m ail: ksfr eit [email protected] ; 3 Advisor, RN, Pr ofessor, Fr ee Lect ur er, e- m ail: m ikim [email protected] ; 4 RN, Doct oral St udent , FAPESP grant holder, e- m ail: kar [email protected], Univer sit y of São Paulo College of Nur sing
I NTRODUCTI ON
T
h e h osp it alizat ion of a f am ily m em b er in an I nt ensive Care Unit ( I CU) gener ally occur s acut elyand w it hout pr ev ious w ar ning, leav ing lit t le t im e for
fam ily adj ust m ent . I n v iew of t his st r essful sit uat ion,
r elat iv es can feel disor ganized and helpless and face
m obilizat ion difficult ies, giv ing r ise t o differ ent t y pes
of n eeds.
Fam ily m em b er s’ n eed s ar e con cep t u alized
as som et hing essent ial, requir ed by people and w hich,
w hen at t ended t o, r elieve or decr ease t heir im m ediat e
af f lict ion an d an gu ish an d im pr ov e t h eir per cept ion
of w ell- being ( 1). Most st udies on r elat iv es of cr it ical
p a t i e n t s h a v e c o n c e n t r a t e d o n d e s c r i b i n g t h e
im p or t an ce of t h eir n eed s an d t h e ex t en t t o w h ich
t hey ar e sat isfied. Nur ses w er e pioneer s in st udy ing
t his t hem e.
Th e f i r st st u d y ab o u t f am i l y n eed s i n t h e
I CU con t ex t w as p u b lish ed b y t h e Nor t h - Am er ican
n u r se Nan cy Molt er in 1 9 7 9 , an d aim ed t o id en t if y
t h e n e e d s p e r c e i v e d b y p a t i e n t s ’ r e l a t i v e s .
Th e r e f o r e , t h e a u t h o r e l a b o r a t e d a q u e st i o n n a i r e
w it h 4 5 needs it em s, scor ed accor ding t o t heir lev el
of im por t ance ( 2).
I n 1986, Jane Lesk e r eplicat ed Molt er ’ st udy
and applied t he sam e quest ionnair e, aft er a r andom
r e o r g a n i z a t i o n o f t h e i t e m s ’ s e q u e n c e . T h i s
q u e st i o n n a i r e w a s ca l l e d t h e Cr i t i ca l Ca r e Fa m i l y
Needs I nv ent or y ( CCFNI ) and consist ed of t he sam e
4 5 n e e d s , t o w h i c h f a m i l y m e m b e r s a t t r i b u t e d
d if f er en t lev els of im p or t an ce, u sin g a r isin g scale
f r o m 1 t o 4 . I n 1 9 9 1 , Le sk e u se d t h e CCFNI t o
con d u ct a st u d y of 6 7 7 r elat iv es an d , af t er f act or
analy sis, t he it em s w er e allocat ed in fiv e dim ensions:
S u p p o r t , Co m f o r t , I n f o r m a t i o n , Cl o s e n e s s a n d
Reassu r an ce ( 2 - 3 ).
Most st udies hav e used t he CCFNI eit her in
it s or iginal for m or t r anslat ed and adapt ed t o differ ent
l a n g u a g e s, co u n t r i e s a n d p o p u l a t i o n s. I n Br a zi l ,
Cast ro( 4) car r ied out t he cr oss- cult ur al adapt at ion and
v alidat ion of t he CCFNI in 1999 and used t he nam e
I n v e n t á r i o d e N e c e s s i d a d e s e Es t r e s s o r e s d e
Fam iliar es em Ter apia I nt ensiva ( I NEFTI ) . I n t his st udy,
74% of needs consider ed ver y im por t ant or im por t ant
w e r e r e l a t e d t o I n f o r m a t i o n a n d Re a s s u r a n c e .
Tw e n t y - s i x p e r c e n t o f n e e d s r e f e r r e d t o I CU
infr ast r uct ur e, or ganizat ion and funct ioning ( 4).
I n in t er n at ion al lit er at u r e, d if f er en t asp ect s
o f r e l a t i v e s ’ n e e d s a t I CU h a v e b e e n e x a m i n e d
a n d e x i s t i n g s t u d y r e s u l t s c o n t r i b u t e t o c r e a t e
a w a r e n e ss a b o u t t h e f a ct t h a t n o si n g l e h o sp i t a l
c a n i g n o r e t h e r e s p o n s i b i l i t y o f a t t e n d i n g t o
f a m i l i es’ n eed s( 5 ).
Ho sp i t a l ca r e i n Br a zi l i s q u i t e se l e ct i v e .
A c c e s s t o h o s p i t a l i z a t i o n i s c o n d i t i o n e d b y t h e
e x i s t e n c e o f t h e n e c e s s a r y r e s o u r c e s , s u c h a s
s p e c i a l i s t s , e q u i p m e n t a n d b e d a n d s e r v i c e
av ailab ilit y, an d f u n d am en t ally d ep en d s on h av in g
f i n a n c i a l r e s o u r c e s o r a h o s p i t a l i z a t i o n f u n d i n g
s y s t e m ( 6 ). H e n c e , d i f f e r e n c e s b e t w e e n t h e
s o c i o e c o n o m i c a n d c l i n i c a l c h a r a c t e r i s t i c s o f
p a t i e n t s a t t e n d e d a t p u b l i c a n d p r i v a t e h e a l t h
i n st i t u t i o n s can p r o b ab l y i n f l u en ce t h e q u al i t at i v e
a n d q u a n t i t a t i v e e x p r e s s i o n o f t h e i r r e l a t i v e s ’
n e e d s.
Th u s, t h i s st u d y a i m e d t o co m p a r a t i v e l y
an al y ze t h e n eed s o f f am i l y m em b er s o f p at i en t s
hospit alized at t he I CU of a public and a pr ivat e hospit al
a n d i d e n t i f y w h a t n e e d s m o st co n t r i b u t e d w h e n
assessin g t h eir im por t an ce an d t h e ex t en t t o w h ich
t hey w er e sat isfied.
METHODS
A cr oss- sect ional and com par at iv e st udy w as
car r ied out at t hr ee I CU in São Paulo Cit y - t w o fr om
a public and one fr om a pr iv at e hospit al. At t he public
hospit al, t he Medical Clinical I CU ( 1 1 beds) and t he
Su r g i cal I CU ( 1 4 b ed s) w er e sel ect ed i n o r d er t o
obt ain a gener al, clinical and sur gical sam ple. At t he
p r iv at e h osp it al, t h e I CU w as select ed w h er e ad u lt
pat ient s r eceiv ed clinical and sur gical t r eat m ent , w it h
1 9 beds.
Th e p r oj ect w as assessed b y t h e h osp it als’
Resear ch Et h ics Com m ission s an d appr ov ed w it h ou t
r est r ict ion s.
St u d y su b j ect s w er e t h e r elat iv es of p at ien t s
h osp it alized at t h e select ed I CU b et w een Nov em b er
2 0 0 4 a n d Fe b r u a r y 2 0 0 5 . On l y o n e r e l a t i v e w a s
i n t er v i ew ed f o r each p at i en t . Fam i l y m em b er w as
d e f i n e d a s t h a t p e r s o n i n d i c a t e d a s b e i n g t h e
c l o s e s t t o t h e p a t i e n t , w i t h o r w i t h o u t b l o o d
r elat ion s, w it h w h om t h e pat ien t w as liv in g in a close
Th e i n cl u si o n cr i t e r i a w e r e : a g e o f 1 8 o r
old er ; h av in g an ad u lt r elat iv e h osp it alized in t h e
I CU f or at least 2 4 h ou r s; h av in g v isit ed t h e p at ien t
at least on e d u r in g t h e h osp it alizat ion p er iod ; b ein g
a b l e t o u n d e r s t a n d a n d a n s w e r t h e i n s t r u m e n t
q u e s t i o n s , a n d a g r e e i n g t o p a r t i c i p a t e i n t h e
r esear ch b y sig n in g t h e Fr ee an d I n f or m ed Con sen t
Te r m .
Sam p le size w as est im at ed at 4 4 r elat iv es
f or each in st it u t ion , con sid er in g a 0 . 0 5 alp h a er r or
and a 0.20 bet a er r or.
Fo u r i n s t r u m e n t s w e r e u s e d f o r d a t a
collect ion : t h e I CU ch ar act er izat ion f or m , t o r ecor d
st r uct ur al and funct ional infor m at ion about t he unit s;
t h e p a t i e n t c h a r a c t e r i z a t i o n f o r m t o c o l l e c t
s o c i o d e m o g r a p h i c a n d c l i n i c a l d a t a ; t h e f a m i l y
m e m b e r c h a r a c t e r i z a t i o n f o r m t o r e g i s t e r
so ci oeco n o m i c, d em og r ap h i c d at a an d i n f or m at i on
abou t h is/ h er r elat ion sh ip w it h t h e pat ien t , an d t h e
I n v e n t á r i o d e N e c e s s i d a d e s e Es t r e s s o r e s d e
Fam iliar es em Ter apia I n t en siv a ( I NEFTI ) t o assess
t h e r elat iv es’ n eeds.
Th e I NEFTI is an in st r u m en t d er iv ed f r om
t h e Cr it ical Car e Fam ily Need s I nv en t or y ( CCFNI ) ,
w h ich w as ad ap t ed an d v alid at ed f or t h e Br azilian
cult ur e( 4) and assesses t he im por t ance of t he needs
of I CU pat ien t s’ f am ily m em ber s an d t h e ex t en t t o
w h ich t h ey ar e sat isf ied. Th e in st r u m en t addr esses
n e e d s r e l a t e d t o f i v e d i m e n s i o n s : I n f o r m a t i o n ,
Reassu r an ce, Closen ess, Su p p or t an d Com f or t . Th e
Por t uguese v er sion consist s of 43 it em s. I n t he abov e
m ent ioned st udy( 4), t he aut hor assessed t he int er nal
co n si st en cy o f t h e i t em s t h r o u g h t h e sp l i t - h a l v es
m et h od, an d obt ain ed Spear m an - Br ow n coef f icien t s
o f 0 . 7 4 a n d 0 . 7 7 . I n t e r n a l co n si st e n cy r e l i a b i l i t y
t h r o u g h Cr o n b a c h ’ s a l p h a c o e f f i c i e n t w a s n o t
a n a l y z e d f o r t h e c o m p l e t e i n s t r u m e n t a n d i t s
d o m a i n s.
The original scoring scale, w hich ranges from
1 t o 4, w as m odified t o a r ange fr om 0 t o 3( 4) in t he
Brazilian v er sion of t he CCFNI . I n t he pr esent st udy,
w e decided t o m aint ain t he sam e range as in original
in st r u m en t , in or d er t o f acilit at e com p ar ison s w it h
r esult s of int er nat ional st udies t hat used t he CCFNI .
The r ange fr om 1 t o 4 w as also adopt ed in anot her
Br azilian st udy ( 7).
Th e sco r e sca l e s a r e r i si n g , t h a t i s, t h e
h ig h er t h e scor e at t r ib u t ed t o t h e it em , t h e h ig h er
t h e lev el of im p or t an ce or sat isf act ion . I n t h is st u d y,
n e e d s w i t h a m e a n s c o r e > 3 w e r e d e f i n e d a s
h a v i n g t h e g r e a t e st i m p o r t a n ce a n d sa t i sf a ct i o n .
T h e s a m e c r i t e r i o n h a s b e e n a d o p t e d i n o t h e r
st u d ies ( 8 - 9 ).
Pat ient s w ho had been hospit alized for at least
24 hours w ere ident ified by consult ing t he unit s’ daily
ce n su s. Fa m i l y m e m b e r s w h o co m p l i e d w i t h t h e
inclusion crit eria w ere invit ed t o part icipat e in t his st udy
and r eceived infor m at ion about it s obj ect ives. I f t hey
agr eed, an appoint m ent w as m ade for an int er v iew ,
accor ding t o t he r elat iv e’s availabilit y. At t he st ar t of
t h e i n t e r v i e w , f a m i l y m e m b e r s w h o a g r e e d t o
p ar t icip at e sig n ed t h e Fr ee an d I n f or m ed Con sen t
Te r m .
I n t er v iew s w er e h eld in a p r iv at e locat ion ,
near or inside t he I CU, and t ook bet w een 20 and 60
m in u t es.
Descript ive st at ist ics w as used t o charact erize
pat ient s and t heir r espect ive r elat ives. Pear son’s
Chi-squar e t est w as used t o com par e cat egor ical dat a of
t h e pu blic an d pr iv at e gr ou ps, an d St u den t ’s t - t est
f or con t in u ou s an d sem i- con t in u ou s d at a. Mu lt ip le
Linear Regr ession w as used t o ident ify t he needs t hat
m ost cont r ibut ed t o t he v ar iat ion in im por t ance and
sat i sf act i o n sco r es. Dep en d en t v ar i ab l es w er e t h e
sat isfact ion and im por t ance scor es, and independent
v ar iables w er e t he needs list ed in t he I NEFTI . I t em s
t h at ap p ear ed as sig n if ican t p r ed ict or s ( p < 0 . 0 5 ) of
sa t i sf a ct i o n a n d i m p o r t a n ce i n t h e si m p l e l i n e a r
r egr ession w er e included in t he m ult iple analy sis.
Rel i ab i l i t y o f t h e I NEFTI w as assessed b y
a n a l y z i n g t h e i n t e r n a l co n si st e n cy o f i t e m s a n d
d om ain s t h r ou g h Cr on b ach ’s alp h a coef f icien t . Th e
v a l u e o f 0 . 7 0 w a s a d o p t e d a s t h e l o w e r l i m i t o f
consist ency ( 10- 11).
Dat a w er e st or ed and analy zed in St at ist ical
Pack ag e f o r t h e So ci al Sci en ces ( SPSS) so f t w ar e,
v er sion 12. 0 for Window s. A significance lev el of p£
0. 05 w as adopt ed for all analy ses.
RESULTS
Ch ar act er ist ics of pat ien t s an d r elat iv es
We st udied 91 pat ient s fr om t w o public and
char act er ist ics in t er m s of age range, gender, r eligion,
m a r i t a l s i t u a t i o n , p r e v i o u s I CU h o s p i t a l i z a t i o n
ex p er i en ce, d eat h r i sk as m easu r ed b y t h e Acu t e
Ph y s i o l o g y a n d Ch r o n i c H e a l t h Ev a l u a t i o n
-Classif icat ion Sy st em I I ( APACHE I I ) an d con d it ion
t o leav e t he I CU ( deat h or dischar ge) . Pat ient s w er e
m o s t l y w o m e n ( 5 3 . 8 % ) , c a t h o l i c ( 7 3 . 6 % ) a n d
m ar r ied ( 52. 7% ) , w it h an av er age age of 59. 6± 19. 3
y ear s; 6 8 . 1 % had been hospit alized in an I CU on a
p r ev i o u s o cca si o n ; m ed i a n d ea t h r i sk w a s 1 9 . 6 %
( 1 0 . 3 % - 3 6 . 9 % ) an d 7 9 . 1 % w er e d i sch ar g ed f r o m
t h e I CU.
We f o u n d si g n i f i ca n t d i f f e r e n ce s b e t w e e n
pat ien t gr ou ps in t er m s of edu cat ion ( p= 0 . 0 3 2 ) , w it h
m o r e p a t i e n t s w i t h a h i g h e r e d u ca t i o n d e g r e e a t
t h e p r i v a t e ( 2 5 . 6 % ) t h a n a t t h e p u b l i c h o sp i t a l
( 6 . 4 % ) ; u n it of or igin ( p= 0 . 0 2 8 ) , as m ost pat ien t s
a t t h e p u b l i c I CU ca m e f r o m t h e o p er a t i n g r o o m
( 4 6 . 8 % ) an d at t h e pr iv at e I CU f r om t h e em er gen cy
c a r e u n i t ( 5 2 . 3 % ) ; r e a s o n f o r h o s p i t a l i z a t i o n
( p = 0 . 0 1 2 ) , w it h h ig h er n u m b er s of p at ien t s in t h e
im m ed iat e p ost op er at iv e st ag e at t h e p u b lic u n it s
( 4 6 . 6 % ) , a g a i n s t p a t i e n t s w i t h c a r d i o v a s c u l a r
d i s e a s e s a t t h e p r i v a t e ( 2 5 . 0 % ) ; a n d I CU
h ospit alizat ion t im e ( p< 0 . 0 0 1 ) : at t h e pu blic h ospit al,
m ost pat ien t st ay ed at t h e I CU f or m or e t h an sev en
d ay s ( 5 5 . 1 % ) w h ile, at t h e p r iv at e, b et w een t h r ee
an d six day s ( 4 3 . 2 % ) .
We i n t er v i ew ed 9 1 r el a t i v es, 4 7 f r o m t h e
p u b lic h osp it al an d 4 4 f r om t h e p r iv at e. Bot h g r ou p s
w er e sim ilar in t er m s of ag e r an g e, g en d er, r elig ion ,
m a r i t a l s i t u a t i o n , w o r k s i t u a t i o n , p r e v i o u s
e x p e r i e n ce w i t h f a m i l y m e m b e r s h o sp i t a l i z e d a t
I CU an d k n ow l ed g e ab ou t t h e p at i en t ’s d i ag n osi s.
Al m ost al l f am i l y m em b er s w er e y ou n g er t h an 5 9
y ear s ( 8 8 % ) an d ab ou t h alf ( 4 9 . 5 % ) w er e b et w een
4 0 an d 5 9 y ear s o l d . Mo st r el at i v es w er e w o m en
( 7 4 . 7 % ) , ca t h o l i c ( 6 4 . 8 % ) a n d m a r r i ed ( 6 1 . 5 % ) ;
m or e t h an h alf p er f or m ed p aid w or k ( 5 8 . 2 % ) an d
h a d p r e v i o u s e x p e r i e n c e w i t h f a m i l y m e m b e r s
h o sp i t a l i ze d a t I CU ( 5 9 . 3 % ) , a n d m o st r e l a t i v e s
w e r e a w a r e o f t h e p a t i e n t ’ s m e d i c a l d i a g n o s i s
( 9 1 . 2 % ) .
St at ist ically sig n if ican t d if f er en ces b et w een
t he public and privat e groups w er e ident ified in t er m s
of educat ional level ( p= 0.024) , degr ee of kinship w it h
t h e p a t i e n t ( p < 0 . 0 0 1 ) , m o n t h l y f a m i l y i n c o m e
( p < 0 . 0 0 1 ) a n d k n o w i n g o f p a t i e n t ’ s p h y s i c i a n
( p= 0.014) and nur se ( 0.003) . At t he pr ivat e hospit al,
m or e fam ily m em ber s had a higher educat ion degr ee
( 5 0 % ) t h an at t h e pu blic h ospit al ( 2 5 . 5 % ) . At bot h
h ospit als, ch ildr en w er e t h e m ost pr esen t r elat iv es,
bu t m or e fr equ en t ly at t h e pr iv at e ( 6 1 . 4 % ) t h an at
t he public ( 44.7% ) ; at t he lat t er, 29.8% w er e siblings,
uncles, cousins and grandchildren w hile, at t he form er,
t hey r epr esent ed a m er e 4.5% of r elat ives; 40.9% of
r elat ives at t he pr ivat e I CU gained an incom e of m or e
t han 10 m inim um w ages, against only 10.6% at t he
public unit s; at t he pr ivat e inst it ut ion, 81.8% of fam ily
m em ber s k new t he phy sician’s nam e, against 57.4%
at t he public hospit al; only 54.5% of r elat ives at t he
pr ivat e and 23.4% at t he public I CU knew t he nur se’s
n a m e.
I NEFTI r eliabilit y an aly sis
Co n s i d e r i n g t h e i m p o r t a n c e m e a s u r e o f
needs, four of t he five CCNFI dom ains ( Reassur ance,
Cl o s e n e s s , I n f o r m a t i o n a n d Co m f o r t ) p r e s e n t e d
reliabilit y coefficient s far below accept able lim it s, w it h
Cr onbach’s alpha r anging bet w een 0.27 and 0.43. I n
t he Suppor t dom ain, an alpha of 0.62 w as found. Wit h
r espect t o sat isfact ion m easur em ent s, Closeness and
Com f or t d om ain s p r esen t ed coef f icien t s t h at eit h er
bor der ed accept able lim it s or indicat ed inconsist ency
( 0.67 and 0.47, r espect iv ely ) . When analy zed j oint ly,
r eliabilit y r at es for t he 4 3 I NFEFTI it em s w er e quit e
sat isfact or y, for t he im por t ance ( Alpha= 0.79) as w ell
as for t he sat isfact ion scale ( Alpha= 0. 86) .
I n v iew of t hese r esult s, fam ily needs w er e
a n a l y ze d b a se d o n t h e f u l l se t o f i t e m s, w i t h o u t
consider ing differ ent dom ains. Despit e t his opt ion, it
should be em phasized t hat , in t his st udy, needs w er e
i n d i v i d u a l l y n a m ed a cco r d i n g t o t h e n a t u r e o f i t s
or igin al dom ain .
Levels of im por t ance and sat isfact ion of I CU pat ient s’
fam ily needs at t he public and t he pr iv at e hospit als
I n t h e t o t a l g r o u p o f 4 3 n e e d s , f a m i l y
m em ber s at bot h inst it ut ions consider ed about 9 0 %
of t hem as im por t ant or ver y im por t ant , adopt ing t he
cr it er ion of it em s w it h a m ean scor e > 3.
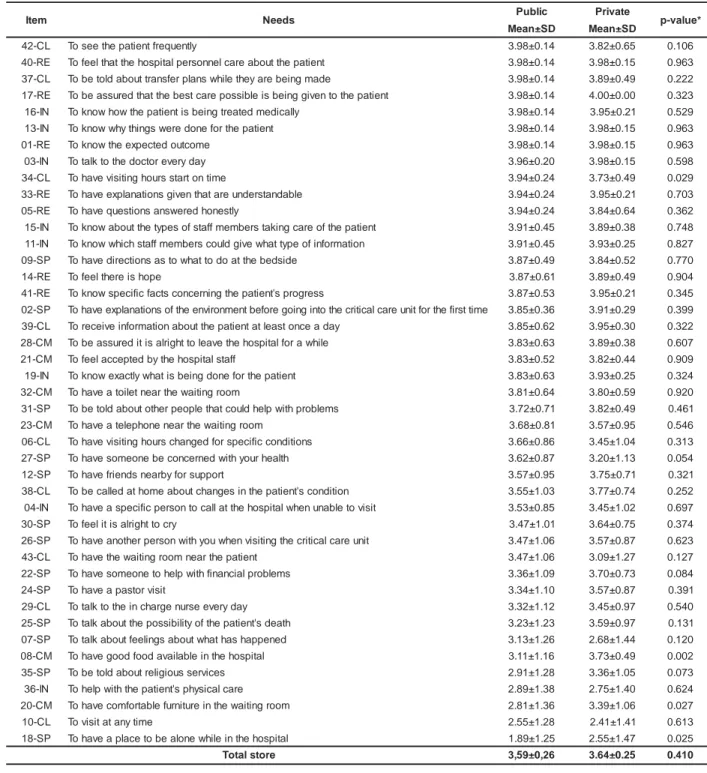
Table 1 sh ow s t h e com par ison bet w een t h e
t w o gr oups of r elat iv es in t er m s of m ean im por t ance
Table 1 - Mean values and st andar d dev iat ion of im por t ance scor es for 43 I NEFTI needs. São Paulo, SP, 2005
Obser vat ions: * St udent ’s t - t est ; RE: Reassur ance, I N: I nfor m at ion, CL: Closeness, SP: Suppor t , CM: Com for t .
Table 1 show s t hat t her e w as no significant
difference bet w een relat ives at t he public and pr ivat e
I CU in t er m s of t ot al im p or t an ce scor e ( p = 0 . 4 1 0 ) .
Th e y c o n s i d e r e d a b o u t 9 0 % o f t h e s e n e e d s a s
im por t ant or ver y im por t ant , adopt ing t he cr it er ion of
it em s w it h m ean scor e > 3.
Th e co m p ar i so n b et w een m ean sco r es f o r
each of t he it em s dem onst rat ed significant differences
b et w een b ot h g r ou p s ab ou t t h e im p or t an ce of f ou r
n eed s on ly : “ t o h av e v isit in g h ou r s st ar t on t im e”
( p = 0 . 0 2 9 ) , “ t o h a v e g o o d f o o d a v a i l a b l e i n t h e
h ospit al” ( p= 0 . 0 0 2 ) , “ t o h av e com f or t able f u r n it u r e
in t he w ait ing r oom ” ( p= 0.027) and “ t o have a place
t o be alone w hile in t he hospit al” ( p= 0. 025) . Ex cept
for t he fir st it em ( hav e v isit ing hour s st ar t on t im e) ,
w h ich r elat iv es at t h e p u b lic I CU con sid er ed m or e
i m p o r t an t , t h e t h r ee o t h er i t em s w er e co n si d er ed
m or e im por t ant by r elat ives at t he pr ivat e inst it ut ion.
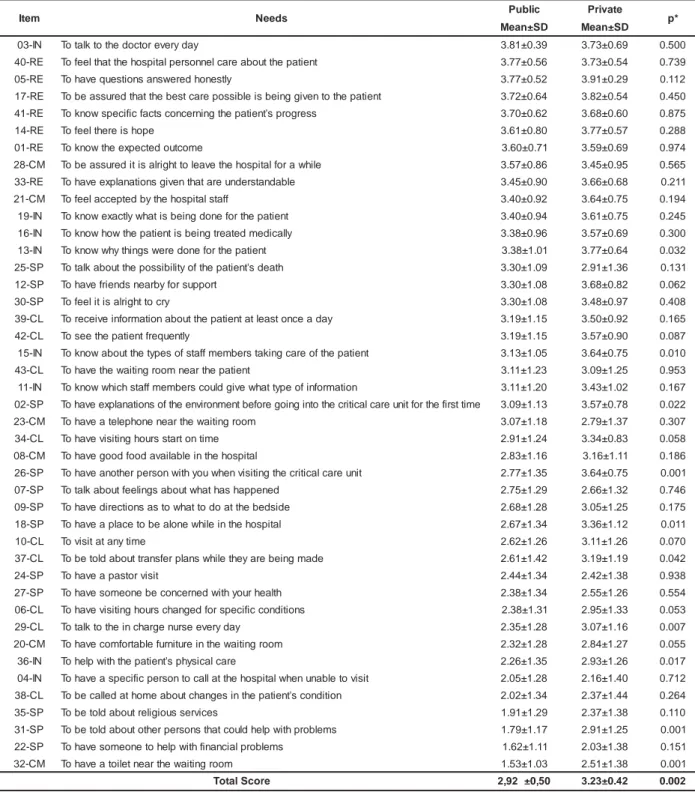
Table 2 below com pares bot h groups in t erm s
of m ean sat isfact ion scores about m eet ing I NEFTI needs.
m e t
I Needs Public Private p-value*
D S ± n a e
M Mean±SD
L C -2
4 Toseethepatientfrequently 3.98±0.14 3.82±0.65 0.106 E
R -0
4 Tofeelthatthehospitalpersonnelcareaboutthepatient 3.98±0.14 3.98±0.15 0.963
L C -7
3 Tobetoldabouttransferplanswhiletheyarebeingmade 3.98±0.14 3.89±0.49 0.222 E
R -7
1 Tobeassuredthatthebestcarepossibleisbeinggiventothepatient 3.98±0.14 4.00±0.00 0.323
N I -6
1 Toknowhowthepatientisbeingtreatedmedically 3.98±0.14 3.95±0.21 0.529 N
I -3
1 Toknowwhythingsweredoneforthepatient 3.98±0.14 3.98±0.15 0.963
E R -1
0 Toknowtheexpectedoutcome 3.98±0.14 3.98±0.15 0.963 N
I -3
0 Totalktothedoctoreveryday 3.96±0.20 3.98±0.15 0.598
L C -4
3 Tohavevisitinghoursstartontime 3.94±0.24 3.73±0.49 0.029 E
R -3
3 Tohaveexplanationsgiventhatareunderstandable 3.94±0.24 3.95±0.21 0.703
E R -5
0 Tohavequestionsansweredhonestly 3.94±0.24 3.84±0.64 0.362 N
I -5
1 Toknowaboutthetypesofstaffmemberstakingcareofthepatient 3.91±0.45 3.89±0.38 0.748
N I -1
1 Toknowwhichstaffmemberscouldgivewhattypeofinformation 3.91±0.45 3.93±0.25 0.827 P
S -9
0 Tohavedirectionsastowhattodoatthebedside 3.87±0.49 3.84±0.52 0.770
E R -4
1 Tofeelthereishope 3.87±0.61 3.89±0.49 0.904 E
R -1
4 Toknowspecificfactsconcerningthepatien'tsprogress 3.87±0.53 3.95±0.21 0.345
P S -2
0 Tohaveexplanationsoftheenvironmentbeforegoingintothecriticalcareunitfortheifrsttime 3.85±0.36 3.91±0.29 0.399 L
C -9
3 Toreceiveinformationaboutthepatientatleastonceaday 3.85±0.62 3.95±0.30 0.322
M C -8
2 Tobeassureditisalrighttoleavethehospitalforawhile 3.83±0.63 3.89±0.38 0.607 M
C -1
2 Tofeelacceptedbythehospitalstaff 3.83±0.52 3.82±0.44 0.909
N I -9
1 Toknowexactlywhatisbeingdoneforthepatient 3.83±0.63 3.93±0.25 0.324 M
C -2
3 Tohaveatoiletnearthewaitingroom 3.81±0.64 3.80±0.59 0.920
P S -1
3 Tobetoldaboutotherpeoplethatcouldhelpwithproblems 3.72±0.71 3.82±0.49 0.461 M
C -3
2 Tohaveatelephonenearthewaitingroom 3.68±0.81 3.57±0.95 0.546
L C -6
0 Tohavevisitinghourschangedforspecificconditions 3.66±0.86 3.45±1.04 0.313 P
S -7
2 Tohavesomeonebeconcernedwithyourhealth 3.62±0.87 3.20±1.13 0.054
P S -2
1 Tohavefriendsnearbyforsupport 3.57±0.95 3.75±0.71 0.321 L
C -8
3 Tobecalledathomeaboutchangesinthepatien'tscondition 3.55±1.03 3.77±0.74 0.252 N
I -4
0 Tohaveaspecificpersontocallatthehospitalwhenunabletovisit 3.53±0.85 3.45±1.02 0.697
P S -0
3 Tofeelitisalrighttocry 3.47±1.01 3.64±0.75 0.374 P
S -6
2 Tohaveanotherpersonwithyouwhenvisitingthecriticalcareunit 3.47±1.06 3.57±0.87 0.623
L C -3
4 Tohavethewaitingroomnearthepatient 3.47±1.06 3.09±1.27 0.127 P
S -2
2 Tohavesomeonetohelpwithfinancialproblems 3.36±1.09 3.70±0.73 0.084
P S -4
2 Tohaveapastorvisit 3.34±1.10 3.57±0.87 0.391 L
C -9
2 Totalktotheinchargenurseeveryday 3.32±1.12 3.45±0.97 0.540
P S -5
2 Totalkaboutthepossibiiltyofthepatien'tsdeath 3.23±1.23 3.59±0.97 0.131 P
S -7
0 Totalkaboutfeeilngsaboutwhathashappened 3.13±1.26 2.68±1.44 0.120
M C -8
0 Tohavegoodfoodavailableinthehospital 3.11±1.16 3.73±0.49 0.002 P
S -5
3 Tobetoldaboutreilgiousservices 2.91±1.28 3.36±1.05 0.073
N I -6
3 Tohelpwiththepatien'tsphysicalcare 2.89±1.38 2.75±1.40 0.624 M
C -0
2 Tohavecomfortablefurnitureinthewaitingroom 2.81±1.36 3.39±1.06 0.027
L C -0
1 Tovisitatanytime 2.55±1.28 2.41±1.41 0.613 P
S -8
1 Tohaveaplacetobealonewhileinthehospital 1.89±1.25 2.55±1.47 0.025
e r o t s l a t o
Table 2 - Mean v alues and st andar d dev iat ion of sat isfact ion scor es for 43 I NEFTI needs. São Paulo, SP, 2005
Obser vat ions: * St udent ’s t - t est ; RE: Reassur ance, I N: I nfor m at ion, CL: Closeness, SP: Suppor t , CM: Com for t
Fam ily m em b er s of p at ien t s at t h e p r iv at e
I CU pr esent ed a higher t ot al sat isfact ion scor e ( 3. 23)
t h an at t h e p u b l i c o n e ( 2 . 9 2 ) , w i t h a st at i st i cal l y
sign ifican t differ en ce ( p= 0 . 0 0 2 ) . Con sider in g t h e 4 3
sat isf act ion it em s, r elat iv es at t h e p u b lic I CU w er e
dissat isf ied or lit t le sat isf ied ( m ean < 3 ) w it h alm ost
h al f of t h e n eed s ( 4 6 . 5 % ) , ag ai n st 3 2 . 5 % am on g
r elat iv es at t h e pr iv at e I CU.
W h e n c o m p a r i n g m e a n s c o r e s p e r i t e m ,
si g n i f i ca n t d i f f e r e n ce s b e t w e e n g r o u p s a p p e a r e d
f o r t e n n e e d s, m o st o f t h e m r e l a t e d t o su p p o r t
a n d i n f o r m a t i o n . On a l l i t e m s , m e a n s c o r e s f o r
r e l a t i v e s a t t h e p r i v a t e I CU i n d i c a t e d g r e a t e r
sa t i sf a ct i o n .
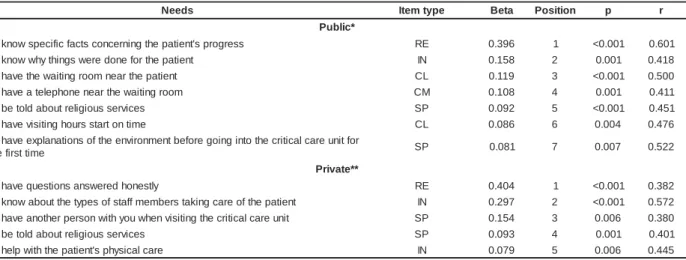
Ta b l e 3 sh o w s Mu l t i p l e Li n e a r Re g r e ssi o n
analy sis r esult s for t he it em s of im por t ance scale.
m e t
I Needs Public Private p*
D S ± n a e
M Mean±SD
N I -3
0 Totalktothedoctoreveryday 3.81±0.39 3.73±0.69 0.500
E R -0
4 Tofeelthatthehospitalpersonnelcareaboutthepatient 3.77±0.56 3.73±0.54 0.739
E R -5
0 Tohavequestionsansweredhonestly 3.77±0.52 3.91±0.29 0.112
E R -7
1 Tobeassuredthatthebestcarepossibleisbeinggiventothepatient 3.72±0.64 3.82±0.54 0.450
E R -1
4 Toknowspecificfactsconcerningthepatien'tsprogress 3.70±0.62 3.68±0.60 0.875
E R -4
1 Tofeelthereishope 3.61±0.80 3.77±0.57 0.288
E R -1
0 Toknowtheexpectedoutcome 3.60±0.71 3.59±0.69 0.974
M C -8
2 Tobeassureditisalrighttoleavethehospitalforawhile 3.57±0.86 3.45±0.95 0.565
E R -3
3 Tohaveexplanationsgiventhatareunderstandable 3.45±0.90 3.66±0.68 0.211
M C -1
2 Tofeelacceptedbythehospitalstaff 3.40±0.92 3.64±0.75 0.194
N I -9
1 Toknowexactlywhatisbeingdoneforthepatient 3.40±0.94 3.61±0.75 0.245
N I -6
1 Toknowhowthepatientisbeingtreatedmedically 3.38±0.96 3.57±0.69 0.300
N I -3
1 Toknowwhythingsweredoneforthepatient 3.38±1.01 3.77±0.64 0.032
P S -5
2 Totalkaboutthepossibiiltyofthepatien'tsdeath 3.30±1.09 2.91±1.36 0.131
P S -2
1 Tohavefriendsnearbyforsupport 3.30±1.08 3.68±0.82 0.062
P S -0
3 Tofeelitisalrighttocry 3.30±1.08 3.48±0.97 0.408
L C -9
3 Toreceiveinformationaboutthepatientatleastonceaday 3.19±1.15 3.50±0.92 0.165
L C -2
4 Toseethepatientfrequently 3.19±1.15 3.57±0.90 0.087
N I -5
1 Toknowaboutthetypesofstaffmemberstakingcareofthepatient 3.13±1.05 3.64±0.75 0.010
L C -3
4 Tohavethewaitingroomnearthepatient 3.11±1.23 3.09±1.25 0.953
N I -1
1 Toknowwhichstaffmemberscouldgivewhattypeofinformation 3.11±1.20 3.43±1.02 0.167
P S -2
0 Tohaveexplanationsoftheenvironmentbeforegoingintothecriticalcareunitfortheifrsttime 3.09±1.13 3.57±0.78 0.022
M C -3
2 Tohaveatelephonenearthewaitingroom 3.07±1.18 2.79±1.37 0.307
L C -4
3 Tohavevisitinghoursstartontime 2.91±1.24 3.34±0.83 0.058
M C -8
0 Tohavegoodfoodavailableinthehospital 2.83±1.16 3.16±1.11 0.186
P S -6
2 Tohaveanotherpersonwithyouwhenvisitingthecriticalcareunit 2.77±1.35 3.64±0.75 0.001
P S -7
0 Totalkaboutfeeilngsaboutwhathashappened 2.75±1.29 2.66±1.32 0.746
P S -9
0 Tohavedirectionsastowhattodoatthebedside 2.68±1.28 3.05±1.25 0.175
P S -8
1 Tohaveaplacetobealonewhileinthehospital 2.67±1.34 3.36±1.12 0.011
L C -0
1 Tovisitatanytime 2.62±1.26 3.11±1.26 0.070
L C -7
3 Tobetoldabouttransferplanswhiletheyarebeingmade 2.61±1.42 3.19±1.19 0.042
P S -4
2 Tohaveapastorvisit 2.44±1.34 2.42±1.38 0.938
P S -7
2 Tohavesomeonebeconcernedwithyourhealth 2.38±1.34 2.55±1.26 0.554
L C -6
0 Tohavevisitinghourschangedforspecificconditions 2.38±1.31 2.95±1.33 0.053
L C -9
2 Totalktotheinchargenurseeveryday 2.35±1.28 3.07±1.16 0.007
M C -0
2 Tohavecomfortablefurnitureinthewaitingroom 2.32±1.28 2.84±1.27 0.055
N I -6
3 Tohelpwiththepatien'tsphysicalcare 2.26±1.35 2.93±1.26 0.017
N I -4
0 Tohaveaspecificpersontocallatthehospitalwhenunabletovisit 2.05±1.28 2.16±1.40 0.712
L C -8
3 Tobecalledathomeaboutchangesinthepatien'tscondition 2.02±1.34 2.37±1.44 0.264
P S -5
3 Tobetoldaboutreilgiousservices 1.91±1.29 2.37±1.38 0.110
P S -1
3 Tobetoldaboutotherpersonsthatcouldhelpwithproblems 1.79±1.17 2.91±1.25 0.001
P S -2
2 Tohavesomeonetohelpwithfinancialproblems 1.62±1.11 2.03±1.38 0.151
M C -2
3 Tohaveatoiletnearthewaitingroom 1.53±1.03 2.51±1.38 0.001
e r o c S l a t o
Table 3 - Mult iple Linear Regr ession of I NEFTI im por t ance scale it em s. São Paulo, SP, 2005
s d e e
N Itemtype Beta Position p-value r
* c i l b u P t n e i t a p e h t r o f e n o d e r e w s g n i h t y h w w o n k o
T IN 0.578 1 <0.001 0.497
n o i t a m r o f n i f o e p y t t a h w e v i g d l u o c s r e b m e m f f a t s h c i h w w o n k o
T IN 0.140 2 <0.001 0.265
y a d y r e v e e s r u n e g r a h c n i e h t o t k l a t o
T CL 0.082 3 <0.001 0.493
s e c i v r e s s u o i g il e r t u o b a d l o t e b o
T SP 0.057 4 <0.001 0.581
l a t i p s o h e h t n i e l b a l i a v a d o o f d o o g e v a h o
T CM 0.046 5 <0.001 0.255
t i s i v r o t s a p a e v a h o
T SP 0.042 6 <0.001 0.396
s m e l b o r p l a i c n a n i f h t i w p l e h o t e n o e m o s e v a h o
T SP 0.040 7 <0.001 0.585
m o o r g n i t i a w e h t n i e r u t i n r u f e l b a t r o f m o c e v a h o
T CM 0.032 8 0.004 0.559
* * e t a v i r P e m o c t u o d e t c e p x e e h t w o n k o
T RE 0.479 1 <0.001 0.366
e d a m g n i e b e r a y e h t e l i h w s n a l p r e f s n a r t t u o b a d l o t e b o
T CL 0.145 2 <0.001 0.152
t r o p p u s r o f y b r a e n s d n e i r f e v a h o
T SP 0.134 3 <0.001 0.401
m o o r g n i t i a w e h t n i e r u t i n r u f e l b a t r o f m o c e v a h o
T CM 0.074 4 <0.001 0.424
y r c o t t h g i r l a s i t i l e e f o
T SP 0.058 5 0.006 0.347
s e c i v r e s s u o i g il e r t u o b a d l o t e b o
T SP 0.056 6 <0.001 0.519
l a t i p s o h e h t n i e l i h w e n o l a e b o t e c a l p a e v a h o
T SP 0.041 7 <0.001 0.685
e m i t y n a t a t i s i v o
T CL 0.031 8 0.002 0.507
Obser vat ions: * adj ust ed r2= 0.99; * * adj ust ed r2= 1.0; RE: Reassur ance, I N: I nfor m at ion, CL: Closeness, SP: Suppor t , CM: Com for t .
I n accor dance w it h Table 3, t he it em t hat m ost
cont r ibut ed t o v ar iat ion in t he t ot al im por t ance scor e
at t he public hospit al w as “ t o k now w hy t hings w er e
done for t he pat ient ” ( b= 0.578) . At t he pr iv at e I CU,
t his w as t he case for “ t o know t he expect ed out com e”
( b= 0. 479) . Am ong t he needs t hat cont inued in bot h
m od els, on ly “ t o h av e com f or t ab le f u r n it u r e in t h e
w ait in g r oom ” an d ” t o b e in f or m ed ab ou t r elig iou s
ser v ices” w er e pr esent in bot h gr oups. How ev er, “ t o
have com for t able fur nit ur e in t he w ait ing r oom ” caused
a gr eat er in cr ease in t h e t ot al scor e at t h e pr iv at e
( ß= 0.074) t han at t he public hospit al ( ß= 0.032) .
Mult iple Linear Regr ession analy sis r esult s of
I NEFTI satisfaction scale item s are presented in Table 4.
Table 4 - Mult iple Linear Regr ession of I NEFTI sat isfact ion scale it em s. São Paulo, SP, 2005
s d e e
N Itemtype Beta Position p r
* c i l b u P s s e r g o r p s 't n e i t a p e h t g n i n r e c n o c s t c a f c i f i c e p s w o n k o
T RE 0.396 1 <0.001 0.601
t n e i t a p e h t r o f e n o d e r e w s g n i h t y h w w o n k o
T IN 0.158 2 0.001 0.418
t n e i t a p e h t r a e n m o o r g n i t i a w e h t e v a h o
T CL 0.119 3 <0.001 0.500
m o o r g n i t i a w e h t r a e n e n o h p e l e t a e v a h o
T CM 0.108 4 0.001 0.411
s e c i v r e s s u o i g il e r t u o b a d l o t e b o
T SP 0.092 5 <0.001 0.451
e m i t n o t r a t s s r u o h g n i t i s i v e v a h o
T CL 0.086 6 0.004 0.476
r o f t i n u e r a c l a c i t i r c e h t o t n i g n i o g e r o f e b t n e m n o r i v n e e h t f o s n o i t a n a l p x e e v a h o T e m i t t s r i f e h
t SP 0.081 7 0.007 0.522
* * e t a v i r P y l t s e n o h d e r e w s n a s n o i t s e u q e v a h o
T RE 0.404 1 <0.001 0.382
t n e i t a p e h t f o e r a c g n i k a t s r e b m e m f f a t s f o s e p y t e h t t u o b a w o n k o
T IN 0.297 2 <0.001 0.572
t i n u e r a c l a c i t i r c e h t g n i t i s i v n e h w u o y h t i w n o s r e p r e h t o n a e v a h o
T SP 0.154 3 0.006 0.380
s e c i v r e s s u o i g il e r t u o b a d l o t e b o
T SP 0.093 4 0.001 0.401
e r a c l a c i s y h p s 't n e i t a p e h t h t i w p l e h o
T IN 0.079 5 0.006 0.445
Obser vat ions: * adj ust ed r2= 0.99; * * adj ust ed r2= 1.0; RE: Reassur ance, I N: I nfor m at ion, CL: Closeness, SP: Suppor t , CM: Com for t .
At t h e p u b lic u n it , sev en ou t of 4 3 I NEFTI
it em s cont inued in t he m odel as sat isfact ion predict ors
w hen adj ust ed by t he ot her it em s. The it em t hat m ost
cont ribut ed t o fam ily m em ber s’ sat isfact ion at t his unit
w as “ t o k n ow specific fact s concer ning t h e pat ien t ’s
p r o g r e ss” ( b = 0 . 3 9 6 ) . Th e o t h e r n e e d s ca u se d a
sm al l er i n cr ease i n t h e f i n al sat i sf act i o n sco r e ( b
r anging fr om 0.081 t o 0.158) .
At the private unit, only five item s continued as
predictors in the m ultiple analysis. The item s that m ost
contributed to the total satisfaction score were “ to have
quest ions answered honest ly” ( b= 0.404) and “ t o know
about the types of staff m em bers taking care of the patient”
( b= 0.297) . Only “ t o be t old about r eligious ser v ices”
appeared in both m odels, leading to a sim ilar variation in
DI SCUSSI ON
Var ious st udies hav e looked at t he needs of
cr it ical p at ien t s’ r elat iv es. Alt h ou g h u sin g d if f er en t
quant it at iv e or qualit at iv e m et hodologies, all of t hem
h av e t h e sam e g oal: g et t in g t o k n ow t h ese f am ily
m em bers’ needs and allowing for int ervent ion planning
in order t o m eet pat ient s’ and fam ilies’ act ual dem ands.
Assessm en t o f t h ese r el a t i v es’ n eed s h a s
b e e n g u i d e d b y t h e p e r ce p t i o n o f t h e d e g r e e o f
im por t an ce an d sat isf act ion w it h aspect s r elat ed t o
p a t i e n t a n d f a m i l y ca r e d e l i v e r y. I d e n t i f y i n g t h e
im p or t an ce m ak es it p ossib le t o g et t o k n ow h ow
fam ilies v alue t hese needs and pr ov ides dat a t o plan
and im plem ent act ions in or der t o m eet t hese needs,
as w ell as t o r edir ect t he possible focus of sit uat ions
w hich r elat ives and pat ient s do not consider im por t ant .
Mea su r i n g sa t i sf a ct i o n l ev el s, o n t h e o t h er h a n d ,
su p p or t s t h e iden t if icat ion of u n m et n eed s an d t h e
assessm ent of car e qualit y.
Despit e t he differ ences in sociodem ogr aphic
pr ofile, bot h gr oups show ed no significant differ ence
b et w een t o t al i m p o r t an ce sco r es ( Tab l e 1 ) . Wh en
com par ing it em s indiv idually, t he t w o gr oups differ ed
in t er m s of t h e im por t an ce t h ey at t r ibu t ed t o som e
needs. Fam ily m em ber s at t he public unit consider ed
“ t o have visit ing hour s st ar t on t im e” m or e im por t ant .
This m ay be relat ed t o const ant delays in visit ing hours
a n d w a i t i n g t i m e s t h e y e x p e r i e n c e d d u r i n g t h e
r est r ict ed v isit s allow ed at t his inst it ut ion. The sam e
g r o u p f o u n d “ t o h a v e g o o d f o o d a v a i l a b l e i n t h e
hospit al”, “ t o have com fort able furnit ure in t he wait ing
r oom ” and “ t o hav e a place t o be alone w hile in t he
hospit al” less im por t ant , a fact t hat w as also obser ved
in ot h er st u d ies ( 8 - 9 ). Th e f act t h at r elat iv es at t h e
p r iv at e I CU at t r ib u t e m or e v alu e t o com f or t n eed s
m ay be associat ed w it h t h eir h igh er edu cat ion lev el
and fam ily incom e, w hich gener al m ak es t hem m or e
d e m a n d i n g a n d a w a r e o f w h a t se r v i ce s t h e y ca n
r equir e fr om t he hospit al and pr ofessionals.
These st udy r esult s ev idenced a significant ly
higher lev el of dissat isfact ion am ong r elat iv es at t he
public inst it ut ion ( Table 2) . The great er dissat isfact ion,
m ainly wit h respect t o support and inform at ion needs,
ca n b e a t t r i b u t ed t o t h e Un i t ’ s a n d t h e r el a t i v es’
charact erist ics: reduced num ber of pat ient visit s, once
per day and w it h lim it ed dur at ion; r est r ict ed cont act
w it h t eam pr ofessionals, w it h phy sicians as t he only
pr ofessionals r esponsible for giv ing infor m at ion about
t he pat ient ’s condit ion; absence of st rat egies for
nurse-f a m i l y i n t eg r a t i o n a n d co m m u n i ca t i o n d i nurse-f nurse-f i cu l t i es,
w h et h er d u e t o l o w er ed u ca t i o n l ev el s o r a l t er ed
em ot ional st at e, which are fact ors t hat affect int eract ion
wit h t he t eam and creat e anguish in fam ily m em bers.
The lack of com parat ive st udies about fam ily m em bers’
needs at different kinds of inst it ut ions m akes it difficult
t o confront t hem wit h t he obt ained research result s.
Th e m u lt iv ar iat e an aly sis p er f or m ed in t h is
st u dy m ade it possible t o an aly ze t h e sim u lt an eou s
effect of independent var iables ( in t his case t he needs)
on t he dependent var iable ( im por t ance or sat isfact ion
l e v e l ) . D i f f e r e n t l y f r o m m e a n s co m p a r i so n t e st s,
r egr ession analy sis can help healt h pr ofessionals and
m anager s t o est ablish pr ior it ies, in v iew of t he w ide
r ange of aspect s t hey need t o t ake int o consider at ion.
S o m e n e e d s t h a t s e e m e d l e s s i m p o r t a n t w h e n
analy zed isolat edly becam e im por t ant w hen assessed
in int er act ion w it h ot her needs. This w as t he case of
com f or t n eed s f or r elat iv es at t h e p u b lic h osp it al.
Hence, if at least t he eight needs t hat m ost cont r ibut ed
t o t h e i m p o r t a n c e s c o r e w e r e m e t , r e l a t i v e s ’
sat isf act ion lev el w ou ld p r ob ab ly in cr ease, as t h eir
m ost im por t ant needs w ould be at t ended t o. I f only
one of t heir needs could be m et , pr ior it ies should be
est ablished on t he basis of t he incr ease ( b) each of
t h em w o u l d p r o v i d e. Th u s, at t h e p u b l i c h o sp i t al ,
infor m ing fam ily m em ber s about w hy t r eat m ent s ar e
offer ed t o t h e pat ien t w ou ld be t h e m ost im por t an t
aspect . At t he pr iv at e inst it ut ion, on t he ot her hand,
t h e p r ior it y w ou ld b e t o in f or m r elat iv es ab ou t t h e
pat ient ’s chances of im pr ov em ent ( Table 3 ) .
Most r esear ch on fam ily m em ber s’ needs have
used descr ipt iv e st at ist ics t o ex am ine t he im por t ance
given t o t hese needs, so t hat t her e ar e no st udies t o
c o m p a r e t h e m u l t i p l e r e g r e s s i o n r e s u l t s w i t h .
I n f or m at ion , Reassu r an ce an d Closen ess h av e been
i d en t i f i ed as t h e m o st i m p o r t an t n eed s f o r f am i l y
m em ber s of cr it ical pat ient s, and Suppor t and Com for t
needs as t he less im por t ant dom ains ( 9,12- 14).
The m ult ivariat e analysis of sat isfact ion levels
about t he 43 needs dem onst r at ed t hat , at t he public
hospit al, r elat iv es’ sat isfact ion lev el is influenced by
a lar ger num ber of needs t han at t he pr ivat e inst it ut ion.
At t h e pu blic u n it , t h e sat isfact ion lev el w as m ain ly
i n f l u e n c e d b y t h e f a c t t h a t r e l a t i v e s r e c e i v e d
in f or m at ion abou t t h e pat ien t ’s clin ical pr ogr ess. At
t he privat e inst it ut ion, on t he ot her hand, sat isfact ion
w as r elat ed t o “ hav ing quest ions answ er ed honest ly ”
and “ know ing about t he t ypes of st aff m em ber s t aking
I t sh o u l d b e em p h a si zed t h a t “ t o b e t o l d
a b o u t r e l i g i o u s se r v i ce s” w a s t h e o n l y n e e d t h a t
cont inued in t he im por t ance and sat isfact ion m odels
at t he public and pr iv at e inst it ut ions. This int er est ing
r e s u l t s e e m s t o b e p e c u l i a r t o o u r r e a l i t y a n d
deser ves m or e in- dept h st udy. Em pir ical st udies hav e
ident ified t hat r eligion and spir it ualit y ex er t significant
i n f l u en ce o n p eo p l e’s p h y si cal an d m en t al h eal t h .
Relig iou s an d sp ir it u al p r act ices ar e con sid er ed as
p s y c h o s o c i a l s u p p o r t t h a t f a v o r s t h e f e e l i n g o f
subj ect iv e w ell- being and t he m anifest at ion of gr eat er
s e c u r i t y , h o p e a n d s e l f - e s t e e m ( 1 5 ). Fo r f a m i l y
m e m b e r s o f i n t e n s i v e c a r e p a t i e n t s , t h e y c a n
r ep r esen t an im p or t an t in t er n al r esou r ce in cop in g
w it h cr it ical sit u at ion s, su ch as p ain , su f f er in g an d
d ea t h .
These st udy r esult s indicat e t he m ain fact or s
capable of cont r ibut ing t o how fam ily m em ber s’ needs
at p u b li c an d p r iv at e I CU can b e m et ad eq u at el y.
How ev er, im p lem en t in g in t er v en t ion s am on g t h ese
persons is not only an individual responsibilit y of I CU
pr ofession als, bu t sh ou ld be assu m ed t oget h er w it h
h e a l t h i n st i t u t i o n m a n a g e r s. Ack n o w l e d g i n g a n d
including pat ient s’ fam ilies as a care focus presupposes
f u n d a m e n t a l ch a n g e s i n t h e p e r sp e ct i v e o n a n d
or ganizat ion of public and pr iv at e healt h inst it ut ions.
Recebido em : 20.2.2006 Apr ovado em : 3.7.2006
REFERENCES
1 . Lesk e JS. Need s of r elat iv es of cr it ical car e p at ien t s: a follow u p. Hear t Lu n g 1 9 8 6 ; 1 5 ( 2 ) : 1 8 9 - 9 3 .
2 . Molt er NC. Needs of r elat iv es of cr it ically ill pat ien t s: a descr ipt iv e st u dy. Hear t Lu n g 1 9 7 9 ; 8 ( 2 ) : 3 3 2 - 9 .
3 . Lesk e JS. I n t er n al psy ch om et r ic pr oper t ies of t h e Cr it ical Ca r e Fa m i l y Ne e d s I n v e n t o r y. He a r t Lu n g . 1 9 9 1 ; 2 0 ( 3 ) : 2 3 6 - 4 4 .
4 . Ca st r o D S. Est r e sse e e st r e sso r e s d o s f a m i l i a r e s d e p aci en t es co m t r au m at i sm o cr ân i o en cef ál i co em t er ap i a int ensiva. [ t ese] . Rio de Janeir o ( RJ) : Escola de Enfer m agem / UFRJ; 1 9 9 9 .
5. Leder er M, Goode T, Dow ling J. The cr it ical car e assist ance p r og r am . Ch est 2 0 0 5 ; 1 2 8 ( 3 ) : 6 6 S- 7 5 S.
6 . Ro ch a JSY. Est u d o d a assi st ên ci a h o sp i t al ar p ú b l i ca e p r i v a d a em b a ses p o p u l a ci o n a i s: 1 9 8 6 - 1 9 9 6 . Rev Sa ú d e Pú b l i ca 1 9 9 9 ; 3 3 ( 1 ) : 4 4 - 5 4 .
7 . Lu cch ese AC. Est u d o sob r e os f am iliar es d os p acien t es i n t e r n a d o s n o h o s p i t a l g e r a l e s u a s n e c e s s i d a d e s . [ disser t ação] . São Pau lo ( SP) : Escola Pau list a de Medicin a d a UNI FESP; 2 0 0 3 .
8. Tin MK, Fr ench P, Leung KK. The needs of t he fam ily t he cr it ically ill n eu r osu r gical pat ien t s: a com par ison of n u r ses’ an d f am ily m em b er s’ p er cep t ion s. J Neu r osci Nu r s 1 9 9 9 ; 3 1 ( 6 ) : 3 4 8 - 5 6 .
9. Lee LY, Lau YL. I m m ediat e needs of adult fam ily m em ber s of adu lt in t en siv e car e pat ien t s in Hon g Kon g. J Clin Nu r s 2 0 0 3 ; 1 2 ( 4 ) : 4 9 0 - 5 0 0
1 0 . Bl a n d MJ, Al t m a n PG. Cr o n b a ch ’ s a l p h a . BMJ 1 9 9 7 ; 3 1 4 : 1 9 3 - 4 .
11. Fay er s P, Machin D. Qualit y of life: assessm ent analy sis and int er pr et at ion. England: Willey ; 2000.
12. Lee I YM, Chien W, Mackenzie AE. Needs of fam ily w it h a r elat iv e in a cr it ical car e unit in Hong Kong. J Clin Nur s 2000; 9 ( 1 ) : 4 6 - 5 4 .
1 3 . Bij t t ebier P, Van oost S, Delva D, Fer din an d P, Fr an s E. Need s of r elat iv es of cr it ical car e p at ien t s: p er cep t ion s of r elat iv es, phy sicians and nur ses. I nt ensiv e Car e Med 2 0 0 1 ; 2 7 ( 1 ) : 1 6 0 - 5 .
14. Hassan MA, Hw eidi I M. The per ceived needs of Jor danian fam ilies of hospit alized, cr it ically ill pat ient s. I nt J Nur s Pr act 2 0 0 4 ; 1 0 ( 2 ) : 6 4 - 7 1 .