1~~~~~~~~~~~
II'1I(((1
lis
1
Sexually Transmitted Diseases
Sexually transmitted diseases (STD) refer to a group of diverse diseases that share only one major feature: sex-ual transmission. Obviously, many diseases, such as streptococcal pharyngitis, measles, and infectious mono-nucleosis, can be transmitted from one person to another during sexual activity, but should not be classified as STD. Thus transmission during sexual activity or sexual intercourse does not fully define this group of diseases. From a practical point of view, STD should include all infections in which sexual transmission is epidemiologi-cally important. In some groups, such as patients who receive blood transfusions, hepatitis B is not an STD. In others, such as those composed of homosexual men, hep-atitis B is a major STD and sexual transmission is a ma-jor epidemiological feature of the disease.
All countries in the Region have limited their concept of STD to the traditional venereal diseases including gonorrhea, syphilis, chancroid, lymphogranuloma vene-reum, and Donovaniasis (granuloma inguinale). In the past decade, the list of STD has grown significantly in both the number of diseases and complexity (Table 1).
STD usually do not cause significant mortality in any age group. In addition, many of the clinical expressions of the infections are mild and innocuous and quite a few may even be asymptomatic. Their importance, as public health problems, however, lies in their ability to produce severe, chronic, debilitating complications. The late
manifestations of neurosyphilis and cardiovascular syph-ilis are well known. Yet new information suggests that some of the other STD may be responsible for equally serious complications. Recent advances have revealed an association between herpes infection and carcinoma of the cervix, and between chlamydial infection and pneu-monia in the newborn.
Recently, the relationship between pelvic inflam-matory disease (PID) and infertility and ectopic preg-nancy has been carefully documented. The role of Neisseria gonorrhloeae in the etiology of pelvic inflamma-tion is well known, but chlamydial infecinflamma-tions have fur-ther magnified the importance of this clinical complex. Data published in the United States reveal that more than 850,000 episodes of PID occur annually, requiring more than 212,000 hospital admissions, 115,000 surgical procedures, and 2,500,000 physician visits. Direct and indirect costs exceeded $1,250 million dollars in 1979.1 The consequences of PID include infertility, ectopic pregnancy, and chronic pelvic pain and occur in young women (25-34 years of age) during child-bearing years. The attention of public health administrators and
plan-'Curran, J. W. Economic coniseqiuenices ot pelvic inilaiinnaitory discase iii the United States. Ami J Obstet Gyc'/ 138:848-851. 1980.
IN THIS ISSUE...
* Sexually Transmitted Diseases
* Diseases Subject to the International Health Regulations * Cancer in Puerto Rico, 1978
* Dengue in Mexico and in the United States. 1980
* Influenza in the Aniericas. 1980-1981
* Status of Leprosy in Rio Grande do Sul. Brazil. 1979 * Courses
* Calendar of Courses on Epidenmiology iii Latin Anierica and the Caribbean. 1981
I~
~
~
~
~
~
~
~~~~
Table 1. Sexually transmitted diseases.
Discase Organlism
Viril
Herpes genitalis Herpes simplex. Tvyp 11 Hepatitis B Hepatitis B virus Cytoniegalovirus infection Cytomegalos irus Con dvloniat a iactl in latluiii Papova virlis
Molluscurii contagiosumii Poxvirus
Chhílovdial
Chlanivdia urethritis Chllanyivdia traclhom;atis (ni uiltiple serotyVes) Chlamynivdia cenicitis
Pelvic inflalnintator disease
Conjulnct itis
Pneuti¡monitis ini the newborn
Lyiiiphogranlo v v re rcun Chia rachomatis (Scrot!pes L)
M\y¡coíl1ís,,líI
Uret hritis 1 -imycopl asma Ccrvicitisa
Bacterial
Urethritis Neisseria gonorriloe;ae Cecricitis
Pelvic inflaniiilmatonr disease Donovaniasis
(granulonia inguinale) Donovlania granululoemlatis Vaginitis Cotrvncbactcrinmiii vaginale
Spirolhetal
Syphilis Treponeniia pallidutii
Protozoal
Trichonioniasis Trichonliontas vagiinale
Scabies Sarcoptes scabiei
Pcdiculosis pubis Phthiruts pubis
lT-hc etiological role of 7T. oincolílls.inl utietlritis/clrvicitis is stili disputed.
Table 2. Reported cases of gonorrhea, by sex, 1978.
Regiotn. country. or
other admiin istrativ e uniit Male Femiale TotalP Carihbban,
Antigua Balhanlas Barbados Bernimuida Caymanii Islands Cuba
Domiinica
Domiinican Reptiblic Grenada Guadeloupc Haiti Janiaica Martinique Montscrrat Netherlands Anltilles Saint Lucia
St. Kitts-Nevis-Anguilla St. Pierre anid Miquelon St. Vintcent
Trinidad and Tobago Tlurks anid Caicos Islands Virgin Islaiids (UK) Virgin Islands (USA)
Subtotal
MidlIle A nlr¡ica
Belizc Costa Rica El Salvador G uateiala
Honduras Mexico Nicaragua Paíanama Subtotal 98 1.185 379 9.692 1.354 40 309 208
.
185 1.494 587517 10.211
- 331 - 18.540 20 2.007 18 627 117
_- 75
-- 2.599
-- 61
-- 76
-- 216
1.074 36.864
4.627 1.742 6.370
- - 6.354
- - 2.867
- - 5,996
-- -- 20.487 1.332 1,791 3.123
2.401 1.242 3.643
8.360 4,775 48,840
.
ners nmust therefore shift fronm concern with traditional venereal disease incidence to the entire range of STD and their complications.
Epidemiology of STD in the Region
The true magnitude of the STD probleni in the Region cannot be assessed. Data on the incidence of all STD are incomplete. out-of-date, or non-existent.
Although many countries maintain statistical data on reported cases of gonorrhea and syphilis, most of theni do not provide detailed information to PAHO and none supply information on the occurrence of other STD or on the magnitude of STD complications. In some cases the latest available information is for 1976 or earlier with no reports received since that year.
Table 2 summarizes available data on the reported in-cidence of gonorrhea by sex for four areas: North Amrnerica, continental Middle America (including Mex-ico), the Caribbean. and South America. The year 1978 was picked arbitrarily since it was the latest year with the
SoUth Almerica Argentiina Bolivia Brazil Clhile Colonmbia Ecuador Falkliand Islanids Frencli Guiaína Guyana Paraguay Peru StUIrinamc Uruguay Vcnezuela Subtotal
-- -- 15.883 1.767
-- _- 11.068
_- -_ 42.889
-- -- 3.489
663 302 967
- - 635
-- -_ 4.629
234
897
Nortll Ainmerica
Canada United States
Subtotal
T'Iotal
29.485
597.639 627.124
160 1.619
- 26.597
462 109.543
17.869 415.797 433.666 48.751 1.013.436 1.062.187 647.735 439,977 1,257.434
Thle sumni of iiiale and feale cases iii sonie couitries may not be cqual to the total nuniber of reported cases because of noín-reporting of SOlliC cases bv sex.
-Data not available.
e
2most complete information reported by the greatest number of countries. Several conclusions can be drawn from these and other data:
1. Countries that report by sex consistently show relatively large male to female case ratios. e.g., 10.6:1.0 for the Carib-bean: 1.9:1.0 for South Anmerica; 1.8:1.0 for Middle Arnerica. and 1.4:1.0 for North America. The ratio for the Caribbean is heavily influenced by the data from Cuba (9.692 nien vs. 517 women). The ratio is directly related to efforts to detect cases in wornen who are generally asymptoniatic and do not seek care.
iin the United States and Canada case-finding efforts through culture screening of women at risk result in lower niale to fenmale ratios. Very few countries in the Region have initiated progranis to diagnose gonorrhea ¡i asyniptoniatic women, the niost vulnerable group for developing PID. Interestingly. two countries. Colombia and Nicaragua. consistently report an ex-cess of female cases.
2. It is inipossible to make an accurate analysis without more information other than total cases. Reporting by age and sex is essential. In South Anierica only 1.2 per cent of all cases
re-ported to PAHO were by sex. In the Caribbean, Middle Anier-ica, and North Anierica the percentages were 33.7, 26.9. and 99.9. respectively.
3. An exanmination of incidence by age group reveals pat-terns throughout the Region which are similar to those found in the United States. Gonorrhea is a disease of young people aged
15-34 years.
4. Surveillance systems vary greatly in their completeness throughout the Region. The United States and Canada together reported 1,062,187 cases. or 84.5 per cent of all the cases in the Region. Yet these two countries together have only 40.6 per cent of the Region's total population. It is doubtful that the
lack of cases reported froni other areas represents a relative
absence of disease.
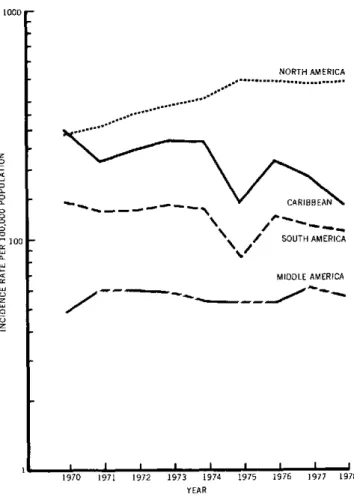
Trends in gonorrhea case rates are presented by area in Figure 1. The rates for North America are heavily in-fluenced by reports from the United States. In North America the increasing trend through 1975 reflects worldwide experience. Vigorous control measures in-cluding widespread application of standard, effective treatment, improvements in clinical services, and active case-finding measures stabilized the incidence from 1976 to the present. Trends in other areas are difficult to inter-pret in the absence of active case-finding efforts among women.
In 1976 the first penicillin-resistant strains of gonor-rhea caused by penicilinase (3-lactamase) producing N.
gonorrhoeae (PPNG) were identified in the Far East.
These strains spread quickly and became established in many countries. In North America spread of this isolate was contained and its occurrence was limited to sporadic importations with minor outbreaks. However, during the first half of 1980, the United States reported dramatic in-creases in PPNG cases which could not be attributed to importation. In Latin America and the Caribbean, only Mexico, Panama, and Argentina have reported a few cases. With these exceptions, nothing is known of the prevalence or distribution of PPNG in these areas.
Figure 1. Trends in reported gonorrhea cases per 100,000 population, by area, 1970-1978.
1000
z0 o D o
-100
o
1
u
Z
c1 uZ
II
NORTH AMERICA
...
...
\ / SOUTH AMERICA
MIDDLE AMERICA
/ ....
_~-r
1970 1971 1972 1973 1974 1975 1976 1977 1978
YEAR
Syphilis surveillance systems also are incomplete. Al-though individual countries maintain more detailed in-formation systems, most of the data reported to PAHO are incomplete and do not permit a careful analysis. As-sessment of the magnitude of infectious syphilis (i.e., pri-mary, secondary, and early latent less than one or two years' duration) is impossible since in 1978 only 13 of 47 countries reported early syphilis cases. Total syphilis cases were available from reports by 35 of 47 countries and are summarized in Table 3.
Although syphilis reporting is more complete than that of gonorrhea, major discrepancies occur. For example, in South America, Argentina, Chile, Colombia, and
Venezuela reported 56,810 cases (85.7 per cent of the
Table 3. Total reported cases of syphilis and rates per 100,000 population, by area, 1978.
Arca No. of cases Rate
North Amrnerica 67.764 28.0
Caribbean 26.029 93.6
Middle Arnmerica 25.123 28.6 South Animerica 66,264 65.3
area total), while no cases were reported by Brasil. The Dominican Republic notified 65.3 per cent of all the
cases in the Caribbean.
Age and sex data are too incomplete to draw meaning-ful conclusions. However, the occurrence of congenital syphilis cases in children less than one year of age may be a good indicator of the seriousness of the problem. Table 4 summarizes available data from a few countries that re-ported congenital syphilis cases. Major differences in rates may reflect the absence of case reporting, the com-pleteness of the surveillance system, or the severity of the syphilis problem. Cuba and the United States have ex-tensive syphilis control programs and active surveillance systems. Their rates, which are similar, probably reflect accurately the true incidence of congenital syphilis. The high rate in Costa Rica probably results from the revital-ization of its STD control program and surveillance sys-tem. Comparisons, however, should be made with cau-tion, since the population estimates for the denominators are subject to error.
STD Control
Available control technology consists of early. effec-tive treatment of infected individuals and their sexual partners. Measures for case-finding include provision of acceptable, accessible health care services, screening programs for populations at high risk, contact-tracing services. and STD education for patients, sexual part-ners, at risk groups, and health care providers. The widespread use of standardized treatment schedules for diseases that can be easily treated must be stressed.
These technologies should be focused, adapted, and implemented to prevent STD complications. This is best
accomplished by preventing disease transmission, but in-terruption of disease transmission is not a prerequisite for eliminating or reducing complications. For example, congenital syphilis and gonococcal ophthalmia neona-torum can be eliminated through specific preventive measures, that is, prenatal serologic screening and ad-ministration of silver nitrate or antibiotic prophylaxis at birth, respectively. Gonococcal PID can be prevented
in part by early treatment of asymptomatic infected women.
In the Region of the Americas, only Canada, the United States, Costa Rica, and Cuba have implemented programs of national scope to control STD. In the United States. the national program focuses essentially on gonorrhea and syphilis. In Latin America and the Caribbean, control programs are spotty and limited generally to a few large cities, and depend on the interest and enthusiasm of a few clinical and public health leaders. They have been restricted, for the most part, to very selective interventions. such as prostitute screening and treatment for syphilis and antenatal serologic testing to prevent congenital syphilis.
The entire STD problem in areas of the Caribbean, Middle America, and South America needs careful epi-demiological investigation in order to identify the magnitude of the problem and the population groups at risk. With ever-increasing urban populations and con-comitant changes in social and cultural behavioral pat-terns, STD control efforts can no longer focus on tradi-tional prostitute control programs nor can they be limited to selected activities for one or two diseases.
(Source: Communicable Disease Control, Division of Disease Prevention and Control, PAHO.)
Table 4. Reported cases of congenital syphilisa under 1 year of age and rates per 100,000 population for selected countries, 1970-1979.
((llmllr, 910 19i 1972 1973 1974 1975 197). 1977 1978 1(979
B.li, Ca:lc 12 24 1. 15 21 29
Ipol) lJlai 19)0.70)1 19.0() 210).)7{) 2190.X)1 21X1.8(1) 2 21112.X)
lalc h.3 .. l 1 2.31 .109 5 7.1 1.1.7
{,(,oioIoa (£''a- t 225 422 431
B)tlIu '
-741) .91) 7(1.,1() 785. (X) 794.995 8.171
es9 99.5 5.1.- 54.8 35
C(ot: Ria (ia c 4 5'1 59 (,9
P~s~ qx~)ut la l{I~ *o 52
~.hO~2()
5.13. 895 h8, 58.312 .10Rals' 91.1 94.i 1(1.1 101.2
C(uba, Ca h 5 ( I ( 8 X 10 10
PI'oprlrar 1í b 2.125(X) 230.190 23,.990* 237.281 i.,05t 188.(9(0 191.320) 193.81)
Rate , 2 .. .1 - 4.2 4... 42 1.2 5.2
M xio-. C(:ac 40 3h 1 34 29 27 15
PoIp u latiro n 4 2.06() 2.134.(XX) 4. 2.2 9.(XX) 2,041.(XX) 2.277.(XX) 2.447.140
IRatc 2.2 1.7 1.5 1.4 40. 1.2
'1iTCdle SlíllCS
rl Aric¡,, (C 's, 345 451 3183 314 270) 1 8( 1h7 144 PI)pul a 1on 3.5(03.X)00 3.l79.(XX) 3.2M .(XX) 3.1,81 .(XX) 3.1( ,.(XX) 3.107h0.(XX .1.027.(XX) 3.171.i00
iRate, 9.8 12.h 11.7 11).2 9.( 5.9 5.5 4.5
aAll I corIled cases }[ syphilis tillder I Ycal, <1 age :rc a:,siuiimcd to, be rclgeclnital syphilirs.
I>
PAHO cinla:oic.
4