www.jped.com.br
ORIGINAL
ARTICLE
Translation,
cultural
adaptation,
and
validation
of
the
celiac
disease
DUX
(CDDUX)
夽
,
夽夽
Manuela
Torres
Camara
Lins
a,b,∗,
Rafael
Miranda
Tassitano
c,
Kátia
Galeão
Brandt
d,
Margarida
Maria
de
Castro
Antunes
d,
Giselia
Alves
Pontes
da
Silva
aaUniversidadeFederaldePernambuco(UFPE),Recife,PE,Brazil
bPediatricGastroenterologyService,InstitutodeMedicinaIntegralProf.FernandoFigueira(IMIP),Recife,PE,Brazil
cPhysicalEducationDepartment,UniversidadeFederalRuraldePernambuco(UFRPE),Recife,PE,Brazil
dMaternal-ChildDepartment,UniversidadeFederaldePernambuco(UFPE),Recife,PE,Brazil
Received5August2014;accepted12November2014 Availableonline6June2015
KEYWORDS
Qualityoflife; Cross-cultural adaptation; Celiacdisease
Abstract
Objective: Totranslate,cross-culturally adapt,andvalidateaspecificquestionnaireforthe evaluationofceliacchildrenandadolescents,theceliacdiseaseDUX(CDDUX).
Methods: The steps suggested by Reichenheim andMoraes (2007) were followed to obtain conceptual,item,semantic,operational,andmeasurementequivalences.Fourpediatric gas-troenterologists;aresearcherwithtoolvalidationbackground;threeEnglishteachers;and33 celiacpatients,aged8---18years,andtheircaregiversparticipatedinthestudy.Thescoresof celiacpatientsandthoseobtainedfromtheircaregiverswerecompared.Amongthepatients, thescoreswerecomparedinrelationtogenderandage.
Results: Allitemswereconsideredrelevanttotheconstructandgoodsemanticequivalence oftheversionwasacquired.Duringmeasurementequivalence,theexploratoryfactoranalysis showedappropriateweight ofall itemsandgoodinternalconsistency,withCronbach’s˛of
0.81.Significantdifferencewasfoundamongthefinalscoresofchildrenandtheircaregivers. Therewasnodifferenceamongthefinalscoresinrelationtogenderorage.
Conclusion: Thequestionnairewastranslatedandadaptedaccordingtoalltheproposedsteps, withallequivalencesadequatelymet.ItisavalidtooltoaccesstheQoLofceliacchildrenand adolescentsinthetranslatedlanguage.
©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:LinsMT,TassitanoRM,BrantKG,AntunesMM,daSilvaGA.Translation,culturaladaptation,andvalidationof theceliacdiseaseDUX(CDDUX).JPediatr(RioJ).2015;91:448---54.
夽夽
StudyconductedatUniversidadeFederaldePernambuco(UFPE),Recife,PE,Brazil.
∗Correspondingauthor.
E-mail:[email protected](M.T.C.Lins).
http://dx.doi.org/10.1016/j.jped.2014.11.005
PALAVRAS-CHAVE
Qualidadedevida; Adaptac¸ão transcultural; Doenc¸aCelíaca
Traduc¸ão,adaptac¸ãotransculturalevalidac¸ãodoCeliac Disease DUX (CDDUX)
Resumo
Objetivo: traduzir, adaptar transculturalmente e validar um questionário específico para avaliac¸ãodequalidadedevida(QV)decrianc¸aseadolescentescomdoenc¸acelíaca(DC), o CeliacDiseaseDUX(CDDUX).
Método: ForamseguidasasetapasdescritasporReichenheimeMoraes(2007)paraobtenc¸ãode equivalênciasconceitual,deitens,semântica,operacionaledemensurac¸ão.Participaramdo estudoquatrogastroenterologistaspediátricos,umprofissionalcomexperiênciaemvalidac¸ão deinstrumentos,trêsprofessoresdeinglêse33pacientescelíacos,entreoitoe18anos,com seusresponsáveis.ForamcomparadososescoresdeQVobtidosdospacientescomosobtidos atravésdosseusresponsáveis.Dentro dogrupodepacientes,compararam-seosescoresem relac¸ãoaosexoeidade.
Resultados: Todosositens foramconsiderados pertinentes ao construto,e foiatingida boa equivalênciasemântica daversão. Aanálise fatorialexploratóriademonstrou cargafatorial adequadadetodosositenseboaconsistênciainterna,com␣ deCronbachde0,81.Foi eviden-ciadadiferenc¸asignificativaentreoescorefinaldoCDDUXdecrianc¸aseseuspais.Nãohouve diferenc¸adoescorefinaldoquestionárioemrelac¸ãoaosexoouàidade.
Conclusão: Atraduc¸ãoeadaptac¸ãoseguiramadequadamenteasetapaspropostas,coma equiv-alênciasendoatingidademaneirasatisfatória.Oinstrumentotraduzidomostrou-seválidopara avaliac¸ãodaQVdecrianc¸aseadolescentescomDC.
©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Celiacdisease(CD)isanautoimmuneenteropathytriggered bygluten,which hasa greatvarietyof clinical manifesta-tionsandoccursingeneticallysusceptibleindividuals.The treatmentconsistsofremovingglutenfromthediet through-out life.1 The gluten-free diet is strict and, therefore,
difficulttoacceptandfollow,asitleadstomodificationof eatinghabitsandlifestyle,whichaffectspatientqualityof life(QoL).2Oncetreatmentisestablished,celiacindividuals
areasymptomatic, showingnoexternalsignindicating the presenceofthedisease.However,theneedtofollowa spe-cialdietgivesvisibilitytothedisease,putting patientsat riskofdenigrationandstigmatizationwithinthesocial con-text,withanegativeimpactontheQoLofthesepatients.3
The operational assessment of QoL is commonly per-formed through questionnaires, which can be generic, encompassing several domains and wide-ranging health problems,orspecific,evaluatingissuesinherenttoacertain groupofindividualsordisease.4
Several QoLassessment studies inchildren and adoles-centswithCDhave been publishedinthelastdecade,5---13
withthevalidationoftwospecificquestionnaires.Thefirst one,theceliacdiseaseDUX(CDDUX)7wasdevelopedby a
DutchpioneergroupinQoLstudiesinceliacindividualsand, in2013, Jordanetal.13 validateda questionnairefor U.S.
childrenandadolescents.
The development of an assessment tool is a time-consuming and costly task; therefore, performing the translation and adaptation of an existing questionnaire is a good option, following specific methodological rec-ommendations, which allows its use in different cultural contexts.14---16
The lack of a QoL assessment tool for celiac chil-drenandadolescentsvalidatedforuseinBrazilmotivated thisstudy, which aimed totranslate, adapt, and validate the(CDDUX),7 adisease-specific questionnaire for
health-relatedQoLassessmentforchildrenwithCD.
Methods
Thisisamethodologicalstudyoftranslation,cultural adap-tation,andvalidationofaquestionnaireforQoLassessment inceliacchildrenandadolescents.The processofcultural adaptation,performedfromMarchof2012toNovemberof 2013,followedtheequivalencestepsproposedby Reichen-heimandMoraes,15asfollows:(a)conceptual,(b)items,(c)
semantics,(d)operational,and(e)measurement.
The first two steps were carried out by a committee consistingoffourpediatricgastroenterologiststhat concep-tually verifiedthe relevance of the tool and the items it comprised.
meaningsof thewords wereverified,asthe literal corre-spondenceofatermdoesnotimplythatthesameemotional reactionisevokedindifferentculturalcontexts.
The pre-final version was tested with a group of five patientsandtheirparents/guardians,toassess the under-standing of the tool, and they were asked about the existence of any unintelligible words or questions. These five were included in the final group, which consisted of 33 celiac individuals, aged between 8 and 18 years, and 33 parents/guardianswho participated in the final stages ofthecross-culturaladaptationprocessofthetool.Among the celiac patients, most were aged between 8 and 11 years(66.7%),werewomen(72.7%),hadgoodreadingskills (81.8%),andreportedtheywerefollowingagluten-freediet (91.9%).Amongtheparents/guardians,mostofthe partici-pantsweremothers(84.8%),hadgoodreadingskills(81.8%), andhadapercapitafamilyincome<½ minimumwageat
thetimeofthestudy(69.7%).
AllpatientswerefollowedatthePediatric Gastroenter-ologyClinicofInstitutodeMedicinaIntegralProf.Fernando Figueira (IMIP), located in the city of Recife, which only treats patients from the Brazilian Unified Health System (SUS)whohavethediagnosisconfirmedbyapediatric gas-troenterologist andare instructed tofollow a gluten-free diet.
Theevaluationofthequestionnaireformat,theorderof appearanceof questions,and themanner and locationof questionnaireapplicationcomprisedtheoperational equiv-alence,performedbytwopediatricgastroenterologists,one withexperienceinresearchwiththisgroupofpatients.
The verification of the psychometric properties of the questionnaire corresponded to the measurement equiva-lence, focusing on the dimensional validity assessment, adequacyofitemsbydomain,andthetool’sinternal con-sistency.
The CDDUX consists of 12 items comprising three domains:Diet(6),Communication(3),andhavingceliac dis-ease(3).Afive-pointLikertscale isusedfortheanswers, aided by a picture diagram with faces expressing differ-ent emotional states related to the answers. There is also a questionnaire version to be answered by the par-ents/guardians about the children, containing the same questionsandansweroptions.7
Thescoresperitemcorrespondingtothepicture-answers rangedfrom1 to5;theoriginalauthorsusedacorrection factorineachquestiontoobtainameanfinalscoreranging from1to100,with1---20beingconsideredverypoorQoL, 21---40 poor, 41---60 neutral,61---80 good and81---100, very good.7
DataweretabulatedusingEpidatasoftware,release3.1 (EpidataAssoc.---Odense,Denmark),andallanalyseswere performed using SPSS 17.0 software (SPSS Inc., Chicago, USA).
SampleadequacywasassessedusingKaiser-Meyer-Olkin (KMO)index,resultinginavalueof0.64,withvalues>0.50 considered acceptable.17 Bartlett’s test of sphericity was
usedtoverifywhetherthecorrelationmatrixwasanidentity matrix.
Additionally, the authors sought to identify the exist-ence of multicollinearity (high correlation, r>0.80) and singularity (perfect correlation, r=1) between questions, using Spearman’s correlation coefficient. The correlation
wasperformed tomeettwoobjectives:toverifywhether the variables were linked to the others that comprised the domain, butwithout having an r>0.80, asthis would meanthesuppressionofoneoftheitemsandidentifiesin whichdomaineachitemshouldremain.Theitemswiththe highest correlation (p<0.05) remained intheir respective domain.
Anexploratoryfactoranalysiswasperformedusing pro-max rotationtoverify the factor loadingof each item of thescale. Eigenvalues≥1.0wereaccepted,in additionto itemswithfactorloading>0.4,inordertodefinethefactors obtained in the analysis. Internal consistency was deter-mined by Cronbach’s ˛, considering ˛ values≥0.7 to be
satisfactory.
Student’st-testwasusedtocomparethemeanscoreof the questionnaires applied tothe children and their par-ents/guardians. ANOVAwasusedtoverifythevariance of patients’meansinrelationtogenderandage.Forthis pur-pose,patientswerecategorizedinrelationtoageintotwo groups: between 8 and 11 years and between 12 and 18 years.
ThisstudywasapprovedbytheResearchEthics Commit-teeofInstitutodeMedicinaIntegralProf.FernandoFigueira (IMIP) (process no. 3420-13). All participating children signed the informed consent and their parents/guardians also signed the informed consent before the start of the study.Thecross-culturaladaptationwasauthorizedbythe researcherresponsiblefortheoriginalquestionnaire.7
Results
Thecommitteeofgastroenterologistsevaluatedallitemsas relevanttothedomainsandconstruct(QoL)inthecultural contextofthetargetpopulationandchosetomaintainall questionsinthefollowingsteps.
Thesemanticequivalencestepswereperformed satisfac-torily.Thetranslationsshowedtobeequivalent,andthere was a consensus between the translators in the develop-ment of the final translation. Table 1 shows the original questionnaireandthefinaltranslatedandadaptedversion. Theback-translationshowedgoodresemblancetothe orig-inal questionnaire, with a few modified terms. The term ‘‘find,’’whichappearsinseveralquestions,wastranslated as‘‘achar’’inPortuguese,butitwasdecidedtoreplaceitby ‘‘sentir’’(feel).Intheinstructions,bothtranslatorsshowed difficulty whentranslatingthe term‘‘faces’’ and,after a consensus, it was decided to translate it as ‘‘carinhas’’
(little faces). Also in the instructions, the phrase ‘‘there arenowronganswers’’wasremoved,initiallytranslatedas ‘‘nãoexistemrespostaserradas’’inPortuguese,soasnotto denoteasenseofevaluation,i.e.thatthepatientwasbeing tested.Inthewordingofthequestions,theterm‘‘express’’ wastranslatedby T1as‘‘expressar’’(express) andby T2 as‘‘mostrar’’(show).The term‘‘mostrar’’waschosento facilitateunderstanding.
Table1 OriginalquestionnaireandfinaltranslatedandadaptedversionofCDDUX.
Originalversion Finaltranslatedandadaptedversion
Wewouldliketoknowhowyoufeelthesedays Nósgostaríamosdesabercomovocêtemsesentidoessesdias Therefore,couldyoupleaseindicatehowyoufeelin
differentsituations?
Vocêpoderiaindicarcomosesenteemdiferentessituac¸ões?
Youcandothatbycirclingineachquestiononeofthe facesthatfitsyoubest.Therearenowronganswers; it’saboutwhatyoufeel
Vocêpodefazerissocirculandoemcadaperguntaacarinha quemostrecomovocêsesente.Nãohárespostascertasou erradas;trata-sedesabercomosesente
Pleaseexpresshowyou’vebeenfeelinglately. Porfavor,circuleacarinhaquemostracomovocêtemse sentidoultimamente.
1.WhenIthinkoffoodcontaininggluten,Ifeel... 1.Quandovocêpensaemcomidacomglúten,vocêsesente...
2.WhenatschoolIamgivenfoodcontaininggluten,I findit...
2.Quandonaescolalhedãocomidacomglúten,vocêsesente
...
3.Talkingaboutmycoeliacdiseasewithothersmyage, Ifind...
3.Quandoprecisafalarparaoutrosdasuaidadesobresua doenc¸acelíaca,vocêsesente...
4.Notbeingabletoeatjusteverything,Ifind... 4.Nãopodercomertudofazvocêsesentir...
5.WhensomeoneoffersmefoodthatIcan’thave,Ifeel
...
5.Quandoalguémlheoferececomidaquevocênãopode comer,vocêsesente...
6.WhenIhavetoexplaintootherswhatceliacdisease is,Ifeel...
6.Quandovocêtemqueexplicaraosoutrosoqueédoenc¸a celíaca,vocêsesente...
7.TalkingaboutceliacdiseaseIfind... 7.Quandosefalasobredoenc¸acelíaca,vocêsesente...
8.Havingtofollowalifelongdiet,Ifind... 8.Terqueseguirumadietaportodaavidafazvocêsesentir
...
9.HavingtopayattentiontowhatIeat,Ifind... 9.Terqueprestaratenc¸ãoaoquevocêcomefazvocêsesentir
...
10.Havingceliacdiseaseis... 10.Terdoenc¸acelíacaé...
11.NotbeingabletoeatanythingIwantlikeother people,Ifind...
11.Nãopodercomertudoquevocêquer,comoasoutras pessoas,fazvocêsesentir...
12.Followingadietformyceliacdiseaseis... 12.Terqueseguirumadietaporcausadasuadoenc¸acelíacaé
...
Also at this stage, it was decided to keep the origi-nal questionnaire format andthe orderof appearance of items.Thequestionnaireswereappliedinthe Gastroenter-ology Departmentconsultation offices where patients are followed, as patients were already familiarized with the environment.
Atthemeasurementequivalencephase,thesample ade-quacy test (KMO) showed a value of 0.64. Analyses of
singularity and multicollinearity showed adequate corre-lation values, as shown in Table 2, and all items were maintainedfortheexploratoryfactoranalysis.
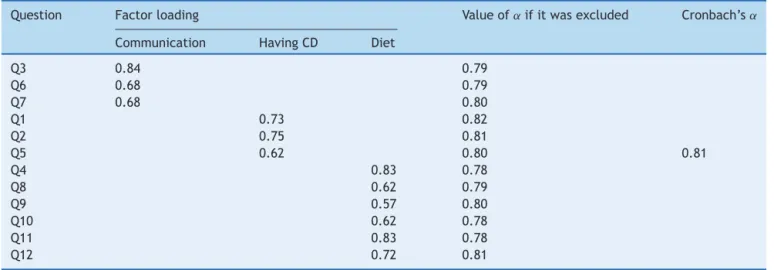
When analyzing the main components, the domains explained70.7%of the scale variance,withgood internal consistency,asshowninTable3,andtheexclusionofonly oneoftheitemswoulddetermineamodestincreasein Cron-bach’s˛value,whichwasnotsignificant.
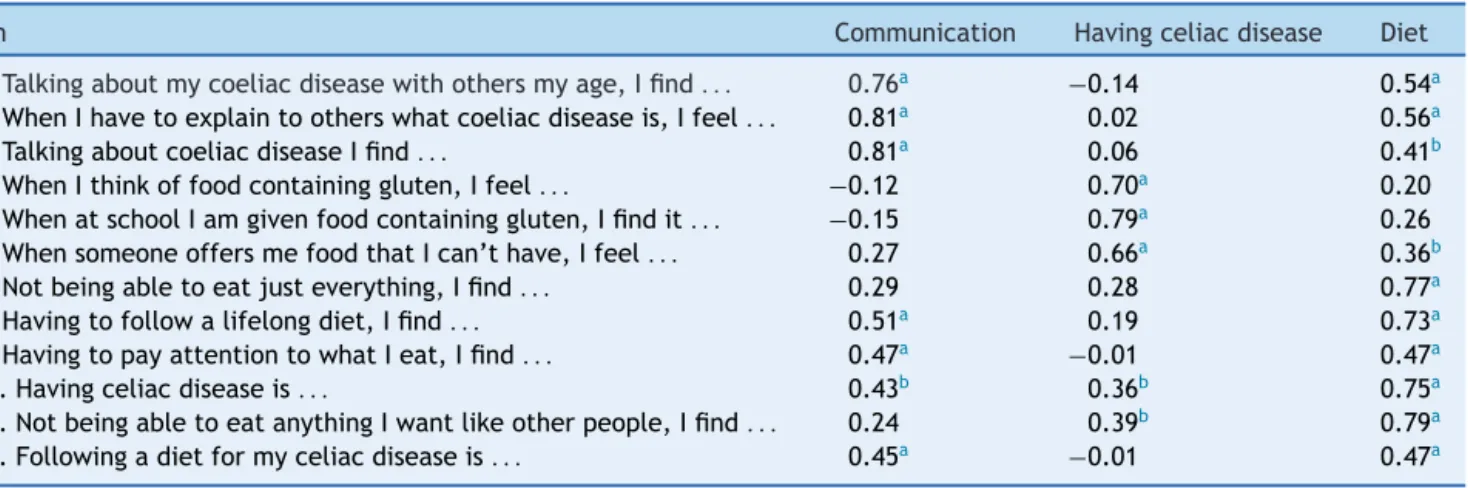
Table2 Spearman’scorrelationcoefficientbetweentheitemsofthetranslatedversionofCDDUXanditsdomains.
Item Communication Havingceliacdisease Diet
Q3.Talkingaboutmycoeliacdiseasewithothersmyage,Ifind... 0.76a −0.14 0.54a
Q6.WhenIhavetoexplaintootherswhatcoeliacdiseaseis,Ifeel... 0.81a 0.02 0.56a
Q7.TalkingaboutcoeliacdiseaseIfind... 0.81a 0.06 0.41b
Q1.WhenIthinkoffoodcontaininggluten,Ifeel... −0.12 0.70a 0.20
Q2.WhenatschoolIamgivenfoodcontaininggluten,Ifindit... −0.15 0.79a 0.26
Q5.WhensomeoneoffersmefoodthatIcan’thave,Ifeel... 0.27 0.66a 0.36b
Q4.Notbeingabletoeatjusteverything,Ifind... 0.29 0.28 0.77a
Q8.Havingtofollowalifelongdiet,Ifind... 0.51a 0.19 0.73a
Q9.HavingtopayattentiontowhatIeat,Ifind... 0.47a −0.01 0.47a
Q10.Havingceliacdiseaseis... 0.43b 0.36b 0.75a
Q11.NotbeingabletoeatanythingIwantlikeotherpeople,Ifind... 0.24 0.39b 0.79a
Q12.Followingadietformyceliacdiseaseis... 0.45a −0.01 0.47a a p<0.01.
Table3 FactoranalysisofthetranslatedversionofCDDUX.
Question Factorloading Valueof˛ifitwasexcluded Cronbach’s˛
Communication HavingCD Diet
Q3 0.84 0.79
Q6 0.68 0.79
Q7 0.68 0.80
Q1 0.73 0.82
Q2 0.75 0.81
Q5 0.62 0.80 0.81
Q4 0.83 0.78
Q8 0.62 0.79
Q9 0.57 0.80
Q10 0.62 0.78
Q11 0.83 0.78
Q12 0.72 0.81
CD,celiacdisease.
Table4 MeanfinalscoreandbydomainsofthetranslatedversionofCDDUXappliedtochildrenandadolescentswithceliac
diseaseandtheirparents/guardians.
Domain Childrenandadolescents Parent/guardian p
Mean SD Mean SD
CDDUX 57.6 12.3 45.4 10.4 <0.01
Havingceliacdisease 44.0 13.8 45.4 14.3 0.68
Communication 71.3 18.1 38.4 10.7 <0.01
Diet 57.6 16.7 52.3 14.1 <0.01
Asignificantdifferencewasobservedbetweenthemean finalscore of the questionnaire answered bythe children andtheir parents/guardians. When assessing the domains separately, only the domain ‘‘Having celiacdisease’’ was notsignificantlydifferentbetweenthetwogroups,asshown inTable4.
There was no difference between the means in the celiac group aged between 8 and 11 years (59.4±11.2) and between 12 and 18 years (54±14.3), with p=0.24; andbetween themeans of female(56.8±13.1)and male patients(59.9±10.3),withp=0.53.
Discussion
Based on the proposal of Reichenheim and Moraes,15 the
translation andcultural adaptation of CDDUX wascarried out,anditwasonlyavailablequestionnaireforQoL assess-mentinchildrenandadolescentswhenthestudystarted.It isknownthatagoodtranslationmaynotbeenoughto main-tainagoodconceptuallevelbetweendifferentculturesand adaptationsareoftennecessary.14,15,18
Inanattempttoanswerspecificquestionsofceliac chil-drenandadolescents,vanDoornetal.7developedCDDUX,
adisease-specifictool,divided intothreedomains:having celiacdisease,Communication,andDiet.
Davisetal.,19 inasystematicreviewoftheconceptual
basisof QoLassessment tools inchildren, suggestedthat, giventhegreatdiversityintheconceptualizationusedand
thesmallnumberofQoLtheoriesthathavebeenidentified, in additiontothe timerequiredtodevelop newtheories, theappropriatechoiceofdomainsanditemsisrequired.
Intheauthors’opinion,theCDDUXdomainscomprehend importantaspectsoftheassessmentofQoLofpatientswith CD,andalltheitemswereassessedasrelevantbythe com-mittee of gastroenterologists.However, other aspectsare notaddressed,suchasthedifficultyforobtainingaccessto gluten-freefoods,especiallyduringtimesofsocial interac-tion.ThisfactishighlightedbyJordanetal.,13 who,when
developing a questionnaire for U.S. celiacchildren, high-lightedotherrelevantissuesintheoriginalculturalcontext, suchastheregularconsumptionoffoodproduced outside thehomeanddifficultieseatinginleisure situations,such aswhentravelling.
Duringthesemanticequivalence,thechoiceofreplacing the term ‘‘find’’ by ‘‘feel’’ was based upon the under-standingofthetranslatorsandgastroenterologistsaboutthe needforthequestiontoevokenotonlyanopinion,butthe patient’s feelingin relationtotheaddressed issue.In the instructions,itwasdecidedtouse‘‘littlefaces’’replacing theterm‘‘faces’’,astheuseofthediminutiveformmakes theexplanationfriendlier.
Fromtheoperationalpointofview,theCDDUXformat, withanswersprovidedthrougha facediagram,facilitates itsapplication,avoidingproblems withwords thatrequire ahigherculturallevel,asfacedbyotherauthors.20 Unlike
that the performance of the interview by the attend-ing physician in the consultation environment may have affectedthefinalscoreofthequestionnaire.
At the measurementequivalence, the observed results indicated good correlation between the items and their domains,aswellasinternalconsistency.Allitemsshoweda significantcorrelation(p<0.01)withtheoriginallyproposed domains.Insome,suchasquestion3,asignificant correla-tionwithanotherdomaincanalsobeobserved,becausethey aresomehowinterrelated,butthiscorrelationwasfoundto bealwayslessthanorequaltothatofthedomaintowhich theitemisassigned.Itisalsonoteworthythatalthough sev-eralitemsnotassignedtoadomainarecorrelatedwithit, most of the items that comprise the domain have higher values.
The tool showed good internal consistency (˛=0.81),
althoughatalowervaluethantheevaluationoftheoriginal tool(˛=0.85).Regardingthefactorialanalysis,only
ques-tion9,‘‘Havingtopayattentiontowhatyoueat,makesyou feel...’’,whichbelongstodomain‘‘Diet,’’showedanitem
value<0.6.Astheexclusionofthisquestionwouldresultin a decreased˛ anditsvalue wasabovethe recommended
one(0.4),itwasdecidedtoretainit.
Reproducibilitycannotbeassessedduetothesmall num-berofpatientsthatattendedtheretest,althoughtheywere allinvitedtodoso.Returningtoperformtheretestseems tobemoreeasilyachievedwithmoresymptomaticclinical conditions.20
Traditionally in QoL studies, parents and guardians are responsible for their children, but they are seen as unreliable responders, as they lack language and cog-nitive capabilities.21 However, in this analysis of QoL,
the authors realize the need for subjective evaluation of the individual in question. Hence, the agreement between responses obtained from children and their parents/guardians through measurement tools has been investigated by some authors.21,22 The low agreement
betweentheanswers,whichsomeresearchersconsiderto beduetotoolinadequacy,mayreflectanatural disagree-ment betweenparents andchildren inmany aspects.The parents’capacitytoassesstheQoLoftheirchildrendepends onwhatQoLdomainsarebeingevaluated,astheyhave dif-ficultyassessingquestionsinternalizedbythechildren,such assadnessandanxiety.22
Although parents/guardians and CD patients classified QoLintheneutralrange(40---60),thefinalscoreofthe par-ents/guardians wassignificantly lower,in agreement with whatwasdescribedbyUptonetal.21inasystematicreview,
showingthatparentsofchildrenwithchronicdiseasestend to underestimate their children’s QoL. When the original toolwasapplied,thefinalscorewasalsosignificantlylower intheparents’assessmentandevenshowedtobeinanother classificationrange.7
However,thedifferencefound inscoresofparents and childreninthecommunicationdomainisnoteworthy.Talking aboutthediseaseandgivingitvisibilitycanhaveanegative impactonthesociallivesofthesechildren,duetopossible stigmatization.However,knowledgeaboutthediseasecan maketheactoflivingandeatinginenvironmentsoutsidethe homeaneasiertask,becauseceliacindividualsdonothave tojustifythefactthattheyhavedifferenteatinghabits.3
Inthissense,explainingandtalkingaboutCDcanbecomea
benefittoceliacchildrenandadolescents,unlikewhatwas predictedby their parents. This factwas notobserved in theoriginalstudy,7possiblybecausethelevelofknowledge
aboutCDinEuropeancountriesishigher.
As described in the literature, no differences were observed in the final score of the translated version of CDDUXinrelationtopatientgenderandage.10,11 However,
theuseofthesametoolinpatientswithinawideagerange isdebatable,astheyfacedifferentsituationsandperform differentsocialroles.13 Inthedevelopmentoftheoriginal
questionnairethrough focal groups, only four adolescents participatedinthestudy; thislimitationisemphasizedby theresearchers.7
Someaspectsmustbeconsideredwhenusingthis trans-lated and adapted version of the CDDUX. The present study interviewed a group of celiac patients followed at a specialized service, withlow socioeconomic status and that included few adolescents. The context in which the adaptation process occurs interferes with the version’s final result and this fact must be analyzed before its implementation.14,23
TheassessmentofQoLduringtheconsultation,evenin thepresenceofa well-establishedphysician---patient rela-tionship,isoftendifficult,especiallyinthosepatientswho tendtoprovidesociallycorrectanswers.AQoLassessment toolcanfacilitate thisapproachandcan beusedto initi-atecommunicationonthesubject,7althoughitshouldnot
replaceit.24
ThefinalversionofCDDUXinPortuguesewaspreparedin accordancewiththestepsoutlinedintheliterature,15with
adequatepsychometricproperties,representingavalidtool forQoLassessmentofchildrenandadolescentswithCD.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.FasanoA,CatassiC.Currentapproachestodiagnosisand treat-mentofceliacdisease:anevolvingspectrum.Gastroenterology. 2001;120:636---51.
2.Sverker A, Hensing G, Hallert C. ‘‘Controlled by food’’ --- lived experiences of coeliac disease. J Hum Nutr Diet. 2005;18:171---80.
3.OlssonC,LyonP,HörnellA,IvarssonA,SydnerYM.Foodthat makesyoudifferent: thestigma experiencedbyadolescents withceliacdisease.QualHealthRes.2009;19:976---84. 4.DuarteP,CiconelliR.Instrumentosparaaavaliac¸ãoda
quali-dadedevida:genéricoseespecíficos.In:SchorN,editor.Guia dequalidadedevida.SãoPaulo:Manole;2006.p.11---8. 5.KolsterenMM,KoopmanHM,SchalekampG,MearinML.
Health-relatedqualityoflifeinchildrenwithceliacdisease.JPediatr. 2001;138:593---5.
6.Rodrigues L[Dissertation] Avaliac¸ãodaqualidadedevida de crianc¸ascelíacasemusodedietaisentadeglúten:umestudo decaso-controle.PortoAlegre,RS:UniversidadeFederaldoRio GrandedoSul;2007.
8.Wagner G, BergerG,Sinnreich U,Grylli V,Schober E,Huber WD,etal.Qualityoflifeinadolescentswithtreatedcoeliac disease:influenceofcomplianceandageatdiagnosis.JPediatr GastroenterolNutr.2008;47:555---61.
9.RosénA,IvarssonA,NordykeK,KarlssonE,CarlssonA, Daniels-son L, et al. Balancing health benefitsand social sacrifices: a qualitative study of how screening-detected celiac dis-easeimpactsadolescents’ qualityoflife.BMC Pediatr.2011; 11:32.
10.ByströmIM,HollénE,Fälth-MagnussonK,JohanssonA. Health-related quality of life in children and adolescents with celiac disease: from the perspectives of children and par-ents. GastroenterolRes Pract.2012;2012. ArticleID986475, 6pages.
11.deLorenzoCM,XikotaJC,WayhsMC,NassarSM,deSouzaPires MM.Evaluationofthequalityoflifeofchildrenwithceliac dis-ease and theirparents:a case---controlstudy.Qual Life Res. 2012;21:77---85.
12.Nordyke K, Norström F, Lindholm L, Stenlund H, Rosén A, Ivarsson A. Health-related quality of life in adolescents withscreening-detectedceliacdisease, beforeand one year afterdiagnosis and initiation ofgluten-free diet,a prospec-tivenestedcase-referentstudy.BMCPublicHealth.2013;13: 142.
13.JordanNE,LiY,MagriniD,SimpsonS,ReillyNR,DefeliceAR, etal.Developmentandvalidationofaceliacdiseasequality oflifeinstrumentforNorthAmericanchildren.JPediatr Gas-troenterolNutr.2013;57:477---86.
14.GuilleminF,BombardierC,BeatonD.Cross-culturaladaptation ofhealth-relatedqualityoflifemeasures:literaturereviewand proposedguidelines.JClinEpidemiol.1993;46:1417---32.
15.Reichenheim M, Moraes C. Operacionalizac¸ão de adaptac¸ão transculturaldeinstrumentosdeaferic¸ãousadosem epidemi-ologia.RevSaudePublica.2007;41:665---73.
16.Herdman M,Fox-Hushby J, Badia X. ‘‘Equivalence’’and the translationandadaptationofhealth-relatedqualityoflife ques-tionnaires.QualLifeRes.1997;6:237---47.
17.PereiraA.SPSS---Guiapráticodeutilizac¸ão:análisededados paraasciênciassociais epsicologia. 7thed.Lisboa: Edic¸ões Silabo;2008.
18.BeatonDE,BombardierC,GuilleminF,FerrazMB.Guidelines fortheprocessofcross-culturaladaptationofself-report meas-ures.Spine.2000;25:3186---91.
19.Davis E, Water E, Mckinnon A, Reddihough D, Graham HK, Mehmet-RadjiO,etal.Paediatricqualityoflifeinstruments:a reviewoftheimpactoftheconceptualframeworkonoutcomes. DevMedChildNeurol.2006;48:311---8.
20.La Scala CS, Naspitz CK, Solé D. Adaptac¸ão e validac¸ão do PediatricAsthma QualityofLifeQuestionnaire (PAQLQ-A)em crianc¸aseadolescentesbrasileiroscomasma.JPediatr(RioJ). 2005;81:54---60.
21.Upton P,Lawford J, Eiser C.Parent---child agreement across childhealth-relatedqualityoflifeinstruments:areviewofthe literature.QualLifeRes.2008;17:895---913.
22.EiserC,MorseR.Canparentsratetheirchild’shealth-related qualityoflife?Resultsfromasystematicreview.QualLifeRes. 2001;10:347---57.
23.SilvaFG,SilvaCR, BragaLB, Neto AS.PortugueseChildren’s SleepHabitsQuestionnaire---validationandcross-cultural com-parison.JPediatr(RioJ).2014;90:78---84.