ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Review
article
Cyclophosphamide
administration
routine
in
autoimmune
rheumatic
diseases:
a
review
夽
Kaian
Amorim
Teles
a,∗,
Patricia
Medeiros-Souza
a,b,∗,
Francisco
Aires
Correa
Lima
c,
Bruno
Gedeon
de
Araújo
d,
Rodrigo
Aires
Correa
Lima
e,faUniversidadedeBrasília(UnB),DepartamentodeCiênciasdaSaúde,Brasília,DF,Brazil bUniversidadeEstadualdeCampinas(Unicamp),Campinas,SP,Brazil
cUniversidadedeBrasília(UnB),HospitalUniversitáriodeBrasília,Servic¸odeReumatologia,AmbulatóriodeColagenoses,Brasília,DF,
Brazil
dHospitalUniversitáriodeBrasília(HuB),Brasília,DF,Brazil
eUniversidadedeBrasília(UnB),HospitalUniversitáriodeBrasília,Servic¸odeReumatologia,Brasília,DF,Brazil
fHospitaldeBasedoDistritoFederal,Servic¸odeReumatologia,AmbulatóriodeArtriteReumatoideInicial,Brasília,DF,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received2August2013 Accepted7April2016
Availableonline24October2016
Keywords:
Cyclophosphamide Antiemetics Chemotherapy Cystitis
a
b
s
t
r
a
c
t
Cyclophosphamideisanalkylatingagentwidelyusedforthetreatmentofmalignant neo-plasiaandwhichcanbeusedinthetreatmentofmultiplerheumaticdiseases.Medication administrationerrorsmayleadtoitsreducedefficacyorincreaseddrugtoxicity.Manyerrors occurintheadministrationofinjectabledrugs.Thepresentstudyaimedatstructuringa routineforcyclophosphamideuse,aswellascreatingadocumentwith pharmacotherapeu-ticguidelinesforthepatient.Theroutineisschematizedinthreephases:pre-chemotherapy, administrationofcyclophosphamide,andpost-chemotherapy,takingintoaccountthedrugs tobeadministeredbeforeandaftercyclophosphamideinordertopreventadverseeffects, includingnauseaandhemorrhagiccystitis.Adversereactionscanalterlaboratorytests; thus,thisroutineincludedclinicalmanagementforchangesinwhitebloodcells,platelets, neutrophils,andsodium,includingcyclophosphamidedoseadjustmentinthecaseof kid-neydisease.Cyclophosphamideisresponsibleforotherrare–butserious–sideeffects,for instance,hepatotoxicity,severehyponatremiaandheartfailure.Otheradversereactions includehairloss,amenorrheaandmenopause.Inthisroutine,wealsoenteredguidelines topost-chemotherapypatients.Thecompatibilityofinjectabledrugswiththevehicleused hasbeendescribed,aswellasstabilityandinfusiontimes.Theroutineaimedattherational useofcyclophosphamide,withpreventionofadverseeventsandrelapseepisodes,factors thatmayburdenthehealthcaresystem.
©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheServic¸odeReumatologia,HospitalUniversitário,UniversidadedeBrasília,Brasília,DF,Brazil. ∗ Correspondingauthors.
E-mails:[email protected](K.A.Teles),[email protected](P.Medeiros-Souza). http://dx.doi.org/10.1016/j.rbre.2016.09.008
Rotina
de
administrac¸ão
de
ciclofosfamida
em
doenc¸as
autoimunes
reumáticas:
uma
revisão
Palavras-chave:
Ciclofosfamida Antieméticos Quimioterapia Cistite
r
e
s
u
m
o
Aciclofosfamidaéumagentealquilantevastamenteusadoparaotratamentodeneoplasias malignasepodeserusadonotratamentodediversasdoenc¸asreumatológicas.Oerrode administrac¸ãodemedicamentospodelevaràdiminuic¸ãodaeficáciaouaoaumentoda toxicidademedicamentosa. Diversoserrosocorremnaadministrac¸ãodemedicamentos injetáveis.Otrabalhoobjetivouaestruturac¸ãodeumarotinadousodeciclofosfamida,bem comoacriac¸ãodeumdocumentodeorientac¸õesfarmacoterapêuticasparaopaciente.A rotinafoiesquematizadaemtrêsfases,apré-quimioterapia,aadministrac¸ãoda ciclofos-famidaeapós-quimioterapia,quelevaramemconsiderac¸ãoosmedicamentosquedevem seradministradosantesedepoisdaciclofosfamidaparaprevenc¸ãoaosefeitosadversos, incluindo náusea ecistite hemorrágica. Asreac¸õesadversas podemalterar os exames laboratoriaisearotinaincluiumanejoclínicoparaalterac¸ãoclínicadosleucócitos,das plaquetas,dosneutrófilosedosódioincluindooajustededosedeciclofosfamidaemcaso deinsuficiênciarenal.Aciclofosfamidaéresponsávelporoutrasreac¸õesadversasraras, massérias,comohepatotoxicidade,hiponatremiaseveraefalênciacardíaca.Outrasreac¸ões adversasincluemperdadecabelo,amenorreiaemenopausa.Arotinafoicomposta tam-bémpororientac¸õesaopacientepós-quimioterapia.Acompatibilidadedosmedicamentos injetáveiscomoveículofoidescrita,bemcomootempodeestabilidadeeotempodeinfusão. Arotinavisouaousoracionaldaciclofosfamidaeprevenirosefeitosadversoseosepisódios derecidiva,osquaispodemonerarosistemadesaúde.
©2016ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Cyclophosphamide(CPM)isanalkylatingagentwidelyused for the treatment of malignancies such as breast cancer,1 multiplemyeloma,2renaldiseasesincludingnephrotic
syn-drome refractory to corticosteroid and focal segmental
glomerulonephritis,andthis drugcanbeusedinthe treat-mentofmultiplerheumaticdiseases,3–5 includingcicatricial
pemphigoid (also called pemphigoid mucous membrane),4
rheumatoid arthritis,5 juvenile dermatomyositis,6 systemic sclerosis,7,8 interstitial lung disease,7 lupus vasculopathy,9
systemic vasculitis, and refractory treatment of
lupus-associatedthrombocytopenicpurpura.10Inadditiontoother
indications of cyclophosphamide, the treatment of
neu-romyelitisopticacanalsobeincluded.11
In children, cyclophosphamide may be used in the
treatment of nephrotic syndrome and systemic lupus
erythematosus.12,13
Cyclophosphamidecanbeadministeredbyoralor
intra-venous route.14 The intravenous administration is more
frequentin the field ofrheumatology, taking into account studies showing an efficacy similar to that of oral treat-ment, but with less toxicity, for example, a decrease in premature ovarianfailure, less severe infection, and lower overall exposure of the urinary tract to acrolein, a toxic
metabolite of cyclophosphamide.15 Cyclophosphamide is
orallyadministeredQD(24–24h),whiletheintravenousroute isadministeredinpulses,andthedoseisadjustedaccording tohematologicandrenaltoxicities.16
Theadministration ofcyclophosphamideinpulses may
follow a weekly or monthly basis, in combination with
a corticosteroid and other chemotherapeutic agents, pro-vided that the attending physician takes into account the
minimum blood count (NADIR) for the administration of
cyclophosphamide.16–18Cyclophosphamidemaycausesome
adverseevents,andwhentheseeffectsarerelatedtothedrug, areclassifiedasanadversedrugreaction.19Theadversedrug reactioncanbeconceptualizedasanunintendedandharmful reactionintothebody,occurringinthoseroutinelyuseddoses inhumansforprophylaxis,diagnosis,diseasetherapy,orfor changesofphysiologicalfunctions.19
Areactionthatoccursinasmallpercentageofthe popu-lation,butthat,ifnotavoided,maycauseirreversibledamage tothepatient,suchasdeath,congenitalabnormalities,birth defectsorconditionsthatrequirepermanenthospitalization, isclassifiedas“severereaction”.19
Someadverse reactionsrelated totheadministrationof
cyclophosphamide are bone marrow suppression,
suscep-tibility to infections, sterility and amenorrhea,18 as well as nephrotoxicity and cystitis,18,19 and also cardiovascular complications, for instance, sinus bradycardia, pericarditis, myocarditis and heart failure.20 Children and adolescents treatedwithhighdosesofcyclophosphamidearemorelikely to develop dental disorders and a decreased salivary flow. Cyclophosphamideisalsoteratogenic.21Alongtermreaction ofcyclophosphamideismalignacies.18 Onecanobserve an increaseintheincidenceofbladdercancerandesophageal
and lung adenocarcionoma, which customarily occur after
Inadditiontoadversedrugreactionsofcyclophosphamide, itiscriticalthatthephysicianadoptallprecautionary meas-ures,becausetheseadversereactionsmaybemoreimportant
in cases where cyclophosphamide is administered
intra-venously,giventhat, withthis routeofadministration,the drug isnotabsorbed, the onset ofits actionisfaster and, becausethedrugdoesnotundergofirst-passmetabolism,the bioavailability, i.e.the bioavailableconcentrationtoexert a pharmacologicalaction,becomesproportionallyhigher ver-sus oral administration of cyclophosphamide.22,23 Another importantaspecttoconsiderconcernstheerrorsassociated withtheadministrationofinjectabledrugs.24
It is known that the use of injections is often associ-ated with medication errors classified as serious events.22 Intravenous-route administrationerrors represent 21.1% of all errors, with possible risk of errors of contamination, administration rate, and dilution.25 Such parenteral drug administrationerrors,especiallythosebyintravenousroute, cancauseanadversedrugreaction.19
Inadditiontohealth-relatedproblems,itisrequiredthat thecostsresultingfromdrugadministrationerrorsaretaken intoaccount. InBrazil,it isestimatedthattheannual cost withthe use of chemotherapeutic drugsexceed 1.1billion reais,andthisvaluecanincreaseincasesofinjectabledrug administrationerrors.24
Thus,onemustbearinmindthatthesecostsmaybe mag-nifiedbytheoccurrenceofadverseevents.26Anadverseevent isanyuntowardmedicaloccurrencethataffectsthepatient beingmedicated,butwithoutadirectcausalrelationshipwith his/hertreatment.19
Thus,itisimportanttostandardizetheadministrationof parenteraldrugsandprovidetheirrationaluse,whichcanbe definedasthepatient’sneedtoreceivetheappropriatedrug inthecorrectdosageforanadequatelengthoftimeandwith thelowestcost.27
Takingintoaccounttherationaluseofdrugs,itis impor-tanttostandardizerulesfortheparenteraladministrationof cyclophosphamide.Theobjectivesofthisstudyareproposing acyclophosphamideadministrationroutineinRheumatology units, andthe creation ofadocumentcontaining pharma-cotherapeuticguidelinesforthepatient,inordertomaximize theefficiencyoftreatmentbasedonaliteraturereview.
Methods
Cyclophosphamideroutine
Aninfusionroutineforcyclophosphamidewasdevelopedin ordertoincreasethebioavailability(effectiveness)ofthisdrug whileminimizingadversereactions,thusrenderingthe treat-mentmoretolerableforthepatient.Theprotocolwasdivided intostagestofacilitatethecomprehensionofthehealthstaff andthereplicationofthecyclophosphamidedosing sched-ule. The drugs of the first (pre-ChT) and third (post-ChT) stepscorrespondtotheadministrationofpharmaceuticalsin ordertopreventthemainadversereactionsresultingfromthe administrationofcyclophosphamide(secondphase), includ-ingnausea,vomiting,andhemorrhagiccystitis.Theclinical
management of adverse reactions that change laboratory
testswas described,aswellasthe clinicalmanagementof cyclophosphamide in renal failure. The rare, but serious, adversereactionswerealsohighlighted.
The most common adverse reactions were emphasized
sothattheattendingphysiciancouldprovideguidancewith respecttothemaincarethatthepatientshouldtakeinhis/her home,afteradministrationofcyclophosphamide.These pre-cautionsareessentialtopreventorminimizeadverseeffects andincreasetreatmentadherence.
Inaddition,thecompatibilityoftheseinjectabledrugswith thevehicle,stabilitytime,andinfusiontimewasascertained. Thesequenceofadministrationofthesedrugshasbeen pre-paredinordertoincreasetheefficacyofcyclophosphamide and diminish the onset of adverse reactions to the drugs administered.
Results
Theroutineadministrationofcyclophosphamidewas
devel-oped in three phases: pre-ChT, cyclophosphamide
admin-istration, and post-ChT. With a view to the prevention of hemorrhagiccystitis,intravenoushydrationwithablood vol-umeexpander(acrystalloid:0.9%saline)wasstandardized.28 In addition,the drugadministrationsequence,the amount ofdiluent,theneed(orotherwise)fordilution,infusionand administrationtimes,and laboratorytestswhichshouldbe monitoredbeforeandaftertheinfusionofcyclophosphamide wereindicated,aswellastheguidelinestothepatient.
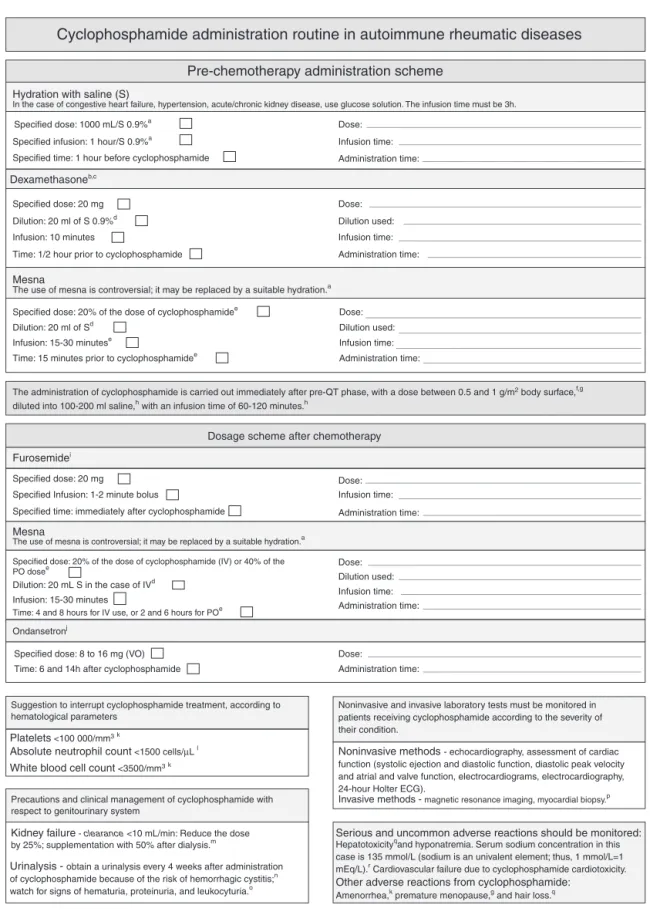
Fig. 1 3,5,20,29–42, lists the routine data, and Fig. 2 44–50 describestheguidelinesforthepatient.Severeand
uncom-mon adverse reactions which should be monitored are
hepatotoxicity,3hyponatremia45(inthiscase,serumsodium level=135mmol/L [sodium is an univalent element; thus, 1mmol/L=1mEq/L)],45 and cardiovascular failure due to cyclophosphamidecardiotoxicity.36
Other adverse reactions from cyclophosphamide are
amenorrhea,18earlymenopause,46andhairloss.3
Discussion
Drug administration errors can decrease the effectiveness
of the pharmacological treatment and increase both the
occurrence of adverse reactions and the financial costs of treatment.24Aretrospectivestudyconductedinhospitalsin Spainbetween2008and2010evaluatedtheincidenceofcost and adverse event. 245,320 episodes were identified, with anoverallcostof1,308,791.97euros.Approximately6.8%of patients experiencedadverse events,representinga riseof 16.2%incosts.Sixofthe tenadverseeventsthatburdened moresignificantlythehospitalsystemoccurredinthe oper-atingroom,correspondingtoanincreaseofexpensesaround 6.7%tothehealthsystem.26
A prospective study conducted between August and
November 1999 and between January and May 2000
Cyclophosphamide administration routine in autoimmune rheumatic diseases
Pre-chemotherapy administration scheme
Hydration with saline (S)
In the case of congestive heart failure, hypertension, acute/chronic kidney disease, use glucose solution. The infusion time must be 3h.
Specified dose: 1000 mL/S 0.9%a
Dexamethasoneb,c
Dose:
Specified infusion: 1 hour/S 0.9%a
Specified time: 1 hour before cyclophosphamide
Time: 1/2 hour prior to cyclophosphamide
The use of mesna is controversial; it may be replaced by a suitable hydration.a
The administration of cyclophosphamide is carried out immediately after pre-QT phase, with a dose between 0.5 and 1 g/m2 body surface,f,g diluted into 100-200 ml saline,h with an infusion time of 60-120 minutes.h
Mesna
The use of mesna is controversial; it may be replaced by a suitable hydration.a
Suggestion to interrupt cyclophosphamide treatment, according to hematological parameters
Precautions and clinical management of cyclophosphamide with respect to genitourinary system
Kidney failure - clearance <10 mL/min: Reduce the dose by 25%; supplementation with 50% after dialysis.m
Urinalysis - obtain a urinalysis every 4 weeks after administration of cyclophosphamide because of the risk of hemorrhagic cystitis;n watch for signs of hematuria, proteinuria, and leukocyturia.o
Mesna
Specified dose: 20 mg
Specified dose: 20% of the dose of cyclophosphamidee Dilution: 20 ml of Sd
Specified dose: 20 mg
Specified Infusion: 1-2 minute bolus
Specified time: immediately after cyclophosphamide
Time: 4 and 8 hours for IV use, or 2 and 6 hours for POe
Specified dose: 20% of the dose of cyclophosphamide (IV) or 40% of the PO dosee
Dilution: 20 mL S in the case of IVd Infusion: 15-30 minutes
Specified dose: 8 to 16 mg (VO) Time: 6 and 14h after cyclophosphamide
Platelets <100 000/mm3k
Absolute neutrophil count <1500 cells/µL l
White blood cell count <3500/mm3k Infusion: 15-30 minutese
Time: 15 minutes prior to cyclophosphamidee
Dose:
Infusion: 10 minutes Dilution: 20 ml of S 0.9%d
Dose: Dilution used:
Dose:
Dose: Dilution used: Infusion time:
Administration time:
Infusion time:
Ondansetronj
Noninvasive and invasive laboratory tests must be monitored in patients receiving cyclophosphamide according to the severity of their condition.
Noninvasive methods - echocardiography, assessment of cardiac function (systolic ejection and diastolic function, diastolic peak velocity and atrial and valve function, electrocardiograms, electrocardiography, 24-hour Holter ECG).
Serious and uncommon adverse reactions should be monitored:
Hepatotoxicityqand hyponatremia. Serum sodium concentration in this case is 135 mmol/L (sodium is an univalent element; thus, 1 mmol/L=1 mEq/L).r Cardiovascular failure due to cyclophosphamide cardiotoxicity.
Other adverse reactions from cyclophosphamide:
Amenorrhea,k premature menopause,g and hair loss.q
Invasive methods - magnetic resonance imaging, myocardial biopsy.p Administration time:
Dose:
Administration time: Infusion time:
Dosage scheme after chemotherapy
Furosemidei
Administration time: Dilution used:
Infusion time: Infusion time:
Administration time:
Administration time:
Fig.1–Cyclophosphamideadministrationroutineinautoimmunerheumaticdiseases.
Sources:aShepherdetal.29;bHawthorn;eCunningham30;cJordanetal.31;dTurneretal.32;eTrissel33;fHaubitzetal.34;
gMardeganetal.35;hDiLisietal.36;iSalidoetal.37;jCalixto-Limaetal.38;kLotanetal.20;lZahnetal.39;mMilman40;nMota
Water intake - the physician should instruct the patient to drink at least two liters of water a day unless in the presence of a kidney condition; thus, the amount of water to be consumed should be individualized. Imprensa electrolytes in the blood.a
Instructions for preventing mucositis - cyclophosphamide can cause mucositis; some precautions are advisable and these should be taken by the patient to minimize risks, including brushing adequately his/her teeth after a meal, using a soft brush and a non-abrasive toothpaste (for children), avoiding alcohol and cigarettes, avoiding too much salt, choosing soft foods, giving preference to food in the form of puddings, porridges, vitamins, gelatin, and caloric-, protein-rich meat, chicken or fish soup.b,c
Clinical management for symptoms of nausea - the patient should eat before getting hungry, with small, frequent (2-2 hours), slowly eaten meals because hunger can increase nausea; also, should avoid very spicy, fatty and sweet food and hot food and drinks. On the other hand, the patient should avoid drinking liquids during meals and should stay away from the kitchen during food preparation, eating in a ventilated and pleasant environment.b
Guidelines for patients with anemia - the patient should consume foods of animal origin such as chicken, fish and especially red meat, and should consume legumes and dark green vegetables such as kale, broccoli and spinach, pea beans and other grains, and combine vegetables with sources of vitamin C (orange, mandarin [tangerine], lemon, acerola). Milk, cheese, cottage cheese, yogurt and other dairy products should be avoided during or close to lunch or dinner time.d,e
Guidelines for disposal of urine and faeces - on the appointed day to take cyclophosphamide and on the next two days, when using the toilet the patient should flush three times with the cover closed. If someone else is responsible for the cleaning of the patient’s excreta, this person should wear gloves and use disposable material. The cleaning procedure must be done in a outside-inside manner; and all content should be placed in two plastic bags, which will then be tightly closed. Cleaning should be completed with bleach.f,g
Guidelines for bathing - the patient must first wash his/her hands, then the face and head. Next, the stomach, back, arms and the catheter (if in use of one of these devices).
Fig.2–Guidelinesforthepatienttakingcyclophosphamide.
Sources:aInstitutoEstadualdeHematologiaArthurdeSiqueira44;bBruiningetal.45;cGonzálezetal.46;dOteroLópez47;
eMedeiros-Souzaetal.48;fMesna49;gTaketomoetal.50.
(3.3%) were due to intoxication. According to the criteria (modified)ofSchumock andTornton,68.4% ofdrug-related problemsareconsideredaspreventable.47
Thecyclophosphamidedosingscheduletookintoaccount
the most common adverse reactions, the administration’s
strategyinthe caseofkidney failure, andthe sequence in theadministrationofpre-ChTdrugs,cyclophosphamide,and post-ChT drugs; tothis end, the dosageofall medications used,theirdilutionandinfusiontimealsowereincluded.
Themainclinicalstrategiesinthefaceofadversereactions
from cyclophosphamide use included the care of
hemor-rhagiccystitis,nausea,andvomiting.18Theadministrationof thesedrugscorrespondstowhatisdefinedasaqualitative polypharmacy, whereinthe administrationofamedication
is performed to correct the adverse reaction of another
medication.48
Several clinical strategies have been proposed to avoid hemorrhagic cystitis, including increased hydration of the patientandtheadministrationofmesnaandfurosemide.28,29 Inthosecasesinwhichthepatientsuffersofaseverekidney impairment,itispreferabletoadministermesnainplaceof hydration,duetothepatient’swaterrestriction.20,29
For the prevention of hemorrhagic cystitis, mesna
is administered in a dose equivalent to 60% of
cyclophosphamide, divided into three doses – 20%
15min before the administration of cyclophosphamide,
20% after cyclophosphamide, and 20% 4 or 8h after
cyclophosphamide.28 Mesnareducesthedepositofacrolein
(a metabolite of cyclophosphamide) in the bladder, thus
preventinghemorrhagiccystitisandbladdercancer.18 Inordertodecreasetheexposureoftheurinarytractto acrolein,thepatientshouldbewellhydratedbefore,during andaftertheadministrationofcyclophosphamide.Thus,at the time ofhis/her admission, the patient should receive, throughavenousaccess,1Lofabloodvolumeexpander(a crystalloid:saline0.9%)for1h,60minbeforethe administra-tionofcyclophosphamide.51
Cyclophosphamidepersecanbeadministeredatanytime. Inturn,theinfusionofmesnadependsontheadministration ofcyclophosphamide.28Mesnamaybeadministeredbyoral orparenteral(subcutaneousorintravenous)route.28
mesna would havealsothe advantageofa likelydecrease
in expenses, due the lower bed occupancy time and less
workloadofthenursingteam.51Stillinthiscontext,another possibledisadvantageisthepatient’snon-compliance;thus, onecannotbesurethatthepatienthastaken,orotherwise, thelastdoseofmesnaPO.52
TheadvantageoftheuseIVmesnaisthatthereisnoneed ofabsorption,andtheonsetofactionofthisdrugisfaster, comparedwithoraladministration.22,23,53Thedisadvantage oftheparenteralrouteisthegreaterriskofcontamination, administrationerrors,lessdosingconvenience,andincrease ofthepatient’shospitalstay.23,53
However,mesna administrationwitha viewto the pre-ventionofhemorrhagiccystitisinpatientsusing
cyclophos-phamide in therapeutic doses for rheumatic diseases is
controversial; thus, mesna may be replaced by a suitable hydrationwith6Lofwaterperday,plusadiureticdrug,or theuseofhydrationwithavolumeof3L/m2perday.54
Furosemideisadministeredaftercyclophosphamide infu-sionatadoseof20mg,inordertostimulatediuresisthat, insynergismwithmesna,decreasestheexposureof urothe-liumtotheactionofacrolein.55Themaximumconcentration offurosemideis10mg/mLadministeredinbolus,achieving atherapeuticconcentrationof10mg/mLperminute.55 The
second dose ofmesna (20% of cyclophosphamidedose) is
administeredintheintervalbetween15and30minafterthe administrationofcyclophosphamide.28
Nauseaandvomitingareconsideredascommonadverse
reactions in chemotherapy, and this also occurs with
cyclophosphamide31 which, in turn, participates of many chemotherapeuticregimens.Inthiscase,aroutinehasbeen proposed forthe treatment of rheumaticdiseases. Nausea causedbytheexclusiveadministrationofcyclophosphamide (withoutatherapeuticscheme)isclassified asalate-onset nausea.56Thus,ondansetronwasnotrequiredtopreventthis effect.56Adecreaseineffectivenessisanotherreasonfornot usingondansetronpriortocyclophosphamide.57
Thisreductioninefficacyoccursbecauseondansetronisan inhibitorofCYP2B.58Thisoccursbecausecyclophosphamide isaprodrug thatmust beactivatedby CYP2B,resulting in
4-hydroxycyclophosphamide and aldophosphamide. These
metabolitesaretransportedtothesiteofaction,wherethey
undergo spontaneous cleavage, producing phosphoramide
mustard,responsible forthe pharmacologicaleffectsofthe drug.58
Moreover,dexamethasonewasaddedpriorto chemother-apy,asaprophylacticagenttoanaphylacticshockandalso as an antiemetic.59 Preferably, dexamethasone should be administered so that its peak coincides with the peak of physiologicalcorticosteroids,whichnormallyoccursat8a.m. and16p.m.58 Apeakindexamethasoneplasma concentra-tionoccurswithin60min,anditsactionbeginsin30min.55,60 Thus,theadministrationofdexamethasoneshouldbestarted inthemorning,30minbeforetheadministrationof cyclophos-phamide,preferablyat7:30a.m.58
Afterthe emesiscausedbycyclophosphamidewas clas-sified as a delayed-type,56 and in view of the decrease of
cyclophosphamide efficacy when ondansetron is
adminis-teredpriortothischemotherapeuticagent,ondansetron(8mg PO31,61 administered at 6 and 14 or 8 and 16h post-ChT,
andwithamaximumdoseof16mgafterchemotherapy,not exceeding32mgperday)wasthelastdrugusedforthe pro-phylaxisofemesiscausedbycyclophosphamide.31
Other important adverse effects of
cyclophos-phamide include hematologic toxicity,18 kidney failure,20 hyponatremia,45,62neurologicalimpairment,45amenorrhea,18 early menopause,46 hair loss,3 hepatotoxicity (rare),3 and
late-onset cancer.18 The dose of cyclophosphamide for
the treatment of systemic lupus erythematosus, including
those patients with neuropsychiatric and/or hematologic
disorders, with class IV lupus nephritis, and with other
serious manifestations of systemic lupus erythematosus,
is 0.5–1g/m2 IV monthly,5,62 with dosage adjustment in patientswithhematological toxicityandkidneyfailure.20,63 Adversehematologicreactionscausedbycyclophosphamide are classified as serious,as theycause high morbidity.19,64
NADIRistheminimumhematologiccountingthatmustbe
observed tosee if the patient may or may notembark on
another chemotherapeuticcycle.65 Themainhematological tests include platelets, neutrophils, white blood cells and neutrophil counts.Neutropenia isdefined asadecrease in absoluteneutrophilcount<1500cells/L.65Themaincauses
ofneutropeniaincludehematologicdisorders,autoimmune diseases,infection,adversedrugreaction,chemotherapy,and radiotherapy.65Thrombocytopeniaoccurs whentheplatelet countis<100,000/mm3.65 Inapatientwithaplateletcount <81,000/mm3 concomitantly experiencing leukopenia, the
treatment should be discontinued until the platelet count increase to99,000/mm3.65 However, cyclophosphamidecan
be used in the treatment of refractory thrombocytopenic
purpura,andinthiscase,amongthehematologicdisorders,
thrombocytopenia,andmicroangiopathichemolyticanemia
are included.Leukopenia10 isdefinedasawhite cellcount <3500/mm3.65
Hepatotoxicityisanadversereactioncausedby
cyclophos-phamide that normally occurs at high doses.3 When
hepatotoxicityoccursatlowdoses,thereactionisclassifiedas arare,butserious,event.19,64Acuteliverfailurewithlow-dose cyclophosphamide (200mg) was described ina casereport ofamaleChineseaged48 yearswithprogressive glomeru-lonephritissecondarytoWegener’sgranulomatosis,24hafter the administrationofcyclophosphamide.3 Thediagnosisof granulomatosiswithpolyangiitis wasestablishedby
patho-logical examination and c-ANCA.3 The patient was being
treated with high-dose methylprednisolone,
plasmaphere-sis,intermittenthemodialysisandlowintravenousdosesof cyclophosphamide.3 Other factors that may be associated withhepatotoxicityhavebeen excluded,including antifun-gals, HIV, and hepatitis B and C.3 Alanine transaminase increasedfrom41U/Lto336U/Latthedayofadministration of200mgofcyclophosphamide; inthenext day, apeakof 566U/Lwasreached.3Twoweekslater,thepatientwastreated withanotherpulseof200mgofcyclophosphamide(second dose),andtheconcentrationofalaninetransaminasereached 1253U/L.3Aliverbiopsywasnotpossible,becausethepatient hadaclottingdisorder.3Anotherlaboratoryparametertobe monitoredissodiumconcentration.Hyponatremiais consid-eredasanelectrolytedisorderidentifiedinclinicalpractice.45
Although many cases are mild or relatively symptomatic,
withhighmorbidityandmortality.Neurologicalsymptomsof hyponatremiaoccuratsodiumlevels<125mmol/L.66Among thecomplicationsofhyponatremia,onecanmentioncentral nervoussystemdisorderssuchasseizures,andevena per-manentdamagetothecentralnervoussystem,anddeath.66 Syndrome of inappropriate antidiuretic hormone secretion (SIADH)wasdescribedinacasereportinwhichthissyndrome wasassociatedwiththeuseofIVcyclophosphamideinadose of500–1000mg/m2,withaserumsodiumlevel<120mmol/L
inapatientpresentingneurologicalcomplications.62
Cyclophosphamide may also cause cardiotoxicity.
Rou-tinely, echocardiography, a noninvasive method, is used
to monitor cardiovascular function in patients treated
with immunosuppressants.36 Other non-invasive methods
most widely used are electrocardiography and 24-h (ECG)
Holtermonitoring.36Invasivemethodssuchasscintigraphy,
magnetic resonance imaging and cardiac biopsy are also
procedures that can beused incases ofadverse reactions classifiedasserious.36
Other adverse reactions caused by cyclophosphamide
include amenorrhea, menopause, and late-onset cancer,
includingesophageal,lungandbladderadenocarcinoma.18,46
Cyclophosphamide was administered at a dose of
750–1000mg/m2 body surfaceinLUMINA(Lupusin
minori-ties,natureversusnurture),amulticenterstudyperformed including567womenagedunder51 years.46 Adecrease in gonadalfunctionwasfound,andgonadalfailurewasdefined astheoccurrenceofamenorrheaformorethansixmonths withoutahistoryofhysterectomy.46Cyclophosphamidehas alsobeenassociatedwithteratogenicity.18
Astocyclophosphamidedoseadjustmentinpatientswith kidneyfailure,thisisonlydoneinseverecases,thatis,with acreatinineclearance<10mL/min.Thetherapeuticregimen ofcyclophosphamideshouldbemodified,itsdoseshouldbe reducedby25%,andsupplementedwith50%afterdialysis.34
Thedilutionofthedrugsusedincyclophosphamide rou-tinewascarriedoutwiththegoalofmaintainingthehighest possibleconcentrationofthedruginitsnon-ionizedform.58 Thus,twoparametersweretakenintoaccount:drug compat-ibilitywiththevehicle(saline,dextroseorringerlactate)and itsstabilitytimeinthevehicle;preferencewasgiventothose drugswhosestabilitytimewaslonger,inordertoensurea moreeffectivetreatment.33
Whenthedrugsusedhaveprovedcompatibleandstable withthesamevehicle,preferencewasgiventothechoiceof thesame vehicle,asthisfacilitatestheiradministrationby thenursingstaffandpreventspharmacokineticinteraction, whichwouldcauseionizationofthedrugsandadecreasein theirefficacy.67
Anotherimportantaspectthatshouldbeaddressedisthe educationofthepatientonthetreatmenttowhathe/sheis beingsubmitted.AstudyinthecityofNatalwith40women diagnosedwithsystemiclupuserythematosusattheHospital Onofrehasshownthatpatientsshowinggreateradherence werethosewhounderstoodcorrectlythetreatmentandalso thedisease;thus,thesewomensatisfactorilyunderstoodthe adverseeventsandtheclinicalmanagement,inorderto min-imizetheseadversedrugreactions.68
Publications on adverse events are important tools for drug safety monitoring after their release for marketing
purposes bythe health authorities of each country.69 This reviewofmedicationadministrationintendedtostandardize the administrationof cyclophosphamide by health profes-sionals,inordertominimizethe adverseeventscausedby drugs,theso-calledadversedrugreaction.19
Conclusion
Theroutinewasdevelopedinordertoincreasetheareaunder thecurve(AUC)forcyclophosphamide,andtoattainan
appro-priate clinical management to minimize the adverse drug
reactions that, if not properly prevented, will cause dam-age tothe patient,forinstance,anincreasedprevalenceof vomiting,andacroleindepositioninthebladder.Theclinical managementofadversereactionsthatalterlaboratorytests wasdescribedinordertoguidetheapplicationofthesetests. Adversereactions,evenbeingrare,werehighlightedbecause theseeventscancausehighmorbidity.Thus,therationaluse ofcyclophosphamideincreasesthe safety ofthe treatment and reducesthecostofadministrationofthis chemothera-peuticagent,sinceourgoalistoavoiderror.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.BurkardME,WisinskiKB,NjiajuUO,DonohueS,HegemanR, StellaA,etal.Feasibilityof4cyclesofdocetaxeland cyclophosphamideevery14daysasanadjuvantregimenfor breastcancer:aWisconsinOncologyNetworkstudy.Clin BreastCancer.2014;14:205–11.
2.HuangBT,TanY,ZhaoWH,ZengQC,LiBS,ChenRL.Howto determinebortezomib-basedregimenforelderlypatients withmultiplemyeloma:PADversusCBd,anobservational study.JCancerResClinOncol.2014;140:303–9.
3.SubramaniamSR,CaderRA,MohdR,YenKW,GhaforHA. Low-dosecyclophosphamide-inducedacutehepatotoxicity. AmJCaseRep.2013;14:345–9.
4.MunyangangoEM,LeRoux-VilletC,DoanS,PascalF,SouedI, AlexandreM,etal.Oralcyclophosphamidewithout
corticosteroidstotreatmucousmembranepemphigoid.BrJ Dermatol.2013;168:381–90.
5.MotaLM,CruzBA,BrenolCV,PereiraIA,Rezende-FronzaLS, BertoloMB,etal.Consenso2012daSociedadeBrasileirade Reumatologiaparaotratamentodaartritereumatoide.Rev BrasReumatol.2012;52:152–74.
6.RosaNetoNS,Goldenstein-SchainbergC.Dermatomiosite juvenil:revisãoeatualizac¸ãoempatogêneseetratamento. RevBrasReumatol.2010;503:299–312.
7.BroadK,PopeJE.Theefficacyoftreatmentforsystemic sclerosisinterstitiallungdisease:resultsfroma meta-analysis.MedSciMonit.2010;16:RA187–90. 8.AppenzellerS,Sampaio-BarrosPD,SamaraAM,Marques
NetoJF.Criserenalcomomanifestac¸ãoinicialdeesclerose sistêmicasinescleroderma.RevBrasReumatol.2004;44:87–9. 9.ChuH,WuLH,SongD,YuF,ZhaoMH.Noninflammatory
necrotizingvasculopathyinlupusnephritis:asingle-center experience.Lupus.2014;23:20–30.
presentationofjuvenilesystemiclupuserythematosus patients.RevBrasReumatol.2013;53:120–6.
11.YaguchiH,SakushimaK,TakahashiI,NishimuraH, Yashima-YamadaM,NakamuraM,etal.Efficacyof intravenouscyclophosphamidetherapyforneuromyelitis opticaspectrumdisorder.InternMed.2013;52:969–72. 12.HobbsDJ,BarlettaGM,RajpalJS,RajpalMN,WeismantelDP,
BirminghamJD,etal.Severepaediatricsystemiclupus erythematosusnephritis–asingle-centreexperience. NephrolDialTransplant.2010;25:457–63.
13.LehmanTJ,SinghC,RamanathanA,AlperinR,AdamsA, BarinsteinL,etal.Prolongedimprovementofchildhoodonset systemiclupuserythematosusfollowingsystematic
administrationofrituximabandcyclophosphamide.Pediatri RheumatolOnlineJ.2014;12:3.
14.Suarez-AlmazorME,BelseckE,SheaB,WellsG,TugwellP. Cyclophosphamidefortreatingrheumatoidarthritis. CochraneDatabaseSystRev.2000:CD001157.
15.CoxPJ.Cyclophosphamidecystitis–identificationofacrolein asthecausativeagent.BiochemPharmacol.1979;28: 2045–9.
16.MavraganiCP,MoutsopoulosHM.Lupusnephritis:current issues.AnnRheumDis.2003;62:795–8.
17.DupuisLL,BoodhanS,HoldsworthM,RobinsonPD,HainR, PortwineC,etal.Guidelineforthepreventionofacute nauseaandvomitingduetoantineoplasticmedicationin pediatriccancerpatients.PediatrBloodCancer.2013;60: 1073–82.
18.FurstDE,TsengCH,ClementsPJ,StrangeC,TashkinDP,Roth MD,etal.AdverseeventsduringtheSclerodermaLungStudy. AmJMed.2011;124:459–67.
19.USDepartmentofHealthandHumanServices.Foodand DrugAdministration.Guidanceforindustryand investigators:safetyreportingrequirementsforINDsand BA/BEStudies.MD:SilverSpring;2012.p.29.Availableat: http://www.fda.gov/downloads/Drugs/.../Guidances/
UCM227351.pdf[accessed08.08.14].
20.LotanE,LeaderA,LishnerM,GottfriedM,PeregD. Unrecognizedrenalinsufficiencyandchemotherapy associatedadverseeffectsamongbreastcancerpatients. AnticancerDrugs.2012;23:991–5.
21.HsiehSG,HibbertS,ShawP,AhernV,AroraM.Associationof cyclophosphamideusewithdentaldevelopmentaldefects andsalivaryglanddysfunctioninrecipientsofchildhood antineoplastictherapy.Cancer.2011;117:2219–27. 22.AndradeED.Terapêuticamedicamentosaemodontologia:
procedimentosclínicoseusodemedicamentosnas
principaissituac¸õesdapráticaodontológica.SãoPaulo:Artes Médicas;1998.
23.FuchsFD,WannamacherL.Farmacologiaclínica: fundamentosdaterapêuticaracional.RiodeJaneiro: GuanabaraKoogan;1992.
24.WannmacherL.Erros:evitaroevitável.Usoracionalde medicmanetos:temaselecionados,vol.2;2005.p.1–6. Availableat:http://www.saudedireta.com.br/
docsupload/1284734732novoerromedico.pdf[accessed 08.08.14].
25.MeloLR,PedreiraMLG.Errosdemedicac¸ãoempediatria: análisedadocumentac¸ãodeenfermagemnoprontuáriodo paciente.RevBrasEnferm.2005;58:180–5.
26.AlluéN,ChiarelloP,BernalDelgadoE,CastellsX,GiraldoP, MartínezN,etal.Impactoeconómicodeloseventosadversos enloshospitalesespa ˜nolesapartirdelConjuntoMínimo BásicodeDatos.GacSanit.2014;28:48–54.
27.MedeirosEFF,MoraesCF,KarnikowskiM,NóbregaOT, KarnikowskiMGdO.Intervenc¸ãointerdisciplinarenquanto estratégiaparaoUsoRacionaldeMedicamentosemidosos. CiêncSaúdeColetiva.2011;16:3139–49.
28.SchuchterLM,HensleyML,MeropolNJ,WinerEP.Updateof recommendationsfortheuseofchemotherapyand radiotherapyprotectants:clinicalpracticeguidelinesofthe AmericanSocietyofClinicalOncology,Chemotherapy,and Radiotherapy.JClinOncol.2002;20:2895–903.
29.ShepherdJD,PringleLE,BarnettMJ,KlingemannHG,Reece DE,PhillipsGL.Mesnaversushyperhydrationforthe preventionofcyclophosphamide-inducedhemorrhagic cystitisinbonemarrowtransplantation.JClinOncol. 1991;9:2016–20.
30.HawthornJ,CunninghamD.Dexamethasonecanpotentiate theanti-emeticactionofa5HT3receptorantagoniston cyclophosphamideinducedvomitingintheferret.BrJ Cancer.1990;61:56–60.
31.JordanK,SippelC,SchmollHJ.Guidelinesforantiemetic treatmentofchemotherapy-inducednauseaandvomiting: past,present,andfuturerecommendations.Oncologist. 2007;12:1143–50.
32.TurnerN,StewartJ,BarnettF,WhiteS.Syndromeof inappropriateanti-diuretichormonesecretionsecondaryto carboplatinafterdocetaxel-carboplatin-trastuzumab combinationforearlystageHER-2positivebreastcancer.Asia PacJClinOncol.2012;8:e9–11.
33.TrisselLA.Handbookoninjectabledrugs.17thed.Bethesda, MD:AmericanSocietyofHealth-SystemPharmacists;2013. 34.HaubitzM,BohnenstengelF,BrunkhorstR,SchwabM,
HofmannU,BusseD.Cyclophosphamidepharmacokinetics anddoserequirementsinpatientswithrenalinsufficiency. KidneyInt.2002;61:1495–501.
35.MardeganLC,SoledadeC,SachettoZ,BertoloMB,Amstalden EMI,SâmaraAM,etal.SíndromedeChurgStrauss:uma vasculiterara.RevBrasReumatol.2004;44:179–84. 36.DiLisiD,BonuraF,MacaioneF,PeritoreA,MeschisiM,
CuttittaF,etal.Chemotherapy-inducedcardiotoxicity:roleof thetissueDopplerintheearlydiagnosisofleftventricular dysfunction.AnticancerDrugs.2011;22:468–72.
37.SalidoM,MacarronP,Hernandez-GarciaC,D’CruzDP, KhamashtaMA,HughesGR.Waterintoxicationinducedby low-dosecyclophosphamideintwopatientswithsystemic lupuserythematosus.Lupus.2003;12:636–9.
38.Calixto-LimaL,MartinsdeAndradeE,GomesAP,GellerM, Siqueira-BatistaR.Dieteticmanagementingastrointestinal complicationsfromantimalignantchemotherapy.NutrHosp. 2012;27:65–75.
39.ZahnKL,WongG,BedrickEJ,PostonDG,SchroederTM, BaumanJE.Relationshipofproteinandcalorieintaketothe severityoforalmucositisinpatientswithheadandneck cancerreceivingradiationtherapy.HeadNeck.
2012;34:655–62.
40.MilmanN.Anemia–stillamajorhealthprobleminmany partsoftheworld!AnnHematol.2011;90:369–77. 41.McDermidJM,LönnerdalB.IronAdvNutr.2012;3:532–3. 42.CentrodeOncologiaUnimedBirigui.Cuidadoscomo
pacienteemquimioterapia.Availableat:http://www. unimedbirigui.net.br/oncologia/downloads/manualcuidados comopacienteempuimioterapia.pdf[acessed08.08.14]. 43.MotaDM,SilvaMG,SudoEC,OrtúnV.Usoracionalde
medicamentos:umaabordagemeconômicaparatomadade decisões.CiêncSaúdeColetiva.2008;13Suppl.:589–601. 44.InstitutoEstadualdeHematologiaArthurdeSiqueira
Cavalcanti(Hemorio).RiodeJaneiro:Manualdopacienteem quimioterapia;2006.Availableat:http://www.hemorio.rj.gov. br/Html/pdf/Manuais/quimioterapia.pdf[accessed08.08.14]. 45.BruiningDM,vanRoonEN,deGraafH,HoogendoornM.
Cyclophosphamide-inducedsymptomatichyponatraemia. NethJMed.2011;69:192–5.
cyclophosphamideuseondamageaccrualinsystemiclupus erythematosuspatientsfromLUMINA,amultiethnicUS cohort(LUMINALXIII).Lupus.2009;18:184–6.
47.OteroLópezMJ.Erroresdemedicaciónygestiónderiesgos. RevEspSaludPública.2003;77:527–40.
48.Medeiros-SouzaP,Santos-NetoL,KusanoLTE,PereiraMG. Diagnosisandcontrolofpolypharmacyintheelderly.Rev SaúdePública.2007;41:1049–53.
49.Mesna.In:UpToDateInc.[basededadosdaInternet]. Waltham,(MA);2013.Availableat:http://www.uptodate.com [accessed01.07.14].Requerassinatura.
50.TaketomoCK,HoddingJH,KrausDM.Pediatricdosage jandbook.Cleveland:Lexi-CompInc.;1992.
51.StoneJH,MerkelPA,SpieraR,SeoP,LangfordCA,Hoffman GS,etal.Rituximabversuscyclophosphamidefor ANCA-associatedvasculitis.NEnglJMed.2010;363:221–32. 52.DewulfNL,MonteiroRA,PassosAD,VieiraEM,TronconLE. Adesãoaotratamentomedicamentosoempacientescom doenc¸asgastrintestinaiscrônicasacompanhadosno ambulatóriodeumhospitaluniversitário.RevBrasCiênc Farm.2006;42:575–84.
53.GolanDE.Princípiosdefarmacologia:abasefisiopatológica dafarmacoterapia.RiodeJaneiro:GuanabaraKoogan;2009. 54.MonachPA,ArnoldLM,MerkelPA.Incidenceandprevention
ofbladdertoxicityfromcyclophosphamideinthetreatment ofrheumaticdiseases:adata-drivenreview.ArthritisRheum. 2010;62:9–21.
55.Mesna:Tampa(FL):GoldStandard;2014.Availableat: http://www.clinicalpharmacology.com[accessed08.08.14]. Requerassinatura.
56.JeongSW,ChoJW,HwangJS,SongJD,ShinS,JangJY,etal. Theantiemeticeffectofanoveltropisetronpatchin anticanceragents-inducedkaolinpicamodelusingrats. EnvironToxicolPharmacol.2005;20:167–74.
57.deJongeME,HuitemaAD,vanDamSM,RodenhuisS,Beijnen JH.Effectsofco-medicateddrugsoncyclophosphamide bioactivationinhumanlivermicrosomes.AnticancerDrugs. 2005;16:331–6.
58.GoodmanL.Goodman&Gilman:asbasesfarmacológicasda terapêutica.RiodeJaneiro:McGraw-Hill;2001.
59.AndrewsPL,SangerGJ.Nauseaandthequestfortheperfect anti-emetic.EurPharmacol.2014;722:108–21.
60.Dexamethasone.In:UpToDateInc.[basededadosda Internet].Waltham,(MA);2013.Availableat:
http://www.uptodate.com[accessed01.07.14].Requer assinatura.
61.CagnoniPJ,MatthesS,DayTC,BearmanSI,ShpallEJ,Jones RB.Modificationofthepharmacokineticsofhigh-dose cyclophosphamideandcisplatin.BoneMarrowTransplant. 1999;24:1–4.
62.GilbarPJ,RichmondJ,WoodJ,SullivanA.Syndromeof inappropriateantidiuretichormonesecretioninducedbya singledoseoforalcyclophosphamide.AnnPharmacother. 2012;46:e23.
63.AbdulRasoolHassanB,YusoffZB,BinOthmanS.Association ofneutropeniaonsetandseveritywithchemotherapy regimensandschedules.AsianPacJCancerPrev. 2011;12:1425–8.
64.VieiraFP,RediguieiriCF,RediguieiriCF.Aregulac¸ãode medicamentosnoBrasil.PortoAlegre:Artmed;2013.p.672. 65.BassanR,HoelzerD.Moderntherapyofacutelymphoblastic
leukemia.JClinOncol.2011;29:532–43.
66.LetmaierM,PainoldA,HollAK,VerginH,EngelR, KonstantinidisA,etal.Hyponatraemiaduring psychopharmacologicaltreatment:resultsofadrug surveillanceprogramme.IntJNeuropsychopharmacol. 2012;15:739–48.
67.Brasil.MinistériodaSaúde,SecretariadeCiência,Tecnologia eInsumosEstratégicos,DepartamentodeAssistência FarmacêuticaeInsumosEstratégicos.Formulárioterapêutico nacional2010:Rename2010.2a
.ed.Brasília:Ministérioda Saúde;2010.SérieB.TextosBásicosdeSaúde.
68.FariaDA,RevoredoLS,VilarMJ,MaiaEM.Resilienceand treatmentadhesioninpatientswithsystemiclupus erythematosus.OpenRheumatolJ.2014;8:1–8.