Changing
patterns
in
leptospirosis:
a
three-decade
study
in
Brazil
Elizabeth
De
Francesco
Daher
a,*
,
Gabriela
Studart
Galdino
de
Carvalho
a,
Douglas
de
Sousa
Soares
a,
Matheus
Henrique
Mendes
a,
Sérgio
Luiz
Arruda
Parente
Filho
a,
Hermano
Alexandre
Lima
Rocha
b,
Geraldo
Bezerra
da
Silva
Junior
caDepartmentofInternalMedicine,SchoolofMedicine,WalterCantídioUniversityHospital,FederalUniversityofCeará,Fortaleza,Ceará,Brazil bDepartmentofCommunityHealth,SchoolofMedicine,FederalUniversityofCeará,Fortaleza,Ceará,Brazil
cSchoolofMedicine,PublicHealthGraduateProgram,HealthSciencesCenter,UniversityofFortaleza,Fortaleza,Ceará,Brazil
ARTICLE INFO
Articlehistory:
Received7March2017
Receivedinrevisedform25April2017 Accepted28April2017
CorrespondingEditor:EskildPetersen, Aar-hus,Denmark
Keywords:
Leptospirosis Changingpatterns Laboratoryfindings Acutekidneyinjury Mortality
SUMMARY
Background:Thisstudywasconductedtoinvestigatechangesintheclinicalpatternofleptospirosisover time,analyzingitsclinicalandlaboratorypresentationsinametropolitancityofBrazil.
Method:Thiswasaretrospectivestudyincludingallpatientswithleptospirosisadmittedtotertiarycare hospitalsinFortalezainthenortheastofBrazil,between1985and2015.Patientsweredividedintothree groupsaccordingtotheyearofhospitaladmission:groupIfortheyears1985–1995,groupIIfor1996– 2005,andgroupIIIfor2006–2015.Demographic,clinical,andlaboratorydatawerecomparedbetween thegroups.
Results:Atotalof507patientswereincluded.Theirmeanagewas37.315.9yearsand82.4%weremale. Themeantimebetweensymptomonsetandadmissionwas74days.Therewasalineardecreaseinthe levels of serumurea (190.192.7,13579.5, and 95.673.3mg/dl, respectively, p <0.0001) and
creatinine(5.82.9,3.82.6,and3.02.5mg/dl,respectively,p<0.0001)ineachdecade,whilelevels
of hemoglobin (10.311.9, 10.82.0, and 11.52.1g/dl, respectively, p <0.0001) and platelets
(57.90052.650, 80.13068.836, and 107.10199.699109/l, respectively, p<0.0001) increased. Therewasatendencytowardsalineardecreaseinmortality(22%,14%,and11.6%,respectively,p=0.060). Conclusions:Leptospirosisshowedsignificantchangesovertimeinthisregion.Themainchangespointto adecreaseindiseaseseverityandcomplications,suchasacutekidneyinjury.Mortalityhasdecreased, beingcloseto11%.
©2017TheAuthors.PublishedbyElsevierLtdonbehalfofInternationalSocietyforInfectiousDiseases. ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(
http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Leptospirosisremainsthemostimportantzoonosisworldwide, with a higher frequency in low-income tropical countries (Victorianoetal.,2009;AdleranddelaPeñaMoctezuma,2010; HaakeandLevett,2015).Ithastraditionallybeenassociatedwith rural areas and people undertaking certain risk occupations, includingabattoirand sewageworkers,militarypersonnel, and individualsinvolved inwater sportsor recreation. However,its epidemiologicalpatternhaschangedoverthelastdecades,witha markedmovetourbanareas,especiallyduringnaturaldisasters (Sarkar et al., 2002). This disease is endemic in Brazil, with outbreaksduringtherainyseason,mostlyduetoprecariousliving
conditions (slums), a lack of basic sanitation, the presence of vectors, and frequentexposure toa contaminatedenvironment duringseasonalheavyrainfallandflooding(Sarkaretal.,2002;Ko etal.,1999;Costaetal.,2015).
Leptospirosis hasbeen recognizedas an important causeof undifferentiatedfeverandisusuallymisdiagnosedasmalariaor dengue,aswellasothercausesofacutefebrileillness,including recentlyemerging viraldiseases such asZika and chikungunya (Costaetal.,2015;Pattersonetal.,2016).Itsclinicalpresentation mayvaryfroma mild non-specificinfluenza-like infectiontoa severediseasewithlife-threateningcomplications,suchasacute kidney injury (AKI), jaundice, pulmonary hemorrhage (Weil’s disease),myocarditis,andliverfailure(Daheretal.,2010;Daher etal.,2011).
Unfortunately, mortality from severe leptospirosis remains unacceptablyhigh, rangingfrom5%to20%,evenwhenoptimal treatmentisprovided(Goswamietal.,2014).Duetothelackofan adequatediagnostictest,theunderreportingofcasesanddeathsis
*Correspondingauthorat:RuaVicenteLinhares,1198Fortaleza,CEP60270-135, CE,Brazil.Tel/Fax:(+5585)3224-9725/(+5585)3261-3777.
E-mailaddresses:[email protected],[email protected]
(E.DeFrancescoDaher).
http://dx.doi.org/10.1016/j.ijid.2017.04.023
1201-9712/©2017TheAuthors.PublishedbyElsevierLtdonbehalfofInternationalSocietyforInfectiousDiseases.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
–
ContentslistsavailableatScienceDirect
International
Journal
of
Infectious
Diseases
still common, leading to underestimations of morbidity and mortality(Costaetal.,2015).Ontheotherhand,somestudieshave shownthattheclinicalpatternofleptospirosishasbeenchanging. Anincreaseinthesevereformsofthediseasehasbeenreported,as wellasitsepidemiologicalspread,butmortalityhasdecreasedin recent decades,mainlydue to improvementsin treatment and medical educationprograms(Daheret al., 2011; Everard etal., 1995; Daheret al.,1999).Nevertheless,AKI remains oneof the most severe complications associated with increased mortality (SilvaJunioretal.,2011).
Therefore,theaimofthisstudywastoinvestigatechangesin theclinicalpatternsofleptospirosisovertime,analyzingitsclinical andlaboratorypresentationsinametropolitancityofBrazil.
Methods
Studypopulation
Thestudyincludedallpatientswithaconfirmeddiagnosisof leptospirosis admitted consecutively to the São José Infectious Diseases Hospital, Walter Cantídio University Hospital, and FortalezaGeneralHospital,inFortalezainthenortheastofBrazil, fromJanuary1985toDecember2015.
Studydesign
Thiswas aretrospectivecross-sectionalstudycoveringthree decades.Datawerecollectedfromthemedicalrecordsofpatients withleptospirosis admittedto thetertiary carehospitals men-tionedabove,whicharethethreereferencehospitalsinthisregion. Patientsweredividedintothreegroupsaccordingtotheperiodof hospitaladmission:groupIfortheyears1985–1995,groupIIfor 1996–2005,and groupIIIfor 2006–2015.Demographic,clinical, and laboratory data were compared between these groups to investigatedifferencesoverthisthree-decadeperiod.
Casedefinition
Leptospirosiswasdefinedasthepresenceofapositiveserology resultwithamicroscopicagglutinationtest(MAT)titerhigherthan 1:800, associated with an epidemiological and clinical history compatiblewithleptospirosis.
Parametersassessed
Demographiccharacteristics suchas age,sex, time between symptomonsetandhospitaladmission,andlengthofhospitalstay wererecorded.Theclinicalinvestigationincludedarecordofall clinicalsignsandsymptomspresentedbyeachpatientathospital admissionandduringtheirhospitalstay,vitalsigns(systolicand diastolic blood pressure, heart rate, and respiratory rate), developmentof AKI, and need for dialysis. Laboratory data on hospital admission included an assessment of serum urea, creatinine,sodium,potassium,directbilirubin,indirectbilirubin, aspartateaminotransferase(AST),alanineaminotransferase(ALT), lactate dehydrogenase (LDH), creatine phosphokinase (CPK), hemoglobin,hematocrit,whiteblood cell(WBC) count,platelet count,andarterialbloodgasanalysis.
Definitions
AKIwas defined accordingtothe KidneyDisease Improving Global Outcomes (KDIGO) criteria; this is currently the most accepted definition and classification for AKI (Kidney Disease OutcomesQualityInitiative,2012).Thrombocytopeniawasdefined asaplateletcountlowerthan150109/l,anemiaashemoglobin
<12g/dl,andleukocytosisasaWBCcount>12109/l. Hypoalbu-minemia was considered as serum albumin <3.5g/dl. The occurrenceofmetabolicacidosiswasconsideredinthepresence of a pH <7.35 and serum bicarbonate <20 mEq/l, and severe metabolic acidosis at a pH<7.10. Tachypneawas defined as a respiratoryratehigherthan25breathsperminute.Oliguriawas defined as urine output <400ml/day after 24h of effective hydration. Hypotension was defined as a mean arterial blood pressure(MAP)of<60mmHg,andtherapywithvasoactivedrugs wasinitiatedwhenMAPremainedlowerthan60mmHgdespite theuseofparenteralfluids.Hypertensionwasdefinedasasystolic pressure 140mmHg and/or diastolic pressure 90mmHg. Regarding dialysis therapy, hemodialysis was the method of choiceratherthanperitonealdialysis,and theintentionwas for thistobeinitiatedearlyafterintensivecareunitadmission(ICU) (< 24hafterAKIdiagnosis)andperformeddaily(untilasignificant improvementinrenalfunction).
Statisticalanalysis
Theresultsareshowninthetables;valueswererecordedasthe meanstandarddeviation(SD).AlldatawereanalyzedusingIBM SPSSStatisticsversion20.0software(IBMCorp.,Armonk,NY,USA). TheKolmogorov–Smirnovtestwasusedfornumericalvariables,to assess variable distribution. Analysis of variance (ANOVA) was used for comparisons of the data between the three groups studied.Thesignificancelevelwassetat5%(p< 0.05).
Ethics
ThestudyprotocolwasapprovedbytheEthicsCommitteeof SãoJoséInfectiousDiseasesHospital,WalterCantídioUniversity Hospital,andFortalezaGeneralHospital,Fortaleza,Ceará,Brazil. Patientidentitywasprotected,sincealldatawereanonymized.
Results
A total of 507 patients wereincluded. Their mean agewas 37.315.9yearsand82.4%weremale.Therewere86patientsin groupI,187ingroupII,and234in groupIII. Therewasa male predominanceinallgroups(76.7%,80.7%,and85.9%,respectively), andpatientsingroupIwereolder(43.217.8vs.34.413.7vs. 37.316.2years, respectively, p < 0.0001). The mean time between symptom onset and hospitalization was nearly 7days inallgroups,asshowninTable1.
Theanalysisof clinicalmanifestationsshowedaprogressive decreaseinthefrequencyofarrhythmias(20%vs.11.1%vs.0.06%, respectively, p< 0.0001), chills (67.1% vs. 56.3% vs. 25.3%, respectively, p< 0.0001), dehydration (60% vs. 57.4% vs. 18.2%, respectively,p< 0.0001),mentalconfusion(21.2%vs.9.5%vs.0%, respectively, p< 0.0001), jaundice (98.8% vs. 84.9% vs. 56%, respectively, p< 0.0001), and secondary infections (11.8% vs. 7.7%vs.4.0%,respectively,p=0.04).Diastolicbloodpressurelevels increasedlinearly(66.516.1vs.67.414.2vs.72.315.4mmHg, respectively,p< 0.002).Ofnote,initiallungmanifestations,which had decreased significantly in the last decade, were more prevalentintheseconddecade,asshowninTable2.
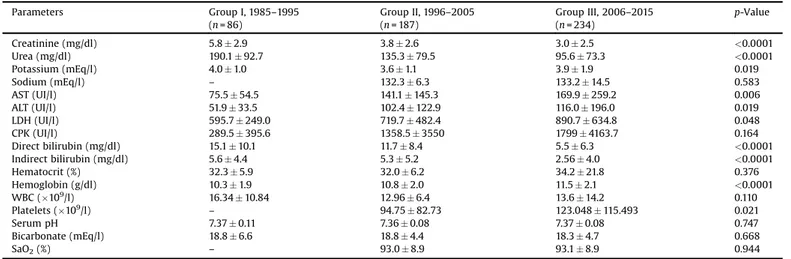
Laboratory data on hospital admission showed a linear reduction in the levels of serum urea (190 92.7 vs. 13579.5 vs. 95.673.3mg/dl, respectively, p < 0.0001) and creatinine(5.82.9vs.3.82.6vs.3.02.5mg/dl,respectively,p < 0.0001), suggesting the occurrence of milder AKI in the last decade. The levels of direct bilirubin showed a consecutive reduction(15.110.1vs.11.78.4vs.5.56.3mg/dl,respectively, p < 0.0001), while hemoglobin (10.31.9 vs. 10.82.0 vs. 11.52.1g/dl, respectively, p< 0.0001) and platelet levels
(57.952.6 vs. 80.168.8 vs. 107.199.7109/l, respectively, p< 0.0001)werehigherineachdecade,asshowninTable3.
The percentage ofpatients withsevereAKI (KDIGOstage3) decreasedconsecutively (96.3%vs. 70.1%vs. 57.4%,respectively, p< 0.0001), as shown in Figure 1. Consequently, the need for dialysis also decreased (75.6%, 29.5%, and 31.6%, respectively, p< 0.0001).Theuseofantibioticsincreasedprogressively(43.8%, 93.8%, and 94.5%, respectively, p< 0.0001), while the use of vasoconstrictors, that could only be analyzed in the last two decades,was significantly lowerin thethird decade (31.0% vs. 16.1%,p=0.05),asshowninTable4.Mortalityalsoshowedatrend towards a linear reduction (22% vs.14% vs.11.6%, respectively, p=0.060),asillustratedinFigure2.
Discussion
This is the first study in the literature to assess data from leptospirosispatients overa three-decadeperiod.Differences in clinicalandlaboratorypatternswereevaluatedacrossthis three-decadeperiod,aswellaschangesintreatment.Thestudyperiod encompassesthetimefromtherecordingofthefirstcasesinthe study region up to recent years, and important changes were observedthroughoutthesedecades,includingadecreaseinAKI severityandmortalityrates.
Leptospirosisisaseriouspublichealthproblemandaneglected disease,withahigherprevalenceintropicalareas,includingBrazil (Daheretal.,2010;Slack,2010).McBrideetal.(2005)recognized thatadvanceshavebeenmadeinunderstandingthepathogenesis ofleptospirosis,andfoundthattheeffectsofeducationalprograms inendemicareashadanimportantimpactindecreasingmortality (Daheretal.,2011).Therehasbeenaclearimprovementinthe disease diagnosis, mainly due to physician awareness of the differentialdiagnosisoffebrileillnessesintropicalcountries, as wellasmoreexperiencewithfebrilediseasesaffectingreturning travelersindevelopedcountries(McBrideetal.,2005;Ricaldiand Vinetz,2006;Waggoneretal.,2015).
Consistentwithpreviousstudies,mostpatientsinthepresent studyweremale.Themale sexhasbeenextensivelyassociated withtheriskofleptospirosisinfection,duetotheconnectionof leptospirosisinfectionwithoccupationstraditionallyattributedto men, such as abattoir and sewage workers, as well military personnel. Consequently, males are usually more exposed to Leptospiraspirochetes(Sarkaretal.,2002;Mikulskietal.,2015). Furthermore,patientsdiagnosedin thelast twodecadesofthis studyweresignificantlyyoungerthanthosein thefirstdecade. Thisfactmayhavestronglyinfluencedthereductioninmortality andpresenceoflesssevereformsofthediseaseinrecentyears, sinceolderpatientsusuallyhavemorecomorbiditiesandahigher
Table2
Comparisonofsigns,symptoms,andvitalsignsbetweengroupsI,II,andIII.a
GroupI,1985–1995 (n=86)
GroupII,1996–2005 (n=187)
GroupIII,2006–2015 (n=234)
p-Value
Signsandsymptoms
Arrhythmias(%) 17(20) 6(11) 1(0.6) <0.0001
Chills(%) 57(67) 90(56.3) 57(25.3) <0.0001
Headache(%) 56(65.9) 129(79.6) 132(58.7) <0.0001
Crackles(%) 12(14) 36(22.8) 20(8.9) 0.001
Dehydration(%) 51(60) 93(57.4) 41(18.2) <0.0001
Mentalconfusion(%) 18(21.2) 4(9.5) 0(0) <0.0001
Jaundice(%) 84(98.8) 141(84.9) 126(56) <0.0001
Secondaryinfections(%) 10(11.8) 12(7.7) 9(4) 0.041
Myalgia(%) 78(91.8) 157(94.6) 166(73.8) <0.0001
Petechiae(%) 11(12.9) 32(20.8) 8(3.6) <0.0001
Tachypnea(%) 17(20) 53(33.5) 20(8.9) <0.0001
Dyspnea(%) 1(1.2) 69(42.3) 71(31.6) <0.0001
Oligo/anuria(%) 20(23.5) 53(33.3) 57(25.3) 0.143
Fever(%) 84(98.8) 159(95.8) 205(91) 0.019
Calfpain(%) 70(82.4) 57(80.3) 109(52.4) <0.0001
Edema(%) 12(14.1) 24(45.3) 21(15.4) <0.0001
Vitalsigns
SBP(mmHg) 110.020.3 108.119.7 116.421.3 0.001
DBP(mmHg) 66.516.1 67.414.2 72.315.4 0.002
HR(/min) – 97.317.3 96.618.4 0.786
RR(/min) – 268 2610 0.716
SBP,systolicbloodpressure;DBP,diastolicbloodpressure;HR,heartrate;RR,respiratoryrate.
aAnalysisofvariance(ANOVA).Valuesareexpressedasthemeanstandarddeviation,orasthenumber(percentage).p-Valuesof<0.05wereconsideredstatistically
significant.
Table1
ComparisonofdemographicdatabetweengroupsI,II,andIII.a
GroupI,1985–1995 (n=86)
GroupII,1996–2005 (n=187)
GroupIII,2006–2015 (n=234)
p-Value
Age(years) 43.217.8 34.413.7 37.316.2 <0.0001
Sex
Male(%) 66(76.7) 151(80.7) 201(85.9) 0.121
Female(%) 20(23.3) 336(19.3) 33(14.1)
Hospitalstay(days) 13.28.7 8.15.0 11.18.2 <0.0001
Timebetweensymptomonsetand hospitalization(days)
72 73 75 0.822
Mortality(%) 22 14 11.6 0.060
aAnalysisofvariance(ANOVA).Valuesareexpressedasthemeanstandarddeviation,orasthenumber(percentage).p-Valuesof
<0.05wereconsideredstatistically
significant.
riskofdeath.Olderageand thepresenceofcomorbiditieshave beenextensivelyassociatedwithdeathinleptospirosispatients (Koetal.,1999;Daheretal.,1999;Dupontetal.,1997).
In contrast to previousreports, the clinical presentation on admissionoftheleptospirosispatientsinthepresentstudyseems tohavebecomemilderoverthelastdecade.Aprogressivedecrease insomeofthelife-threateningmanifestations,suchas arrhyth-mias,chills,dehydration,mentalconfusion,jaundice,and second-ary infections, was noted, suggesting a decrease in severe leptospirosis,mostlyinthelastdecade.Itwasalsoobservedthat
the time between symptom onset and hospital admission remained nearly the same, while the length of hospital stay decreased.Thisprobablyreflectsamilderformofdisease,which maybeattributedtobettersanitaryconditionsinBrazilandearly diagnosis.Poorsanitationhasbeenstronglyassociatedwiththe developmentofleptospirosisinmanycountries(Mwachuietal., 2015).In addition,onlypeoplewithsevereformsofthedisease wouldhavebeendiagnosedandhospitalizedinthefirstdecadeof thisstudy.Thediagnosisandhospitalizationofmildercaseshave becomemorefrequentinrecentyears,probablyduetoeffective
Table3
ComparisonoflaboratorydatabetweenpatientsfromgroupsI,II,andIII.a
Parameters GroupI,1985–1995 (n=86)
GroupII,1996–2005 (n=187)
GroupIII,2006–2015 (n=234)
p-Value
Creatinine(mg/dl) 5.82.9 3.82.6 3.02.5 <0.0001
Urea(mg/dl) 190.192.7 135.379.5 95.673.3 <0.0001
Potassium(mEq/l) 4.01.0 3.61.1 3.91.9 0.019
Sodium(mEq/l) – 132.36.3 133.214.5 0.583
AST(UI/l) 75.554.5 141.1145.3 169.9259.2 0.006
ALT(UI/l) 51.933.5 102.4122.9 116.0196.0 0.019
LDH(UI/l) 595.7249.0 719.7482.4 890.7634.8 0.048
CPK(UI/l) 289.5395.6 1358.53550 17994163.7 0.164
Directbilirubin(mg/dl) 15.110.1 11.78.4 5.56.3 <0.0001 Indirectbilirubin(mg/dl) 5.64.4 5.35.2 2.564.0 <0.0001
Hematocrit(%) 32.35.9 32.06.2 34.221.8 0.376
Hemoglobin(g/dl) 10.31.9 10.82.0 11.52.1 <0.0001
WBC(109/l) 16.34
10.84 12.966.4 13.614.2 0.110
Platelets(109/l)
– 94.7582.73 123.048115.493 0.021
SerumpH 7.370.11 7.360.08 7.370.08 0.747
Bicarbonate(mEq/l) 18.86.6 18.84.4 18.34.7 0.668
SaO2(%) – 93.08.9 93.18.9 0.944
AST,aspartateaminotransferase;ALT,alanineaminotransferase;LDH,lactatedehydrogenase;CPK,creatinephosphokinase;WBC,whitebloodcellcount;SaO2,oxygen
saturation.
aAnalysisofvariance(ANOVA).Valuesareexpressedasthemeanstandarddeviation.p-Valuesof
<0.05wereconsideredstatisticallysignificant.
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
1985 - 1995 1996 - 2005 2006 - 2015
p <0.001
KDIGO 1
KDIGO 2
KDIGO 3
Figure1.AcutekidneyinjurystagesaccordingtotheKidneyDiseaseImprovingGlobalOutcomes(KDIGO)criteria,inpatientswithleptospirosisinthethreedifferent decades.
Table4
ComparisonoftreatmentinstitutedforpatientswithsevereleptospirosisbetweengroupsI,II,andIII.a
GroupI,1985–1995 (n=86)
GroupII,1996–2005 (n=187)
GroupIII,2006–2015 (n=234)
p-Value
Vasoconstrictors(%) – 9(31.0) 31(16.1) 0.05
Ceftriaxone(%) 9(64.3) 0(0) 125(67.9) 0.046
Penicillin(%) 7(22.6) 114(82.6) 64(28.4) <0.0001
Diuretics(%) 3(11.5) 10(34.5) 42(21.8) 0.118
Needfordialysis(%) 65(75.6 54(29.5) 74(31.6) <0.0001
Hemodialysis(%) 3(4.6) 53(98.1) 67(90.5) <0.0001
Peritonealdialysis(%) 62(95.4) 1(1.9) 7(9.5) <0.0001
aAnalysisofvariance(ANOVA).Valuesareexpressedasthenumber(percentage).p-Valuesof<0.05wereconsideredstatisticallysignificant.
medical education programs (Daher et al., 2011). The early diagnosis of leptospirosis has been associated with fewer complications and a faster recovery from the infection (Daher etal.,2010;Dupontetal.,1997;Spichleretal.,2008).
Moreover,changesinthehemodynamicstatusandlaboratory parameters were observed, including a decrease in bilirubin levels and an increase in hemoglobin and platelet levels. The better hemodynamic status of the patients on admission, demonstrated by higher blood pressure levels, confirms the presenceof themilderformsofthediseasein thelastdecade. Hyperbilirubinemia is extremely common in leptospirosis patients,more frequentlyin associationwith skin rash,which usuallyleadstothepresenceofa‘rubinicjaundice’pattern(Puca et al., 2016).Elevated bilirubin levels and jaundice have been associatedwithdeathandpooroutcomesinleptospirosis(Daher etal.,2016;Herrmann-Storcketal.,2010;Abgueguenetal.,2008), and their lower levels in the last decades among the study patients also reflect a reduction in disease severity in these patientsthroughthedecades.
Improvementsinhematologicalparameters,including hemo-globin and platelet levels, may be evidence of a less severe infectionandmayhavecontributedtothedecreaseinmortality.A decreaseinhemoglobinlevelsisacommonfindinginleptospirosis patients andhasbeen associatedwithseveredisease and poor outcomes(De Silva et al.,2014; Prabhu and Ramesh, 2016). In addition,thrombocytopenia isalsoextremelyfrequentin lepto-spirosispatients and it is usuallyassociated with hemorrhagic phenomena and complications. It hasbeen strongly associated with mortality and severity in leptospirosis and it has been includedinarecentdiagnosticscoringsystemforleptospirosisina resource-limited setting (Spichler etal., 2008;Rajapakse et al., 2016).InastudycarriedoutinPuertoRico,elevatedWBClevels wereassociatedwithfatal outcomes(Sharpetal.,2016).Inthe presentstudy,thiselevationmayhaveresultedfromamoresevere disease presentation on admission and a possible secondary infection.
The presence of arrhythmiasis alsoa predictorof death in leptospirosis.Arrhythmiasarethemostcommoncardiac manifes-tationofleptospirosisandoftenderivefromelectrolytedisorders, such as hypokalemia and hypocalcemia, which are usually secondarytoAKI(Sacramentoetal.,2002;NavinanandRajapakse, 2012;Soaresetal.,2017).Electrocardiographicabnormalitieshave
beendescribedasriskfactorsfordeathinleptospirosispatients (Daheretal.,1999;Dupontetal.,1997).
Interestingly,therewasasignificantlinearreductioninserum ureaandcreatinineinthepatientsincludedinthepresentstudy.A progressivereductionofsevereAKIcases(KDIGOstage3)ineach decadewasalsoshown,suggestingearlydiagnosisandtreatment. Consequently,lessrenalreplacementtherapywasneededoverthe lastdecades,arelevantfactorthathascontributedtothedecrease inmortality,sinceAKIisstronglyassociatedwithahigherriskof deathinleptospirosis(SilvaJunioretal.,2011;Daheretal.,2008; Telesetal.,2016).LeptospirosisisasignificantcauseofAKIin low-and middle-income tropical countries (Bouchard and Mehta, 2016).AKIisalsoanimportantcomponentofthesevereformof leptospirosis(Weil’ssyndrome),leadingtoseveralcomplications. Referraltospecializedcare,includinganephrologistconsultation, aswellasearlyimplementationofdialysis,seemstobeessential forslowingtheprogressionofAKItomoresevereformsandfor decreasing mortality (Andrade et al., 2007). Regarding the treatmentofAKI, intermittent peritonealdialysis(IPD)was the predominantmethodin theperiodfrom 1985to1996,usedin 95.4%ofpatientswhoneededdialysis;dailyhemodialysis(DHD) wasthemethodmostoftenusedintheperiodfrom1997to2015. Theinstitutionofearlyhemodialysis(<24hafterAKIdiagnosis) insteadofIPDwasessentialforthebetterprognosisofpatientsin thesecondandthirddecadesofthestudy,withprovenbenefitsin leptospirosis patients (Andrade et al., 2007). Furthermore,it is hypothesized that the reduction in AKI development and AKI severity,aswellastheestablishmentofearlyandeffectiverenal replacementtherapywerekeypointsinthereductionofmortality inthesepatientsinrecentyears.
Acleardecreasingtrendinmortalitywasseenoverthesethree decades(decreasingfrom22%to14%,andthento11.6%inthelast decade),whichprobablyreflectstheearlydiagnosisof complica-tionsandtheprovisionofadequatetreatment.Althoughprevious studieshaveshownevidencethatmortalitydoesnotseemtobe significantlyinfluencedbyantibioticuse(Daheretal.,2012;Costa etal.,2003),arecentstudybythepresentinvestigatorgroupfound that ceftriaxone was a protective factor for ICU admission in leptospirosispatients(Daheretal.,2016).Thereisalsoevidence thattheuseofpenicillinisassociatedwithareductioninhospital lengthofstayandfewercomplications,includingAKI(Daheretal., 2012).Itwasalsodemonstratedinthepresentstudythattheuseof
Figure2. Decreaseinmortalityofleptospirosiscasesoverthethree-decadeperiodp=0.06.
antibioticsincreasedprogressivelythroughoutthedecadesinthis cohort(43.8%,93.8%,and94.5%,respectively,p< 0.0001),although itwasnotdirectlyassociatedwithadeclineinmortalityaccording tothemultivariateanalysis.Theuseofantibioticsinleptospirosisis now a consensus in the literature and it is believed that the increase in use has probably contributed to a reduction in mortality,sincetheuseofantibioticshasbeenassociatedwitha shorterlengthofhospitalstay,milderAKI,andlessneedfordialysis (Daheretal.,2012),aswellasalowerfrequencyofICUadmission (Daheretal.,2016).
In summary, leptospirosis is a life-threatening neglected tropicaldiseaseanditspresentationhaschangedsignificantlyin thestudyregionovertime.Themainchangespointtoareduction inseverityandcomplications,suchasAKI.Mortalityhasshowna cleardecreasingtrendinrecentdecades.
Studylimitations
Themainlimitationsofthisstudyderivefromitsretrospective design.Admissiondatawerenotavailableinsomepatientrecords. ThestudywasperformedinonlyoneregionofBrazil,sodisease patternsmaydifferinotherregionsofBrazilandworldwide.
Non-technicalsummary
Leptospirosis is a bacterialdisease transmitted byrat urine, whichisverycommonintropicalcountries.Thecharacteristicsof patientswithleptospirosisinalargecityinBrazilwereassessed, overaperiodofthreedecades.Thereisevidencethatthedisease hasbecomemilder,includingmilderformsofrenalfailure,oneof themostseverediseasecomplications.Adecreaseinmortalitywas alsofound. These findings could bedue tomore frequent and earlieridentificationofthediseasebyclinicians,andconsequently tobetterhealthcareprovision.
Financialsupport
E.F.DaherandG.B.SilvaJuniorarerecipientsofagrantfromthe Conselho NacionaldeDesenvolvimentoCientíficoeTecnológico (CNPq).Thefundershadnoroleinthestudydesign,datacollection andanalysis,decisiontopublish,orpreparationofthemanuscript.
Conflictofinterest
The authors declare no conflicts of interest regarding this manuscript.
Acknowledgements
Weareverygratefultotheteamofclinicians,medicalresidents, medical students, and nurses fromSão José InfectiousDiseases Hospital,WalterCantídioUniversityHospital,andFortalezaGeneral Hospital fortheassistance providedto thepatientsand for the technicalsupportprovidedforthedevelopmentofthisresearch.
References
AbgueguenP,DelbosV,BlanvillainJ,ChennebaultJM,CottinJ,FanelloS,etal. Clinicalaspects and prognosticfactors of leptospirosis in adults.J Infect 2008;57:171–8.
AdlerB, delaPeñaMoctezumaA.Leptospiraandleptospirosis.VetMicrobiol 2010;140:287–96.
AndradeL,CletoS,SeguroAC.Door-to-DialysisTimeandDailyHemodialysisin Patientswith Leptospirosis:Impact onMortality. Clin J Am SocNephrol 2007;2:739–44.
BouchardJ,MehtaRL.AcuteKidneyInjuryinWesternCountries.KidneyDis(Basel) 2016;2:103–10.
CostaE,LopesAA,SacramentoE,CostaYA,MatosED,LopesMB,etal.Penicillinat thelatestageofleptospirosis:arandomizedcontrolledtrial.RevInstMedTrop SaoPaulo2003;45:141–5.
CostaF,HaganJE,CalcagnoJ,KaneM,TorgersonP,Martinez-SilveiraMS,etal.Global MorbidityandMortalityofLeptospirosis:ASystematicReview.PLoSNeglTrop Dis2015;9:e0003898.
DaherE,ZanettaDM,CavalcanteMB,AbdulkaderRC.Riskfactorsfordeathand changingpatternsinleptospirosisacuterenalfailure.AmJTropMedHyg 1999;61:630–4.
DaherEF,MarquesCN,LimaRSA,SilvaJúniorGB,BarbosaAS,BarbosaES,etal.Acute kidneyinjuryinaninfectiousdiseaseintensivecareunit-anassessmentof prognosticfactors.SwissMedWkly2008;138:128–33.
DaherEDF,deAbreuKLS,daSilvaJuniorGB.Leptospirosis-associatedacutekidney injury.JBrasNefrol2010;32:400–7.
DaherEF,SilvaGB,LimaRSA,MotaRMS,RochaHAL,deAbreuKLS,etal.Different PatternsinaCohortofPatientswithSevereLeptospirosis(WeilSyndrome): EffectsofanEducationalPrograminanEndemicArea.AmJTropMedHyg 2011;85:479–84.
Daher EF, Silva GB, de AbreuKLS, MotaRMS, Batista DV, RochaNA, et al. Leptospirosis-associatedacutekidneyinjury:penicillinatthelatestageis still controversial: Penicillinin leptospirosis. J Clin Pharm Ther 2012;37: 420–5.
DaherEF,SoaresDS,deMenezesFernandesATB,GirãoMMV,SidrimPR,Pereira EDB,etal.Riskfactorsforintensivecareunitadmissioninpatientswithsevere leptospirosis:acomparativestudyaccordingtopatients’severity.BMCInfect Dis2016;16:40.
DeSilvaNL,NiloofaMJR,FernandoN,KarunanayakeL,RodrigoC,DeSilvaHJ,etal. Changesinfullbloodcountparametersinleptospirosis:aprospectivestudy.Int ArchMed2014;7:31.
DupontH,Dupont-PerdrizetD,PerieJL,Zehner-HansenS,JarrigeB,DaijardinJB. Leptospirosis:prognosticfactors associatedwith mortality.Clin InfectDis 1997;25:720–4.
Everard CO, Edwards CN, EverardJD, CarringtonDG. A twelve-yearstudy of leptospirosisonBarbados.EurJEpidemiol1995;11:311–20.
GoswamiRP,GoswamiRP,BasuA,TripathiSK,ChakrabartiS,ChattopadhyayI. Predictors of mortalityin leptospirosis:an observational study from two hospitals in Kolkata,easternIndia.TransR SocTrop Med Hyg2014;108: 791–6.
Haake DA, Levett PN. Leptospirosis in humans. Curr TopMicrobiol Immunol 2015;387:65–97.
Herrmann-StorckC,Saint-LouisM,FoucandT,LamauryI,DeloumeauxJ,BarantonG, etal.Severeleptospirosisinhospitalizedpatients,Guadeloupe.EmergInfect Dis2010;16:331–4.
KidneyDiseaseOutcomesQualityInitiative.KDIGOclinicalpracticeguidelinesfor acutekidneyinjury–Summaryofrecommendationstatements.KidneyInt Suppl2012;2:1–138.
KoAI,GalvãoReisM,RibeiroDouradoCM,JohnsonWD,RileyLW.Urbanepidemicof severe leptospirosis in Brazil. Salvador Leptospirosis Study Group. Lancet 1999;354:820–5.
McBrideAJ,AthanazioDA,ReisMG,KoAI.Leptospirosis.CurrOpinInfectDis 2005;18:376–86.
MikulskiM,BoisierP,LacassinF,Soupé-GilbertMRE,MauronC,Bruyere-OstellsL, etal.SeverityMarkersinsevereleptospirosis.EurJClinMicrobiolInfectDis 2015;34:687–95.
MwachuiMA,CrumpL,HartskeerlR,ZinsstagJ,HattendorfJ.Environmentaland behaviouraldeterminantsofleptospirosistransmission:asystematicreview. PLoSNeglTropDis2015;9:e0003843.
NavinanMR,RajapakseS.Cardiacinvolvementinleptospirosis.TransRSocTrop MedHyg2012;106:515–20.
Patterson J, Sammon M, Garg M.Dengue, Zika and Chikungunya:emerging arbovirusesinthenewworld.WestJEmergMed2016;17:671–9.
PrabhuMV,RameshV.Fever,thrombocytopenia,andAKI-Aprofileofmalaria, dengue,andleptospirosiswithrenalfailureinaSouthIndiantertiary-care hospital.ClinNephrol2016;86:128–30.
PucaE,PilacaA,KaloT,PiperoP,BinoS,HysenajZ,etal.Ocularandcutaneous manifestationofleptospirosisacquiredinAlbania:aretrospectiveanalysiswith implicationsfortravelmedicine.TravelMedInfectDis2016;14:143–7.
RajapakseS,WeeratungaP,NiloofaR,FernandoN,deSilvaNL,RodrigoC,etal.A DiagnosticScoringModelforLeptospirosisinResourceLimitedSettings.PLoS NeglTropDis2016;10:e000451.
RicaldiJN,VinetzJM.Leptospirosisinthetropicsandintravelers.CurrInfectDisRep 2006;8:51–8.
Sacramento E,LopesAA, CostaE, PassosOL,Costa YA,MatosED. Electrocar-diographic alterations in patients hospitalized with leptospirosis in the BraziliancityofSalvador.ArqBrasCardiol2002;78:267–70.
Sarkar U, Nascimento SF, Barbosa R, MartinsR, Nuevo H, Kalofonos I, etal. Population-basedcase-controlinvestigationofriskfactorsforleptospirosis duringanurbanepidemic.AmJTropMedHyg2002;66:605–10.
SharpTM,GarcíaBR,Pérez-PadillaJ,GallowayRL,GuerrAM,RyffKR,etal.Early IndicatorsofFatalLeptospirosisduringthe2010EpidemicinPuertoRico.PLoS NeglTropDis2016;10:e0004482.
SilvaJuniorGB,AbreuKL,MotaRM,BarretoAG,AraújoSM,RochaHA,etal.RIFLE and Acute Kidney Injury Network classifications predict mortality in leptospirosis-associated acutekidney injury.Nephrology (Carlton)2011;16: 269–76.
SlackA.Leptospirosis.AustFamPhysician2010;39:495–8.
SoaresDS,GaldinoGS,RodriguesBC,SilvaJuniorGB,DaherEF.Arrhythmiasin leptospirosis-associatedacutekidneyinjury:acaseseries.BrazJInfectDisin press2017;inpress.
SpichlerAS,VilaçaPJ,AthanazioDA,AlbuquerqueJO,BuzzarM,CastroB,etal. PredictorsoflethalityinsevereleptospirosisinurbanBrazil.AmJTropMedHyg 2008;79:911–4.
TelesF,deMendonçaUchôaJV,MendonçaDMB,CostaAFP.Acutekidneyinjuryin leptospirosis:theKidneyDiseaseImprovingGlobalOutcomes(KDIGO)criteria andmortality.ClinNephrol2016;86:303–9.
VictorianoAFB,SmytheLD,Gloriani-BarzagaN,CavintaLL,KasaiT, Limpakarnja-naratK,etal.LeptospirosisintheAsiaPacificregion.BMCInfectDis2009;9:1.
WaggonerJJ, SodaEA, Seibert R, GrantP, Pinsky BA.Molecular detection of Leptospiraintworeturnedtravelers:higherbacterialloadincerebrospinalfluid versusserumorplasma.AmJTropMedHyg2015;93:238–40.