www.jped.com.br
ORIGINAL
ARTICLE
Parental
tobacco
consumption
and
child
development
夽
Nadine
F.
Santos
a,∗,
Raquel
A.
Costa
a,baUniversidadedeTrás-os-MonteseAltoDouro,VilaReal,Portugal
bUniversidadeEuropeiaLaureateInternationalUniversities,Lisbon,Portugal
Received3June2014;accepted17September2014 Availableonline27February2015
KEYWORDS
Psychomotor development;
Tobaccouse;
Parenting
Abstract
Objective: Toanalyzetheassociationbetweenparentaltobaccoconsumptionandthe preva-lenceofpsychomotordevelopmentdisordersinchildrenbetween6and22monthsofage.
Method: Onehundredandninemothers,fathers,andtheirbabiesparticipatedinthestudy.The sociodemographicandclinicalconditionswereassessedusingquestionnaires.Tobacco consump-tionwasassessedusingtheFagerströmTestforNicotineDependence(FTND).Childdevelopment wasevaluatedusingtheScaleofPsychomotorDevelopmentinEarlyChildhood.
Results: There was a significant negative correlation between the father’s morning smok-ing(FTND)andthechild’slanguagedevelopmentquotient;r=-0.41,p=0.005,r2=0.15.The
childrenofmotherswithoutnicotinedependencehadahighermeanlanguagedevelopment quo-tientthanchildrenofmotherswithnicotinedependence;F(1,107)=5.51,p=0.021,p2=0.05. Conclusion: Parentalsmokingappearstohaveadetrimentaleffectonchilddevelopment. ©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Desenvolvimento psicomotor;
Consumodetabaco;
Parentalidade
Consumodetabacoparentaledesenvolvimentoinfantil
Resumo
Objetivo: Analisararelac¸ãoentreoconsumodetabacoparentaleaprevalênciadedistúrbios nodesenvolvimentopsicomotoremcrianc¸asentreosseiseosvinteedoismesesdeidade.
Método: Cento e nove mães, pais e seus bebês participaram no estudo. Ascircunstâncias sociodemográficas e clínicas foram avaliadas com recurso a questionários. O consumo de tabacofoiavaliadoutilizandooTestedeFagerströmparaaDependênciaTabágica(Heatherton, Kozlowski,Frecker,&Fagerström,1991).Odesenvolvimentoinfantilfoiavaliadoutilizandoa EscaladoDesenvolvimentoPsicomotordaPrimeiraInfância(Brunet&Lézine,1951).
夽
Pleasecitethisarticleas:SantosNF,CostaRA.Parentaltobaccoconsumptionandchilddevelopment.JPediatr(RioJ).2015;91:366---72. ∗Correspondingauthor.
E-mail:[email protected](N.F.Santos).
http://dx.doi.org/10.1016/j.jped.2014.09.006
Resultados: Háumacorrelac¸ão negativasignificativaentreofumo matinal(FTND) dopaie o quociente de desenvolvimentode linguagem da crianc¸a, r=-0,41, p=0,005, r2=0,15. As
crianc¸asdemãessemdependênciatabágicatêmemmédiaumquocientededesenvolvimento delinguagemsuperioràscrianc¸asdemãescomdependênciatabágica,F(1,107)=5,51,p=0,021,
p2=0,05.
Conclusão: Oconsumodetabacoparentalpareceterumefeitoprejudicialparao desenvolvi-mentodacrianc¸a.
©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Development inthe firstyearsof lifeis essential. Several
environmental factors, such as the parental consumption
ofsubstances,canincrease thelikelihoodof
developmen-tal difficulties in childhood,1 especially in the emotional,
educational,2social,behavioral,andpsychologicallevels.3
Tobacco consumption, specifically---which has high preva-lence in Portugal (22%)4---is an important public health
problem, and has been associated with difficulties in self-regulation; increased excitability and activation in the neonatal period;5 lower birth weight;6,7 learning
difficulties;6 lower volume of the frontal and cerebellar
lobes---responsiblefor emotional functioning,impulse con-trol,andattention;8smallerheadcircumference;9cognitive
andlanguageneurodevelopmentaldisorders;10,11and
child-hoodemotionalandbehavioraldisorders.6Thisassociation
canbeexplainedbythefactthatduringchildhood,thebrain continuesto develop andis particularlysensitive to envi-ronmentalpollutants,6orbybraindisordersresultingfrom
exposuretonicotineduringpregnancy.8
Asenvironmentalriskfactorsappeartoberelatedto chil-dren’sdevelopmentaldisorders,especiallymotor,language, social, cognitive, behavioral, and psychological disorders, thestudyofpsychomotordevelopmentassociatedtothese factorsis the aim of thisstudy.Although thereis a great dealofliteraturerelatedtochilddevelopment,the associ-ationbetweentobaccousebybothparentsandpsychomotor developmentisstilllargelyunknown.Therefore,thisstudy differs from previous studies due to the fact that (1) it analyzes several aspects of child development - posture, language,visual-motorcoordination,andsocial---ratherthan beinglimitedtooveralldevelopment;(2)moststudiesfocus on the effects of this consumption on children’s health, and/orduringpregnancyandnotafterit;(3)bothparents wereconsidered.
Methods
Participants
Participants were recruited from four day care centers
located in the city of Funchal-Madeira, Portugal, after
authorizationbytheDirec¸ãoRegionaldeEducac¸ão(Regional
Education Board). Most of the participants were of
Por-tugueseorigin(94.3%)andwhite(98.0%).
Participationinthestudy wasproposedto124 mothers
and124fathers;87.9%agreedtoparticipate,9.3%refused
toparticipateduetolackoffreetime,and2.8%werenot
interestedin participating. Thus,the sample consisted of
109mothers,109fathers,and109babies.Thesample
inclu-sioncriterionwas: (1) tobethemother/father ofa child
agedbetween6and22months;theexclusioncriteriawere:
(1)illiteracyand(2)theexistenceofdiseasesinthebabies.
Thestudywasperformedduring2011andthedatacollection
phaselastedthreemonths.
Tools
Sociodemographicandclinicaldata
Aquestionnairewasusedtocollectsocialanddemographic
data(age,gender,maritalstatus,yearsofeducation,
profes-sionalstatus,physical andpsychologicaldiseases, medical
or psychological treatment, numberof pregnancies,
num-berof miscarriages, number of children, age of children,
andchildren’sphysicalandpsychologicaldiseases),aswell
as clinical information on the pregnancy and newborn
(pregnancy planning, prenatal care, risk pregnancy,
ges-tational age, type of delivery, type of anesthesia, Apgar
score,weightandheight,headcircumference,reanimation,
healthproblemsatbirth,currentsleeppattern---monophasic
(longperiodsofcontinuoussleep)vs.biphasic(alternation
between periods of sleep and wakefulness), and type of
feeding.
Nicotinedependence
Fagerström Test for Nicotine Dependence (FTND)12,13
Thistestwasdevelopedtocompensateforthe
psychomet-riclimitationsoftheFagerströmToleranceQuestionnaire,12
and aims to measure the nicotine dependence of an individual.13 It consists of six items related to smoking
habits and behaviors, rated on a Likert scale ranging from0-3points.Higher resultsindicateagreater smoking dependence,14 in which a score of 0-3 indicates absence
of nicotine dependence, 4-6 indicates moderate nicotine dependence,and≥7indicatesseverenicotinedependence. ThePortugueseversionhasacceptablepsychometric prop-erties,withCronbach’s␣=0.66.13Test-retestreliabilitywas
ensuredbycorrelationvaluesoftheoriginalscaleof0.99. Factor analysis showed the existence of two factors: (1) cigaretteconsumption---dailyconsumptionpatterns---and(2) morningsmoking- degree of urgencyto restorethe level ofnicotineafterthenighttimeabstinence.13Inthepresent
Psychomotordevelopment
ScaleofPsychomotorDevelopmentinEarlyChildhood15
This scale allows the evaluation of the child’s
develop-mentallevel(1-30months)ineachofthefollowingareas:
postural---child’s movements such as rolling over, sitting,
and walking; visual-motor coordination---manipulation of
objects,visual-manualcoordination,andsolvingproblems;
language---expressionand understanding; and social---social
andpersonalrelations,especiallyadaptationtosocial
situa-tions,games,andrelationswithothers.15
Itconsistsof150 items,whicharedistributedin levels (1-30).Thisscaleallowsthecalculationofthe Developmen-talQuotient(DQ=DA×100/CA),inwhichDArepresentsthe developmentalageandCAthechronologicalage.ADQ≤75 indicateslowerdevelopment,whereasDQof76to100 indi-catesnormaldevelopment,and>100demonstrateshigher development.15
The scale validity criterion is 0.68, with a test-retest correlationcoefficientof0.85.15
Procedures
Allevaluationprocedureswereperformedandapprovedby
theethicscommitteeoftheinstitution.Mothersandfathers
received an explanation on the purpose and procedures
of thestudy, andafter the informedconsent wassigned,
theywereaskedtocompleteasocio-demographic/clinical
questionnaire and the FTND12,13 (approximate duration of
20-25minutes).
The Scale of Psychomotor Development in Early Childhood15 was used to assess the infant’s psychomotor
development. This assessment was always performed by thesame investigator, appropriately trained and familiar-izedwiththescale applicationprocedures.Eachbabywas observedindividually and only ata specific time (approx-imately 30to 40minutes), while thedaycare professional waspresent, but away fromthe baby’s visual range. The questionspertainingtoeachsubtestwereansweredbythe daycareprofessionalattheendofeachobservation.
Statistical
procedures
Pearson’sCorrelationtestwasusedtoassesswhetherthere
wasacorrelationbetweenthedegreeofnicotine
depend-ence(FTND)of themotherandthe fatherandthe child’s
postural,visual-motor,language,social,andoverall
devel-opmentquotient.16
The significance of nicotine dependence factor (FTND ≥ 7) of the mother and father on the composite of the variableschild’spostural,visual-motor,language,andsocial developmentquotientwasevaluatedbyseveralMultivariate AnalysisofVariance(MANOVAs).17Thesignificanceofthe
dif-ferencebetweenthechild’soveralldevelopmentquotient accordingtonicotinedependenceofthemotherandfather (FTND≥7)wasevaluatedbyusingthet-testforindependent samples.16
The chi-squaredtest wasusedtoassesswhether there wasan association betweenchild’s overall developmental quotient(lower, normal,upper)and thenicotine depend-ence(FTND≥7)ofthemotherandfather.16
Effectsizesofeachoftheanalysesperformedand inter-preted based on the classification proposed by Maroco,17
KinnearandGray,18andCohen.19
Results
Mostpregnancieswereplanned(65.1%)anddesired(97.2%).
Mostmothershadprenatalcare(98.2%)andanormal
preg-nancy(79.8%),lasting37weeksormore(94.7%,M=39.34,
SD=1.70). Most babies were born by vaginal delivery
(62.3%), and 37.7% were born by cesarean section, with
mostmothersreceivingepiduralanesthesia(73.4%).Apgar
score valuesranged from 3-10 (M=8.96, SD=1.06) at the
firstminuteoflife(97.2%≥7)andbetween7-10(M=9.74,
SD=0.57) at the fifth minute. At birth, weight varied
between 1.990kg and 4.530kg (M=3.31, SD=0.45), and
mosthadabirthweight≥2.500kg(99.1%),whereasheight
ranged from 36.00-59.05cm (M=48.85, SD=3.06), and
head circumference ranged between 30-37cm (M=34.64,
SD=1.22).Mostbabiesdidnotrequirereanimationatbirth
(97.2%) and had no health problems (95.4%). Most had a
pattern ofbiphasic sleep(59.6%).Mostmothersbreastfed
(81.7%)foraperiodoftimerangingfromonemonthto22
months(M=7.29,SD=5.29).
Maternalagerangedbetween19and45years(M=33.17,
SD=5.88)andpaternalagerangedbetween20and50years
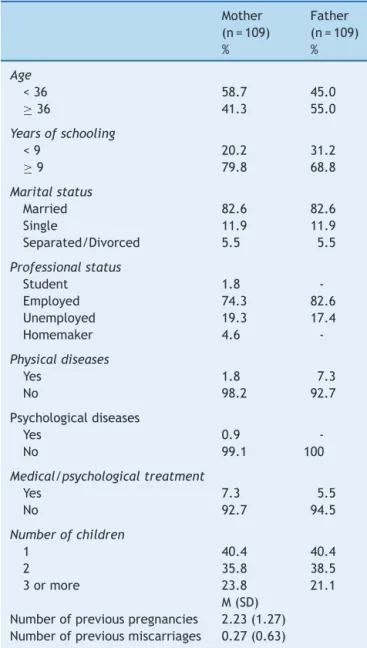
(M=36.29,SD=6.03).Thesociodemographiccharacteristics
areshowninTable1.
Babieswereagedbetween6and22months,withmost being aged ≥ 12 months (M=14.50, SD=4.62). Approxi-matelyhalfweremales(50.5%;Table1).
AssociationbetweenMaternalandPaternal NicotineDependence(FTND)andChild DevelopmentQuotient
There was no statistically significant correlation between
the mother’s nicotine dependence and cigarette smoking
(FTND)andthepostural,visual-motor,language,social,and
overall childdevelopmentquotient,withsmalleffectsize
(r2 ≤ 0.1). There was no statistically significant
correla-tion between the mother’s morning smoking (FTND) and
the postural, visual-motor, language, social, and overall
child development quotient, with small effect size (r2 ≤
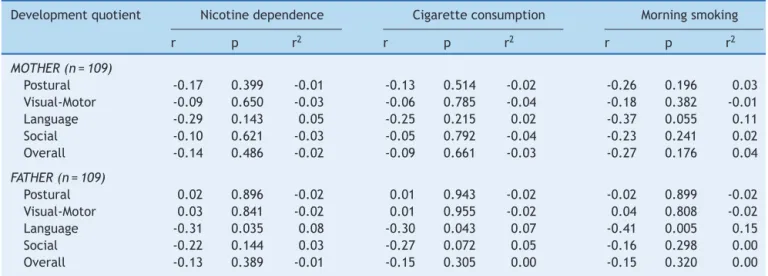
0.1).However,therewasanegativeandmarginally
signif-icant correlation between the mother’s morning smoking
(FTND)andthechild’slanguagedevelopmentquotient,with
medium-sizedeffectsize(r2=0.11)(Table2).Thus,ahigher
degreeofmaternalmorningsmokingwasassociatedwitha lowerlanguagedevelopmentquotient.
Table1 Sociodemographicdata. Mother (n=109)
Father (n=109)
% %
Age
<36 58.7 45.0
≥36 41.3 55.0
Yearsofschooling
<9 20.2 31.2
≥9 79.8 68.8
Maritalstatus
Married 82.6 82.6
Single 11.9 11.9
Separated/Divorced 5.5 5.5
Professionalstatus
Student 1.8
-Employed 74.3 82.6
Unemployed 19.3 17.4
Homemaker 4.6
-Physicaldiseases
Yes 1.8 7.3
No 98.2 92.7
Psychologicaldiseases
Yes 0.9
-No 99.1 100
Medical/psychologicaltreatment
Yes 7.3 5.5
No 92.7 94.5
Numberofchildren
1 40.4 40.4
2 35.8 38.5
3ormore 23.8 21.1
M(SD) Numberofpreviouspregnancies 2.23(1.27) Numberofpreviousmiscarriages 0.27(0.63)
smoking were associated with a lower language
develop-mentquotient.
ImpactofMaternalandPaternalNicotine
Dependence(FTND)ontheChild’sDevelopment Quotient
Thematernalnicotinedependencefactor(FTND<7vs.FTNP
≥7)hadastatisticallysignificant effectonthe
multivari-atecompositeofchilddevelopmentquotient,=0.91,F(4,
104)=2.59, p=0.041, p2=0.09, with the eta value
sug-gestingamedium-sizedeffect.Univariateanalysisshowed
thatchildrenofmotherswithoutnicotinedependencehad
ahighermeanvisual-motor development,F(1,107)=4.61,
p=0.034andlanguagequotientF(1,107)=5.51, p=0.021,
than children of mothers withnicotine dependence, with
theetavalue suggestingsmalleffectsize(Table3).There
werenosignificantdifferencesbetweenchildrenof moth-erswithnicotinedependencevs.childrenofmotherswith no nicotine dependence in terms of overall development
quotient,t(107)=1.16,p=0.248;however,Cohen’sd-value suggestsamedium-sized effect(Table3).The children of motherswith nonicotine dependence had a highermean overalldevelopmentquotientthanchildrenofmotherswith nicotinedependence.
Paternalnicotinedependencefactor (FTND<7vs.FTNP ≥ 7) did not have a statistically significant effect on themultivariatecompositeofchilddevelopmentquotient, =0.99, F(4, 104)=0.32, p=0.865, p2=0.01, with the eta value suggesting a small effect size. There were no significant differences between children of fathers with nicotinedependence vs.children of fatherswithno nico-tinedependenceintermsofoveralldevelopmentquotient, t(107)=0.16,p=0.875,withCohen’sd-valuesuggestinga smalleffectsize(Table3).
AssociationbetweenMaternalandPaternal NicotineDependence(FTND)andChild DevelopmentQuotient
There was no significant association between the overall
developmentquotientofthechildandthematernalnicotine
dependence(FTND<7vs.FTNP≥7),2(2)=1.56,p=0.459,
andthepaternaldependence, 2(2)=1.01,p=0.605, with
smalleffectsize(Table4).
Discussion
This study was conducted to analyze the association
between parental consumption of tobacco and child
development. The results show that there was such an
association,withparentaldailyconsumptionpattern,
nico-tinedependence,andtheurgency ofconsumption aftera
nocturnalabstinenceperioddemonstratingassociationwith
language difficulties; there was an especially significant
associationbetweenmaternalnicotinedependenceand
lan-guage,visual-motor,andglobaldevelopment.Theseresults
areespeciallyimportantbecausetheyshowthattheeffect
of parentalnicotine dependence is harmful not only
dur-ingpregnancy,asotherstudieshaddemonstrated10butalso
afterdelivery.In fact, thisstudy does notclarify the dif-ferentialeffectof prenatalor postnatalmaternalnicotine dependenceonchilddevelopment.However,when consid-eringthe effectofpaternalsmokingdependence onchild development,itcanbeassumedthatthisreferstothe post-natal period, which draws attention to the vulnerability of the newborn topassive exposure to parental smoking. The mechanisms that explain the effect of tobacco con-sumption during pregnancy on the fetus have been well studiedin recent years, andthereis some evidence indi-catingthattheconsumption ofnicotineandother tobacco components influence gestational duration,20 have toxic
effectsonfetalbraindevelopmentduringpregnancy,10and
areassociatedwithfetalhypoxia,changesintheserotonin uptake,changesinthedopaminergicsystems,andchanges inDNAandRNA synthesisin thebrain.17 Nicotineappears
totarget specific neurotransmitter receptors in the fetal brain, causing abnormalities in cell proliferation and dif-ferentiation,resultingincellnumberdeficitsandchanges in synapticactivity,21 impairingthe fetal-placental
Table2 Associationbetweennicotinedependence,cigaretteconsumption,morningtobaccoconsumption,andchild develop-mentquotient.
Developmentquotient Nicotinedependence Cigaretteconsumption Morningsmoking
r p r2 r p r2 r p r2
MOTHER(n=109)
Postural -0.17 0.399 -0.01 -0.13 0.514 -0.02 -0.26 0.196 0.03 Visual-Motor -0.09 0.650 -0.03 -0.06 0.785 -0.04 -0.18 0.382 -0.01 Language -0.29 0.143 0.05 -0.25 0.215 0.02 -0.37 0.055 0.11 Social -0.10 0.621 -0.03 -0.05 0.792 -0.04 -0.23 0.241 0.02 Overall -0.14 0.486 -0.02 -0.09 0.661 -0.03 -0.27 0.176 0.04
FATHER(n=109)
Postural 0.02 0.896 -0.02 0.01 0.943 -0.02 -0.02 0.899 -0.02 Visual-Motor 0.03 0.841 -0.02 0.01 0.955 -0.02 0.04 0.808 -0.02 Language -0.31 0.035 0.08 -0.30 0.043 0.07 -0.41 0.005 0.15 Social -0.22 0.144 0.03 -0.27 0.072 0.05 -0.16 0.298 0.00 Overall -0.13 0.389 -0.01 -0.15 0.305 0.00 -0.15 0.320 0.00
r2,sizeeffectcoefficientdeterminant. Pearson’scorrelationtest.
Table3 Parentalnicotinedependenceandchilddevelopmentquotient. Development
quotient
MOTHER FATHER
Without nicotine dependence (FTND<7) (n=82)M (SD)
With nicotine dependence (FTND≥7)
(n=27)M (SD)
p p2 Without
nicotine dependence (FTND<7) (n=82)M (SD)
With nicotine dependence (FTND≥7)
(n=27)M (SD)
p p2
Posturala 97.61(16.54) 98.04(17.49) 0.909 0.00 98.79(17.36) 96.24(15.81) 0.433 0.01
Visual-motora
91.29(12.20) 85.59(11.19) 0.034 0.04 90.71(12.71) 88.74(12.19) 0.405 0.01
Languagea 84.55(16.36) 76.07(15.96) 0.021 0.05 83.16(15.94) 81.48(17.60) 0.604 0.00
Sociala 92.20(12.96) 88.00(12.67) 0.145 0.02 92.33(13.42) 89.54(12.55) 0.269 0.01
d d
Overallb 91.50(14.27) 88.00(11.14) 0.248 0.27 90.81(15.24) 90.39(11.12) 0.875 0.03
FTND,FagerströmTestforNicotineDependence;M,mean;SDstandarddeviation;p2,etasquared---sizeeffectforMANOVA;d,Cohen’s d-value---sizeeffectfort-test.
aMANOVA.
b t-testforindependentsamples.
Table4 Associationbetweenparentalnicotinedependenceandchilddevelopmentquotient.
MOTHER FATHER
Development Quotient
Withoutnicotine dependence
Withnicotine dependence
Withoutnicotine dependence
Withnicotine dependence (FTND<7)(n=82) (FTND≥7)(n=27) (FTND<7)(n=63) (FTND≥7)(n=46)
% % V % % V
.12 .10
LowerDQa 7.3 7.4 7.9 6.5
NormalaDQa 70.7 81.5 69.9 78.3
UpperDQa 22.0 11.1 22.2 15.2
for the newborn.23 As a consequence, there are
signifi-cant changesin thebrain physiologyresponsiblefor basic perceptual skills;24 loss of centralnervoussystem cells in
the postnatal period; reduction of the frontal lobe and cerebellarvolumesresponsibleforattention,emotion,and impulsecontrol;8aswellasasmallerheadcircumferencein
newborns.9Thesephysiological alterationsmaybe
respon-siblefor developmentaldisordersfoundin thesechildren, suchasself-regulatorydifficulties, increasedexcitability,5
decrease in cognitive functions, and learning and mem-orydeficits.10,11Overalldevelopmentaldifficultiesobserved
inthis study,withemphasisonlanguageandvisual-motor skills, are consistent with previous studies that indicate an association between parental consumption of tobacco andchilddevelopmentdisorders,25especiallypsychomotor
disorders.26 Regarding the effect of tobacco consumption
bytheparents,theeffectiscausedbyexposureafterbirth, whichindicatesthenewborn’sspecificvulnerabilityto expo-suretotoxinsreleasedbytobaccoconsumption.27 Because
ofthe implications,parentalsmokingduringtheperinatal periodisanimportantpublichealthproblem,andtherefore interventionprogramsinperinatalhealththattarget smok-ingcessation,notonlyforfuturemothersbutalsoforfuture fathers,shouldbeconsideredaprioritytoensureabetter qualityoflifeforfamilies.
Despitethelimitationsofthisstudy---especiallybecause it did not consider a detailed analysis of the behavior associatedwithtobaccoconsumptionorregardingparental consumptionhistory---it shouldbeconsideredan important contributiontothestudyoftheeffectofparentalsmoking, asithelpstobetterunderstandtheeffectofconsumption notonlybymothers,butalsobyfathers,thus encompass-ingbothparentsinordertoanalyzetheindividualeffecton psychomotordevelopment.
Future studies should assess not only the differential effectofconsumption byeachparent,butalsothe differ-entialeffectofprenatalandpostnataltobaccoconsumption onchilddevelopment.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
The authors would like tothank the Regional Director of
EducationforallowingthestudytobecarriedoutinRegião
AutónomadaMadeira(RAM)daycarecenters.Theauthors
are alsovery grateful to the headsof educational
estab-lishments, teachers, and kindergarten assistants, and the
parents who allowed the observation of the psychomotor
developmentoftheirbabiesandspentpartoftheirprecious
timetoanswerthequestionnaire.
Thisstudywasdevelopedaspartoftheproject‘‘Therole
ofgenotype-environmentinteractionontheresilienceand
vulnerabilitytodevelopmentalandmentalhealthproblems
inthefirst18monthsoflife’’(PTDC/PSI-PCL/119152/2010)
fundedbytheFundac¸ãoparaaCiênciaeTecnologia
(Foun-dationforScienceandTechnology).
References
1.WillrichA,AzevedoCC,FernandesJO.Desenvolvimentomotor na infância: influência dos fatores de risco e programas de intervenc¸ão.RevNeurocienc.2008;17:51---6.
2.BlanchardKA,SextonCC,MorgensternJ,McVeighKH,McCrady BS, Morgan TJ, et al. Children ofsubstance abusing women onfederalwelfare:implicationsforchildwell-beingandTANF policy.JHumBehavintheSocialEnv.2005;12:89---110. 3.WellsK.Substanceabuseandchildmaltreatment.PediatrClin
NorthAm.2009;56:345---62.
4.BridgeheadInternationalEuropequitting-progressand path-ways.London:Pfizer;2011March.ReportNo.USC1184. 5.StroudL,PasterR,PapandonatosG,NiauraR,SalisburyA,Battle
C,etal.Maternalsmokingduringpregnancyandnewborn neu-robehavior:effectsat10to27days.JPediatr.2009;154:10---6. 6.AgrawalA,ScherrerJ,GrantJ,SartorC,PergadiaM,Duncan A,etal.Theeffectsofmaternalsmokingduringpregnancyon offspringoutcomes.PrevMed.2010;50:13---8.
7.ChertokI,LuoJ,AndersonR.Associationbetweenchangesin smokinghabitsinsubsequentpregnancyandinfantbirthweight inWestVirginia.MaternChildHealthJ.2011;15:249---54. 8.Ekblad M, Korkeila J, Parkkola R, Lapinleimu H, Haataja
L, Lehtonen L, et al. Maternal smoking during pregnancy and regional brain volumes in preterm infants. J Pediatr. 2010;156:85---90.
9.KallenK.Maternalsmokingduringpregnancyandinfanthead circumferenceatbirth.EarlyHumDev.2000;58:197---204. 10.Kiechl-KohlendorferU,RalserE,PuppU,ReiterG,Griesmaier
E,TrawögerR.Smokinginpregnancy:ariskfactorforadverse neurodevelopmentaloutcomeinpreterminfants?ActaPaediatr. 2010;99:1016---9.
11.WehbyG,PraterK,McCarthyA,CastillaE,MurrayJ.Theimpact ofmaternalsmokingduringpregnancyonearlychild neurode-velopment.JHumCap.2011;5:207---54.
12.HeathertonTF,KozlowskiLT,FreckerRC,FagerströmKO.The Fagerström Test for NicotineDependence: a revisionof the FagerströmToleranceQuestionnaire.BritishJournalof Addic-tion.1991;86:1119---27.
13.FerreiraPL,QuintalC,LopesI,TaveiraN.Testede dependên-ciaànicotina:validac¸ãolinguísticaepsicométricadotestede Fagerström.DependênciaTabágica.2009;27:37---56.
14.FagerströmKO,KunzeM,SchoberbergerR,BreslauN,Hughes JR,HurtRD,etal.Nicotinedependenceversussmoking preva-lence:comparisonsamongcountriesandcategoriesofsmokers. TobaccoControl.1996;5:52---6.
15.BrunetO,LézineI.Ledevelopmentpsychologiquedela pre-mièreenfance.Paris:PressesUniversitairesdeFrance;1951. 16.MartinsC.Manualdeanálisededadosquantitativoscomrecurso
aoIBMSPSS:saberdecidir,fazer,interpretareredigir.Braga: Psiquilibrios;2011.
17.MarocoJ. Análiseestatísticacomutilizac¸ãodo SPSS.Lisboa: Edic¸õesSílabo;2007.
18.KinnearPR,GrayCD.PASWstatistics17madesimple.NewYork: PsychologyPress;2010.
19.CohenJ.Statisticalpoweranalysisforthebehavioralsciences. NewJersey:LawrenceErlbaumAssociates,Inc;1988. 20.Mello PR, Pinto GR, Botelho C. Influência do tabagismo na
fertilidade, gestac¸ão elactac¸ão. JPediatr (Rio J). 2001;77: 257---64.
21.Slotkin TA. Fetalnicotine or cocaineexposure:which one is worse?JPET.1998;285:931---45.
22.Jauniaux E,BiernauxV,Gerlo E,Gulbis B. Chronicmaternal smokingandcordbloodaminoacidandenzymelevelsatterm. ObstetGynecol.2001;97:57---61.
24.Key A, FergusonM, Molfese F,Peach K, Lehman C, Molfese V. Smoking during pregnancy affects speech-processing abil-ity in newborn infants. Environ Health Perspect. 2007;115: 623---9.
25.Poole-DiSalvoE,LiuYH,BrennerS,WeitzmanM.Adult house-holdsmokingisassociatedwithincreasedchildemotionaland behavioralproblems.JDevBehavPediatr.2010;31:107---15.
26.Andraca I,Pino P, La ParraA, Rivera F,Castillo M.Factores de riesgo para el desarrollo psicomotor em lactentes naci-dos em óptimas condiciones biológicas. Rev Saude Publica. 1998;32:138---47.