www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Hearing
performance
as
a
predictor
of
postural
recovery
in
cochlear
implant
users
夽
Mario
Edvin
Greters
a,
Roseli
Saraiva
Moreira
Bittar
b,∗,
Signe
Schuster
Grasel
b,
Jeanne
Oiticica
b,
Ricardo
Ferreira
Bento
baPontifíciaUniversidadeCatólicadeCampinas(PUC---Campinas),DepartamentodeOtorrinolaringologia,Campinas,SP,Brazil bUniversidadedeSãoPaulo(FMUSP),FaculdadedeMedicina,DepartamentodeOtorrinolaringologia,SãoPaulo,SP,Brazil
Received4August2015;accepted4January2016 Availableonline31March2016
KEYWORDS
Dizziness; Balance; Hearingloss; Posturography; Auditoryevoked potentials; Cochlearimplant
Abstract
Objective:Thisstudyaimedtoevaluateifhearingperformanceisapredictorofposturalcontrol incochlearimplant(CI)usersatleastsixmonthsaftersurgery.
Methods:Cross-sectionalstudyincluding(CI)recipientswithpost-lingualdeafnessandcontrols whoweredividedintothefollowinggroups:nineCIuserswithgoodhearingperformance(G+), fiveCIuserswithpoorhearingperformance(G−),andsevencontrols(CG).Foreachpatient, computerizeddynamic posturography(CDP)tests,asensoryorganizationtest (SOT),andan adaptationtest(ADT)wereappliedasdualtaskperformance,withfirsttest(FT)andre-test (RT)onthesameday,includinga40---60minintervalbetweenthemtoevaluatetheshort-term learningabilityonposturalrecoverystrategies.Theresultsofthegroupswerecompared.
Results:ComparingthedualtaskperformanceonCDPandtheweightedaveragebetweenall testconditions,theG+groupshowedbetterperformanceonRTinSOT4,SOT5,SOT6,andCS, whichwasnotobservedforG− andCG.TheG− grouphadsignificantlylowerlevelsof short-termlearningabilitythantheothertwogroupsinSOT5(p=0.021),SOT6(p=0.025),andCS (p=0.031).
Conclusion:TheCIuserswithgoodhearingperformancehadahigherindexofposturalrecovery whencomparedtoCIuserswithpoorhearingperformance.
© 2016 Publishedby Elsevier EditoraLtda. on behalf ofAssociac¸˜ao Brasileira de Otorrino-laringologiaeCirurgiaC´ervico-Facial.ThisisanopenaccessarticleundertheCCBYlicense (http://creativecommons.org/licenses/by/4.0/).
夽 Pleasecitethisarticleas:GretersME,BittarRS,GraselSS,OiticicaJ,BentoRF.Hearingperformanceasapredictorofposturalrecovery incochlearimplantusers.BrazJOtorhinolaryngol.2017;83:16---22.
∗Correspondingauthor.
E-mail:[email protected](R.S.M.Bittar).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.01.002
1808-8694/©2016PublishedbyElsevierEditoraLtda.onbehalfofAssociac¸˜aoBrasileiradeOtorrinolaringologiaeCirurgiaC´ervico-Facial.
PALAVRAS-CHAVE
Tontura; Equilíbrio; Perdaauditiva; Posturografia; Potenciaisevocados auditivos;
Implantecoclear
Desempenhoauditivocomopreditorderecuperac¸ãoposturalemusuáriosde implantecoclear
Resumo
Objetivo: Opresenteestudoteveporobjetivoavaliarseodesempenhoauditivoépreditorde controleposturalemusuáriosdeICpelomenos6mesesapósacirurgia.
Método: Estudotransversal consistindo emrecipientes de implantecoclear(IC) comsurdez pós-lingualecontroles,queforamdivididosnosseguintesgrupos:noveusuáriosdeICcombom desempenhoauditivo(G+),cincousuáriosdeusuáriosdeICcomdesempenhoauditivo insatis-fatório(G-)esetecontroles(GC).Aplicamosotestedeposturografiadinâmicacomputadorizada (PDC),testedeorganizac¸ãosensitiva(TOS)etestedeadaptac¸ão(TAd)comodesempenhode duplatarefa,primeiroteste(PT)ereteste(RT)nomesmodia,comintervalode40-60 minu-tosentretestes,comoobjetivodeavaliaracapacidadedeaprendizadoemcurtoprazonas estratégiasderecuperac¸ãopostural.Comparamososresultadosdostestes.
Resultados: ComparandoodesempenhodeduplatarefanotestePDCeamédiaponderalentre todas ascondic¸ões de teste,ogrupo G+ demonstrou melhor desempenho noRT nos TOS4, TOS5,TOS6eEC,oquenãofoiobservadoparaosgruposG-eGC.OgrupoG-obteveníveis significantemente maisbaixosdecapacidadedeaprendizadoem curtoprazovs.outrosdois gruposnoTOS5(p=0,021),TOS6(p=0,025)eEC(p=0,031).
Conclusão:Usuários de IC com bom desempenho auditivo tiveram índice melhor de recuperac¸ãopostural,quandocomparadosausuáriosdeICcomdesempenhoauditivo insat-isfatório.
© 2016Publicadopor ElsevierEditora Ltda.em nomede Associac¸˜ao Brasileira de Otorrino-laringologia eCirurgiaC´ervico-Facial.Este ´eumartigo Open Accesssob umalicenc¸a CCBY (http://creativecommons.org/licenses/by/4.0/).
Introduction
Cognitiveresourcesfromtherightcerebralhemisphere sig-nificantlycontributetoposturalcontrol.Theassessmentof adultswithvestibulardisordersshowedthatimplementation ofmentaltasksduringtheperformanceoftheplatformtest canboth increase or reduce subjectoscillationsand body balancecontrol.1Workingmemory,short-termmemory,and executivefunctionarefrequentlyandmorehighlydisturbed inthosestrickenbybacterialmeningitis.2Inapreviousstudy performedat thepresentclinicwithcochlearimplant(CI) users (study submitted), a significant increase was found inP3latency inpatientswithpost-lingualdeafnessdueto meningitis,suggestinganimpairmentofcognitivefunction. Sensoryinputcomingfromhearing,vision,vestibular,and proprioceptivesystemsisprocessedinthecentralnervous system(CNS),resultinginspatialorientation,imagefixation ontheretina, andbalance control.3Postural adjustments necessary forbalance stabilityresultfromcomplexmotor responses,learnedmotortasks,andproactiveand feedfor-wardposturalstrategies.4
Balancecontrolistheabilitytomaintainbodymovement within the base of support without falling. It is a com-plexcontrol process that depends on mainly twodistinct andinterdependentsystems:(1)thegazestabilization sys-tem,whichmaintainsgazedirectionoftheeyesandvisual acuityduringheadandbodymovements,and(2)the pos-turalstabilizationsystem,whichkeepsthebodyinbalance while standingand moving in dailylife. They aredistinct becausethey rely oninputs from differentsenses, motor reactionsfromdifferentpartsofthebody,andaremediated bydifferentbrainpathways.Theyarealsointerdependent
because gaze stability is not possible unless the body is alsostable,and becauseaccurate vision is a critical sen-soryinputforposturalcontrol.Therefore,balancedepends onvarioussensoryinputswhichinformthebrainaboutbody positionrelatedtotheenvironment.Itisahighlycomplex network that includes numerous synaptic pathways, non-synapticpathways,andtheirintersections.Thebrainmust analyzeandplanthemotorresponsesandmovements nec-essaryforposturalstabilization.5
At this moment cognitive function is required for the accuratesensoryintegrationtoachieveasuitablebody bal-ancecontrol. The following arepart of cognition: (1)the sensory input integration of the brain map composed of movementstrategieslearnedthroughoutlife,(2) appropri-atelatencies of posturalresponses, and (3)the ability to planandexecutemovementpatternsnecessaryfor control-lingthecenterofthebodymass.Thecortexmustprocess andintegratethesefunctionstobeawareoftheriskandthe taskbeingperformed.Thus,balancecontrolisinfluencedby cognitivefactors like attention, motivation,memory, and intent. In normal individuals, the whole system works in harmonyand is processed automatically, but mayrequire voluntarycontrolwhenthereisimbalanceatsomepointof thetrack.
limit vestibular compensation. Likewise, speech under-standingandinterpretationdependonlearningandmemory. TheDepartmentofOtolaryngologyatHospitaldas Clíni-casUniversityofSãoPauloSchoolofMedicine(HC-FMUSP) performsdozensofCIsurgeriesondeafpatientseveryyear; allof them have routineauditory evoked potentialtests. Basedontheauthors’clinicalexperience(studysubmitted), it wasobserved that subjects withpoor word discrimina-tionhad aprolonged P3latency in the cognitiveauditory evokedpotentialtest.ItwasshownthatCIuserswithpoor hearing performance (≤80% speech recognition in open-setsentences), particularlythosedeaf due tomeningitis, show longer P3 latencies as compared to deaf patients withgoodhearingperformanceafterCI(studysubmitted). Thus,theP3testseemstobeusefultodetectimpairment of central sensory integration after auditory stimulation. Theliteraturedemonstratesintersectionsbetweenauditory, vestibular,learning, and memory pathways. There is evi-denceofhearingtestsaspredictorsoffalls6 andevidence thatcomputerizeddynamicposturography(CDP)shows sec-ondarychangesduetonoise-inducedhearingloss.9
Both auditory memory and balance depend on the integrity of CNS structures. So, it would be plausible to assumethatsubjectssufferingfromcentralauditory path-wayimpairmentcouldalsohavetroubleintasksofpostural recoveryinvolvingcognition.Inordertoevaluatethe rela-tionshipbetweenauditoryandvestibularcognitivedistress, theauthorsdeveloped amethodtoassess postural recov-ery (short-term memory, a taskthat depends directly on properfunctioningofthehippocampus)insubjectswithand withoutgoodhearingperformanceafterCIsurgery.
Objectives
Thisstudyaimedtoevaluatewhetherhearingperformance is a predictor of postural control in CI users at least six monthsaftersurgery.
Methods
Sample
Cross-sectionalstudy conducted between 2008 and 2011, including111CIuserswithpostlingualdeafnessfromtheCI GroupofHC-FMUSP.Thefollowingvariableswereassessed: gender,age,causeofdeafness,andCIelectrodetype.The study was carried out according to the guidelines of the Ethics Committee of the University of São Paulo School ofMedicine andwasapprovedin2007 underprotocol No. 1059/07.
Selectioncriteria
Patientswereconsideredeligibleaccordingtothefollowing criteria:(a)CIusersactivatedfor atleast sixmonths;(b) completeinsertionof theCIelectrodes;(c)bothgenders; (d)aged18yearsorgreater;(e)performedtheauditory cog-nitivepotential;(f)wereawareoftheresearchandsigned theinformedconsent.Exclusioncriteriawere:(a)patients withorthopedicorneurologicalrestrictionsthatprevented
the performance of the CDP; (b) patients complaining of dizzinessorimbalance.
Casuistic
At the time of the research 111 patients with post lin-gualdeafness wereimplantedin thisservice; 60were<18 yearsoldandwereexcluded.Theremainingpatientswere contacted by phoneand26gave positiveresponses. Eigh-teen of themagreed toparticipatein the study.Subjects who declined reported the following reasons: some lived in states with sufficient support for CI recipients; others didnot wanttoparticipateinthis scientificstudy.Of the 18 individuals whoagree to participate,only 14 met the selection criteria and were divided into two groups: (a) Group+ (G+)composed ofnine CIuserswithgoodhearing performance; (b) Group− (G−) consisted of five CI users with poor hearing performance. All patients were fitted withmulti-channelcochlearimplants(Nucleus22,Nucleus 24) activatedfor atleast sixmonths. Completeelectrode insertion wascontrolled by postoperativeradiologic stud-ies.For‘‘poor’’speechperformers,theinternalCIunitwas testedandretestedusingthesoftwareprovidedbythe man-ufacturer(ImpedancecheckRA26,CochlearCorporation ---Denver,CO,UnitedStates).
ForeachCIuseracontrolsubjectwasselected,matched forageandeducation.The controlgrouphad26subjects, 15females,withmeanageof44.7years(range23---68,SD 14.75).Allcontrol subjectshadbilateralpure-tone audio-metricthresholdsof25dBHLorbetterfrom500to8000Hz, nohearingortinnituscomplaints,andnohistoryof otologi-caldiseases.Theexclusioncriteriawerethesameasforthe studygroup.
Goodhearingperformancewasdefinedas≥80%speech recognition in open-set sentences. Athird group of seven normal-hearingsubjects,withnormalpuretoneaudiometry (PTA),speechrecognitionthresholds(SRT),andspeech dis-criminationscores(SDS),wasusedasthecontrolgroup(CG) ofthestudy.
Computerized
dynamic
posturography
CDP is an objectiveand non-invasivetest thatallows the graphic recordingof bodypositionagainstvariousstimuli. The CDPis a uniqueassessment techniqueusedto objec-tively quantify interactions among vestibular, visual, and somatosensory inputsnecessaryfor balancecontrol, coor-dination of motor responses,and alignmentof the center of gravity (COG). Therefore, CDP analyzes the ability to maintainorregaincontrolofbodyposture underavariety of sensory conditions.This study used theSmart Equitest System®(NeurocomInternationalInc.---Clackamas,Oregon,
UnitedStates).Each oftheselectedpatientsperformed a dualtasktestinordertoassessshort-termmemory,which dependsdirectlyonproperfunctioningofthehippocampus. To evaluate the short-termlearning ability in the perfor-manceofposturalrecoverystrategies,twoCDPtestswere selected:(1)thesensoryorganizationtest(SOT);and(2)the adaptationtest(ADT).
control dependsonthe interactionbetween vision, vesti-bular,andproprioceptiveinputs.Thesubjectwasinstructed tostandasstillaspossible,withtheheaderect,eyes look-ingforward,andhandsalongthebodyduringspecificvisual, floorsurface,andvisualsurroundmanipulations.An equilib-riumscorebasedonthemagnitudeoftheCOGmovements, expressedaspercentageofthelimitsofstability,was cal-culated for each trial. A score of 100% indicates perfect stabilityand0%indicatesswaythatexceedsthelimitsof sta-bilityorafall.Acompositescore(CS),aweightedaverage ofthescoresforthesixsensoryconditions,wascalculated andusedinthestatisticalanalyses,aswellastheresultsof eachindividualcondition.
The ADT assesses the ability of the automatic motor system to adapt to an unexpected external disturbance. Adaptation is assessed by determining the ability to sup-pressinappropriateresponsestotheexternaldisturbance. The test consistedof fivetrialsin whichthefloor surface wastiltedupward(toesup)andfivetrialsinwhichthefloor surfacewasrotateddownward(toesdown).Eachofthefive rotationslasted400mswithanamplitude of8◦.The time
betweenthetrialswasrandomizedfrom3to5s.The ADT scorequantifiesthemagnitudeoftheanterior-posterior(AP) swayandmusclereactionsforbodybalancecontrol follow-ingunexpectedsupportrotationsthatdetermineankleangle changes.The meanscores oftoes-up andtoes-downsway energywere included inthe statistical analyses.Similarly tothe SOT, the program providesthe results in graphical andnumericalscales.
For each patient, both CPDtests (SOT and ADT) were appliedasdualtaskperformanceonthesameday, witha 40---60min intervalbetweenthem. Patientswereaskedto memorizethetest conditionsandstrategiesusedfor body balancecontrolduringthefirsttest(FT),inordertosmooth andimprovethere-test(RT)performance.
Statisticalanalyses
Data did not follow a normal distribution, thus non-parametric tests were performed. The Wilcoxon test was
usedtodeterminedifferencesbetweenthe:(1)individual equilibriumscoresacrossthesixsensoryconditions(SOT1, SOT2, SOT3, SOT4, SOT5, SOT6); (2) the CS; and (3) the toesupandtoesdownswayenergyscores,betweentheFT andRTperformancesmeasures.TheKruskal---Wallistestand Tukey’smultiplecomparisonswereusedtoverifythe hier-archyofdifferencesbetweengroups.Asignificancelevelof 95%(p<0.05)wasadopted,accordingtothestandardsused inbiologicalstudies.
Results
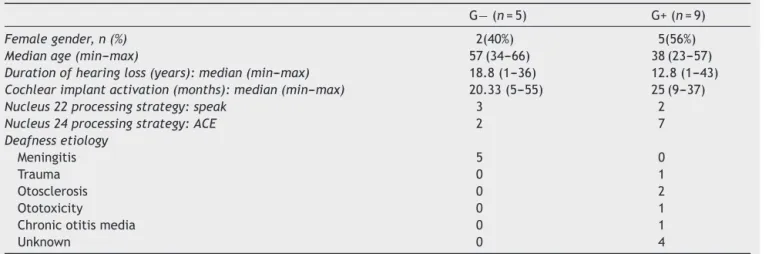
The average age of the 14 patients was 50.43±14.35 yearsandofthesevencontrols47.57±13.5years.Gender distribution was similar between all groups. The char-acteristics of the patients, duration and etiology of the deafness, CIdevice, and activation timeare described in
Table1.
Comparing hearing performance in open-set sentences andmonosyllabic words amongthe groups, includingfree opensetandmonosyllablesdiscrimination,G+showed sim-ilarresultstotheCG(p=0.836andp=0.264,respectively). Bothoutperformed theG− group(p<0.001in bothcases, Kruskal---WallistestandTukey’smultiplecomparisons).The resultsshowthatthehearingperformanceandword discrim-inationofG+ afterCIsurgeryweresimilartoCGsubjects (Table2).
InthefirstCDPtest,bothG+andG−hadsimilar perfor-manceinall six sensorialconditions,but underperformed CG,whoseresultsweresignificantlybetterinSOT3,SOT4, SOT5andSOT6 andCS(Table3).Comparingthe dualtask performance on CDP and the weighted average between alltested conditions,the G+group showed asignificantly better performance at RT in SOT4, SOT5, SOT6, and CS, whichwasnotobservedforG−andCG.IntheCDPretest, G+ outperformed G− in SOT5, SOT6, and CS, suggesting moreeffectivelearninginG+ascomparedtotheothertwo groups(Table4).
IntheADTdualtaskperformance,whencomparingtoes upandtoesdownswayenergymeansscores,nostatistical
Table1 Clinicalanddemographicdataofstudygroupsubjects(n=14).
G−(n=5) G+(n=9)
Femalegender,n(%) 2(40%) 5(56%)
Medianage(min---max) 57(34---66) 38(23---57)
Durationofhearingloss(years):median(min---max) 18.8(1---36) 12.8(1---43)
Cochlearimplantactivation(months):median(min---max) 20.33(5---55) 25(9---37)
Nucleus22processingstrategy:speak 3 2
Nucleus24processingstrategy:ACE 2 7
Deafnessetiology
Meningitis 5 0
Trauma 0 1
Otosclerosis 0 2
Ototoxicity 0 1
Chronicotitismedia 0 1
Unknown 0 4
Table2 Speechrecognitioninopen-setsentencesandmonosyllabicvocaldiscriminationofstudyandcontrolgroupsubjects.
Groups G+ G− CG Kruskal---Wallis
test(p)
Tukey’smultiple comparisons(p)
Open-setsentences Median(min---max) 100(80---100) 0(0---20) 100(100---100) 0.004a G+=CG>G−(<0.001)
Monosylabicvocal discrimination
Median(min---max) 84(58---100) 0(0---88) 100(96---100) 0.001a G+=CG>G−(<0.001)
n 9 5 7
G+,cochlearimplantuserswithgoodhearingperformance;G−,cochlearimplantuserswithpoorhearingperformance;CG,control
group;min---max,minimum---maximum.
aStatisticalsignificancelevel.
Table3 FTresultsaccordingtogroups.
Groups G+ G− CG Kruskal---Wallis
test(p)
Tukey’smultiple comparisons(p)
SOT1FT Median(min---max) 94.3(91.3---95.7) 93(92---97.7) 96(92.3---97) 0.172 G+=G−=CG SOT2FT Median(min---max) 92.7(86.7---94.3) 90(88---96) 94.7(90---97.7) 0.088 G+=G− =CG
SOT3FT Median(min---max) 91(79.7---95.3) 90(82.7---91.3) 94(93.3---97) 0.018a G+=G−<CG(0.036b)
SOT4FT Median(min---max) 68.7(55.3---83) 81.7(29---85.7) 87.7(83.7---93.3) 0.003a G+=G−<CG(0.039b)
SOT5FT Median(min---max) 47.7(0---61.3) 0(0---25.7) 68.7(59.3---76) 0.001a G+=G−<CG(<0.001b)
SOT6FT Median(min---max) 4.3(0---66.7) 0(0---7.3) 66(20---82.3) 0.003a G+=G−<CG(0.001b)
CESFT Median(min---max) 58(42---77) 51(37---58) 81(69---88) 0.002a G+=G−<CG(0.001b)
n 9 5 7
G+,cochlearimplantuserswithgoodhearingperformance;G−,cochlearimplantuserswithpoorhearingperformance;CG,control
group;min---max,minimum---maximum,CDP,computerizeddynamicposturography;SOT,sensoryorganizationtest;CES,compositescore;
FT,firsttest.
aStatisticalsignificancelevel.
b CGshowedsignificanthigherscoresascomparedtoG+andG−inSOT3,SOT4,SOT5,SOT6,andCESconditions.
difference between the groups could be found (p=0.616 and0.563,atbothtestsconditions,Kruskal---Wallistestand Tukey’smultiplecomparisons).
In the P3 test, this study observed significantly longer P3latenciesamongG−ascomparedtoG+andCGforthe 2000/1000and1000/1500Hztestconditions(p=0.007and
p<0.001fortheformer;p=0.001andp<0.001forthelatter test),butnodifferencebetweenG+andCG(p=0.177and
p=0.601)(Kruskal---WallistestandTukey’smultiple compar-isons),asshowninTable5.
Discussion
TheCDPisanobjective,non-invasivetest.Dualtask perfor-mancewaschosen, withabriefintervalbetweenthemto assessshort-termlearningandmemoryabilityaspartof pos-turalrecoverystrategies.Thechoiceoftheintervalbetween eachperformanceallowedarestperiodofabout40---60min. Thus,thepatientcouldrecoverfrommuscular effort dur-ingFTtoensurethatfatiguewouldnotinterfereduringRT, sotheRTresultwouldreflectonlytheshort-termmemory
Table4 RTresultsaccordingtogroups.
Groups G+ G− CG Kruskal---Wallis
test(p)
Tukey’smultiple comparisons(p)
SOT1RT Median(min---max) 94(90.3---95.3) 94.7(90.7---95) 95.7(94.7---97.7) 0.005a G+=G−<CG(0.012b)
SOT2RT Median(min---max) 90.3(85---94.3) 89.3(83---92) 94(90.7---97.7) 0.012a G−<CG(0.010b)
SOT3RT Median(min---max) 89.3(76.3---95.7) 90(80---95) 93.3(92---97.7) 0.076 G+=G−=CG SOT4RT Median(min---max) 82(64.3---88.3) 85.7(40---90) 88.3(85.3---95.3) 0.023a G−<CG(0.050b)
SOT5RT Median(min---max) 64.3(0---78.3) 0(0---29.3) 74.7(59.3---80.3) 0.007a G−<G+<CG(0.001b)
SOT6RT Median(min---max) 27.3(0---70.7) 0(0---0) 77.3(38---81.7) 0.001a G−<G+<CG(<0.001b)
CESRT Median(min---max) 66(48---82) 52(39---58) 83(72---89) 0.001a G−<G+<CG(<0.001b)
G+,cochlearimplantuserswithgoodhearingperformance;G−,cochlearimplantuserswithpoorhearingperformance;CG,control
group;min---max,minimum---maximum;CDP,computerizeddynamicposturography;SOT,sensoryorganizationtest;CES,compositescore;
RT,re-test.
aStatisticalsignificancelevel.
Table5 P3latenciesinthe2000/1000Hzand1000/1500Hztestconditionsaccordingthestudygroup.
G+(n=9) G− (n=5) CG(n=7) Kruskal---Wallis test(p)
Tukey’smultiple comparisons(p)
P3latency 2000/1000Hz
Median (min---max)
351(327---450) 423(399---492) 342(261---351) 0.006a G−>G+=CG(<0.001a)
P3latency 1000/1500Hz
Median (min---max)
345(330---474) 457.5(450---501) 351(308---390) 0.023a G−>G+=CG(<0.001a)
G+,cochlearimplantuserswithgoodhearingperformance;G−,cochlearimplantuserswithpoorhearingperformance;CG,control
group;min---max,minimum---maximum.
a Statisticalsignificancelevel.
ability.10 The CS improvement during RT is expected for thosesubjectswhohavenormalshort-termlearningability andproperhippocampusfunction.
Thesmallsamplesizeresultsfromtherestrictive selec-tioncriteria: onlypatientswithfull CIelectrodeinsertion wereincluded,inordertoeliminatesurgicalbias.Ageand CI activation time were used as group pairing variables, becauseitisknownthatbothcouldchangeSOTperformance andP3latencies.11,12
ThebetterRTperformanceofG+inSOT4,SOT5,SOT6, andCSsuggeststhatCIsubjectsareableto‘‘learn’’the pre-sentedsensoryconditionsintheFTandusethislearningand memoryabilityduringRT.Thisabilitycomesfroman accu-rate CNS sensoryinput integration,responsible for motor strategies to assure body balance control.10 Thus, these subjectsactuallyhaveanaccurateshort-termmemoryand learningability.ThedifficultyoftheG−patientscouldbe attributedtofunctionalimpairmentof structuresinvolved withspeechdiscrimination,stimulusrecognition,and learn-ingskills,abilitiesrequiredtogenerateappropriatemotor responsesforposturalcorrectionaswellasstabilizationand balancecontrol.ConsideringthatCGshowedagreater FT response,asignificantimprovementinRTwasnotexpected, whichisinagreementwiththeresults(Table4).
Hearingprovidesacousticinformationaboutthe environ-ment,enablingustonoticeandavoidenvironmentalhazards that may lead toa fall.6 Studies testing the associations betweenhearingacuityandposturalbalancearescarceand showconflicting results.Occupational health studieshave shownacorrelation betweennoiseexposureandimpaired posturalbalance.13,14Studyingolderfemaletwins,Viljanen etal.6showedthat poorhearingacuityincreasedtherisk offallswhencomparedtosisterswithgoodhearingacuity, whichcouldbepartiallyexplainedbytheirpoorerpostural control. The present study observed longer P3 latencies in CI users with poor hearing performance, as compared to CI recipients withgood hearing performance and con-trols.Thesefindingsindicatethathearingimpairmentmay directlyorindirectlyinterfereincognitivetasksevaluated by the P3test. The same group G− showed a worse CDP performancecomparedtotheothergroups.Postural stabil-ityduring staticand dynamic taskscould bedescribed as theabilitytomodulateposturalresponsemagnitude,thus generatinganaccuratemotorresponse.Itshouldbe remem-beredthat postural controlcomes fromand relieson the interactionbetween somatosensory, vestibular, andvisual systems,andthatposturalimbalanceincreaseswith increas-ing number of underlying affected systems. Although the
auditory system is not usuallycited and included in cen-tralprocessingintegrationof peripheralinputsinvolvedin posturalcontrol,thesefindingssuggestadirectorindirect influenceofhearing,demonstratedbytheworseSOTresults ofG−withpoorauditoryperformance.
Toes-up or toes-down tilts of a platform on which a subjectstands induce early responses of the leg muscles stretchedandlateresponsesintheantagonistmuscles.The supportsurfaceisslowlyrotatedabout8degreeswhilethe bodyisstationary.Therotationalmovementoftheplatform triggersanautomaticposturalresponseasdefenseagainst theposturaldisturbance.AccordingtoNardoneetal.,15the originofthelateresponsesintheantagonistmusclecomes fromtheoverall posturalimbalance andthe posturalset. Thus, it does not correlate with or depend on cognition. Whenanalyzing ADTdualtaskperformanceresults,it was notpossibletofindastatisticaldifferencecomparingFTand RTamongthegroups.SinceADTisusedtoinvestigatethe automaticpostural control,memoryandcognitionarenot requiredforthistask.Therefore,divergingresultsbetween groupswerenotexpectedaswereduringSOTconditions.15 Long-latency components of event-related potentials (liketheP3)correlatewiththeabilityofsubjectstodetect and process unexpected, novel, or task-relevant stimuli. Task-relevantlatepositivecomponentscanberecordedin theneocortex andhippocampuswhileperformingan audi-tory discrimination task.16 The cortical potential elicited inthe contextof auditory target detectiontasks includes theN1,P2,andP3components.Theconcordancebetween magnetoencephalographic(MEG)andbrainelectric source analysis(BESA) source localization supports the notion of generators in temporal lobes for the N1/P2 complex and generatorsin temporal andhippocampal areas for the P3 component.17 Thus, as literature reports, CNS structures functionallyinvolvedwithexplicitmemorygiveriseto audi-tory,visual,andsomatosensorycentralintegration,andcan belocalizedinthehippocampusandtemporallobe.16,17 In fact,Viljanenetal.6havealreadyreportedhearinglossas apredictoroffallsandpoorerposturalbalancecontrol.In their study,6 pure tone thresholds were reported without speechreceptionthresholds. Therefore it is possible that thehigherriskoffallsinthissamplemaynotberelatedto hearinglossitself,butrathertoalackofsensoryinputor cognitiveimpairment.
factthat25subjectscouldnotbecontactedbyphoneand thatsomelivedtoofar awaytoenterthestudy.Only five patientshadpoorhearingperformance,reflectingthe selec-tioncriteriaforCIsurgeryforpost-lingualdeafpatientsat thiscenterandindicating thatalmostallCIsurgerieswith complete electrode insertionwere successful toestablish usefulhearingandspeechdiscrimination.Duetothestrict inclusioncriteriaasmallnumberofsubjectsineachgroup were expected,reducing statistical power, so more stud-iesincluding patients from multiple CI centersshould be conductedtoovercomethislimitation.
Itisnotpossibletoaffirmthatthefindingsareexclusively relatedtoauditoryand/orvestibularneuralpathway impair-ment,becauseallG−patientsweredeafduetomeningitis. Besidescausingdeafness,meningitiscanalsoaffectseveral otherfunctionalandanatomicalCNSareas.2,18,19Asthegoal wastoevaluate posturalrecovery in CIusers,G+and G− groupshadtoshowdistinctauditoryperformance,so etiol-ogyofhearinglosswasnotequallydistributedamongboth groups.Neithercanitbeclaimedthattheresultsarisefrom learningand memory network involvement. Thus,further studiesarenecessarytoclarifythesequestions.
According to the results, postural recovery appears to berelatedtolearningandmemory,aswellastospeechand auditoryperformance.Itisalsopossiblethatacompromised networkinterferesinbothauditoryperformanceand learn-ingstrategiesnecessaryforbodybalancecontrol.Ifproven tobeeffective,therelationshipbetweenauditoryand vesti-bularpathwaysopensanewresearchfield,andstrengthens the role of cognitive auditory potentials and speech dis-criminationtestsaspredictorsofposturalperformanceand vestibularrehabilitation.
Conclusions
Comparing the dual task performance in CDP and the weightedaverage between alltested conditions,cochlear implantuserswithgoodhearingperformanceshowed bet-terre-test resultsin SOT4, SOT5, SOT6, andCS, and also had a higher index of postural recovery, as compared to CIuserswithpoor hearingperformance.Cochlearimplant users without good hearing performance had significantly lowerlevels of short-termlearning ability than the other twogroupsinSOT5,SOT6,andCS.
Funding
FundedbyConselhoNacionaldeDesenvolvimentoCientífico eTecnológico---CNPQ.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.AndersonG,HagmanJ,TalianzadehR,SvedbergA,LarsenHC. Effect of cognitiveload on posturalcontrol. BrainRes Bull. 2002;58:135---9.
2.SchmidtH,HeimannB,DjukicM,MazurekC,FelsC,Wallesch CW,etal.Neuropsychologicalsequelaeofbacterialandviral meningitis.Brain.2006;129Pt2:333---45.
3.JacobsonGP,NewmanCW,Kartush JM.Handbookofbalance functiontesting.StLouis:MosbyYearBook;1993.
4.JahnK,WagnerJ,DeutschländerA,KallaR,HüfnerK,StephanT, etal.Humanhippocampalactivationduringstanceand locomo-tion:fMRIstudyonhealthy,blind,andvestibular-losssubjects. AnnNYAcadSci.2009;1164:229---35.
5.Jones GM. Posture. In: Kandel ER, Schwartz JH, Jessell T, editors.Principlesof neural science. 4thed.New York, NY: McGraw-Hill;2000.p.816---31.
6.ViljanenA,KaprioJ,PyykköI,SorriM,PajalaS,KauppinenM, etal.Hearingasapredictoroffallsandposturalbalanceinolder femaletwins.JGerontolABiolSciMedSci.2009;64:312---7.
7.DoyonJ.Motorsequencelearningandmovementdisorders.Curr OpinNeurol.2008;21:478---83.
8.SmithPF.Vestibular---hippocampalinteractions.Hippocampus. 1997;7:465---71.
9.Ben-DavidJ,TeszlerCB,DuchmanH,PodoshinL.Evaluationof tulliophenomenonbycomputerizeddynamicposturography.Int TinnitusJ.1997;3:105---12.
10.Tjernstrom F, Fransson PA, Hafstrom A, Magnusson M. Adaptation of postural control to perturbations --- a pro-cess that initiates long-term motor memory. Gait Posture. 2002;15:75---82.
11.KagaK,KoderaK,HirotaE,TsuzukuT.P3responsetotonesand speechsoundsaftercochlearimplant:acasereport. Laryngo-scope.1991;101:905---7.
12.Kubo T, YamamotoK, IwakiT, Matsukawa M, Doi K, Tamura M.Significanceofauditoryevokedresponses(EABRandP3)in cochlearimplantsubjects.ActaOtolaryngol.2001;121:257---61.
13.KilburnKH,WarshawRH,HanscomB.Arehearinglossand bal-ancedysfunctionlinkedinconstructionironworkers?BrJInd Med.1992;49:138---41.
14.JuntunenJ,MatikainenE,YlikoskiJ,YlikoskiM,OjalaM,Vaheri E. Postural bodysway and exposure to high-energy impulse noise.Lancet.1987;2:261---4.
15.Nardone A, Giordano O, Corra T, Schieppati M. Response of leg muscles in human displaced while standing. Brain. 1990;113:65---84.
16.BrankackJ,SeidenbecherT,Müller-GärtnerHW.Task-relevant latepositivecomponentinrats:isitrelatedto hippocampal thetarhythm?Hippocampus.1996;6:475---82.
17.Tarkka IM, Stoki´c DS, Basile LF, Papanicolaou AC. Electric sourcelocalization of theauditory P3 agreeswithmagnetic source localization. Electroencephalogr Clin Neurophysiol. 1995;96:538---45.
18.HugossonS,CarlssonE,BorgE,BrorsonLO,LangerothG,Olcén P.Audiovestibularandneuropsycologicaloutcomeofadultswho hadrecoveredfromchildhoodmeningitis.IntJPediatr Otorhi-nolaryngol.1997;42:149---67.