www.revportcardiol.org
Revista
Portuguesa
de
Cardiologia
Portuguese
Journal
of
Cardiology
ORIGINAL
ARTICLE
Profiles
of
hospitalized
patients
with
valvular
heart
disease:
Experience
of
a
tertiary
center
Ana
Fátima
Esteves
a,
Dulce
Brito
a,∗,
Joana
Rigueira
a,
Inês
Ricardo
a,
Raquel
Pires
b,
Mónica
Mendes
Pedro
a,
Fátima
Veiga
a,
Fausto
Pinto
aaCardiologyDepartment,HospitaldeSantaMaria,CHLN,CCUL,CentroAcadémicodeMedicinadeLisboa,FaculdadedeMedicina
daUniversidadedeLisboa,Portugal
bCardiovascularResearchSupportUnit(GabinetedeApoioàInvestigac¸ãoCardiovascular-GAIC),CCUL,CentroAcadémicode
MedicinadeLisboa,FaculdadedeMedicinadaUniversidadedeLisboa,Portugal
Received26December2017;accepted1February2018
KEYWORDS Valvularheart disease; Epidemiology; Hospitalization; Aorticstenosis; Mitralregurgitation Abstract
Introduction:Valvularheart disease(VHD)isincreasingworldwide,mostlybecauseofaging. Percutaneousvalveinterventionisthepreferredtherapeuticoptioninhigh-riskpatients.
Objective: TocharacterizetheprofilesofpatientswithVHDadmittedtothecardiologyward atatertiaryreferralcenter.
Methods:On thebasisofICD-9codes forVHD,thedischargenotesof287patients hospital-izedovera22-monthperiodwerereviewedandanalyzed.Onehundredcharacteristicswere considered.
Results:Medianagewas74(23-93)years,and145(51%)weremale.Theadmissionswere elec-tive(forvalveintervention)in36%.Heartfailure(HF)wasthereasonforurgentadmissionsin 29.3%.Multiplecomorbiditieswereobservedin53%ofpatients.EtiologyofVHDwas degenera-tivein68%,functionalin15.3%andrheumatic(predominantlyinwomenandyoungerpatients) in8.7%.Aorticvalvediseasewaspresentin63%(aorticstenosisin56%),andwasassociated withHF(p=0.004),atrialfibrillation(AF)(p=0.01),andleftventricular(LV)dilatation(p=0.003) orhypertrophy(p<0.001).Mitralvalvedisease(51%),mostlymitralregurgitation(degenerative orfunctional),predominatedinwomen,andwasassociatedwithHF,AF,LVdilatation(p<0.001) andreducedLVejectionfraction(p=0.003).Significanttricuspidregurgitation(34.8%) associ-atedwiththepresenceofpreviouslyimplantedcardiacdevices(p<0.001).Valveintervention (mostlytranscatheteraorticvalveimplantation)wasperformedin41%ofpatients.Meanlength ofhospitalstaywas12±14.3daysandoverallin-hospitalmortalitywas9.8%.
AnaFátimaEstevesandDulceBritoarebothfirstauthorsinthestudy.
∗Correspondingauthor.
E-mailaddress:[email protected](D.Brito). https://doi.org/10.1016/j.repc.2018.02.012
0870-2551/©2018SociedadePortuguesadeCardiologia.PublishedbyElsevierEspa˜na,S.L.U.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Conclusions:Nowadays,theprofilesofhospitalizedpatients withVHDaredominatedbythe elderly,withdegenerativediseaseandmultiplecomorbidities,presentingwithHF,AFandLV remodeling,whofrequentlyundergovalveintervention,usuallyviaapercutaneousapproach. Mortalityremainssignificantinthishigh-riskpopulation.
©2018SociedadePortuguesadeCardiologia.PublishedbyElsevierEspa˜na,S.L.U.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE
Doenc¸avalvular cardíaca; Epidemiologia; Hospitalizac¸ão; Estenoseaórtica; Regurgitac¸ãomitral
Perfisdedoenteshospitalizadoscomdoenc¸acardíacavalvular:experiênciadeum centroterciário
Resumo
Introduc¸ão:A doenc¸acardíacavalvular (DCV)éproblemacrescente,relacionando-secomo envelhecimentopopulacional.Aintervenc¸ãovalvularporviapercutâneaéopc¸ãopreferencial emalgunscontextos,inclusiveemdoentesdeelevadorisco.
Objetivo:Caracterizac¸ãodoperfildominantedodoentecomDCVadmitidoemenfermariade cardiologia(centroterciáriodereferência).
Métodos: Revisãodeprocessosclínicosde287doentes(códigosICD-9paraDCV)internadosnum períodode22meses.Foramconsideradasparaanálise100características.
Resultados: Idade-74(23-93)anos;145(51%)homens.Admissõeseletivas(intervenc¸ão valvu-lar):36%.Insuficiência cardíaca (IC):causa deadmissãourgente em 29,3%.Comorbilidades múltiplas: 53% dos doentes. Etiologias: degenerativa (68%); funcional (15,3%); reumática (8,7%)--- predominantementeem mulheres eem doentesmaisjovens. Doenc¸avalvular aór-tica-63%(estenoseem56%),associou-seàpresenc¸adeIC(p=0,004),fibrilhac¸ãoauricular (FA)-p=0,014---ehipertrofia(p<0,001)oudilatac¸ãoventricularesquerda(VE)---p=0,003. Doenc¸avalvularmitral(51%)-predominantementeregurgitac¸ão-degenerativaoufuncional, maisfrequente em mulheres; associou-seà presenc¸a deIC, FA, dilatac¸ão VE ---p< 0,001 -efrac¸ão deejec¸ão VEdiminuída (p=0,003).Insuficiênciatricúspide(34,8%), associou-seà presenc¸adeeletrocatéterespreviamenteimplantados(p<0,001).Intervenc¸õesvalvulares:41% dosdoentes,predominantementeTAVI.Durac¸ãodeinternamento:12±14,3dias;mortalidade globalintra-hospitalar:9,8%.
Conclusões:OperfilatualdodoentehospitalizadocomDCVédominadopeloidosocomdoenc¸a degenerativaemúltiplascomorbidades,apresentandoremodelagemVE,ICeFA,esendo fre-quentementesubmetido aintervenc¸ãovalvular(predominantementeporviapercutânea).A mortalidadeésignificativanessapopulac¸ãoderiscoelevado.
©2018SociedadePortuguesadeCardiologia.PublicadoporElsevierEspa˜na,S.L.U.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Valvular heart disease (VHD) has recentlybeen described as‘‘thenext cardiacepidemic’’,1 in particular dueto its
increased prevalence in the elderly mainly from degen-erative causes in industrialized countries.1,2 However,
rheumaticetiologyisstillthemostfrequentcauseofVHD indevelopingcountriesandpredominantlyaffectsyounger populations.3
Theepidemiology ofVHDis especiallydifficult tostudy asmostcases runtheir naturalhistory without significant symptomsforvarying periodsoftime,andimagingstudies (particularly echocardiography) are required for accurate diagnosis and characterization.2,3 Based on data from
largepopulation-based epidemiologicalstudies in theUSA whichincludedindividualsfromthegeneralpopulationwho had been assessed prospectively with echocardiography,3
the estimated prevalence of significant VHD in developed countries is 2.5%. Mitral regurgitation (MR) wasfound to be the most frequent VHD, especially in the elderly.3
However,intheEuroHeartSurvey,aprospectivestudy con-ducted in 25 European countries that included inpatients and outpatients with moderate to severe VHD, infective endocarditis, or prior valve intervention,4 the most
fre-quentVHD(43.1%)wasaorticstenosis(AS),predominantlyof degenerativecause.Rheumaticetiologywasfoundin22%of cases.4
PublisheddataclearlyshowahighprevalenceofASand MR in industrialized countries, where VHD mainly affects the elderly population due to increased life expectancy, and in association with functional and structural cardiac abnormalities.2,5VHDislinkedtosignificantcardiovascular
andall-causemortality,independentlyofventricular func-tionandcomorbidities.5
DegenerativeAS,aconsequenceofacontinuousprocess ofvalvesclerosisandcalcification,6 increasessignificantly
in prevalence withage,2,3,6,7 and around40% of
individu-als aged over 75 years areestimated to have a calcified aortic valve. When intervention is indicated, the deci-sion between surgical aortic valvereplacement (SAVR) or transcatheter aortic valve implantation (TAVI) should be madebytheheartteamaccordingtotheindividualpatient’s characteristics.8
Functional MR is the most frequent valve disease in theUSA,3,9,10 asaconsequenceoftheleftventricular(LV)
remodeling and dilatation commonly seen in both non-ischemiccardiomyopathy(mostlyduetohypertensiveheart diseaseoridiopathicdilatedcardiomyopathy)andischemic heart disease.10 As theprevalence ofheart failure(HF)is
increasing, functional MR is also likelyto increase in the future.Inpatientswithsevereprimaryorsecondary (func-tional)MR,inadditiontooptimalmedicalmanagementof HF,11valverepairorreplacementmaybenecessary,andthe
recentadventofpercutaneoustechniqueshasprovidedan effectiveandsafewayofimprovingHFsymptomsinsuitable candidates.8,11,12
Indeveloping countriesrheumaticheartdisease(which mainlyaffectsthemitralvalve) isstillthemajorcauseof VHD,duetothepersistentlyhighprevalenceofrheumatic fever,andisassociatedwithreducedlifeexpectancy.2,13,14
The prevalence of rheumatic heart disease in developed countrieshasdecreased,butasdegenerativevalvedisease affectingtheelderlyisincreasing,14theburdenofVHDwill
islikelytogrowsubstantiallyinthefuture.3
Thepresentstudyaimstocharacterizethecurrent pro-filesofpatientswithsignificantVHDadmittedoveraperiod of22consecutivemonthstothecardiologywardatalarge referraltertiaryhospitalcenterinsouthwesternEurope (Lis-bon,Portugal).
Methods
Datasources
Patient data were acquired by searching for electronic discharge notes coded with a diagnosis of valve disease according to the International Classification of Diseases, Ninth Revision(ICD-9)of allpatientsadmitted tothe car-diologywardinthe CardiologyDepartmentofSanta Maria UniversityHospitalbetweenJanuary1,2014andOctober3,
2015(seeAppendix1fordetails).
Thesearchidentified391patients,whosedischargenotes were then manually reviewed. Only patients with signif-icant VHD and those withprior heart valve interventions were selected. Accordingly, only patients who underwent echocardiographic assessment during the hospitalization understudy(indexhospitalization)wereincluded.
Significant VHD was defined on the basis of clinical plus imaging criteria (mainly echocardiography),15,16 and
includedmoderatetoseverevalvularstenosisand/or regur-gitationofanycardiacvalve(ormultiple valves)thatwas responsible in any wayfor the index hospitalization.Left ventricular ejection fraction (LVEF) was considered to be reducedif<50%.17
Studypopulationanddesign
In accordance with the above criteria, 66 patients were excludedforpresentingonlymildvalvulardisease; addition-ally,38patientswerealsoexcludedbecauseofinsufficient informationavailableinthesystem(patientsadmitted elec-tivelyto undergo selective examinations only or patients withhospitalstaylessthan24hours).Thefinalstudy popu-lationincluded287patients.
Dischargenotesof thesepatientswerecarefully manu-allyreviewed.InadditiontocharacterizationofVHD(valves involved,diseaseseverityandetiology)onthebasisofall theavailableinformation,thefollowingdatawerecollected andanalyzed:demographics(gender,age, ethnicity,place ofbirth),admissionanddischargedates,typeofadmission tothecardiologyward(electiveorurgent),mainreasonfor hospitaladmission,lengthofhospitalstay(LOS),major car-diovascular risk factors (systemic hypertension, diabetes, dyslipidemia,smoking),presenceandtypeofcomorbidities, historyofchronicHFandNewYorkHeartAssociation(NYHA) functionalclass,presenceofadvancedatrioventricular(AV) block,bundlebranchblock (BBB)oratrial fibrillation(AF) (chronic or new-onset), presence of pulmonary hyperten-sion(assessedinvasivelyorbyechocardiography),coronary artery disease (CAD) (assessed by coronary angiography), coronary artery bypass grafting (CABG) during the index admission,implantedcardiacdevices(duringtheindex hos-pitalization or in the past), valvular intervention (during the index hospitalization or in the past), hospital admis-sions due to VHD in the 12 months preceding the index hospitalization,mortality(andcause of death) duringthe indexhospitalization,anddestinationafterdischarge. Var-ious echocardiographic parameters and indices (assessed during the index hospitalization before any new valvular intervention)werealsocollected,includingcardiac cham-bersize and measures of systolicLVand right ventricular (RV)function.
In addition to the descriptive data, we looked for associations between the type and etiology of VHD and demographic, clinical, electrocardiographic and echocar-diographic features, in order toimprove characterization oftheprofilesofhospitalizedpatientswithVHD.
Statisticalanalysis
ThestatisticalanalysiswasperformedwithMicrosoftExcel 2013® and IBM SPSS® version 22.0. A descriptive analy-sisof the different variables was performed and possible differences between genders were assessed. Quantitative variables are expressed as means ± standard deviation, andqualitativevariablesasabsoluteorrelativefrequencies (percentages).TheStudent’sparametricttestfor indepen-dentvariableswasusedtocomparequantitativevariablesas afunctionofthepresenceandtypeofVHD(mitral,aortic, mitral-aorticortricuspidvalvedisease).Categorical varia-bles wereanalyzed usingthe chi-square test and Fisher’s exact test, as appropriate. Possible associations between typeofVHDanddemographic,clinical,electrocardiographic andechocardiographicfeatureswereanalyzed using Pear-son’scorrelationtest.
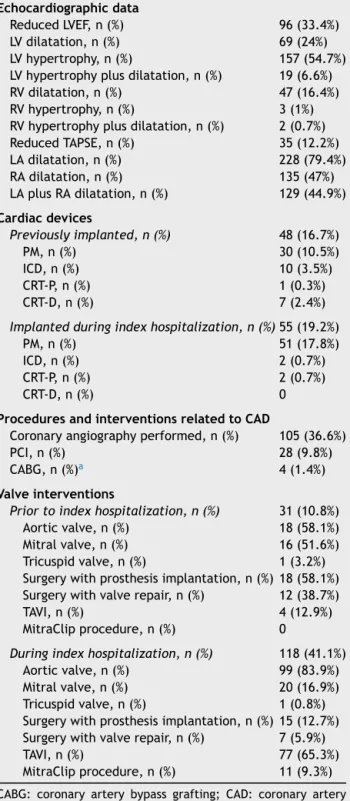
Table1 Populationwithvalvularheartdisease: character-isticsandprocedures.
Echocardiographicdata
ReducedLVEF,n(%) 96(33.4%) LVdilatation,n(%) 69(24%) LVhypertrophy,n(%) 157(54.7%) LVhypertrophyplusdilatation,n(%) 19(6.6%) RVdilatation,n(%) 47(16.4%) RVhypertrophy,n(%) 3(1%) RVhypertrophyplusdilatation,n(%) 2(0.7%) ReducedTAPSE,n(%) 35(12.2%) LAdilatation,n(%) 228(79.4%) RAdilatation,n(%) 135(47%) LAplusRAdilatation,n(%) 129(44.9%) Cardiacdevices Previouslyimplanted,n(%) 48(16.7%) PM,n(%) 30(10.5%) ICD,n(%) 10(3.5%) CRT-P,n(%) 1(0.3%) CRT-D,n(%) 7(2.4%)
Implantedduringindexhospitalization,n(%) 55(19.2%) PM,n(%) 51(17.8%) ICD,n(%) 2(0.7%) CRT-P,n(%) 2(0.7%)
CRT-D,n(%) 0
ProceduresandinterventionsrelatedtoCAD
Coronaryangiographyperformed,n(%) 105(36.6%) PCI,n(%) 28(9.8%) CABG,n(%)a 4(1.4%) Valveinterventions
Priortoindexhospitalization,n(%) 31(10.8%) Aorticvalve,n(%) 18(58.1%) Mitralvalve,n(%) 16(51.6%) Tricuspidvalve,n(%) 1(3.2%) Surgerywithprosthesisimplantation,n(%)18(58.1%) Surgerywithvalverepair,n(%) 12(38.7%) TAVI,n(%) 4(12.9%) MitraClipprocedure,n(%) 0
Duringindexhospitalization,n(%) 118(41.1%) Aorticvalve,n(%) 99(83.9%) Mitralvalve,n(%) 20(16.9%) Tricuspidvalve,n(%) 1(0.8%) Surgerywithprosthesisimplantation,n(%)15(12.7%) Surgerywithvalverepair,n(%) 7(5.9%) TAVI,n(%) 77(65.3%) MitraClipprocedure,n(%) 11(9.3%)
CABG: coronaryartery bypass grafting; CAD: coronary artery disease; CRT-D: cardiac resynchronization therapy defibrilla-tor;CRT-P:cardiacresynchronizationtherapypacemaker;ICD: implantable cardioverter-defibrillator; LA: left atrium; LOS: lengthofhospitalstay;LV:leftventricular;LVEF:leftventricular ejectionfraction;PCI:percutaneouscoronaryintervention;PM: pacemaker;RA:rightatrial;RV:rightventricular;SAVR:surgical aorticvalvereplacement;TAPSE:tricuspidannularplanesystolic excursion;TAVI:transcatheteraorticvalveimplantation.
aTwopatientsalsounderwentSAVR.
Ap-valueof<0.05foraconfidence intervalof95%was consideredstatisticallysignificant.
Results
Populationcharacteristicsandinterventionsaredisplayedin
Table1.
Populationandhospitalization-relateddata
The study population included 142 females (49.5%) and 145 males (50.5%), mean age 74.86±13.39 years (range 23 to 93), with no difference between genders. Most patientswereborninPortugaland11%wereoriginallyfrom Portuguese-speakingAfricancountries.
The majority of patients were admitted through the emergency room or by transfer from other departments orhospitals(66.9%),while33.1%wereelectiveadmissions. Fifty-sixpatients(19.51%)werehospitalizedforcausesnot directlyrelatedtoVHD,primarilywithacutecoronary syn-drome(ACS)(71.4%ofthesecasesand16.4%ofallpatients withVHD),andvalvulardiseasewasasecondarydiagnosis.
Regardingallpatients witha diagnosisof VHD, decom-pensated HF wasthe most frequent reason for admission (84patients,29.3%).Thisproportionwasevenhigherinthe groupof231patientsadmittedforVHD(35.5%).Eighty-four (36.4%)wereadmittedelectivelyforvalveintervention,70 (24.4%)becauseofadysrhythmia(AFin9.1%),15(5.2%)in thecontextofasyncopalepisode(fourofwhichweredue tocomplete AVblock), and seven (2.4%)due to infective endocarditis.
Fortypatients(13.9%)hadbeenhospitalizedforreasons relatedtoVHDinthe12monthsprecedingtheindex hospi-talization.
Etiologyandtypeofvalvulardisease
Etiologies and types of valvular disease are shown in
Figure 1. Most patients (67.9%) had degenerative
aor-tic and/or mitral valve disease, followed in frequency (15.3%) by significant functional mitral and/or tricuspid regurgitation(TR)(secondary toleftand/or right ventric-ular dilatation due to ischemic heart disease or dilated
Degenerative (n=195) Functional (n=44) Rheumatic (n=25) IE (n=11) MVP (n=8) Congenital (n=2 Aortic and/or mitral VHD Functional MR and/or TR )
Figure1 Etiologies ofvalvular heartdisease. IE:infectious endocarditis;MR:mitralregurgitation;MVP:mitralvalve pro-lapse;TR:tricuspidregurgitation;VHD:valvularheartdisease.
cardiomyopathy).Rheumaticetiologywasdiagnosedin8.7% ofpatients.Otheretiologiesincludedinfectious endocardi-tis(3.8%),mitralvalveprolapse(2.8%),andcongenitalVHD (0.7%).
Mostpatientswithrheumaticvalvediseasewerewomen (84%, p<0.001), with no significant gender differences observed in other etiologies. Agecorrelated directly with degenerativeetiology(r=0.473;p<0.001),andinverselywith rheumaticdisease(r=-0.36;p<0.001).
Aorticvalvediseasewasdocumentedinmostcases(181 patients,63.1%),ofwhom89%(56%ofallpatients)hadAS, and27.1%(17.1%ofallpatients)hadaorticvalve regurgita-tion.Mitraldiseasewasdiagnosedin146patients(50.9%), mostlyMR (90.4%,46%ofallpatients);mitralstenosiswas observed in 15% of these patients (7.7% of all patients). Concomitantaorticandmitralvalvediseasewaspresentin 22.3%ofpatients.
There were no documented cases of tricuspid valve stenosis, but significant TRwasdiagnosed in 100patients (34.8%), and was associated with mitral valve disease in 69patients(69.7%ofpatientswithTR,24%ofallpatients). Isolatedmoderate tosevere TR wasobserved in 20 cases (6.97%).
Moderatepulmonaryvalveregurgitationwasinfrequent (13patients),andwasdiagnosedinthecontextof predomi-nantmitralvalvediseaseandTR;itdidnotrequiretargeted therapeuticinterventioninanypatient.
Cardiovascularriskfactorsandothercomorbidities
AsignificantproportionofpatientsadmittedhadchronicHF (39.4%), and47.4% hadchronic AF.Systemic hypertension wasthemostfrequentcardiovascularriskfactorobserved, presentin219(76.3%)patients,while177(61.7%)patients hadmorethanoneoftheclassicalcardiovascularrisk fac-tors.Multiplecomorbiditieswerefoundin53%ofpatients. The most common was CAD (n=81; 28.21%), followed by chronickidneydisease(n=60;20.9%),chronicanemia(n=76; 26.5%),chronic pulmonary disease(n=43; 15%) and malig-nancies(n=39;13.6%).
Coronary angiographywasperformed in 105 (36.6%)of patients, mostlyin the contextof ACS, but alsodue to a previoushistory ofCADor asastandard procedurebefore valveintervention. Significant CADwasdocumented in 55 (52.4%)ofcases.Coronaryrevascularizationwasperformed in32(11.1%)patients,byapercutaneousapproachin28and byCABGinfour.
Electrocardiographicdata
AFwasdiagnosedin136 (47.4%)patients,andwas signifi-cantlyassociatedwithaorticvalvedisease(p=0.014),mitral valvedisease(p<0.001)orTR(p<0.001).AdvancedAVblock wasalsofrequent,with29patients(10.1%)havingcomplete AVblockatpresentation(16patientswithASand13withMR; AS and MR coexisted in fivepatients). CompleteAVblock wastheprimaryreasonforpacemakerimplantationinthe indexhospitalization.However,itwasnotafrequently doc-umented cause of syncope onadmission. Other causes of syncope at presentation weresinus node dysfunction and ventriculartachycardia.
Echocardiographicdata
Reduced(<50%)LVEFwasdocumentedin33.4%ofpatients andwasassociatedwithmitraldisease(p=0.003).In12.2% ofpatientsRVlongitudinalsystolicfunctionassessedby tri-cuspid annular plane systolic excursion (TAPSE) was also compromised,coexistingwithLVsystolicdysfunctionin22 (62.9%)patients.
LVdilatation(24%)andLVhypertrophy(54.7%)wereboth associatedwith aortic valvedisease, but only the former withmitraldisease.Theleftatriumwasdilatedin79.4%of patients,buttherewasnosignificantassociationwithaortic ormitralvalvedisease.RVdilatationwaspresentin16.4% ofcasesandrightatrial dilatation in47%;bothconditions wereassociatedwiththepresenceofsevereTR.
Cardiacdevices
Forty-eight(16.7%)patients hadacardiac devicein place priortotheindexadmission:apacemaker(PM)in30(10.5%), an implantedcardioverter-defibrillator (ICD)in 10 (3.5%), and a cardiac resynchronization therapy (CRT) device in eight(2.7%)patients. Severe chronic TRwasdocumented in62.5%ofthesepatients,andwasassociatedwithmitral valvediseasein21(43.8%;significantchronicMRin50%of these)andwithaorticvalvediseasein10patients(20.8%; moderateorsevereASin41.7%).
Inaddition,in55patients(19.2%)adevicewasimplanted forthefirsttimeduringtheindexhospitalization:aPMin 51(17.8%)patients,anICDintwo(0.7%),andaCRT pace-makerinanothertwo.
Associations
between
valvular
heart
disease
and
demographic,
clinical
and
functional
data
Aorticvalvedisease
Diseaseoftheaorticvalveshowednogenderpredominance, butcorrelateddirectlywithage(p<0.001),degenerative eti-ology(p<0.001)andpresenceofHF(p=0.004),AF(p=0.014), LVdilatation(p=0.003),andLVhypertrophy(p<0.001).There wasnosignificantassociationbetweenaorticvalvedisease andrheumaticetiology,reducedLVEF,leftatrial(LA) dilata-tion,AVblockorbundlebranchblock(p=NSforall).
Mitralvalvedisease
Mitral disease wasmore frequent in women than in men (58.9% vs. 41.1%, p=0.002), and was associated directly with rheumatic etiology (p=0.011), ischemic heart dis-ease (p<0.001), HF (p=0.001), AF (p<0.001), LV dilatation (p<0.001)andreducedLVEF(p=0.003).Nosignificant asso-ciation was found between mitral valve disease and LA dilatation.
Tricuspidvalveregurgitation
The presence of moderate-to-severe TR did not differ betweengenders(p=0.702),andcorrelateddirectlywithage (p<0.001)and withthe presence of previously implanted
cardiac devices (p<0.001). The latter association was observed only when TR coexisted with aortic or mitral disease (of any etiology). A significant association was alsofound betweenTRandmitraldisease(p<0.001), right chamberdilatation (p<0.001),AF(p<0.001)andpulmonary hypertension(p<0.001),butnotwithchronicpulmonary dis-ease.
Valveinterventionprocedures
Thirty-onepatients(10.8%)hadpreviouslyundergonevalve intervention(repairorreplacement),mostfrequentlySAVR (58.1%), followed by mitral valverepair (38.7%) and TAVI (12.9%).Nopatienthadbeenpreviouslysubmittedto per-cutaneousmitralvalveintervention.
During the index hospitalization, 118 patients (41.1%) underwent valve intervention. Percutaneous procedures werethe mostfrequently performed (74.6%), mainlyTAVI (65.3%); surgical replacement was performed in 12.7% of patients(aorticvalvein12patients, mitralvalveinfour), and surgical repair in 5.9% of cases (mitral valve in four patients and aortic valve in three). Percutaneous mitral valveinterventionswereperformedin11(9.3%)patients.
Regardingthe31patientswhohadpreviouslyundergone valve intervention, most were admitted with decompen-sated HF (48.4%), 16.1% were admitted electively for anothervalveprocedure,and6.5%presentedwithinfectious endocarditis.Furthermore,35.5%ofthispopulation under-went valve intervention again, 25.8% onthe same valve. In-hospitalmortalitywas12.9%inthishigh-riskpopulation. Of note, 4 patients underwent CABG during the index hospitalization,and2alsounderwentSAVR.
Dischargeandpost-dischargedata
Overall, mean LOS was 11.98±14.33 days. Most patients weredischargedhomefromhospital(84.3%)and5.2%were transferredtoanotherhospital(intheirareaofresidence) forcontinued care.Overall in-hospitalmortalitywas9.8% andcardiovascularmortalitywas8.7%.Mostdeaths(33.3%) occurredinthecontextofACS,followedbyadvanced refrac-toryHFandcardiogenicshock duetoVHD(29.6%),andto severerefractorypulmonaryhypertension(relatedtovalve diseaseand/orpulmonaryembolism)in7.4%.Othercauses ofdeathwere infectiousendocarditis of prostheticvalves (7.4%) or devices (3.7%), acute complications after pros-theticvalveimplantation(surgicalorpercutaneous)(7.4%), andpericardialeffusion(3.7%).
Discussion
Fromanoverallanalysisofthedataonthispopulation,the firstpointtohighlightisthatsignificantVHDhasnogender predominance,afindingconsistentwiththeresultsoflarge populationstudies.2---4Thesecondpointisthemedianageof
thepopulation,almost10yearsolderthanthoseincludedin theEuroHeartSurvey.4AccordingtoEurostat2015data,18
theproportionofpeopleaged65yearsormoreinPortugal was20.5%,comparedtotheoverallmedianpercentageof 19% in Europe,but thissmall differencedoes not appear
toaccountforthediscrepancy.Themostlikelyexplanation isthattheEuroHeartSurveyincluded bothinpatientsand outpatients, whereas the cohort presented here included only inpatients, a population with more advanced and severe disease, andprobablyalso an older onecompared toVHDpatientsinanoutpatientsetting.1,4Thisdifference
wouldalsoexplainthe56%ofpatientswithASfoundinour hospitalized population comparedto the 43% reported in theEuroHeartSurvey.4Ofnote,wefoundapredominance
of females in patients with rheumatic valve disease and consequently in patients with mitral disease (which was significantly associated with the latter), and rheumatic etiologymainlyaffectedyoungerpatients.
Although about 11% of included patients were born in Portuguese-speaking African countries, most of them had beenlivinginPortugalfordecades,anditwasthus impossi-bletocomparetheepidemiologyofvalvediseaseinAfrica andPortugal.IntheVALVAFRICstudy,aprospectivehospital registryofpatientswithrheumaticvalvediseaseinwestand centralsub-SaharanAfrica,40.2%presentedwithmoderate to severe disease, the median age of the population was 29.3±15.6years,andfemalegenderpredominated(60%).14
Decompensated HF wasthe main reason for admission in ourreflectingthelong-termevolution ofvalvedisease, theadvancedageofthepopulation,andtheseverityofthe clinicalconditionofpatientswithVHDneeding hospitaliza-tion.Additionally,AFandpulmonaryhypertensionrelatedto valvediseasewerebothfrequentconditionswithsignificant hemodynamicconsequences.Underlyingtheclinicalimpact ofVHD,asignificantproportionofpatientsalsopresented withechocardiographicevidenceofLVhypertrophyand/or dilatation, features linked to an unfavorable prognosis.19
Contrary to expectations, neither aortic nor mitral valve diseasewassignificantlyassociatedwithLAdilatation, high-lightingthemultiplicityofconditionsthatcancontributeto alterationsinatrialarchitectureandfunction.
Agingisassociatedwithdegenerativechangesthataffect not only the aortic annulus but also the conduction sys-tem,andcompleteAVblockwasanotherfrequentreasonfor hospitaladmission,particularlyinpatients with degenera-tiveAS,andwasacommonindicationforPMimplantation. AdvancedAVblockwasalsopresentinmanypatientswith MR,albeitlessfrequently,asitmayoccurasaconsequence ofCADandfibrosis.
The majority of patients withVHD had several cardio-vascular risk factors and multiple comorbidities, mostly significantCAD,anotherfrequentcauseforhospital admis-sion. In a recent retrospective study, Emren et al.20
assessedtheprevalenceofconcurrentCADin241patients (51% female) whounderwent surgery due to severe VHD. CADwasdetectedin57.7%ofpatientswithASandin41.9% ofthosewithMR.CADandsevereASfrequentlycoexist,20---22
althoughthesignificanceandseverityofCADinASmaybe particularlydifficulttoassess.ConcomitantCADhada clini-calnegativeimpactinourcohort,beingresponsiblefor33% ofall-causein-hospitalmortality,highlightingtheneedfor CADtobemanagedconcurrentlyduringhospitalizationfor VHD.
Coronary revascularization at the time of aortic valve replacement may be associated with improved long-term survival without affecting operative risk in some patient subsets.23 However,this is an open-ended issue and most
studieslookingattheoutcomesofCADandPCIinpatients undergoingTAVIrevealnobenefitinterms ofmortalityor majorcardiovascularevents.22---27
Asignificantproportionofpatients(35%)presentedwith TRassociatedwithother valvedisease,mostlymitral dis-ease,thusshowingasignificantassociationwithrheumatic disease and with secondary MR. Dilated cardiomyopathy wasparticularly observed, in agreementwiththe current literature.1 Besides, cardiac devicespreviously implanted
intherightheartwereassociatedwithdevelopmentofTR, aspreviouslydescribed,1withmostpatientsalsohavingMR.
Decisionfor interventioninmoderate-to-severesecondary TRis frequently amatter of debate, beingrecommended whenleft-sidedvalvesurgeryisindicated,orwhenrightHF ismanifest.8
In the index hospitalization 40% of patients under-went valve intervention, primarily TAVI, reflecting recent changes in the paradigm regarding valve disease mana-gement. Calcified AS is associated with a higher risk of myocardial infarction,strokeanddeath, independentlyof traditionalcardiovascularriskfactors,andsincethereisno effective medicalapproachand five-yearsurvival without interventionranges from15%to50%,9 percutaneousvalve
interventions areincreasingly important in the setting of theold,frailpatientwithmultiplecomorbidities,who fre-quentlyisnotconsideredsuitableforsurgery.6
Insummary,thefindingsinthecohortpresentedherein may be considered a real-world picture of current VHD in developed countries. Globally, VHD is most commonly degenerative, mainly affects the elderly with multiple comorbidities,issevereandhasalreadyrunalongcourse. Itis frequentlyassociatedwithCAD, HF,AF andadvanced conductiondisease,andhasanunfavorableimpacton prog-nosis. This includes quality of life (particularly symptoms andlongLOS)andin-hospitalmortality.Valveintervention isoftennecessary,andthepercutaneousapproachisa ther-apeuticoptioninmanyofthesehigh-riskpatients.
Limitations
Thedatapresentedarederivedfromasinglecenterandmay notreflectthecircumstances ofothercentersspecializing inthemanagementofpatientswithVHD.Furthermore,the informationwasnotacquired in the setting ofa prospec-tive registry, but consists of retrospective data collected fromclinicalfilesandechocardiographic reports,whichin somecasesmaynotbeasdetailedaswouldbedesirable. However,the data collectedreflect the actual profiles of patientshospitalizedwithVHDinthecardiologywardofa tertiaryhospital,andthethoroughmanualanalysisand mul-tiple revisions performed provide a precise and objective setofreal-worldinformation,similaringeneralrespectsto previousworkpublishedinthisfield.
Theinfluenceofthedifferentvariablesonmortalitywas notstudied,asthiswasbeyondthescopeofthisstudy.Our aimwastocharacterize the profiles ofpatients withVHD currently admitted toa tertiaryhospital in contemporary Europe,inwhichthenewtherapeuticoptionsforpatients withVHDareavailable,andwheretheEuropeanguidelines forthetreatmentofheartdiseaseareapplied.
Conclusion
On the basis of the data presented, two main profiles canbedelineatedfor patientscurrently hospitalizedwith VHD:adominantone,characterizedbytheelderlypatient, maleorfemale,withmultiplecomorbidities,admittedwith decompensatedHFinthesetting ofdegenerativeAS, pre-senting with LV hypertrophy and/or dilatation but with preservedLVEF,frequentlywithAF,whoispreferablytreated by TAVI; and a second, less prevalent profile, that of a youngerpatient,predominantlyfemale,alsoadmittedwith decompensatedHFbut in the setting of functional mitral regurgitation(secondarytoischemicheartdiseaseordilated cardiomyopathy),alsopresentingwithAFandLVdilatation butwithreducedLVEF,wholessoftenundergoesvalve inter-vention,butistreatedmedicallyforHF. Ofnote,common denominatorsofbothprofileswereHFandAF.
Author
contributions
AFE and DB conceived and designed the research, and draftedthefirstversionofthemanuscript;JR,IR,MMP,and FVcontributedtotheresearchanddataanalysis;AFEand RPperformedthestatisticalanalysis.Allauthorscritically reviewedthe manuscriptfor drafting andkey intellectual content,helpedrevisethepaperandgavefinalapprovalfor theversiontobepublished.
Conflicts
of
interests
Theauthorshavenoconflictsofinteresttodeclare.
Appendix
1.
ICD-9(InternationalClassificationofDiseases)diagnosis of valvediseasesused:
394.0 (rheumatic mitral stenosis), 394.1 (rheumatic mitralregurgitation),394.2(rheumaticmitralstenosiswith insufficiency),394.9(otherandunspecifiedmitralvalve dis-eases),395.0(rheumaticaorticstenosis),395.1(rheumatic aorticinsufficiency),395.2(rheumaticaorticstenosis with insufficiency),395.9(otherandunspecifiedrheumatic aor-ticdiseases), 396.0(mitralvalvestenosisandaortic valve stenosis), 396.1 (mitral valve stenosis and aortic valve insufficiency),396.2 (mitral valveinsufficiency and aortic valvestenosis),396.3(mitralvalveinsufficiencyandaortic valveinsufficiency),396.8 (multipleinvolvementof mitral andaorticvalves),396.9(mitralandaorticvalvediseases, unspecified), 397.0 (diseases of tricuspid valve), 397.1 (rheumaticdiseasesofpulmonaryvalve),397.9(rheumatic diseasesofendocardium,valveunspecified),424.0(mitral valvedisorders),424.1(aorticvalvedisorders),424.2 (tri-cuspid valve disorders, specified as nonrheumatic), 424.3 (pulmonary valve disorders) and/or 424.9 (endocarditis, valveunspecified).
References
1.CoffeyS,CairnsBJ,IungB.Themodernepidemiologyofheart valvedisease.Heart.2016;102:75---85.
2.Iung B, VahanianA. Epidemiology ofacquiredvalvular heart disease.CanJCardiol.2014;30:962---70.
3.NkomoVT,GardinJ,SkeltonT,etal.Burdenofvalvularheart diseases:apopulation-basedstudy.Lancet.2006;368:1005---11. 4.Iung B,BaronG,ButchartEG,etal. Aprospectivesurveyof patientswithvalvularheartdiseaseinEurope:TheEuroHeart SurveyonValvularHeartDisease.EurHeartJ.2003;24:1231---43. 5.RezzougN,VaesB,MeesterC,etal.Theclinicalimpactof valvu-larheartdiseaseinapopulation-basedcohortofsubjectsaged 80andolder.BMCCardiovascDisord.2016;16:7.
6.ThadenJJ,NkomoVT,Enriquez-SaranoM.TheGlobalBurdenof AorticStenosis.ProgCardiovascDis.2014;56:565---71. 7.OsnabruggeRLJ,MylotteD,HeadSJ,etal.Aorticstenosisin
theelderly---diseaseprevalenceandnumberofcandidatesfor transcatheter aortic valvereplacement: a meta-analysis and modelingstudy.JAmCollCardiol.2013;62:1002---12.
8.Baumgartner H, Falk V,Bax JJ, et al., ESC Scientific Docu-mentGroup.2017ESC/EACTSGuidelinesforthemanagement ofvalvularheartdisease.EurHeartJ.2017;36:2739---91. 9.Vahanian A, Alfieri O, AndreottiF, et al.,Guidelines onthe
managementofvalvularheartdisease(version2012),TheJoint Task Forceon theManagement of ValvularHeart Diseaseof the European Society ofCardiology (ESC) and the European AssociationforCardio-ThoracicSurgery(EACTS).EurHeartJ. 2012;33:2451---96.
10.DucasRA,WhiteCW,WassefAW,etal.Functionalmitral regur-gitation:currentunderstandingandapproachtomanagement. CanJCardiol.2014;30:173---80.
11.AsgarAW,MackMJ,StoneGW.Secondarymitralregurgitation in heartfailure:pathophysiology, prognosis, and therapeutic considerations.JAmCollCardiol.2015;65:1231---48.
12.Schillinger W, Senges J. TRAMI (Transcatheter Mitral Valve Interventions)-Register.Herz.2013;38:453---9.
13.SeckelerMD,HokeTR.Theworldwideepidemiology ofacute rheumaticfeverandrheumaticheartdisease.ClinEpidemiol. 2011;3:67---84.
14.KinguéS,BaSA,BaldeD,etal.,TheVALVAFRICstudy:aregistry ofrheumaticheartdiseaseinWesternandCentralAfrica.Arch CardiovascDis.2016;109:321---9.
15.LancellottiP,TribouilloyC,HagendorffA,etal. Recommenda-tionsfortheechocardiographicassessmentofnativevalvular regurgitation:anexecutivesummaryfromtheEuropean Asso-ciation of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging.2013;14:611---44.
16.BaumgartnerH,HungJ,Bermejo J,etal.Echocardiographic assessment of valve stenosis:EAE/ASE recommendations for clinicalpractice.EurJEchocardiogr.2009;10:1---25.
17.PonikowskiP,VoorsAA,AnkerSD,etal.ESCGuidelinesforthe diagnosis and treatment ofacute and chronic heartfailure: TheTaskForceforthediagnosisandtreatmentofacuteand chronicheartfailureoftheEuropeanSocietyofCardiology(ESC) Developedwiththespecial contributionoftheHeartFailure Association(HFA)oftheESC.EurHeartJ.2016;37:2129---200. 18.http://www.pordata.pt/Europa/Popula%C3%A7%C3%A3o+
residente+total+e+por+grandes+grupos+et%C3%A1rios+ (percentagem)-1865-202233[accessed25.07.17].
19.Minamino-Muta E, Kato T, Morimoto T, et al. Impact of the left ventricular mass index on the outcomes of severe aortic stenosis. Heart. 2017, http://dx.doi.org/10.1136/ heartjnl-2016-311022.
20.EmrenZY,EmrenSV,Kılıc¸aslanB,etal.Evaluationofthe preva-lenceofcoronaryarterydiseaseinpatientswithvalvularheart disease.JCardiothoracSurg.2014;9:153.
21.KvidalP, Bergstrom R, Horte LG,et al. Observed and rela-tivesurvivalafteraorticvalvereplacement.JAmCollCardiol. 2000;35:747---56.
22.D’AscenzoF,ConrottoF,GiordanaF,etal.Mid-term prognos-tic value of coronary artery disease in patients undergoing transcatheter aortic valve implantation: a meta-analysis of adjusted observational results. Int J Cardiol. 2013;168: 2528---32.
23.ThaljiNM,Suri RM,DalyRC, etal.Theprognosticimpactof concomitantcoronaryarterybypassgraftingduringaorticvalve surgery:implicationsforrevascularizationinthetranscatheter era.JThoracCardiovascSurg.2015;149:451---60.
24.Abdel-WahabM,MostafaAE,GeistV,etal.Comparisonof out-comesin patientshaving isolated transcatheter aortic valve implantationversuscombinedwithpreproceduralpercutaneous coronaryintervention.AmJCardiol.2012;109:581---6. 25.Gasparetto V, Fraccaro C, Tarantini G, et al. Safety and
effectivenessofaselectivestrategyforcoronaryartery revas-cularization before transcatheter aortic valve implantation. CatheterCardiovascInterv.2013;81:376---83.
26.Ussia GP,Barbanti M, ColomboA, et al. Impactof coronary artery disease in elderly patients undergoing transcatheter aortic valveimplantation: insight from theItalian CoreValve Registry.IntJCardiol.2013;167:943---50.
27.ParadisJ,WhiteJM,GenereuxP,etal.Impactofcoronaryartery diseaseseverityassessedwiththeSYNTAXScoreonoutcomes followingtranscatheteraorticvalvereplacement.JAmHeart Assoc.2017;6:e005070.