www.jped.com.br
ORIGINAL
ARTICLE
Impact
of
chronic
kidney
disease
on
quality
of
life,
lung
function,
and
functional
capacity
夽
,
夽夽
Carolina
Guimarães
Teixeira,
Maria
do
Carmo
M.B.
Duarte,
Cecília
Maciel
Prado,
Emídio
Cavalcanti
de
Albuquerque,
Lívia
B.
Andrade
∗InstitutodeMedicinaIntegralProf.FernandoFigueira(IMIP),Recife,PE,Brazil
Received3December2013;accepted28February2014 Availableonline17June2014
KEYWORDS
Renalinsufficiency, chronic;
Child;
Pulmonaryfunction test;
Qualityoflife
Abstract
Objectives: Toevaluatetheimpactofthechronickidneydisease(CKD)onqualityoflife,from thechildren’sandtheirparents’perspective,respiratorymusclestrength,lungfunction,and functionalcapacityinchildrenandadolescents.
Method: Cross-sectional study ofchildren withCKDaged 8to17 years.Thoseincapableof takingthetestswereexcluded.Afteraninterview,qualityoflifebyPediatricQualityofLife Inventory)(PedsQLTM),muscularstrength,pulmonaryfunctiontests,andthe6-minute
walk-ingtest(6MWT)wereapplied.Student’st-test,ANOVA(differenceinmeans),andPearson’s coefficientofcorrelationwereused.Thelevelofsignificancewassetat5%.
Results: Ofthe40patients,themeandistancewalkedatthe6MWTwas396meters,andthe meanfinalscoreatthequalityoflifetestasperceivedbythechildrenandparentswas50.9 and51,respectively.Fromthechildren’sperspective,thetransplantedpatientshadahigher qualityoflifescorewhencomparedtothoseundergoinghemodialysis(p<0.001);thosewho practicedphysicalactivityhadbetterqualityoflifewhencomparedtothesedentarychildren (p<0.001).Fromthechildren’sandtheparents’perspectives,themalegenderhadahigher qualityoflifescore(p<0.05).Therewasapositivecorrelationbetweenthedistancewalkedat the6MWTandage,height,finalPedsQLTM,forcedvitalcapacity(FVC),andforcedexpiratory
volumeinthefirstsecond(FEV1),aswellasanegativecorrelationbetweenFEV1/FVCandthe
distancewalked.
Conclusion: A significant reduction in the quality of life and the functional capacity was observedinchildren withCKD, influencedby thetypeoftreatment,gender,andsedentary lifestyle.
©2014SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:TeixeiraCG,DuarteMC,PradoCM,AlbuquerqueEC,AndradeLB.Impactofchronickidneydiseaseonquality oflife,lungfunction,andfunctionalcapacity.JPediatr(RioJ).2014;90:580---6.
夽夽
StudyperformedatInstitutodeMedicinaIntegralProf.FernandoFigueira(IMIP),Recife,PE,Brazil. ∗Correspondingauthor.
E-mail:[email protected],[email protected],[email protected](L.B.Andrade). http://dx.doi.org/10.1016/j.jped.2014.03.002
PALAVRAS-CHAVE
Insuficiênciarenal crônica;
Crianc¸a;
Func¸ãopulmonar; Qualidadedevida
Repercussãodadoenc¸arenalcrônicanaqualidadedevida,func¸ãopulmonare
capacidadefuncional
Resumo
Objetivos: Avaliarrepercussõesdadoenc¸a renalcrônica(DRC)sobreaqualidadedevidana percepc¸ãodascrianc¸asedospais,forc¸amuscularrespiratória,func¸ãopulmonarecapacidade funcionalemcrianc¸aseadolescentes.
Método: Estudotransversaldecrianc¸aseadolescentescomDRCdeoitoa17anos.Excluídas asincapazes derealizarostestes.Apósentrevista, aplicou-sequestionáriodequalidadede vida(PedsQLTM),testesdeforc¸amuscular,func¸ãopulmonaretestedecaminhadade6minutos
(TC6min).FoiutilizadootestetdeStudenteANOVA(diferenc¸asdemédias)eocoeficientede correlac¸ãodePearson.Considerou-seníveldesignificânciade5%.
Resultados: Dentreos40pacientes,amédiadadistânciapercorridanoTC6minfoide396±71 metros,eamédiadoescorefinaldequalidadedevidapercebidapelascrianc¸asepelospaisde 50,9e51,respectivamente.Napercepc¸ãodascrianc¸as,ostransplantadosapresentarammaior escoredequalidadedevida,comparadosaosemhemodiálise(p<0,001),eaoscomatividade física emelhorqualidadedevida,comparadas àssedentárias(p<0,001).Napercepc¸ãodas crianc¸asedospais,osexomasculinoapresentoumaiorescoredequalidadedevida(p<0,05). Houvecorrelac¸ãopositivaentreadistânciapercorridanoTC6mineasvariáveisidade,altura, PedsQLTM finalda crianc¸a, capacidade vital forc¸ada (CVF)e volume expiratório forc¸ado no
primeirosegundo(VEF1)enegativaentreVEF1/CVFeadistânciapercorrida.
Conclusão: Observou-sereduc¸ãosignificativanaqualidadedevidaenacapacidadefuncional emcrianc¸ascomDRCinfluenciadaspelotipodetratamento,sexoesedentarismo.
©2014SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Chronicrenalfailure(CRF)ischaracterizedbyslowly pro-gressive,irreversibleloss ofkidney function.1 Inchildren,
chronic kidneydisease(CKD) isassociatedwithsignificant cardiovascular morbidity and mortality, hospitalizations, andcommonspecificproblems,suchasimpairedgrowthand biopsychosocialchangesthathave animpactonqualityof life(QoL).2
Data from the Brazilian Society of Nephrology in 2012 showedthat0.3%ofchildrenwithCKDaged1to12yearsand 4.2%between13and18yearsundergodialysis.1Inrecent
years,thenumberofpatientsondialysishasdoubled,with anincreaseof8%peryear,increasingfrom18,000patients in2001to91,314in2011,resultinginsignificanthealthcare costs.3
Studies have shown thatchildren andadolescentswith CKD may have alterations in QoL, muscle strength, lung function,andfunctionalcapacity.4,5
Theassessmentofhealth-relatedQoLisanimportant cri-terionwhenevaluatingtheeffectivenessoftreatmentsand interventionsinhealthcare,makingitimportantto under-standtheexistingassociationbetweenthediseaseandQoL.6
Goldsteinetal.,7in2008,developedthePedsQLTM
question-nairetospecificallyassessQoLinchildrenandadolescents withCKD.Thisquestionnaireassessessevendomains (gen-eral fatigue, kidney disease, treatment, interaction with familyandfriends,worry,physicalappearance,and commu-nication), and is applied to patients with CKD and their parents or guardians.Studies on QoL using the PedsQLTM
have verified the impact of CKD on QoL of children and adolescents.7,8
The PedsQLTMversion 3.0wastranslatedandculturally
adaptedintoBrazilianPortuguesein2011,9butthereareno
publishedstudiesonitsvalidationinBrazil.
The reduction in functional capacity and performance ofphysicalandrecreationalactivitiescanbeinfluencedby physicaldeconditioning,muscle disuseatrophy,weakness, fatigue,lower-limb edema, andbackpain,amongothers, hinderingtheperformanceofdailylivingactivitiesbythese children.10,11Otherfactorsmayimpairthemuscularsystem
ofCKD patients, suchas decreased protein-calorieintake andproteinimbalance.The respiratorymusclesmayshow decreasedstrengthandendurancepropertiesduetouremic myopathy.12---14
Respiratory muscle strength measurement aids in the early identification of muscle weakness, as well as iden-tification of the severity, functional consequences, and evolutionofpulmonaryandneuromusculardisorders.15,16A
studyhasdemonstratedthatchildrenandadolescentswith CKDhavesignificantlylowermuscularstrengthvalues,when comparedtohealthysubjects.4
Walking tests aresubmaximal testsused inthe assess-ment of functional capacity of children with physical exertion limitations. They are easy to perform, repro-ducible, low-cost, and show good correlation with the maximum oxygenconsumption obtained at maximal exer-cisetests.17---19Astudyhasdemonstratedthatchildrenwith
ThepresentstudyaimedtoevaluatetheimpactofCKDon QoLfromthechildren’sandtheirparents’perception, respi-ratorymusclestrength,pulmonaryfunction,andfunctional capacityinchildrenandadolescents.
Methods
Thiswasanobservationalcross-sectionalstudywithchildren andadolescentswithCKD,treatedatthePediatric Nephrol-ogyUnitoftheInstitutodeMedicinaIntegralProf.Fernando Figueira(IMIP),inPernambuco,whichisareferencecenter forkidneydiseaseandtransplantationinNortheastBrazil.
The study was approved by the Ethics Committee on HumanResearchof IMIP(No.3334-13), andthose respon-siblefor thechildrenand adolescentssigned ANinformed consentbeforethestudywasinitiated.
Childrenand adolescents,aged8to17 yearsand with CKD,andoneoftheirparentswereincluded.Children inca-pableofperformingthesix-minutewalktest(6MWT),those withdifficultiesinunderstandingdirectionstoperformthe maneuvers,andpatientswithcomplexcongenitalheart dis-ease and severe pulmonary disease were excluded. Data collectionwasperformedfromDecember2012toApril2013. Initially,demographic,anthropometric,andclinicaldata wererecordedonstandardizedinvestigationforms contain-ingthevariablesofinterestforthestudy.Educationaldelay was defined as regular age-grade correspondence > two years, according to the criteria adopted by the Brazilian MinistryofEducation;familyincomewascalculatedbythe sumofindividualincomesofthehousehold’sresidents.The levelofphysicalactivitywasassessedthroughtheHabitual LevelofPhysicalActivity(HLPA)questionnaireassedentary lifestyle,regularphysicalactivity(upto2hoursaweek),and competitive/organizedsports physical activity (morethan 2hoursaweek).20 The typeoftreatment wascategorized
asconservative,peritonealdialysis,hemodialysis,andrenal transplantation.
Subsequently, the PedsQLTM QoL questionnaire was
applied,after authorizationof use by the MAPI Research Trust,responsiblefor thepermissionstousethe question-naire, followed by lung function and respiratory muscle strength assessment and the 6MWT. The tests were con-ductedbythemainresearcherandanappropriatelytrained physicaltherapystudent.
Qualityoflife
QoL assessment was performed by applying the PedsQLTM
questionnaire (version 3.0).9 It consists of 34 questions
grouped into seven items comprising health-related per-ception in the areas of general fatigue, kidney disease, treatment, interaction with family and friends, worry, physicalappearance,andcommunication,asperceivedby parentsandthechildren/adolescents.Valuesrangefrom0 to4,with0representing ‘‘itis nevera problem;’’1,‘‘it is almost never a problem;’’2, ‘‘it is sometimes a prob-lem;’’3,‘‘itisoftenaproblem;’’and4,‘‘itisalmostalways aproblem.’’The questions areconvertedintoscores, for which values areproportionally assigned, the sum ranges from0to100points.Thehigherthevalueofthefinalscore, thebettertheQoLofpatients.
Strengthandlungfunction
Maximal respiratory pressures were measured through manovacuometry,usingan analog manovacuometer (Com-ercialMédica®,SãoPaulo,Brazil).Thetestwasperformed withthechildsittingcomfortablytomeasurethemaximal inspiratorypressure(MIP)throughaninspiratorymaneuver basedonthefunctionalresidualcapacity,whereasmaximal expiratorypressure(MEP)wasevaluatedbasedontotallung capacityforaforcedexpiration,afterclippingthenose.For both measures,threemaneuvers wereperformed andthe bestofthethreewaschosenusingthetechniquebasedon Wilson’sstudy.21
Lung function assessment was performed by spirome-try using a digital spirometer OneFlow® model (Clement ClarkeInternational;Harlow,UK)andtechnicalprocedures, criteriafor acceptability,andreproducibilityfollowed the guidelinesoftheAmericanThoracicSociety andEuropean RespiratorySociety(ATS/ERS).22Theforcedexpiratory
vol-umeinonesecond(FEV1),forcedvitalcapacity(FVC),peak
expiratoryflow(PEF),andFEV1/FVCratioweredetermined.
The maneuverwasperformed threetimes andthehighest valuewasused.
6-MinuteWalkingTest
Submaximal functional capacity was evaluated using the 6MWTaccordingtotheATSstandardization,22 onaflat,
30-meter corridor. The children/adolescentswere instructed to walk as far as possible in six minutes without run-ning, and the test couldbe interrupted at any time.The children/adolescentswereverballyencouraged, minute-by-minute,accordingtotheteststandardization,andaftersix minutestheywereaskedtostopwheretheywereinorderto recordthedistancewalkedinmeters.Theparameters eval-uatedpre-andpost-testincludedheartrate(HR)andpulse oxygen saturation (SpO2) by pulse oximetry model
OXP-10 (EMAI Equipamentos Médicos Hospitalares, São Paulo, Brazil),systemicbloodpressurethrougha sphygmomanome-ter model CE0050 (Tycos/WelchAllyn, Skaneateles Falls, USA),respiratoryrate(RR)(countedbychestwallincursions perminute),andthemodifiedBorgscalescoretomeasure dyspnea.23
Thecriteriafor testinterruptionwere: severedyspnea or fatigueexpressedbythepatient,SpO2<85%,orrefusal
tocontinue theexamination. Based onthereference val-uessuggestedbyPriesnitzetal.24forhealthychildren,the
predictedwalkeddistanceatthe6MWTforthechildrenwas calculatedusingtheformula6MWT=145.343+[11.78xage (years)]+[292.22xheight(m)]+[0.611x(HRFinal-HRInitial)]
-[2,684xweight(kg)]toevaluatetestperformance.This referencewasused becauseitis froma study onhealthy Brazilianchildren.Basedonthesevalues,thedifferenceof meansbetween thedistancewalkedbythepatientat the 6MWT(WD)andthepredicteddistance(PD)wasobtained.
morethantwogroups.Student’s t-test wasusedfor com-parisonof paired means. Pearson’s correlation coefficient wasusedtoassesscorrelation.DatawereanalyzedinSPSS 13.0forWindows(IBMCorp,Armonk,USA)andExcel2007 (Microsoft,MicrosoftExcel,Washington,USA).Asignificance levelof5%wasusedinalltests.
Results
Ofthetotal127childrenandadolescentswithCKDtreated atthePediatricNephrologyUnitofIMIP,40wereincludedin thestudyand87wereexcluded(31duetoincapacityto per-formthe6MWT,46duetodifficultiesinunderstandinghow toperformthe respiratorytests,and tenfor having com-plexheartdisease orsevere chroniclung disease).Of the 40eligiblepatients,themeanage±SDwas13±2.6years, 52.5%weremales,59.5%hadeducationaldelay,and85%did notpracticeanyphysicalactivity.ThemeanfinalQoLscore was50.9±16.5forthechildrenand51±16.5forthe par-ents.Themeanwalkeddistanceinmetersatthe6MWTwas 396±71,whereasthemeanwalkeddistancepredictedby theformulawas620.2±44meters,withasignificant differ-ence(p<0.001),representing63.7%ofthepredictedvalues (Table1).
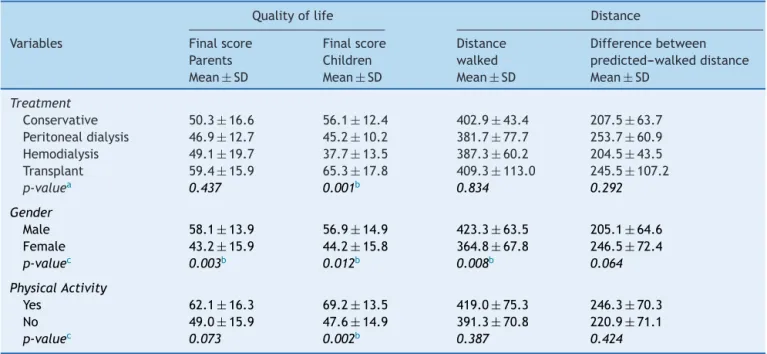
When comparing QoL and the type of treatment, it was observed that transplanted patients had the high-est scores (65.3) when compared to the group submitted to hemodialysis (37.7; p<0.001) from the children’s per-ception. Additionally, there was a significant association betweenQoLandgender fromtheparents’andchildren’s perception,wheremaleshadabetterfinalQoLscore(58.1 and56.9,respectively).RegardingQoLandphysicalactivity, it was observed that those whoperformed regular physi-calactivityhadabetterQoLwhencomparedtosedentary individuals(p=0.002)fromthechildren’sperception.
Comparingthemeansbetweenthewalkeddistanceand the gender of the child, it was observed that the dis-tancewalkedbymaleswashigherthanfemales(p=0.008) (Table2).
When analyzing the correlation between the distance walkedin the6MWTandthe studyvariables, therewasa significant positivecorrelation, i.e.,thehigher thevalues ofthevariables,thebetterthetestperformanceregarding variablesage,height,finalPedsQLTM,FVC,predicted FVC,
FEV1,andpredictedFEV1.Anegativecorrelationbetween
FEV1/FVCandthewalkeddistancewasalsoobserved,that
is,thehighertheratio,thelowerthetestperformance.The respiratoryrateevaluatedafterthe6MWTshowedapositive correlationwiththedifferencebetweenthewalkedandthe expecteddistance (Table 3).Theother variablesanalyzed inthisstudyshowednosignificantcorrelation.
Discussion
The present studydemonstratesthatchildren and adoles-cents with CKD have a significant reduction in QoL and functionalcapacity.ThisstudyusedthePedsQLTMQoL
ques-tionnaire version 3.0, as it is specific for children and adolescents with CKD, and is probably more sensitive to detectpossiblealterationsinthehealthofthesepatients. Inaddition,theauthorsdidnotfindstudiesintheliterature
Table1 Characteristicsof40childrenwithchronickidney diseasetreatedatareferralcenterforpediatricnephrology, 2013,Brazil.
Variables
Ageyears(mean±SD) 13±2.6
Weightkg(mean±SD) 40±16.3
Heightmeters (mean±SD)
1.5±0.2
BMI(mean±SD) 18.3±4.6
Educationaldelay(n,%) 22(59.5%)
Maternalschooling≤8 years(n,%)
27(67.5%)
Familyincome(n,%)
≤1MW 8(20.0%)
1to2MW 12(30.0%)
≥2MW 20(50.0%)
Physicalactivity(n,%)
Regularactivity 6(15.0%)
Sedentary 34(85.0%)
Treatment(n,%)
Conservative 13(32.5%)
Peritonealdialysis 9(22.5%)
Hemodialysis 10(25.0%)
Transplant 8(20.0%)
FinalPedsQLTMofchild
(mean±SD)
50.9±16.5
FinalPedsQLTMof
parents(mean±SD)
51±16.5
Respiratorymuscularstrength(mean±SD)
MIP 60.75±37.63
MEP 62.63±35.61
Pulmonaryfunction(mean±SD)
PredictedFVCvalue 2.56±0.79 PredictedFEV1value 2.28±0.68
FEV1/FVC 0.89±0.13
Distancewalkedin meters(mean±SD)
396±71.2a
Predicteddistance (mean±SD)
620.2±44.63a
Values expressed as mean and standard deviation (SD) and numbers (n)and percentage (%). BMI, bodymassindex; MW, minimumwage;MIP,maximalinspiratorypressure;MEP, maxi-malexpiratorypressure;FVC,forcedvitalcapacity;FEV1,forced
expiratoryvolumeinonesecond;PedsQLTM,qualityoflife ques-tionnaire.
a p<0.001.
associatedtobetterQoLasperceivedbyparentsofchildren andadolescentswithCKDthathadusedthePedsQLTM.
Inthisstudy,themeanfinalQoLscoreperceivedbythe children was50.9, a significantlylower resultwhen com-paredtothoserecorded by Goldestein etal.,7 in a study
performedintheUnitedStates(72.5),andbyParketal.,8
inKorea(69.4).Thelowerscoreinthepresentstudymaybe duetothefactthattheevaluatedchildrenhadlow socioe-conomicstatus.
Table2 Comparison ofmeans ofquality oflife,walked distance, anddifference between thepredicted andthe walked distance,subdividedbytypeoftreatment,gender,andphysicalactivityinchildrenandadolescentswithchronickidneydisease.
Qualityoflife Distance
Variables Finalscore
Parents
Finalscore Children
Distance walked
Differencebetween predicted---walkeddistance
Mean±SD Mean±SD Mean±SD Mean±SD
Treatment
Conservative 50.3±16.6 56.1±12.4 402.9±43.4 207.5±63.7 Peritonealdialysis 46.9±12.7 45.2±10.2 381.7±77.7 253.7±60.9 Hemodialysis 49.1±19.7 37.7±13.5 387.3±60.2 204.5±43.5 Transplant 59.4±15.9 65.3±17.8 409.3±113.0 245.5±107.2
p-valuea 0.437 0.001b 0.834 0.292
Gender
Male 58.1±13.9 56.9±14.9 423.3±63.5 205.1±64.6
Female 43.2±15.9 44.2±15.8 364.8±67.8 246.5±72.4
p-valuec 0.003b 0.012b 0.008b 0.064
PhysicalActivity
Yes 62.1±16.3 69.2±13.5 419.0±75.3 246.3±70.3
No 49.0±15.9 47.6±14.9 391.3±70.8 220.9±71.1
p-valuec 0.073 0.002b 0.387 0.424
Valuesexpressedasmeanandstandarddeviation(SD).
aANOVA. b p<0.05. c Student’st-test.
reportedin a study conducted in Korea involving 92 chil-dren withCKD.8 Another studyin Texaswith186 children
andadolescentswithCKDdemonstratedthat,inadditionto betterQoL,childrensubmittedtorenaltransplantationhad improvedsurvival.Thisfactisjustifiedbytheauthorsforthe highriskofcomplicationsinpatientsundergoingperitoneal dialysisandhemodialysis.5
HigherscoringinthefinalQoLscoreasperceivedbymale children and adolescents was also demonstrated for the
Table3 Correlationbetweenthewalkeddistance, differ-encebetweenthepredictedandthewalkeddistance,and studyvariablesinchildrenwithchronickidneydisease.
Variables Distances
Distance walked
Differencebetween predictedandwalked distance
Age 0.339a 0.162
Height 0.356a 0.111
FinalPedsQLTM 0.340a −0.061
FVC 0.350a 0.092
PredictedFVC 0.375a 0.048
FEV1 0.395a 0.074
PredictedFEV1 0.368a 0.063
FEV1/FVC −0.315a 0.226
RRafter6MWT −0.243 0.3271
PedsQLTM, quality of life questionnaire; FVC, forced vital
capacity; FEV1, forcedexpiratoryvolume inone second; RR,
respiratoryrate.
aSignificantcorrelation(Pearson’scorrelation)p<0.05.
perceptionofadolescentsaged15to18yearswithCKDina studybyMaxwelletal.25
Better scoring in the final QoL score according to the perceptionofchildrenthatpracticedphysicalactivitywas alsoobservedbyotherauthors.Akberetal.26evaluatedthe
levelofphysicalactivitythroughtheuseofpedometersin patients aged 7 to 20 years with CKD and observed that lowlevelsofphysicalactivityinthisagegroupwere associ-atedwithhighercardiovascularrisks.Theresearchersalso statedthatlow levelsofphysicalactivity wereassociated withpoorerphysicalperformanceandworseself-reported QoL.26
Patients with CKD may have muscle dysfunction due to interrelatedfactors, such asdecreased protein-calorie intake,muscledisuseatrophy,andproteinimbalance.These factorsleadtochangesintypeIImusclefibersand reduc-tionofthecapillaryvascularbed,intravascularpresenceof calcification, and reductionof local blood flow,thus con-tributingtomusclealterations.27
Discordantdata tothose ofthe present study refer to musclestrength.ThestudybyCoelhoetal.4inMinasGerais,
involving30childrenwithCKD,foundlowervaluesin maxi-malexpiratorypressure.
Whenassessing pulmonary function,a positive correla-tion wasobserved between FVCand FEV1 with functional
capacity. Childrenwithbetter vitalcapacity andFEV val-uesshowedbetterperformanceatthe6MWT,suggestingthe influenceofthesevariablesonthetest.InchildrenwithCKD, adecreaseinspirometricvariablesisrelatedtoreversible airwayobstructionandairtrappingcausedbyaccumulation offluidnearthesmallairways.28AstudyconductedinFrance
withdecreasedmusclestrength,responsiblefor thedelay inskeletalmusclefibercontraction.29
The positive correlationfound between thefinal respi-ratory rate and the difference between the walked and predicted distances indicates worse performance at the test.Thisisconsistentwithastudyof30childrenand adoles-centswithCKD,whereanassociationwasobservedbetween shorterwalkeddistanceandanincreaseinthefinal respira-toryrate,bloodpressure,pulseoxygensaturation,andBorg perceivedexertion,thussuggestingaworseperformancein functionalactivities.4
Functional capacity assessed by the mean walked dis-tanceatthe6MWTfound inthepresent study(396±71.2 meters) was lower than that observed in other stud-ies, whose mean walked distances ranged from 515 to 560 meters. However, in all these studies, the values were significantly lower than those predicted.4,18,26
Sev-eral anthropometric, clinical, and biological factors can influence children with CKD to have poorer performance in physical activities, such as maternal education, body mass index(BMI), height, andage. A study demonstrated thatchildrenofmotherswithhighereducationallevelwere more activewhen compared tochildren of less educated mothers.30
Regarding the correlations between walked distance and variables of interest in the study, it was observed that the older the children and adolescents were, the better their performance at the 6MWT, indicating better functional capacity. Another study also found a positive correlationbetweenageandwalkeddistance, demonstrat-ing that the older the age, the better the functional capacity.26
Regarding the correlation between functional capacity assessedbythe6MWT,itcanbeobservedthattallerpatients walkedasignificantlygreaterdistancewhencomparedwith healthychildren. ABelgian study of25 children withCKD observedthatheightisanimportantfactorforthedistance walkedduringthe6MWT,explainedbythefactthattaller individuals have greater stride length and better perfor-manceatthetest.18
Regardinggender,maleindividualsshowedbetter perfor-manceatthe6MWT.Thepresent dataareconsistentwith a study conducted in China, which found higher exercise capacityand better performance at the 6MWT in healthy malechildren, probablyas a resultof their greater mus-cle mass.17 Conversely, a U.S. study with 44 participants
assessedphysicalactivityinCKDpatientsaged7to20years, andobservedthatfemaleswalkedagreaterdistance than malesinthe6MWT.26
The positive correlation between distance walked and QoL perceived by the children demonstrated that the greater the distance walked, the better the score; how-ever,theauthorsdidnotfindotherstudiesrelatedtothese findingsintheliterature.
Despite the importance of this study,some limitations needtobehighlighted,suchasthesamplesize,whichmay nothavehadsufficientpowertodemonstrateallthestudied differences,suchasrespiratorymusclestrength.However, alleligiblechildrenwithCKDfromtheNephrologyPediatric CenterofIMIPwereincluded.Itisnoteworthy,however,that thisstudyistheinBraziltoevaluateQoLthroughPedsQLTM
inchildrenandadolescentswithCKD.
Finally,itis concludedthatthestudy sampleshoweda significantreductioninQoL,functionalcapacity,and phys-icalactivityinchildrenandadolescentswithCKD.Positive associationswerealsofoundbetween functionalcapacity, pulmonaryfunction,andQoL.However,nocorrelationwas foundbetweenrespiratory musclestrengthandfunctional capacity,suggestingtheneedfornewstudiestobetter elu-cidatethisfinding.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Sociedade Brasileira de Nefrologia. Censo brasileiro de nefrologia. 2012. [cited 01 Aug 2013]. Available from: http://www.sbn.org.br/pdf/publico2012.pdf
2.HarambatJ,KarlijnJ,VanStralen,KimJJ,TizardEJ. Epidemi-ology ofchronickidneydisease inchildren.Pediatr Nephrol. 2012;27:363---73.
3.Junior RE. Doenc¸a renal crônica: definic¸ão, epidemiologia e classificac¸ão.JBrasNefrol.2004;26:1---9.
4.CoelhoCC,AquinoES,LaraKL,PeresTM,BarjaPR,LimaEM. Repercussõesdainsuficiência renalcrônicanacapacidadede exercício,estadonutricional,func¸ãopulmonaremusculatura respiratória decrianc¸aseadolescentes.RevBrasdeFisioter. 2008;12:1---6.
5.Goldstein SL, Rosburg NM, Warady BA, Seikaly M, McDonald R,LimbersC,etal.Pediatricendstagerenaldisease health-related quality of life differs by modality: a PedsQL ESRD analysis.PediatrNephrol.2009;24:1553---60.
6.FeberJ,DupuisJM,ChapuisF,BraillonP,Jocteur-MonrozierD, DaudetG,etal.Bodycompositionandphysicalperformancein childrenafterrenaltransplantation.Nephron.1997;75:13---9. 7.Goldstein SL, GrahamN, Warady BA, SeikalM, McDonald R,
BurwinkleTM,et al.Measuring health-related qualityoflife inchildrenwithESRD:performanceofthegenericand ESRD-specific instrumentofthePediatricQuality ofLife Inventory (PedsQL).AJKD.2008:285---97.
8.Park KS,HwangYJ, ChoMH,Ko CW,HaIS, KangHG, et al. Qualityoflifeinchildrenwithend-stagerenaldiseasebasedon aPedsQLESRDmodule.PediatrNephrol.2012;27:2293---300. 9.KochVHK,LopesM,VarnijamesW.Traduc¸ãoeadaptac¸ão
cultu-raldoPedsQLTMESRDparaalínguaportuguesa.JBrasNefrol. 2011;33:448---56.
10.LimaFF,Miranda RCV,RossieSilvaRC,MonteiroHL,YenLS, FahurBS,etal.Avaliac¸ãofuncionalpréepós-programade exer-cíciofísico depacientesem hemodiálise.Transinf[Internet]. 2013;46:24-35.
11.Schardong TJ, Lukrafka JL, Garcia VD. Avaliac¸ão da func¸ão pulmonareda qualidadede vida em pacientes com doenc¸a renal crônica submetidos à hemodiálise. J Bras Nefrol. 2008;30/1:40---7.
12.Cury JL, Brunetto AF,Aydos RD. Efeitosnegativos da insufi-ciênciarenalcrônicasobreafunc¸ãopulmonareacapacidade funcional.RevBrasFisioter.2010;14:91---8.
13.Nascimento LC,Coutinho ÉB,Silva KN. Efetividadedo exer-cício físico na insuficiência renal crônica. Fisioter Mov. 2012;25:231---9.
14.JohansenKL.Exerciseandchronickidneydisease:current rec-ommendations.SportsMed.2005;35:485---99.
respiratória:terapiaintensiva ereabilitac¸ão.RiodeJaneiro: GuanabaraKoogan;2008.p.111---24.
16.Fiore Junior JF, Paisani DM, Franceschini J, Chiavegato LD, FaresinSM.Pressõesrespiratóriasmáximasecapacidadevital: comparac¸ãoentre avaliac¸õesatravés debocal edemáscara facial.JBrasPneumo.2004;30:515---20.
17.LiAM,YinJ,YuCC,TsangT,SoHK,WongE,etal.Thesix-minute walktestinhealthychildren:reabilityandvalidity.EurRespir J.2005;25:1057---60.
18.American Thoracic Society. Guidelines for the six-minute walk test. Am J Resp Crit Care Med. 2002;166: 111---7.
19.TakkenT,EngelbertR,VanBergenM,GroothoffJ,NautaJ,Van HoeckK,etal.Six-minutewalkingtestinchildrenwithESRD: discriminationvalidityandconstructvalidity.PediatrNephrol. 2009;24:2117---223.
20.Santuz P, Baraldi E, Zaramella P, Filippone M, Zacchello F. Factors limitingexercise performance in long termsurvivors of brochopulmonary dysplasia. Am J Respir Crit Care Med. 1995;152:1284---9.
21.WilsonSH,CookeNT,EdwardsRH,SpiroSG.Predictednormal valuesformaximalrespiratorypressuresinCaucasianadultsand children.Thorax.1984;39:535---8.
22.ATSCommitteeonProficiencyStandardsforClinicalPulmonary Function Laboratories.ATSstatement:guidelinesfor the six-minute walk test. Am J Respir Crit Care Med. 2002;166: 111---7.
23.BorgG.EscalaCR10deBorg.In:BorgG,editor.EscalasdeBorg paraadoreesforc¸opercebido.São Paulo:Manole;2000. p. 43---7.
24.Priesnitz CV, Rodrigues GH, Stumpf C, da S, Viapiana G, Cabral CP, Stein RT, et al. Reference values for the 6-min walktestinhealthychildrenaged6-12years.PediatrPulmo. 2009;44:1174---9.
25.MaxwellH,MacKinlayD,WatsonAR.Qualityoflifeorhealth statusinchildrenwithchronickidneydisease.PediatrNephrol. 2010;25:1191---2.
26.AkberA, Portale AA. Johansen.Pedometer-assessed physical activityinchildrenandyoungadultswithCKD.ClinJAmSoc Nephrol.2012;7:720---6.
27.AdeyD,KumarR,MccarthyJT,NairKS.Reducedsynthesisof muscleproteinsinchronicrenal failure.JPhysiolEndocrinol Metab.2000:219---25.
28.DujicZ,TociljJ,LjuticD,EterovicD.Effectsofhemodialysis and anemiaon pulmonary diffusing capacity,membrane dif-fusingcapacityandcapillarybloodvolumeinuremicpatients. Respiration.1991;58:277---81.
29.SiafakasNM, ArgyrakopoulosT, AndreopoulosK, TsoukalasG, TzanakisN,BourosD.Respiratorymusclestrengthduring con-tinuous ambulatoryperitoneal dialysis(CAPD). EurRespir J. 1995;8:109---13.