w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
The
impact
of
comorbidities
on
the
physical
function
in
patients
with
rheumatoid
arthritis
Wanessa
Vieira
Marques
a,∗,
Vitor
Alves
Cruz
b,
Jozelia
Rego
b,
Nilzio
Antonio
da
Silva
b aMedicalSchool,UniversidadeFederaldeGoiás,Goiânia,GO,BrazilbDepartmentofRheumatology,HospitaldasClínicas,MedicalSchool,UniversidadeFederaldeGoiás,Goiânia,GO,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received22August2014 Accepted28January2015 Availableonline10August2015
Keywords:
Rheumatoidarthritis Comorbidities Physicalfunction Mobility
a
b
s
t
r
a
c
t
Objectives:Toinvestigatetheassociationofcomorbiditieswithmobilitylimitationand func-tionaldisabilityinpatientswithrheumatoidarthritisandtoidentifywhichcomorbidity indicatoristhemostappropriatetodeterminethisassociation.
Methods:Sixtyrheumatoidarthritispatientswereenrolledinacross-sectionalstudyfor aperiodof11months.Comorbiditieswereassessed usingthreeindicators:(i)thetotal numberofcomorbidities;(ii)theCharlsoncomorbidityindex;and(iii)thefunctional comor-bidityindex.DiseaseactivitywasassessedusingtheDiseaseActivityScore28.Functional capacitywasmeasuredusingtheHealthAssessmentQuestionnaire,andmobilitywas mea-suredusingTimedUpandGoTestandFive-Times-Sit-to-StandTest.Statisticalanalysiswas performedusingastepwiselog-linearmultipleregressionwithasignificancelevelof5%.
Results:Inthefinalmodel,onlycomorbiditywasassociatedwithmobilitylimitation.The functionalcomorbidityindexscoreexplained19.1%ofthevariabilityofthe Five-Times-Sit-to-StandTest(coefficientofdetermination[R2]=0.191)and19.5%oftheTimedUpandGo
Testvariability(R2=0.195).Withregardtofunctionaldisability,theassociatedfactorswere
comorbidityanddiseaseactivity,whichtogetherexplained32.9%ofthevariabilityofthe HealthAssessmentQuestionnairescore(adjustedR2=0.329).
Conclusion:Comorbiditieswereassociatedwithmobilitylimitationandfunctionaldisability inrheumatoidarthritispatients.Thefunctionalcomorbidityindexprovedtobean appro-priatecomorbidityindicatortodeterminethisassociation.
©2015ElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](W.V.Marques).
http://dx.doi.org/10.1016/j.rbre.2015.07.009
Influência
das
comorbidades
na
capacidade
funcional
de
pacientes
com
artrite
reumatoide
Palavras-chave:
Artritereumatoide Comorbidades Capacidadefuncional Mobilidade
r
e
s
u
m
o
Objetivos: Investigaraassociac¸ãodascomorbidadescomalimitac¸ãodamobilidadeecom aincapacidadefuncionalempacientescomartrite reumatoide,bemcomoidentificaro indicadordecomorbidademaisapropriadoparadeterminaressaassociac¸ão.
Métodos: Emumestudotransversalforamincluídos60pacientescomartritereumatoide porumperíodode11meses.Comorbidadesforamavaliadaspormeiodetrêsindicadores: (i)númerototaldecomorbidades;(ii)índicedecomorbidadedeCharlson;e(iii)índicede comorbidadefuncional. Aatividadedadoenc¸afoiavaliadapelo Índicede Atividadeda Doenc¸a28.AcapacidadefuncionalfoimensuradapeloQuestionáriodeAvaliac¸ãodaSaúde, eamobilidadefoimensuradapelostestessenta-levantadacadeiracincovezesetimedgetup andgo.Aanáliseestatísticafoirealizadaatravésderegressãomúltiplalog-linearStepwise comníveldesignificânciade5%.
Resultados: Nomodelofinal,apenasofatorcomorbidadesesteveassociadoàmobilidade. Oescore noíndicede comorbidadefuncional explicou19,1%da variabilidade doteste senta-levantadacadeiracincovezes(coeficientededeterminac¸ão[R2]=0,191)e19,5%da
variabilidadedotimedgetupandgo(R2=0,195).Emrelac¸ãoàincapacidadefuncional,os
fatoresassociadosforamofatorcomorbidadeseaatividadedadoenc¸aqueemconjunto explicaram32,9%da variabilidadedoescoredoQuestionáriodeAvaliac¸ãodaSaúde(R2
ajustado=0,329).
Conclusão: Ascomorbidadesestãoassociadascomalimitac¸ãodamobilidadeea incapaci-dadefuncionalempacientescomartritereumatoide.Oíndicedecomorbidadefuncional demonstrouserumindicadordecomorbidadeapropriadoparadeterminaressaassociac¸ão. ©2015ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Rheumatoidarthritis(RA)isachronic,progressive,systemic inflammatorydiseasewhichmainlyaffectsthesynovial mem-brane of joints, which may cause general impairment in functionalstatusofpatients.1
Thestudyoffunctionaldisabilityandassociatedfactorsin RAisrelevant,sincethefunctionalstatusisrelatedtoother clinicaloutcomesinthispopulation,suchasmortality,2,3loss
ofworkcapacity,4,5anduseofhealthresources.6,7
Thereisincreasingevidencepointingtotheeffectofthe comorbidityfactorinfunctionaldisabilityinpatientswithRA. Radneretal.8,9demonstratedthenegativeimpactof
comor-biditiesinallareasoffunctionalcapacity,regardlessofthe levelof disease activity.Michaudet al.,10 ina longitudinal
study,showedthatageover65yearsandpresenceof comor-biditieswerethemainpredictorsoffunctionalcapacitylossin RAandthatthesefactorsnotassociatedwiththetreatmentof RAhadthegreatesteffectinscoreprogression,asmeasuredby theHealthAssessmentQuestionnaire(HAQ),incomparison withtheeffectofthetreatmentwithbiologicalagents.
ThestudyofNortonetal.11showedaconsiderable
preva-lenceofcomorbiditiesatthetimeofdiagnosisofRAandthat it increasesover the courseofthe disease.After a15-year follow-up,81%ofRApatientspresentedcomorbiditiesand,in addition,presenceofcomorbiditieswasassociatedwith mor-talityandlossoffunctionalcapacityinthesepatients.11Inan
11-yearlongitudinalstudy,VandenHoeketal.12observedthat
somaticcomorbiditiesanddepressionwereassociatedwith decreasedfunctionalcapacity.
The published literature reveals that comorbidities are commonconditionsinthispopulation,andonaverageeach patient with RA has 1.6 comorbidities; and this number increaseswithage.13,14Inthissense,therehasbeenagrowing
interestfromresearchersinstudyingcomorbiditiesandtheir impactondifferentclinicaloutcomesinRA,suchas hospital-ization,mortality,functionalcapacityandmedicalcosts.13–15
Comorbidity is defined as a disease or medical condi-tion that coexists with the disease of interest, identified, in this case as RA.13 There are several ways to assess
comorbidities.13,15 Theassessmentofthe impactof
comor-biditiesindifferentclinicaloutcomesinpatientswithRAis usually performedthrough asimple countingof the num-berofexistingcomorbiditiesfromaspecificlistestablished byresearchers.15 Usingsuchanapproach,eachconditionis
equallyscored,irrespectiveofitsweight.15
Anotherwayofmeasuringcomorbiditiesinvolvestheuse ofvalidatedcomorbidityindexesforpredictingacertain clin-icaloutcome.13Mostofcomorbidityindexesaredesignedto
determinemortality,whichisthecaseofCharlson comorbid-ityindex(CCI)16andKaplan–Feinsteinindex.17CCIhasbeen
developedbyCharlsonetal.,16andcontainsalistof19
condi-tions,eachofthemhavingaweightaccordingtoitsone-year riskofdeath.Thereisalsoacomorbidityindexspecifically developedtopredictfunctionality,thefunctionalcomorbidity index(FCI).18FCIwasdevelopedbyGrolletal.18usinga
North-Americanpopulationaffectedmainlybyorthopedicproblems and that used the Quality of Life Questionnaire (SF-36) to quantifythesubjects’functionalcapacity.
throughtheHealthAssessmentQuestionnaire(HAQ)and/or bythephysicaldomaincomponentoftheQualityofLife Ques-tionnaire(SF-36);these toolswere developed toassess the functional capacity of patients in activities of daily living. Noneofthesestudieshasaddedmobilitytestsinthe assess-mentoffunctionality.Thus,thementionedstudies8–12didnot
analyzetheassociationofcomorbiditieswithmobility limita-tioninpatientswithRA.
Thepurposeofthisstudywastoinvestigatetheassociation ofcomorbidities,measuredbythreeindicatorsofcomorbidity (totalnumberofcomorbidities,CCIandFCI)withmobility lim-itationandfunctionaldisabilityinpatientswithRA,aswellas toidentifywhichindicatorofcomorbidityismostappropriate todeterminethisassociation.
Methods
Studydesignandparticipants
Across-sectionalstudyincludingpatientswithRAwascarried outtoevaluatetheassociationofcomorbiditieswithmobility limitationandfunctionaldisabilityintheseindividuals.
Sixtypatientsparticipatedinthestudyandwererecruited from the Rheumatology Outpatient Clinic of Hospital das Clínicas, Faculdade de Medicina, Universidade Federal de Goiás(UFG)inthecityofGoiânia,from September13,2012 toAugust22,2013.
At inclusion, all patients met the American College of Rheumatology (ACR 1987) criteria for RA.19 Thosesubjects
withhospitalizationduetoacuteinfectionintheperiodof sixmonthspriortotheinterviewandwithpresenceofsome temporarydisabilitymakingitimpossibletocarryout mobil-ity tests (e.g.,foot fracture) were excluded. Thestudy was approvedbytheResearchEthicsCommitteeoftheHospital das Clínicas (UFG)and all participantssigned aninformed consentform.
Assessmenttools
At the time study enrollment, patients completed a stan-dardizedquestionnaire,includingdetailsof:(i)demographic factorssuchasage,genderand self-reportedrace;(ii) pres-enceofapositiverheumatoidfactor(RF);(iii)diseaseduration; (iv)existing comorbidities;(v)historyoffallsina12-month periodprecedingtheinterview;(vi)useofwalkingaids;(vii) medications inuse; (viii)lifestyle habits (i.e., smoking sta-tus–currentorformersmoker,neversmoked)andphysical activitypractice.Thisquestionnairewassupplementedwith informationfromparticipants’medicalrecords.
In this standardized questionnaire, comorbidities were evaluatedthroughalistofchronicdiseases,accordingtothose coveredbyCCI16andFCI.18Thepresenceofotherchronic
dis-easesnotincludedintheseindexesbutreportedbypatients andconfirmedintheirmedicalrecordswasalsoregistered. Fromthesecollecteddata,comorbiditiesweremeasuredby threeindicators:(i)totalnumberofcomorbidities(NCom);(ii) CCIscore;and(iii)FCIscore.
CCIiscomposedofalistof19comorbidities,andeach dis-easehasaweightrangingfrom1to6,establishedaccording
toitsone-yearriskofdeath.16ThescoreobtainedinCCIis
assigned by summing all comorbiditiespresent with their respective weights, resulting in a number which can vary from0to33.16
FCIisalistof18comorbidities,withnodifferenceinweight amongthem.18FCIscoreisobtainedbysummingall
comor-bidities,rangingfrom0to18.18
Inthe“connectivetissuediseases”itemcontemplatedin CCI, thetool consideredas “comorbidcondition” the pres-ence ofsystemiclupuserythematosus,polymyositis,mixed connective tissue disease and polymyalgia rheumatica, as suggestedbyCharlsonetal.16Ontheotherhand,inFCI,in
its“arthritis” item,onlypresenceofosteoarthritiswas con-sidered.
DiseaseactivitywasassessedbytheDiseaseActivityScore basedon28jointsandonESRvalue(DAS-28/ESR).20
To assess mobility limitation, the following tests were applied:(i)Five-Times-Sit-to-StandTest(STS)21and(ii)Timed
UpandGoTest(TUG).22
STStestisusedtoevaluatemusclestrengthoflowerlimbs, mobilityandriskoffalls.21,23,24Thistest,measuresthefastest
timetostandandsitfiveconsecutivetimeswitharmsfolded. Thelongerthetimespenttocompletethetest,theworsethe individualmobility.21
TUGtestisusedtoidentifypatientsatriskoffallsandwith mobility restriction.22,25 Toperformthis test,the patientis
timedwhiletheyrisefromanarmchair,walkatacomfortable andsafepacetoalineonthefloor3maway,turnandwalk backtothechairandsitdownagain.Thegreaterthetime,the worsetheindividualmobility.22
FunctionaldisabilitywasmeasuredbytheHealth Assess-mentQuestionnaire(HAQ).26,27
Statisticalanalysis
Continuousdataareshownasmean(standarddeviation[SD]) ormedian(interquartilerange[IQR]),whereappropriate,and categoricaldatawereshownasfrequency(percentages).
Aregressionanalysisusingquasi-likelihoodmodel,28with
variancefunctionproportionaltothemeanandlogarithmic link function, was carried out, in order to investigate the associationofindicatorsofcomorbidity(NCom,CCIandFCI) withmobilitylimitation(STSandTUG)andfunctional disabil-ity(HAQ).Tomonitortheeffectofconfounding variables,a linearregression modelusingstepwise regressionwas con-structed.Thepotentialconfounding variableschosenwere: age, gender, disease duration,physicalactivity, positive RF test,DAS-28/ESRscore.
The final model ofmultiple regression analysis for the dependentvariablesSTS,TUGandHAQwascalledstepwise log-linearregression.
Thecomparisonbetweencomorbidityindicators,withthe aimtoestablishthemostappropriatetooltodeterminethe association of comorbidities with mobility limitation and functional disabilityinpatientswithRA,wasperformedby comparingthecoefficientsofdetermination(R2)ofadjusted modelsagainsteachindicator.29
Table1–Characteristicsofparticipants.
Characteristics Values
Demographics
Age,mean(SD)(min–max),years 59(9.1)(43–80)
Women,n(%) 53(88.3%)
Self-reportedrace,n(%)
Caucasian 26(43.3%)
African 11(18.3%)
Brown 23(38.3%)
PositiveRF,n(%) 43(71.7%)
Diseaseduration,mean(SD)(min–max),years 11.5(8.9)(0.4–30) Historyoffalls,n(%) 16(26.7%) Useofwalkingaids,n(%) 8(13.3%) Smokersorformersmokers,n(%) 37(61.7%) Practitionersofphysicalactivity,n(%) 10(16.7%)
Evaluationofcomorbidities
NComscore,mean(SD)(min–max) 3.6(2.1)(0–8) CCIscore,mean(SD)(min–max) 0.25(0.51)(0–2) FCIscore,mean(SD)(min–max) 2.0(1.5)(0–5)
Diseaseactivityassessment
ESR,median(IQR),mm/hour 22.5(10.5–34.5) DAS-28/ESR,mean(SD)(min–max) 3.7(1.4)(0.5–6.8)
Mobilityassessment
STS,median(IQR),seconds 12.5(10.5–20.4) TUG,median(IQR),seconds 12.8(10.9–16.3)
Assessmentoffunctionalcapacity
HAQscore,mean(SD)(min–max) 1.07(0.76)(0–3)
SD,standarddeviation;IQR,interquartilerange;RF,rheumatoid factor;NCom,totalnumberofcomorbidities;CCI,Charlson comor-bidityindex;FCI,functionalcomorbidityindex;ESR,erythrocyte sedimentationrate;DAS-28/ESR,DiseaseActivityScorebasedon 28jointsandonESRvalue;STS,Five-Times-Sit-to-StandTest;TUG, TimedUpandGoTest;HAQ,HealthAssessmentQuestionnaire.
Results
Clinicalfeaturesofparticipants
Sixtypatientsparticipatedinthestudy.Patientcharacteristics aresummarizedinTable1.
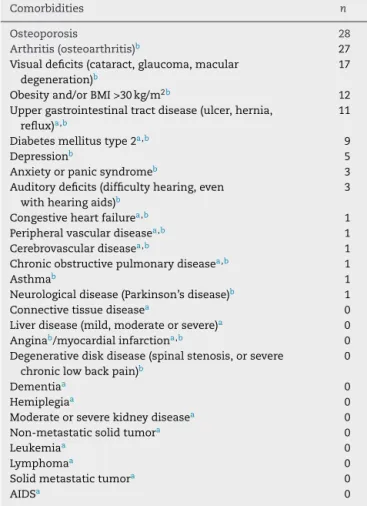
Table2depictsthecomorbiditiesthatmakeupCCIandFCI, aswellasthenumberofpatientsaffectedbyeach comorbid-itypresentintheseindexes.Theprevalenceofcomorbidities given byCCI was 21.7%, i.e., 13 patients had at least one comorbidity,accordingtothisindicator.Intheotherhand,the evaluationbyFCIshowedthat49(81.7%)patientshadatleast onecomorbidity.
Patients had other comorbidities, besides those shown inTable2,suchasfibromyalgia,anemia,epilepsy, hypothy-roidism, secondarySjögren syndrome and cardiac arrhyth-mias.Thus,theprevalenceofcomorbiditiesgivenbyNCom was90%,i.e.,54patientshadatleastonecomorbidity.
Analysisoftheassociationofcomorbiditieswithmobility limitationandfunctionaldisability
Table3summarizeslog-linearregressionunivariateanalyses offactorsassociatedwithmobilitylimitation(STSandTUG) andfunctionaldisability(HAQ)inpatientswithRA.
The independent factors that significantly explain part ofthe variability ofSTSin the univariatemodelwere: age (coefficientofdetermination[R2]=0.074;p=0.023),male gen-der(R2=0.058;p=0.049),diseaseduration(R2=0.056;p=0.042),
NCom score (R2=0.121; p=0.005) and FCI score (R2=0.191, p<0.001).Theindependentfactorsassociatedwith variabil-ity of TUG in the univariate model were: age (R2=0.063; p=0.052), NCom score (R2=0.144, p=0.005) and FCI score (R2=0.195; p=0.001). On the other hand, the independent
factors associated with variability of HAQ in the univari-atemodelwere:diseaseduration(R2=0.047;p=0.040),NCom
score(R2=0.077;p=0.012),FCIscore(R2=0.178,p<0.001)and
DAS-28/ESR(R2=0.244,p<0.001)(Table3).
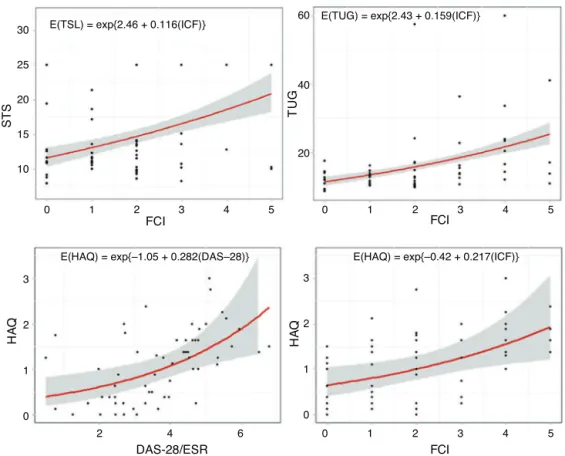
Thelog-linearregressioncurvesofthemainindependent factorsassociatedwithvariabilityofmobility(STSandTUG) andfunctionalcapacity(HAQ)areshowninFig.1.
Inthefinalmodeloflog-linearregressionusingstepwise regression with respecttofactors associated withmobility limitation(STSandTUG),onlythe“comorbidities”factor, eval-uatedbyFCI,wassignificant(Table4).Theexponentvalues ofbetacoefficient(expˇ)fortheassociationbetweenFCIand STSwas1.128(95%confidenceinterval[95%CI]1.062–1.201;
p<0.001);andforTUGwas1172(95%CI1.073–1.285;p=0.001) (Table4).
Astofactorsassociatedwithfunctionaldisability(HAQ)in thefinalmodel,thefollowingvariablesweresignificant: dis-easeactivity,measuredbyDAS-28/ESR(expˇ=1.279, 95%CI 1.132–1.451; p<0.001)and comorbiditiesasassessedbyFCI (expˇ=1.167,95%CI1.054–1.290;p=0.005)(Table4).FCIand DAS-28/ESRfactorsweresignificanttoexplain,together,32.9% ofthevariabilityofHAQscore(adjustedR2=0.329)(Table4).
Comparisonamongcomorbidityindicators
FCIprovedtobethemostappropriatecomorbidityindicator todeterminetheassociationofcomorbiditieswithmobility limitation(STSand TUG)and functionaldisability(HAQ)in patients withRA,accordingtovalues ofthe coefficientsof determination(R2)ofcomorbidityindicators(NCom,CCIand
FCI)(Table3).
TheR2valueforanassociationbetweenFCIandSTSwas
0.191;forTUGwas0.195;andforHAQwas0.178.Ontheother hand,R2betweenNComandSTSwas0.121;forTUG,R2=0.144;
andforHAQ,R2=0.077.AndtheR2valuebetweenCCIandSTS
was0.021;forTUG,R2=0.000;andforHAQ,R2=0.000(Table3).
Discussion
This study demonstrated the association of comorbidities withmobilitylimitationandfunctionaldisabilityinpatients withRAandindicatedFCIasanappropriatecomorbidityindex indeterminingthisassociation.
Table2–ComorbiditiesthatcomposetheCharlson
comorbidityindexandthefunctionalcomorbidityindex
andnumberofaffectedpatients.
Comorbidities n
Osteoporosis 28
Arthritis(osteoarthritis)b 27 Visualdeficits(cataract,glaucoma,macular
degeneration)b
17
Obesityand/orBMI>30kg/m2b 12
Uppergastrointestinaltractdisease(ulcer,hernia, reflux)a,b
11
Diabetesmellitustype2a,b 9
Depressionb 5
Anxietyorpanicsyndromeb 3
Auditorydeficits(difficultyhearing,even withhearingaids)b
3
Congestiveheartfailurea,b 1
Peripheralvasculardiseasea,b 1
Cerebrovasculardiseasea,b 1
Chronicobstructivepulmonarydiseasea,b 1
Asthmab 1
Neurologicaldisease(Parkinson’sdisease)b 1
Connectivetissuediseasea 0
Liverdisease(mild,moderateorsevere)a 0
Anginab/myocardialinfarctiona,b 0
Degenerativediskdisease(spinalstenosis,orsevere chroniclowbackpain)b
0
Dementiaa 0
Hemiplegiaa 0
Moderateorseverekidneydiseasea 0
Non-metastaticsolidtumora 0
Leukemiaa 0
Lymphomaa 0
Solidmetastatictumora 0
AIDSa 0
CCI, Charlson comorbidity index; FCI, functional comorbidity index;BMI,bodymassindex;AIDS,acquiredimmunodeficiency syndrome.
a ComorbiditypresentinCCI.
b ComorbiditypresentinFCI.
was32.9%;and“diseaseactivity”,measuredbyDAS-28/ESR, wasthemainvariableresponsibleforexplainingpartofthis variability, followed bythe factor “comorbidities”,assessed byFCI. In the finalmodel – afterFCI and DAS-28/ESRhad explainedpartofthevariabilityofHAQscore,andafterFCI hadexplainedpart ofthevariabilityofSTSand TUG–the remaininganalyzedvariablesdidnotcontributesignificantly toexplain the mobilitylimitation and functional disability observed,showingtheimportanceofthefactor “comorbidi-ties”inthefaceofothervariables,suchasage,gender,disease duration,physicalactivityandapositiveRF.
FunctionaldisabilityinRAischaracterizedbyits multi-dimensionality,beingassociatedwithmultiplefactors,aside thefactor“comorbidities”,8–12suchaspain,30,31reducedjoint
mobility,30articularcartilagedestruction,32decreasedmuscle
strength,31diseaseduration33anddiseaseactivity.31
Theassociationofcomorbiditieswithfunctionaldisability inpatientswithRAhasbeenshowninsomestudies,8–12 in
whichtheauthorsassessedthefunctionalcapacityofpatients throughactivitiesofdailylivingquestionnaires(HAQand/or SF-36).
Toour knowledge,thisis thefirst study onRApatients todeterminetheassociationofcomorbiditieswithmobility limitationmeasuredbytimedtests(STSandTUG).
ThefactthatRAisresponsibleforageneralimpairment intermsoffunctionalstatusofpatients,causingimpairment inactivitiesofdailyliving,musclestrengthandmobilityand increasing the risk offalls, emphasizes the importanceof mobilitystudiesinthispopulation.31,34,35
Theriskoffallscanbeevaluatedthroughthetimespent toperformSTSandTUGtests24,25,36and,inparallel,studies
haveshownaworseperformanceonthesetestsinpatients withRA,whencomparedtothepopulationwithoutRA.37,38
Böhleretal.36showedthatdiseaseactivityandfunctional
disability (HAQ) in patientswith RAcorrelated with worse performanceinSTSandTUGtests;but theauthorsdidnot evaluatethe association ofcomorbidities withriskoffalls. Jamisonetal.39demonstratedthatpatientswithRAwitha
his-toryoffallsexhibitedahighernumberofcomorbiditiesthan thosewithoutsuchhistory,drawingattentiontothe associa-tionbetweencomorbiditiesandtheoccurrenceoffallsinthis population.AsoccurredinthestudybyBöhleretal.,36Jamison
etal.39havenotstudiedtheassociationofcomorbiditieswith
performancetestsforfallriskassessment(STSandTUG). Thestudyoffactorsassociatedwithriskoffallsinpatients with RA isa relevant task, sincethe risk of fallsin these patientsisincreased.34–37,39,40Falls,inturn,arerelatedtothe
occurrenceoffractures;andthiscontingencyhastheeffect ofcompromisingthefunctionality,worseningtheprognosis ofrheumatologicdiseases.35Alsonoteworthyisanincreased
prevalenceofosteoporosisinpatientswithRA.11,13,15Inour
study,28patients(47%)hadosteoporosis,andthisisa comor-biditywhichincreasesfracturerisk.37,41
In the present study, we evaluated the association of comorbiditieswithmobilitylimitationandfunctional disabil-ity inpatients with RAby computingthe total number of comorbidities(NCom)and throughthe scoreobtainedwith theuseofCCIandFCI.
FCIprovedtobethemostappropriatecomorbidity indica-torindeterminingthisassociation,whencomparedtoNCom andCCIinoursample.Theassociationofcomorbidities evalu-atedbyFCIwasstrongerversusthatmeasuredbyNCom.This resultwasexpected,sinceFCIhasbeenspeciallydeveloped asatooltopredictfunctionality.18Thisfindingishighlighted
by the fact that RA patients studied often presentedwith comorbiditiespresentinFCI,thesebeingconditionsclearly associatedwithfunctionalimpairment.18
Ontheotherhand,thelackofassociationofthose comor-biditiesassessedbyCCIinoursample,notwithstandingthe demonstrationofthisrelationshipwiththeuseofCCIinother studies,8,9,11canbeexplainedintwoways.First,wemust
con-siderthatCCIwasprimarilydevelopedasaninstrumentto predictmortality.16Andsecondly,wedidnotfindinour
sam-pleareasonableamountofcomorbiditiespertainingtothe calculationofICC,andthisfactmayhavehamperedthe abil-ity ofthis indexinpredictingfunctionalityinourpatients. Perhapsthisscenariowouldrequirealargersample,asthe comorbidities that make up CCI are not those most often foundinoutpatientswithRA.8,9,11
Table3–Analysisofindependentfactorsassociatedwithmobilitylimitation(Five-Times-Sit-to-StandTestandTimed
UpandGoTest)andfunctionaldisability(HealthAssessmentQuestionnaire).
Independentvariables Dependentvariables
STS TUG HAQ
Age,years R2 0.074a 0.063a 0.002
Malegender R2 0.058a 0.010 0.000
PositiveRF R2 0.000 0.000 0.000
Diseaseduration,years R2 0.056a 0.020 0.047a
Physicalactivity R2 0.000 0.003 0.013
NComscore R2 0.121b 0.144b 0.077b
CCIscore R2 0.021 0.000 0.000
FCIscore R2 0.191b 0.195b 0.178b
DAS-28/ESR R2 0.033 0.056 0.244b
STS,Five-Times-Sit-to-StandTest;TUG,TimedUpandGoTest;HAQ,HealthAssessmentQuestionnaire;R2,coefficientofdetermination;RF, rheumatoidfactor;NCom,totalnumberofcomorbidities;CCI,Charlsoncomorbidityindex;FCI,functionalcomorbidityindex;DAS-28/ESR, DiseaseActivityScorebasedon28jointsandonESRvalue.
Univariatelog-linearregressions. a Significantp≤ 0.05.
b Significantp≤ 0.01.
reportsandonmedicalrecords;thus,thisidentificationwas subjecttounderdiagnosis, whencompared toasystematic searchofassociateddiseases.Inaddition, inNCom indica-torallcomorbiditiesreportedbypatientsandpresentintheir medicalrecordswereconsidered,withoutestablishing spe-cificcriteriaonwhichdiseaseswouldbe,ornot,takeninto
account.ThismethodmayhavehamperedtheabilityofNCom indicatorindeterminingtheassociationwithfunctional dis-abilityinoursample,whereasotherstudieshavestressedthis association.10–12
Thus, it becomes apparent the importance of knowing whatarethemaincomorbiditiesthatultimatelyinfluencethe
DAS-28/ESR
FCI FCI
STS TU
G
HA
Q
HA
Q
30
10
3
2
1
0
3
2
1
0
2 4 6
0 1 2 3 4 5 0 1 2 3 4 5
15 20
20 40 60
25
E(TUG) = exp{2.43 + 0.159(ICF)} E(TSL) = exp{2.46 + 0.116(ICF)}
E(HAQ) = exp{–1.05 + 0.282(DAS–28)} E(HAQ) = exp{–0.42 + 0.217(ICF)}
FCI
0 1 2 3 4 5
Fig.1–Log-linearregressioncurvesofthemainpredictorsofmobilityvariability(Five-Times-Sit-to-StandTestandTimed UpandGoTest)andfunctionalcapacity(HealthAssessmentQuestionnaire).Scatterplotswithlog–linearregressioncurves.
STS,Five-Times-Sit-to-StandTest;TUG,TimedUpandGoTest;HAQ,HealthAssessmentQuestionnaire;FCI,functional
Table4–Impactofcomorbidity(functionalcomorbidityindex)anddiseaseactivity(DiseaseActivityScorebased
on28jointsandonESRvalue)inmobility(Five-Times-Sit-to-StandTestandTimedUpandGoTest)andfunctional
capacity(HealthAssessmentQuestionnaire).
Dependentvariables Independentvariables exp(ˇ) 95%CI p AdjustedR2
STS FCI 1.128 1.062–1.201 <0.001 0.191
TUG FCI 1.172 1.073–1.285 0.001 0.195
HAQ FCI 1.167 1.054–1.290 0.005 0.329
DAS-28/ESR 1.279 1.132–1.451 <0.001
STS,Five-Times-Sit-to-StandTest;TUG,TimedUpandGoTest;HAQ,HealthAssessmentQuestionnaire;exp(ˇ),exponentialofbetacoefficient; 95%CI,confidenceintervalof95%;R2,coefficientofdetermination;FCI,functionalcomorbidityindex;DAS-28/ESR,DiseaseActivityScorebased on28jointsandonESRvalue.
Multivariatelog-linearregressionmodelusingstepwiseregression.
functionalityinpatients withRA;withthis,we canobtain moresuitable criteria,when establishingthe comorbidities associatedwithfunctionalstatusofthispopulation.
This study has relevance for pointing out the effect of
comorbiditiesonlimitingthemobilityand,hence,on increas-ingtheriskoffallsinpatientswithRA;itmustbetakeninto
accountthatthetestsused(STSandTUG)arerecommended
inthefallriskassessment.Inaddition,thestudyalsodraws attentiontotheuseofFCIasanalternativetooltoevaluate theimpactofcomorbiditiesonfunctionalityofpatientswith RA.
Inconclusion,thecomorbiditiesinpatientswithRAare associatedwithmobilitylimitationandfunctionaldisability; andtheindicatorFCIisanappropriatecomorbidityindexin thedeterminationofthisassociation.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. ScottDL,WolfeF,HuizingaTW.Rheumatoidarthritis.Lancet. 2010;376:1094–108.
2. WolfeF,MichaudK,GefellerO,ChoiHK.Predictingmortality inpatientswithrheumatoidarthritis.ArthritisRheum. 2003;48:1530–42.
3. FarragherTM,LuntM,BunnDK,SilmanAJ,SymmonsDP. Earlyfunctionaldisabilitypredictsbothall-causeand cardiovascularmortalityinpeoplewithinflammatory polyarthritis:resultsfromtheNorfolkArthritisRegister.Ann RheumDis.2007;66:486–92.
4. deCroonEM,SluiterJK,NijssenTF,DijkmansBA,Lankhorst GJ,Frings-DresenMH.Predictivefactorsofworkdisabilityin rheumatoidarthritis:asystematicliteraturereview.Ann RheumDis.2004;63:1362–7.
5. AllaireS,WolfeF,NiuJ,LaValleyMP,ZhangB,ReisineS. Currentriskfactorsforworkdisabilityassociatedwith rheumatoidarthritis:recentdatafromaUSnationalcohort. ArthritisRheum.2009;61:321–8.
6. MichaudK,MesserJ,ChoiHK,WolfeF.Directmedicalcosts andtheirpredictorsinpatientswithrheumatoidarthritis:a three-yearstudyof7.527patients.ArthritisRheum. 2003;48:2750–62.
7. YelinE,WankeLA.Anassessmentoftheannualand long-termdirectcostsofrheumatoidarthritis:theimpactof
poorfunctionandfunctionaldecline.ArthritisRheum. 1999;42:1209–18.
8.RadnerH,SmolenJS,AletahaD.Impactofcomorbidityon physicalfunctioninpatientswithrheumatoidarthritis.Ann RheumDis.2010;69:536–41.
9.RadnerH,SmolenJS,AletahaD.Comorbidityaffectsall domainsofphysicalfunctionandqualityoflifeinpatients withrheumatoidarthritis.Rheumatology(Oxford). 2011;50:381–8.
10.MichaudK,WallensteinG,WolfeF.Treatmentand
nontreatmentpredictorsofhealthassessmentquestionnaire disabilityprogressioninrheumatoidarthritis:alongitudinal studyof18,485patients.ArthritisCareRes(Hoboken). 2011;63:366–72.
11.NortonS,KoduriG,NikiphorouE,DixeyJ,WilliamsP,Young A.Astudyofbaselineprevalenceandcumulativeincidence ofcomorbidityandextra-articularmanifestationsinRAand theirimpactonoutcome.Rheumatology(Oxford).
2013;52:99–110.
12.vandenHoekJ,RoordaLD,BoshuizenHC,vanHessJ,RuppI, TijhuisGJ,etal.Long-termphysicalfunctioningandits associationwithsomaticcomorbidityandcomorbid depressioninpatientswithestablishedrheumatoidarthritis: alongitudinalstudy.ArthritisCareRes(Hoboken).
2013;65:1157–65.
13.MichaudK,WolfeF.Comorbiditiesinrheumatoidarthritis. BestPractResClinRheumatol.2007;21:885–906.
14.GabrielSE,MichaudK.Epidemiologicalstudiesinincidence, prevalence,mortality,andcomorbidityoftherheumatic diseases.ArthritisResTher.2009;11:229–45.
15.GullickNJ,ScottDL.Co-morbiditiesinestablishedrheumatoid arthritis.BestPractResClinRheumatol.2011;25:469–83. 16.CharlsonME,PompeiP,AlesKL,MacKenzieCR.Anewmethod
ofclassifyingprognosticcomorbidityinlongitudinalstudies: developmentandvalidation.JChronicDis.1987;40:373–83. 17.KaplanMH,FeinsteinAR.Theimportanceofclassifying
initialco-morbidityinevaluatingtheoutcomeofdiabetes mellitus.JChronicDis.1974;27:387–404.
18.GrollDL,ToT,BombardierC,WrightJG.Thedevelopmentofa comorbidityindexwithphysicalfunctionastheoutcome.J ClinEpidemiol.2005;58:595–602.
19.ArnettFC,EdworthySM,BlochDA,McShaneDJ,FriesJF, CooperNS,etal.TheAmericanRheumatismAssociation 1987revisedcriteriafortheclassificationofrheumatoid arthritis.ArthritisRheum.1988;31:315–24.
20.PrevooML,van‘tHofMA,KuperHH,vanLeeuwenMA,vande PutteLB,vanRielPL.Modifieddiseaseactivityscoresthat includetwenty-eight-jointcount:developmentand
validationinaprospectivelongitudinalstudyofpatientswith rheumatoidarthritis.ArthritisRheum.1995;38:44–8.
assessinglowerextremityfunction:associationwith self-reporteddisabilityandpredictionofmortalityand nursinghomeadmission.JGerontol.1994;49:M85–94.
22.PodsiadloD,RichardsonS.ThetimedUp&Go:atestofbasic functionalmobilityforfrailelderlypersons.JAmGeriatrSoc. 1991;39:142–8.
23.BohannonRW.Sit-to-standtestformeasuringperformanceof lowerextremitymuscles.PerceptMotorSkill.1995;80:163–6.
24.BuatoisS,Perret-GuillaumeC,GueguenR,MigetP,Vanc¸onG, PerrinP,etal.Asimpleclinicalscaletostratifyriskof recurrentfallsincommunity-dwellingadultsaged65years andolder.PhysTher.2010;90:550–60.
25.PanelonPreventionofFallsinOlderPersons,American GeriatricsSocietyandBritishGeriatricsSociety.Summaryof theUpdatedAmericanGeriatricsSociety/BritishGeriatrics Societyclinicalpracticeguidelineforpreventionoffallsin olderpersons.JAmGeriatrSoc.2011;59:148–57.
26.FriesJF,SpitzP,KrainesRG,HolmanHR.Measurementof patientoutcomeinarthritis.ArthritisRheum.1980;23:137–45.
27.FerrazMB,OliveiraLM,AraujoPM,AtraE,TugwellP. Crossculturalreliabilityofthephysicalabilitydimensionof thehealthassessmentquestionnaire.JRheumatol. 1990;17:813–7.
28.WedderburnRWM.Quasilikelihoodfunctions,generalized linearmodels,andtheGauss–Newtonmethod.Biometrika. 1974;61:439–47.
29.CameronAC,WindmeijerFAG.R-squaredforcountdata regressionmodelswithapplicationsforhealth-care utilization.JBusEconStat.1996;14:209–20.
30.HäkkinenA,KautiainenH,HannonenP,YlinenJ,
Arkela-KautiainenM,SokkaT.Painandjointmobilityexplain individualsubdimensionsofthehealthassessment
questionnaire(HAQ)disabilityindexinpatientswith rheumatoidarthritis.AnnRheumDis.2005;64:59–63.
31.HäkkinenA,KautiainenH,HannonenP,YlinenJ,MäkinenH, SokkaT.Musclestrength,pain,anddiseaseactivityexplain
individualsubdimensionsoftheHealthAssessment Questionnairedisabilityindex,especiallyinwomenwith rheumatoidarthritis.AnnRheumDis.2006;65:30–4.
32.AletahaD,FunovitsJ,SmolenJS.Physicaldisabilityin rheumatoidarthritisisassociatedwithcartilagedamage ratherthanbonedestruction.AnnRheumDis.2011;70:733–9.
33.AletahaD,WardMM.Durationofrheumatoidarthritis influencesthedegreeoffunctionalimprovementinclinical trials.AnnRheumDis.2006;65:227–33.
34.ArmstrongC,SwarbrickCM,PyeSR,O’NeillTW.Occurrence andriskfactorsforfallsinrheumatoidarthritis.AnnRheum Dis.2005;64:1602–4.
35.StanmoreEK,OldhamJ,SkeltonDA,O’NeillT,PillingM, CampbellAJ,etal.Fallincidenceandoutcomesoffallsina prospectivestudyofadultswithrheumatoidarthritis. ArthritisCareRes(Hoboken).2013;65:737–44.
36.BöhlerC,RadnerH,ErnstM,BinderA,StammT,AletahaD, etal.Rheumatoidarthritisandfalls:theinfluenceofdisease activity.Rheumatology(Oxford).2012;51:2051–7.
37.KazKazH,JohnsonD,KerryS,ChinappenU,TweedK,PatelS. Fall-relatedriskfactorsandosteoporosisinwomenwith rheumatoidarthritis.Rheumatology(Oxford).
2004;43:1267–71.
38.ButlerAA,MenantJC,TiedemannAC,LordSR.Ageand genderdifferencesinseventestsoffunctionalmobility.J NeuroengRehabil.2009;6:31–40.
39.JamisonM,NeubergerGB,MillerPA.Correlatesoffallsand fearoffallingamongadultswithrheumatoidarthritis. ArthritisRheum.2003;49:673–80.
40.MarquesWV,CruzVA,RegoJ,SilvaNA.Theinfluenceof physicalfunctionontheriskoffallsamongadultswith rheumatoidarthritis.RevBrasReumatol.2014;54:404–8.