REVISTA
PAULISTA
DE
PEDIATRIA
www.rpped.com.br
REVIEW
ARTICLE
Diagnosis
of
infant
synostotic
and
nonsynostotic
cranial
deformities:
a
review
for
pediatricians
Enrico
Ghizoni
a,∗,
Rafael
Denadai
b,
Cesar
Augusto
Raposo-Amaral
b,
Andrei
Fernandes
Joaquim
a,
Helder
Tedeschi
a,
Cassio
Eduardo
Raposo-Amaral
baUniversidadeEstadualdeCampinas(Unicamp),Campinas,SP,Brazil
bInstitutodeCirurgiaePlásticaCrânioFacial,HospitalSOBRAPAR,Campinas,SP,Brazil
Received20October2015;accepted11January2016 Availableonline23February2016
KEYWORDS
Craniofacial abnormalities; Craniosynostosis; Diagnosis; Pediatricians
Abstract
Objective: Toreviewthecurrentcomprehensivecarefornonsyndromiccraniosynostosis and
nonsynostoticcranialdeformityandtoofferanoverallviewofthesecraniofacialconditions.
Datasource:ThereviewwasconductedinthePubMed,SciELO,andLILACSdatabaseswithout
timeorlanguagerestrictions.Relevantarticleswereselectedforthereview.
Datasynthesis: Weincludedtheanatomyandphysiologyofnormalskulldevelopmentof
chil-dren,discussingnuancesrelated tonomenclature,epidemiology,etiology,andtreatmentof
the mostcommonforms ofnonsyndromic craniosynostosis.The clinicalcriteria for the
dif-ferential diagnosis between positional deformities andnonsyndromic craniosynostosis were
also discussed,givingtothepediatrician subsidiesforaquick andsafe clinicaldiagnosis.If
positionaldeformityisaccuratelydiagnosed,itcanbetreatedsuccessfullywithbehavior
mod-ification.Diagnosticdoubtsandcraniosynostosispatientsshouldbereferredstraightawaytoa
multidisciplinarycraniofacialcenter.
Conclusions: Pediatriciansareintheforefrontofthediagnosisofpatientswithcranial
defor-mities.Thus,itisofparamountimportancethattheyrecognizesubtlecranialdeformitiesasit
mayberelatedtoprematurefusionofcranialsutures.
©2016SociedadedePediatriadeS˜aoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen
accessarticleundertheCCBYlicense(http://creativecommons.org/licenses/by/4.0/).
∗Correspondingauthor.
E-mail:[email protected](E.Ghizoni).
http://dx.doi.org/10.1016/j.rppede.2016.02.005
PALAVRAS-CHAVE
Anormalidades craniofaciais; Craniossinostose; Diagnóstico; Pediatras
Diagnósticodasdeformidadescranianassinostóticasenãosinostóticasembebês: umarevisãoparapediatras
Resumo
Objetivo: Revisaroatendimentointegralatualdecraniossinostosenãosindrômicae
deformi-dadecraniananãosinostóticaeoferecerumavisãoglobaldessascondic¸õescraniofaciais.
Fontesdedados: A revisãofoi realizada nasbasesde dadosPubMed,SciELO, LILACSesem
restric¸õesdetempoouidioma.Artigosrelevantesforamselecionadosparaarevisão.
Síntesedosdados: Foramincluídasaanatomiaefisiologiadodesenvolvimentonormaldocrânio
emcrianc¸as,discutindonuancesrelacionadasànomenclatura,epidemiologia,etiologiae
trata-mentodasformasmaiscomunsdecraniossinostosenãosindrômica.Tambémforamdiscutidosos
critériosclínicosparaodiagnósticodiferencialentredeformidadesposicionaise
craniossinos-tosenãosindrômica,dandoaospediatrassubsídiosparaumdiagnósticoclínicorápidoeseguro.
Sedeformidadesposicionaisforemdiagnosticadascomprecisão,elaspodemsertratadascom
sucessoatravésdamodificac¸ãodocomportamento.Dúvidasdediagnósticoepacientes
porta-doresdecraniossinostosedevemserencaminhadosimediatamenteaumcentromultidisciplinar
craniofacial.
Conclusões: Ospediatrasestãonavanguardadodiagnósticodepacientescomdeformidades
cranianas.Assim,édesumaimportânciaquereconhec¸amdeformidadescranianassutis,pois
elaspodemestarrelacionadasàfusãoprematuradassuturascranianas.
©2016SociedadedePediatriadeS˜aoPaulo.PublicadoporElsevierEditoraLtda.Este ´eum
artigoOpenAccesssobumalicenc¸aCCBY(http://creativecommons.org/licenses/by/4.0/).
Introduction
Cranialdeformities are a common complaint in pediatric units,since25%ofinfantsofsinglepregnanciesand50%of multiplepregnancieshavesomedegreeofskulldeformityat birth.Ingeneral,parentsusuallyrecognizethesechangesin thefirst weeksor months of life.1 However,in some
sce-nariosthediagnosismaybeoverlookedby thefamilythat tends to deny the problem. In these cases, pediatricians mustbe awareof theseissues andcounsel the familyfor theimportancetoseekacraniofacialteam.Inaddition,itis offundamentalimportancethatpediatricianbepreparedat firstconsultationtomakethedifferentialdiagnosisbetween apositionaldeformityandcraniosynostosis,consideringthat childrenbornwithapositionaldeformitydoesnotneedto beexposedtothe ionizingradiation ofacomputed tomo-graphy(CT),apartfromthecostsoftheprocedureandthe sedationriskstoachieveit.2
Inthisreport,wereviewtheanatomyandphysiologyof normal skulldevelopment of children, discussing nuances relatedtonomenclature,epidemiology,etiology,and treat-mentof the most commonforms ofcraniosynostosis. The clinicalcriteriaforthedifferentialdiagnosisbetween posi-tionaldeformitiesandcraniosynostosisarealsopresented, allowingthepediatriciansubsidiesforaquickandsafe clin-icaldiagnosis.
Method
The present study is a literature review, with a descrip-tive approach. We performed a literature review by searching the Medline (PubMed), SciELO, and LILACS databaseswithouttimeor languagerestrictions.The final
literature review was performed on July 2015. To iden-tify all relevant articles (review articles, clinical trials, andcohortstudies)about thecurrentcomprehensive care for nonsyndromic craniosynostosis and nonsynostotic cra-nial deformity the following search terms were used: ‘‘nonsyndromic craniosynostosis’’, ‘‘nonsynostotic cranial deformity’’, ‘‘positional deformity’’. ‘‘nonsynostotic pos-terior plagiocephaly’’, and ‘‘positional plagiocephaly’’. Each relevant study was individually reviewed to iden-tify information concerning normal skull development of children, nomenclature, epidemiology, etiology, diag-nosis, and treatment of the most common forms of nonsyndromic craniosynostosis and nonsynostotic cranial deformity.
Cranialanatomy
The skullofanewborniscomposedofmultiplebonesand suturesthatmakeitmalleableandsubjecttoexternalforces thatdeformit,toenableitspassagethroughthebirthcanal andtoaccommodatetheencephalon,sincethebrainvolume isquadrupledinthefirsttwoyearsoflife.3
The skullis composed of fourmajor sutures (metopic, sagittal, coronal,and lambdoid), threesecondary sutures (frontonasal, temporal squamosal, and frontosphenoidal), andfourmainbones(temporal,frontal,parietal,and occip-ital).Themetopicsutureseparatesthefrontalbonesfrom eachother,thesagittalsuturefromtheparietalbones;the coronal suture from the parietal and frontal bones, and thelambdoidsuturefromtheparietalandoccipitalbones.3
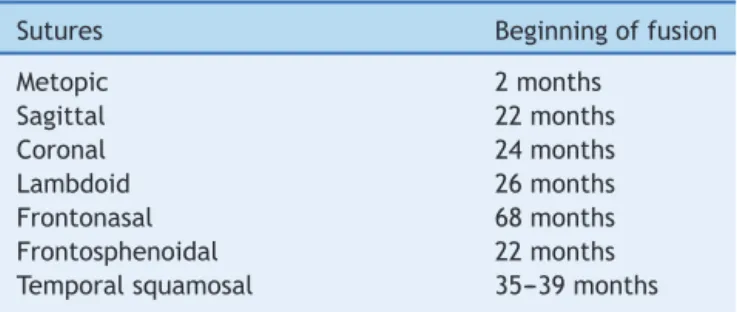
Table1 Majorandsecondaryskullsuturesandageatthe
onsetoffusion3
Sutures Beginningoffusion
Metopic 2months
Sagittal 22months
Coronal 24months
Lambdoid 26months
Frontonasal 68months
Frontosphenoidal 22months
Temporalsquamosal 35---39months
thefrontalandparietalbones)andtheposteriororlambdoid (boundedbytheoccipitalboneandparietalbones).
Under physiological conditions, the cranial sutures progressintofusionwithdifferentinitialperiodsoffusion accordingtoeachmajorsuture(Table1).Thesameoccurs withthefontanelles,whichusuallyclosethemselvesbythe secondyear(Table2).
Animportantdetailisthattheskullbonesare membra-nous(withoutapriorcartilaginousphase),whichresultsin growththroughthebonedepositintheregionofthesutures; thisgrowthoccursperpendiculartothesuture.For exam-ple,coronalsuturesallowtheanterior-posteriorgrowthof the skull, while the sagittal suture allows growth of the biparietalskull.3
Craniosynostosis
The definition of craniosynostosisis the prematurefusion ofoneor morecranial sutures.The occurrenceis approx-imately one for 2000 to2500 live births.4 The premature
fusionofsuturespreventsperpendiculargrowthoftheskull, and an increase inbrain volumeleads to acompensatory growthoftheskullparalleltothis.
Craniosynostosis areclassifiedasprimaryor secondary. Primarycraniosynostosisresultsfromgeneticand environ-mentalinfluences,beingclassifiedassimpleandcomplex. Complex craniosynostosis are divided even further into nonsyndromic and syndromic (Table 3).5---8 Due to the
greater prevalence, we will discuss the diagnosis of sim-ple primary craniosynostosis, namely sagittal, coronal, metopic,andlambdoidsynostoses(Fig.1).Thenthe nonsyn-ostotic posterior plagiocephaly (positional plagiocephaly) will be presented, emphasizing important features for differential diagnosis with lambdoid synostosis (posterior plagiocephaly).
Table2 Ageofclosureofcranialfontanelles3
Fontanelles Ageofclosure
Anteriororbregmatic 24months
Posteriororlambdoid 3months
Anterolateral(Sphenoid) 6---24months
Posterolateral(Mastoid) 6---24months
Table3 Classificationofcraniosynostoses.
1.Primary
Simple(involvingasinglesuture):Sagittal,Coronal,
Metopic,andLambdoid
Complex(fusionoftwoormoresutures)
Nonsyndromic:Bicoronal
Syndromic:Crouzon,Apert,Pfeiffer,andSaethre-Chotzen
2.Secondary
Metabolicdisorders:Hyperthyroidism,InbornErrorsof
Metabolism
Variousmalformations:Microcephaly,Encephalocele
AfterventricularshuntwithexcessivedrainageofCSF
(cerebrospinalfluid)
Fetalexposuretocertainsubstances:Valproicacid,
Phenytoin
Mucopolysaccharidosis
Geneticaspects
Multiple hypotheses have been proposed to explain the pathogenesis of abnormal suture fusion. Both environ-mental (especially intrauterine fetal head constraint) andgenetics factors (single genemutations, chromosome abnormalities and polygenic background) predispose to craniosynostosis.9---11 Mutationsin 7genes(namely,FGFR1,
FGFR2, FGFR3, TWIST1, EFNB1, MSX2 and RAB23) are unequivocallyassociatedwithMendelianformsofsyndromic craniosynostosis.9---11 In contrast, the genetic etiology of
nonsyndromiccraniosynostosisremainedpoorlyunderstood until very recently.9---11 In the last years, epidemiologic
and phenotypic studies clearly demonstrate that nonsyn-dromic craniosynostosis is a complex and heterogeneous conditionsupportedbyastronggeneticcomponent accom-panied by environmental factors that contribute to the pathogenesisnetworkofthisbirth defect.9,10 Infact,rare
mutations in FGFRs, TWIST1, LRIT3, ALX4, IGFR1,EFNA4, RUNX2,andFREM1havebeenreportedinaminorfractionof patientswithnonsyndromiccraniosynostosis.9,10 The
mini-mummoleculargenetictestsrecommendedforeachclinical presentation (syndromic and nonsyndromic craniosynosto-sis)havebeenpreviouslypublishedreview10 andareoutof
thescopeofthisreport.Furtherresearchofalarge popu-lationwithphenotypicallyhomogeneoussubsetsofpatients isrequired tounderstand the complexgenetic,maternal, environmental,andstochasticfactorscontributingto non-syndromiccraniosynostosis.9---11
Generaldiagnosticapproach
Pediatricians are expected to be able to recognize skull deformitiesandtodiagnosethemaseithercraniosynostosis orapositionalskulldeformity.Ifaskulldeformityispresent, the physical examination and clinical history (key fea-turesdescribedinthenextsubheads)arethemosthelpful andrevealing pieces of information in thechild’s evalua-tion.Apreviouspublishedanamnesticflowchart12servesas
Figure1 (A,Left)Frontalphotographofpatientwithprematurefusionofsagittalsutureshowingthecharacteristictemporal
pinching.(Right)Lateralphotographrevelingincreaseintheanterior-posteriordiameteroftheskull(longnarrowskull),thefrontal
bossingandoccipitalbulging(occipitalbullet),whicharethemainclinicalcharacteristicsofsagittalcraniosynostosis.(B,Left)
Frontalphotographofpatientwithprematurefusionoftherightcoronalsutureshowingtheretrusionoftheipsilateralfrontalbone
fusionandcompensatorycontralateralbulging,asymmetryoftheeyebrows,orbits,ears,nose,jaw,aswellasconvergentstrabismus
ofthelefteye.(Right)3DCTreconstructionshowingtheprematurefusionoftherightcoronalsutureandtheelevationofthe
ipsilateralsphenoidwingleadingtoanelongateorbit,recognizedasthe‘‘harlequinorbit’’.(C,Left)Frontalphotographofpatient
withprematurefusionofmetopicsutureshowingthetriangularaspectoftheforeheadwithretrudedcrestsoftheorbitsbilaterally
andhypoteleorbitism(approximationoforbits).(Right)Basalview revealingthetriangularappearanceoftheskull.(D)Lateral
photographofpatient withprematurefusionoflambdoidsutureshowingtheturricephalicaspectoftheskull.Two-dimensional
photographsandradiologicaldocumentationsbelongtoSOBRAPARHospital’sarchives.Informedconsentformsweresignedbythe
patient’sparents.
craniosynostosesfromthenonsynostoticdeformitiesare:(1) ‘‘Isdeformitypresentatbirth?’’Craniosynostosisispresent atbirth,whereasnonsynostoticdeformitiesdevelopinthe neonatalperiod;(2)Isthereapreferredsleepposition?;(3) ‘‘Isthereimprovementofthedeformity?’’Craniosynostosis getsworse withtime,whereasthenonsynostotic deformi-tiesimproveasthechilddevelopsheadcontrolandtheskull nolongerhaslocalizedpressureforlongperiods’’.12
In rare and difficult cases, when the examination and historyarenotdiagnostic,agood-quality four-view radio-graphic series (anteroposterior, Towne and two lateral projections)might be sufficient toexclude craniosynosto-sisandavoid furtherradiationexposure.13 Ifit isunclear,
because of the very young age of the patient, it is rec-ommendedto repeatX-skull after 1 or 2 months.14 CT is
not the recommended modality for screening because of the associated radiation exposure and high imaging costs
anddiagnosticsbypediatricianswithCTisassociatedwith furtherdelayinreferral.13,14
Aftertheclinicalsuspicion(orconfirmation)of craniosyn-ostosis,thechildrenshouldbereferredtoamultidisciplinary team specialized in craniofacial anomalies (anesthesiol-ogist, plastic surgeon, speech therapist, neurosurgeon, orthodontist, otorhinolaryngologist,andpsychologist).15 In
thesecenters,theradiologicalexamofchoiceisthe three-dimensionalCTscanthatcontributestoelucidationofthe extensionofsuturefusionandtheconsequentcraniofacial deformityandsubsequentsurgicalplanning.Itis notewor-thythatthecephalicperimetergenerallydoes notchange duetocompensatorygrowthofotherbonesinthemajority ofcaseswithsimplecraniosynostosis.
ofchildrenwithcomplexcraniosynostosisand20%of carri-ersofsimplecraniosynostosis;cognitiveanddevelopmental disorders,poorweightgain,visual, hearing,andlanguage disorders; and psychological problems such as low self-esteem and social isolation. Therefore, the objective of surgicaltreatmentistopreventICHandtocorrect cranio-facialabnormalities.Overall,theoptimaltimingofsurgical correctioninmostcasesisbetween6and9monthsofage. The motivations for performingthe surgerybefore 1year ofageincludetheabilityofthechildyoungerthan1year tocompletelyreossify,themalleablecharacterofthe cal-variaduringthisage,andthetremendousbraingrowththat occursduringthefirstyear,whichallowsgoodremodelingof theskull.19Satisfactorycraniofacialformandesthetic
pleas-ing outcomeshave alsobeen associatedwith craniofacial surgicalinterventionsperformedbefore1yearof age.18,19
ItisnoteworthythatthepresenceofICHsigns(irritability, swellingofthepapilla,bulgingfontanelle,andimaging find-ings)mayresultintheneedforearliersurgicalintervention, toperformdecompression proceduresor ventricularshunt surgeryifassociatedwithhydrocephalus.
Sagittalsynostosis
It is the most common form of simple craniosynostosis and accounts for 40---60% of cases, being more prevalent among males (75---85%). The skull has an elongated and narrowshape,similartoaboat,hencebeingcalled scapho-cephaly(Fig.1A).20Uponphysicalexamination,aridgecan
bepalpatedonthesagittalsuture.Itshouldbenotedthat the anteriorfontanelle maynot beclosed. Compensatory frontalbossingandoccipitalprotrusionmayoccurinvarying degrees.
Surgicaltreatmentisindicatedbetween3and12months ofage,andproceduresmayvaryfromasimpleendoscopic resection of thesagittal suture tototal reconstructionof the skull, depending on the severity of the clinical pre-sentation.Inourservice,we recommendsurgerybetween 6 and 9 months of age and use the craniectomy in a ‘‘’’ fashion (named Hung Spun procedure),21 associated withseveralosteotomies(bonecuts)parallelrectanglesof approximatelytwocentimeters long in theparietal bone, between the coronaland lambdoidsutures, which permit greater lateral space for further accommodation of the brain.Barrelstaveosteotomies(lateralbonecuts)stillallow forreductionoftheanteriorposteriordiameterandbetter remodelingoftheskull,withexcellentestheticresults.22
Coronalsynostosis
It is the second most common form, accounting for up to25%of craniosynostosiscases.The closure ofa coronal sutureiscalledanteriorplagiocephaly,23,24whiletheclosure
of twosutures is termed brachycephaly(commonly found insyndromic craniosynostosis).6---8 Itpredominantly affects
females(60%),withsimilarincidenceonbothsides. Early fusion of the coronal suture leads to a flatten-ing of the frontal bone and the ipsilateral orbital rim to the fusion, with a compensatory contralateral frontal bossing.23,24 Strabismus is a common finding (50---60% of
cases) and is the result of morphological changes in the
orbitalroofandtrochlea,alteringthefunctionofthe supe-riorobliquemuscle.25 Elevationoftheipsilateralsphenoid
wingcanbeseeninsimpleskullradiographyandis recog-nizedasthe‘‘harlequinorbit’’(Fig.1B).26Prematurefusion
ofthe coronal suture alsocauses a deviation of the skull base, changing the position of the orbits, asymmetry of theeyebrows,asymmetryoftheearposition,deviationof themandible,andchangeof occlusion,withanimportant estheticeffect.23,24
Therefore,surgicaltreatmentisindicatedforcorrection ofthemorphological skulldeformity anditsrepercussions onthe face, but also because of strabismus and risks of developingICH.We recommendthe procedure between6 and9monthsofage,whenthereisalreadysufficientbone maturityforremodeling.Basically,afront-orbital advance-mentassociatedwithfrontalremodelingisperformedand releasingbothcoronalsutures.24 Furtherproceduresmight
benecessaryasfatinjectioninthecraniofacialskeletonto decreasefacialasymmetriesandcorrection ofeyelid pto-sis. At the end of facial growth orthognatic surgery and rhinoplastywithseptoplastymaybeperformedbyaplastic surgeonwithacraniofacialtraining.
Metopicsynostosis
Correspondsto10%ofallcraniosynostosisandpredominates in males (75---85% of cases). Early fusion of the metopic suture restricts the transversal growth of frontal bones, and in more severe cases can restrict the expansion of the anterior fossa, which leads to hypoteleorbitism, and consequently totrigonocephaly (Fig. 1C). Metopic cranio-synostosis is the single suture synostosis most frequently associatedwithmorecognitivedisorders,primarily dueto thegrowthrestrictionofthefrontallobes.27
The increase in the anterior fossa volume is the main objectiveinthetreatmentofpatientswithtrigonocephaly, aswell asfrontal remodeling andfronto-orbital advance-ment. The best time for treatment is between 6 and 9 monthsofage.
Lamboidsynostosis
Thisis therarestformof simplecraniosynostosis,withan incidenceofabout 0.3per10,000 livebirths, correspond-ingtoapproximately1.0---5.5%ofallcraniosynostosis.When evaluatedinapopulationofchildrenwithoccipital flatten-ing(alsocalledposteriorplagiocephaly),itisresponsiblefor only0.9---4.0%ofthecases.28
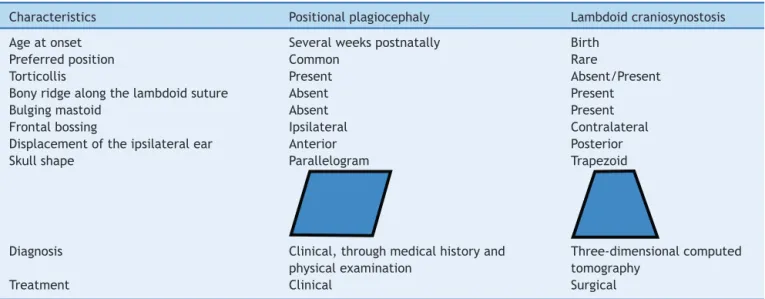
Table 4 Important characteristics to subsidize the differential diagnosis of positional plagiocephaly versus lamboid
synostosis21,24,25
Characteristics Positionalplagiocephaly Lambdoidcraniosynostosis
Ageatonset Severalweekspostnatally Birth
Preferredposition Common Rare
Torticollis Present Absent/Present
Bonyridgealongthelambdoidsuture Absent Present
Bulgingmastoid Absent Present
Frontalbossing Ipsilateral Contralateral
Displacementoftheipsilateralear Anterior Posterior
Skullshape Parallelogram Trapezoid
Diagnosis Clinical,throughmedicalhistoryand
physicalexamination
Three-dimensionalcomputed
tomography
Treatment Clinical Surgical
3D,three-dimensional;CT,computedtomography.
Surgicaltreatmentisbasedonvolumeexpansionofthe posteriorportionoftheskull(parietalandoccipitalregion) andreleasingthelambdoidsutures.However,thisregionhas large venous drainage, with innumerable scalp veinsthat crossthebonetowardtheduralsinuses,greatlyincreasing thesurgical risk ofa craniotomyandbone remodeling.In ourservice, we choose a posterior distractiontechnique, inwhich thecranial volumeisgraduallyincreased, signif-icantly reducing the risk of bleeding and need for blood transfusions.30
Positionalplagiocephaly
Thetermplagiocephalymeansobliqueskullandcorresponds toa unilateralor bilateraloccipital flattening,whichmay ariseduetothecontinualinfluenceofexternalforcesonthe immature skull (nonsynostotic posterior plagiocephaly) or becauseofprematurefusionofoneorbothlambdoidsutures (synostoticposteriorplagiocephaly).Anteriorplagiocephaly canbeusedtodefinethecranialdeformationcharacterized byprematureunilateralfusionofthecoronalsuture.
Positional or deformational plagiocephaly is the most common cause of plagiocephaly (prevalence of 5---48% in healthy newborn infants)31 versus an incidence of 0.003%
ofsynostoticplagiocephaly(lamboidsynostosis).28
Based onthe introduction of the campaign to prevent Sudden InfantDeath Syndrome (‘‘Back toSleep’’), in the beginningofthe 1990s--- whichrecommendedthat babies remain in the supine position --- a significant increase in theincidenceofchildrenwithpositionalplagiocephalywas noticed(5---48%).31 This deformityresults froman ongoing
actionofgravitationalforcesontheoccipitalregion, caus-ingaflattenedregionoftheposteriorcraniofacialskeleton. Ifnointerventionisperformed,thedeformitycancontinue and,insevere cases,evolve withfacialdeformities. Posi-tional plagiocephaly occurs more often on the right side (70% of cases) and affects more males. The major risk
factorsinclude:torticollis,prematurity,multiparity,anda fixedsleepingposition.
Diagnosis is eminently clinical, and the differentiation withsynostoticplagiocephaly(unilateralfusionofthe lamb-doid or coronal sutures) is essential.28 Anamnesis and
physical examination are sufficient to establish the dif-ferential diagnosis between a positional deformity and craniosynostosis in the vast majority of cases (Table 4). Classically,patientswithprematurefusionofthelambdoid suture already have the deformity at birth, while those withapositionaldeformityhaveanormalskullatbirthand developthedeformityinthesubsequentweeksormonths. When asked, parents may mention that there is a pre-ferred position of the baby’s positioning in patients with positional plagiocephaly,while in patients withsynostotic plagiocephaly,thereisnopreferredposition.
Pediatriciansshouldperformaphysicalexaminationwith theaidoftheparents;initially,thepatientremainsonthe mother/father’slapfacingthepediatricianandafterfacing theparents;finally,theexaminershouldobservethechild fromasuperiorview.Duringthephysicalexamination, sym-metries between the skull, forehead, and ears should be carefullyanalyzed.
Positionalplagiocephalypresentsaformatofa parallelo-gramskull,whilesynostoticposteriorplagiocephalyhasthe shape of a trapezoid.32 Still, an ipsilateralbulging in the
Figure2 Representationofpositionalplagiocephalyandtrue(synostotic)posteriorplagiocephaly.(A)Positionalplagiocephaly
showing:absenceoflambdoidsuturestenosis,formatofaparallelogramskull,ipsilateralcompensatoryfrontalbossing,ipsilateral
earinananteriorposition,asifithadbeenpushed.(B)Trueposteriorplagiocephalyshowing:presenceoflambdoidsuturestenosis,
shapeofatrapezoid,ipsilateralbulginginthemastoidregion,contralateralcompensatoryfrontalbossing,ipsilateralearstenosis
tendstobeinaposteriorpositionanddownwards,asifthesuturepulledit.Credits:PatrickBraga.
congenital torticollis and/or thickeningof the sternoclei-domastoidmuscle,whicharedirectlyrelatedtopositional plagiocephaly.
Thediagnosisandtreatmentofpositionalplagiocephaly areclinical.32 Someguidanceshouldbegiventoparentsat
thefirst childcareconsultation,howtoavoid badposture positionsforsleepingoronthechangingtable,tonotethe presenceoftorticollis,tospendaslittletimeaspossiblein the‘‘babycomfort’’,andtoencouragethatthebabystay for a longertime in theventral decubitus position,while undersupervision.Itisimportanttodiagnoseanycervical restriction(e.g.,congenitaltorticollisorthickeningofthe sternocleidomastoid muscle) andguide parents about the needofearlyphysiotherapytreatment.
Inadditiontotheguidelines,therapeuticmeasures can beemployed,suchashowtoforcethebabytosleeponthe contralateral side of the deformity, toencourage moving thelocationofthecribandchangingtable,inordertoforce thebabytoturnhisheadtothesideheison,besides stim-ulatingthe babytosit.Such measures areeffective until 4---6monthsastreatmentofpositionalplagiocephaly.32,33
Theprevalenceofpositionaldeformitytendstodecrease withageandmaybeaslowas3.3%at2yearsofage,which highlightsthenaturalabilityofskullremodeling.32However,
after 6 months of age, the use of a specific helmet may beindicated in patients withsevere deformitiestoaid in remodelingtheskull.Itshouldbeemphasizedthatthe hel-metrequires at least 23h of use per day tobeeffective,
which may result in pressure sores and local abrasions, besidesthe highcostof theappliance andbothersome to thechild.34
Conclusions
Cranial deformities are common complaints and highly prevalentintheroutineofpediatricians.Althoughthevast majority of children present positional deformities, early diagnosisofcraniosynostosisandreferringthemto special-izedtreatment in a timely manner is criticalto optimize surgicaloutcomes.Thediagnosisofpositionaldeformitiesis usuallyclinical,andtreatmentconsistsofsimpleguidelines and measures to prevent worsening the condition. When thereisadiagnosisofcraniosynostosis,amultidisciplinary approachofthechildwithcraniosynostosisiscrucialfora greatersurgicalsuccessrateandtominimizecomplications.
Funding
Thisstudydidnotreceivefunding.
Conflicts
of
interest
References
1.Peitsch WK, Keefer CH, LaBrie RA, Mulliken JB. Incidence of cranialasymmetryin healthynewborns. Pediatrics. 2002; 110:e72.
2.PearceMS,SalottiJA,LittleMP,McHughK,LeeC,KimKP,etal. RadiationexposurefromCTscansinchildhoodandsubsequent risk ofleukaemia and braintumours: a retrospective cohort study.Lancet.2012;380:499---505.
3.FuruyaY,EdwardsMS,AlpersCE,TressBM,OusterhoutDK, Nor-manD.Computerizedtomographyofcranialsutures. Part1: comparisonofsutureanatomyinchildrenandadults.J Neuro-surg.1984;61:53---8.
4.Slater BJ, Lenton KA, Kwan MD, Gupta DM, Wan DC, Lon-gakerMT.Cranialsutures:abriefreview.PlastReconstrSurg. 2008;121:170e---8e.
5.Aviv RI, Rodger E, Hall CM. Craniosynostosis. Clin Radiol. 2002;57:93---102.
6.Raposo-Amaral CE, Neto JG, Denadai R, Raposo-AmaralCM, Raposo-AmaralCA.Patient-reportedqualityoflifein highest-functioningApertandCrouzonsyndromes:acomparativestudy. PlastReconstrSurg.2014;133:182e---91e.
7.GhizoniE,Raposo-AmaralCA,MathiasR,DenadaiR, Raposo-AmaralCE.Superiorsagittalsinus thrombosisasa treatment complication of nonsyndromic Kleeblattschädel. J Craniofac Surg.2013;24:2030---3.
8.Raposo-AmaralCE,TongA,DenadaiR,YalomA,Raposo-Amaral CA,BertolaD,etal.AsubcranialLeFortIIIadvancementwith distractionosteogenesisasaclinicalstrategytoapproach pycn-odysostosiswithmidfaceretrusionandexorbitism.JCraniofac Surg.2013;24:1327---30.
9.Heuzé Y, Holmes G, PeterI, Richtsmeier JT, Jabs EW. Clos-ingthegap:geneticandgenomiccontinuumfromsyndromic tononsyndromiccraniosynostoses.CurrGenetMedRep.2014; 2:135---45.
10.Johnson D, Wilkie AO. Craniosynostosis. Eur J Hum Genet. 2011;19:369---76.
11.Passos-Bueno MR, Serti Eacute AE, Jehee FS, Fanganiello R, YehE.Geneticsofcraniosynostosis:genes,syndromes, muta-tions and genotype-phenotype correlations. Front Oral Biol. 2008;12:107---43.
12.Bredero-BoelhouwerH,TreharneLJ,MathijssenIM.Atriage sys-temforreferralsofpediatricskulldeformities.JCraniofacSurg. 2009;20:242---5.
13.MedinaLS, RichardsonRR, CroneK. Childrenwithsuspected craniosynostosis: a cost-effectiveness analysis of diagnostic strategies.AJRAmJRoentgenol.2002;179:215---21.
14.MathijssenIM. Guideline for care ofpatients withthe diag-noses ofcraniosynostosis:workinggroup oncraniosynostosis. JCraniofacSurg.2015;26:1735---807.
15.Tamburrini G, Caldarelli M, Massimi L, Santini P, Di Rocco C. Intracranial pressure monitoring in children with single sutureandcomplexcraniosynostosis:areview.ChildsNervSyst. 2005;21:913---21.
16.StarrJR,CollettBR,GaitherR,Kapp-SimonKA,CradockMM, CunninghamML,etal.Multicenterstudyofneurodevelopment in3-year-oldchildrenwithandwithoutsingle-suture craniosyn-ostosis.ArchPediatrAdolescMed.2012;166:536---42.
17.PhillipsJ,WhitakerLA.Thesocialeffectsofcraniofacial defor-mityanditscorrection.CleftPalateJ.1979;16:7---15.
18.WarrenSM, ProctorMR, BartlettSP, Blount JP, Buchman SR, BurnettW,etal.Parametersofcareforcraniosynostosis: cra-niofacialand neurologic surgeryperspectives.Plast Reconstr Surg.2012;129:731---7.
19.Persing JA. MOC-PS(SM) CME article: management consider-ationsinthetreatmentofcraniosynostosis.PlastReconstrSurg. 2008;121Suppl.4:1---11.
20.MassimiL,CaldarelliM,TamburriniG,PaternosterG,DiRocco C.Isolatedsagittalcraniosynostosis:definition,classification, andsurgicalindications.ChildsNervSyst.2012;28:1311---7. 21.McCarthy JG, Bradley JP, Stelnicki EJ, Stokes T, Weiner
HL. Hung span method of scaphocephaly reconstruction in patients with elevated intracranial pressure. Plast Reconstr Surg.2002;109:2009---18.
22.Raposo-AmaralCE,DenadaiR,TakataJP,GhizoniE,BuzzoCL, Raposo-AmaralCA.Progressivefrontalmorphologychanges dur-ingthefirstyearofamodifiedPiprocedureforscaphocephaly. ChildsNervSyst.2016;32:337---44.
23.Raposo-do-AmaralCE,SilvaMP,MenonDN,SomensiRS, Raposo-do-AmaralCA,BuzzoCL.Estudoantropométricodasassimetrias craniofaciaisnacraniossinostosecoronalunilateral.RevBrasCir Plast.2011;26:27---31.
24.Raposo-AmaralCE,Denadai R,Ghizoni E,Buzzo CL, Raposo-AmaralCA.Facialchangesafterearlytreatmentofunilateral coronal synostosis question the necessity of primary nasal osteotomy.JCraniofacSurg.2015;26:141---6.
25.Raposo-do-AmaralCE,Raposo-do-AmaralCA,GuidiMC,Buzzo CL.Prevalênciadoestrabismonacraniossinostosecoronal uni-lateral.Hábenefíciocomacirurgiacraniofacial?RevBrasCir Craniomaxilofac.2010;13:73---7.
26.DiRocco C,PaternosterG, CaldarelliM,Massimi L, Tambur-riniG.Anteriorplagiocephaly:epidemiology,clinicalfindings, diagnosis, and classification. A review. Childs Nerv Syst. 2012;28:1413---22.
27.Van der Meulen J. Metopic synostosis. Childs Nerv Syst. 2012;28:1359---67.
28.MatushitaH,AlonsoN,CardealDD,AndradeFG.Majorclinical featuresofsynostoticoccipitalplagiocephaly:mechanismsof cranialdeformations.ChildsNervSyst.2014;30:1217---24. 29.TamburriniG,CaldarelliM,MassimiL,GaspariniG,PeloS,Di
RoccoC.Complexcraniosynostoses:areviewoftheprominent clinicalfeaturesandtherelatedmanagementstrategies.Childs NervSyst.2012;28:1511---23.
30.NowinskiD,DiRoccoF,RenierD,SainteRoseC,LeikolaJ,Arnaud E.Posteriorcranialvaultexpansioninthetreatmentof cranio-synostosis.Comparisonofcurrenttechniques.ChildsNervSyst. 2012;28:1537---44.
31.LoseeJE, MasonAC.Deformational plagiocephaly:diagnosis, prevention,andtreatment.ClinPlastSurg.2005;32:53---64. 32.PoglianiL,MameliC,FabianoV,ZuccottiGV.Positional
plagio-cephaly:whatthepediatricianneedstoknow.Areview.Childs NervSyst.2011;27:1867---76.
33.LaughlinJ,LuerssenTG,DiasMS,theCommitteeonPractice and Ambulatory Medicine, Section on Neurological Surgery. Preventionandmanagementofpositionalskulldeformitiesin infants.Pediatrics.2011;128:1236---41.