www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Setting
of
an
endoscopic
nasal
reference
point
for
surgical
access
to
the
anterior
base
through
an
anatomical
study
on
cadavers
夽
Andressa
Vinha
Zanuncio
a,∗,
Paulo
Fernando
Tormin
Borges
Crosara
b,
Helena
Maria
Gonc
¸alves
Becker
b,
Celso
Gonc
¸alves
Becker
b,
Roberto
Eustáquio
dos
Santos
Guimarães
b,∗aUniversidadeFederaldeSãoJoãodel-Rei(UFSJ),CampusCentro-Oeste,Divinópolis,MG,Brazil
bUniversidadeFederaldeMinasGerais(UFMG),FaculdadedeMedicina,DepartamentodeOftalmologiaeOtorrinolaringologia,
BeloHorizonte,MG,Brazil
Received27March2015;accepted29October2015 Availableonline6May2016
KEYWORDS Skullbase;
Endoscopicsurgery; FESS;
Paranasalsinuses; Facialsinuses
Abstract
Introduction:Diseases of paranasalsinuses,nasal cavity, and skull base canbe treated by endonasal operations using anasal rigid endoscope. Whenconducting this kind ofsurgery, anatomicalreferencesarecriticalforsafety.
Objective:Tomeasurethedistancefromtheposteriorwallofthemaxillarysinustotheskull base,accordingtosocio-demographiccharacteristics,andtodetailananatomicalreference pointfor paranasalsinusoperationsandforanaccess totheanteriorskullbase, comparing anatomicalvariationsbetweenrightandleftsides,gender,height,weight,age,andethnicity incadavers.
Methods:Measuresweretakenfromthe90◦angle(thestartingpointwheredeflectionofthe skullbasebeginstoformtheanteriorwallofthesphenoid,alsoknownas90◦)totheupper, middle,andlowerpointsoftheposteriorwallofthemaxillarysinus.Thisstudyused60cadavers agedover17years,andevaluatedthesebodieswithrespecttoage,height,BMI,weight,gender, andethnicity,comparingmeasurementsofrightandleftsides.
Results:Themeasurementswere>1.5cminall cadaversanddidnotvarywithage,height, weight,gender,andethnicityontheirrightandleftsides.Thelackofassociationbetweenthe measurementfrom90◦totheupper,middle,andlowerposteriorwallsofthemaxillarysinus (categoricalorquantitative)isnoteworthy,consideringthecharacteristicsstudied.
夽 Pleasecitethisarticleas:ZanuncioAV,CrosaraPF,BeckerHM,BeckerCG,GuimarãesRE.Settingofanendoscopicnasalreferencepoint
forsurgicalaccesstotheanteriorbasethroughananatomicalstudyoncadavers.BrazJOtorhinolaryngol.2016;82:630---5.
∗Correspondingauthors.
E-mails:[email protected](A.V.Zanuncio);[email protected](R.E.Guimarães).
http://dx.doi.org/10.1016/j.bjorl.2015.10.021
Conclusion: Themethodologydefinedthenasalpointofreference,consideringanabsenceof variationinthecadavers’characteristics.
© 2016 Publishedby Elsevier Editora Ltda. onbehalf of Associac¸˜ao Brasileira de Otorrino-laringologiaeCirurgiaC´ervico-Facial.ThisisanopenaccessarticleundertheCCBYlicense (http://creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE Basedocrânio; Cirurgias endoscópicas; FESS;
Seiosparanasais; Seiosdaface
Definic¸ãodopontodereferênciaendoscópicanasalaoacessocirúrgicoàbase anteriorporestudoanatômicoemcadáveres
Resumo
Introduc¸ão: Doenc¸as dos seios paranasais, cavidades nasais e doenc¸as da base do crânio podemsertratadascomoperac¸ãoendonasalutilizando-seendoscópiorígidonasal.Referências anatômicassãoimportantesparaaseguranc¸adurantearealizac¸ãodessasoperac¸ões.
Objetivo: Mediradistânciadaparedeposteriordoseiomaxilaràbaseanteriordocrâniode acordocomcaracterísticas sócio-demográficas.Detalharum pontode referênciaanatômico paraoperac¸õesdosseiosparanasaiseacessoàbaseanteriordocrâniocomparandovariac¸ões anatômicasentreosladosdireitoeesquerdo,gênero,altura,peso,idadeeetniaemcadáveres.
Método: Medidasdoângulode90◦(pontoondeiniciaadeflexãodabasedocrânioparaformar aparedeanteriordoesfenoide,chamadodeângulode90◦
90◦)aospontossuperior,médio einferiordaparedeposteriordoseiomaxilar.Foramutilizados60cadáverescomidadeacima de17anos,eavaliadoscomidade,altura,pesoIMC,gêneroeetnia,comparando-seasmedidas dosladosdireitoeesquerdo.
Resultados: Asmedidasforammaioresque1,5cmemtodososcadáveresenãovariaramcom aidade,altura,peso,gêneroeetnianosladosdireitoeesquerdodoscadáveres.Destaca-se faltadeassociac¸ãoentreamedidado90◦ àparedeposteriorsuperior;médiaeinferiordo maxilar(categóricoouquantitativo)comascaracterísticasestudadas.
Conclusão:Ametodologiaempregadadefiniuopontodereferêncianasalpornãovariarcom ascaracterísticasdoscadáveres.
© 2016Publicadopor ElsevierEditora Ltda.em nomede Associac¸˜ao Brasileira de Otorrino-laringologia eCirurgiaC´ervico-Facial.Este ´eumartigo Open Accesssob umalicenc¸a CCBY (http://creativecommons.org/licenses/by/4.0/).
Introduction
Endonasalsurgeryguidedbyanasalrigidendoscope(called
endoscopicsinussurgery)isusedfor thetreatment of
dis-eases of paranasal sinuses, nasal cavities, and skull base
diseases.Thus,onemusthaveadetailedknowledgeofnasal
anatomy;aCTscanoffacialsinusesandanasolaryngoscopy
studyareindispensableforthisprocedure.Theanatomyof
thesinusesvariesindividually.1---3
Functional endoscopic sinus surgery is used to treat
chronic rhinosinusitis with or without nasal polyps, for
resection of nasal and paranasal sinus tumors, in
malfor-mations of the nasal cavity such as choanal atresia, in
variousinflammatoryand infectiousdiseases ofnasal
cav-ityandparanasalsinuses, andinskullbase diseases,with
less morbidity/complications. Skullbase surgeryand
revi-sionprocedureswithdistortedanatomyaretheprocedures
mostinneedofpreciseanatomicalreferences.4---6
Knowledge of fixed measures (with slight variation in
characteristics suchasgender, ethnicity,age,weight,and
height)suchasthedistance fromtheposteriorwallofthe
maxillary sinus to 90◦ (starting point where the
deflec-tion of the skull base begins, to form the anterior wall
ofthe sphenoid)in theanteriorskullbase,wouldprovide
greatersafetytosurgeons.Withsuchknowledge,iatrogenic
complicationstotheposteriorsinusescouldbeminimized.
Thesemeasureshavenotbeendescribedintheliterature,
andwillbepresentedinthisarticle.7---9
Theaimofthisstudywastomeasuredistancesfromthree
pointsoftheright-andleft-sideposteriorwallofthe
max-illarysinusestotheanteriorskullbase(90◦)andcompare
them with the sociodemographic characteristics of
inter-est;set other benchmarksfor endoscopic surgical access;
comparetheanatomicalvariationsofthereferencepoints
measured in relation togender, height, weight,age, and
ethnicityoncadavers;andtodetailanewanatomical
ref-erencepointtoperformsurgeriesof theparanasalsinuses
andanteriorskullbaseinasaferenvironment.
Methods
ThisstudywasapprovedbytheResearchEthicsCommittee
oftheinstitutionunderprotocolNo.0591.0.203.000-8.
The nasalcavities(right andleft)weredissected in60
cadavers,allagedover17years,ofvaryingage,ethnicity,
height,andgender.The medialwallofthemaxillarysinus
wasopened,andanteriorandposteriorethmoidsinusesand
Middle meatus
LT
Uncinate process
LT
Ethmoid bulla MT
MT
MT Septum Septum
Septum
A
B
C
LT
Ethmoid bulla
Maxillary sinus
Ethmoid
Maxillary sinus
Maxillary sinus MT
MT
Sphenoid
Septum
Septum
MT
Septum
D
E
F
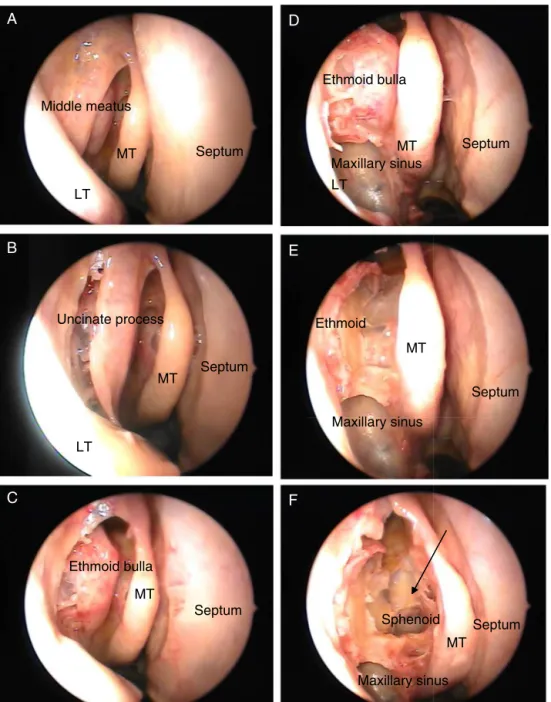
Figure1 Right nasalcavity(MT,middleturbinate;LT,lowerturbinate).(A)Thebeginningofdissection;(B)uncinateprocess; (C)ethmoidbulla;(D)maxillarysinusexposure;(E)ethmoidsinusexposure;(F)sphenoidsinusexposure.Thearrowindicatesthe 90◦.
identify the point where the deflection of the skull base
begins,to formthe anteriorwall of thesphenoid, known
90◦(Fig.1),andtomeasurethedistancefromthatpoint
totheupper,middle,andlowerpointsoftheposteriorwall
ofthemaxillarysinuses.
Thedissectionwasperformed withmicrosurgical
mate-rial through nasal endoscopy with zero-degree optics
coupledwithacamera,withDVDrecording.
The framework for this study was established in the
autopsy room with a video camera, a notebook, a nasal
aspirator,alightsource,surgicalinstruments,zero-degree
optics,and fiber opticlight cable. After the autopsy,the
cadaversunderwentparanasalsinusdissection,andatthis
momentthemeasuresweretaken.
The following measurementswere performed (Fig. 2):
upper,middle,andlowerpartsoftheposteriorwallofthe
maxillarysinus tothe angle of90◦, basedona previously
stipulatedprotocol.
Covariatesheight,weight,age,bodymassindex(BMI),
gender,andethnicitywereassessedinrelationtothethree
measuresstudied.
The descriptive results presented in the Results
sec-tion were obtained through the use of frequencies and
percentages for the characteristics of the various
cate-gorical variables, and from the performance of central
tendency measures (mean and median) and dispersion
measures (standard deviation) for the quantitative
Table1 Descriptivestatisticsofthefeaturesofthemeasurementofthedistancefrom90◦ tothesuperior(SPW),middle (MPW),andlower(LPW)posteriorwallofmaxillarysinusesofthestudiedcadaversonboth(rightandleft)sides.
Features n Mean SD Min 1Q Med 3Q Max
Rightside
90◦(SPW) 60 2.1 0.3 1.5 2.0 2.0 2.5 3.0
90◦(MPW) 60 1.9 0.5 1.0 1.5 2.0 2.0 3.0
90◦(LPW) 60 1.7 0.5 0.5 1.5 1.5 2.0 2.5
Leftside
90◦(SPW) 60 2.2 0.4 1.5 2.0 2.0 2.5 3.0
90◦(MPW) 60 1.7 0.4 1.0 1.5 2.0 2.0 2.5
90◦(LPW) 60 1.6 0.4 0.5 1.5 1.5 2.0 2.5
n,numberofobservations;SD,standarddeviation;Min,minimum;1Q,1stquartile;Med,median;3Q,3rdquartile;Max,maximum.
Maxillary sinus: posterior wall Sphenoid ∆90º
Measurement performed
Figure2 Performanceofmeasuresonthecadaversstudied
90◦ (thestartingpointwherethedeflectionoftheskullbase beginstoformtheanteriorwallofthesphenoid).
ThePearsoncorrelationcoefficient(r)wasusedto com-parethemeasurementsandcharacteristicsinquantitative forms(age,height,weight,andBMI).
Student’st-testwasusedforcomparisonsofmeasuresin quantitativeformwithgenderandethnicity,sincetheusual assumptionsofthistestweremet(normality---Shapiro---Wilk testandhomoscedasticity---Levene).10
Thethreeselectedmeasuresweredichotomizedintotwo
groups:≥2and<2,consideringthat,insurgicalpracticeit
wasobservedthatgenerallythedistanceswere≥2.
Results
Descriptiveanalysis
Therewasaprevalenceofmale(55%)andwhite(78.3%)
indi-viduals.Meanage,height,weight,andBMIofthecadavers
was64years;1.70m;67.1kg,and22.5,respectively.There
wasaprevalenceofcadaversagedbetween48and88years
old,withheightbetween1.70and1.75m,weightbetween
60and80kg,andBMIbetween18and26.
Table 2 Categorized description ofthemeasurement of thedistancefrom90◦totheupper,middle,andlower pos-teriorwallsofthemaxillarysinusofthestudiedcadaverson both(rightandleft)sides.
Frequency
Rightside Leftside
Features n % n %
90upper
<2 5 8.3 5 8.3
≥2 55 91.7 55 91.7
90middle
<2 23 38.3 29 48.3
≥2 37 61.7 31 51.7
90lower
<2 32 53.3 35 58.3
≥2 28 46.7 25 41.7
n,numberofobservations.
Descriptivestatisticsbetweenrightandleftsides
Thecadavershadthefollowingmeasuresontheirrightside: a mean of 2.1cm from90◦ tothe upper posterior wall ofthemaxillarysinus;ameanof1.9cmfrom90◦ tothe middleposteriorwallofthemaxillarysinus;andameanof 1.7cmfrom90◦tothelowerposteriorwallofthemaxillary sinus.Ontheleftside,thesemeasureswere2.2cm,1.7cm, and1.6cm,respectively(Table1).
The measurefrom90◦ totheupper posterior wallof
themaxillarysinuswas≥2cmonbothsidesin91.7%ofthe
studiedcadavers.Whenmeasuringthedifference(byside)
between the distance from90◦ tothe middle posterior
wallofthe maxillarysinus andthe distancefrom90◦ to
thelowerposteriorwallofthemaxillarysinus,itwasfound
thatin61.7%ofthestudiedcadaversontherightsideand
in 51.7% onthe leftside, the distance from90◦ tothe
middleposteriorwallofthemaxillarysinuswas≥2cm.
Fur-thermore, the distance from 90◦ tothe lower posterior
wallofthemaxillarysinuswas≥2cmin46.7%andin41.7%
Table3 Comparisonofthemeasurementofthedistancefrom90◦ totheupper,middle,andlowerposteriorwallsofthe maxillarysinusofthestudiedcadaversbyside(rightandleft).
Side
Right Left
Features Mean SD Med Mean SD Med p-Value
90◦upper 2.1 0.3 2.0 2.2 0.4 2.0 0.277a
90◦middle 1.9 0.5 2.0 1.7 0.4 2.0 0.020a
90◦lower 1.7 0.5 1.5 1.6 0.4 1.5 0.4172
SD,standarddeviation;Med,median.
aPairedt-test.
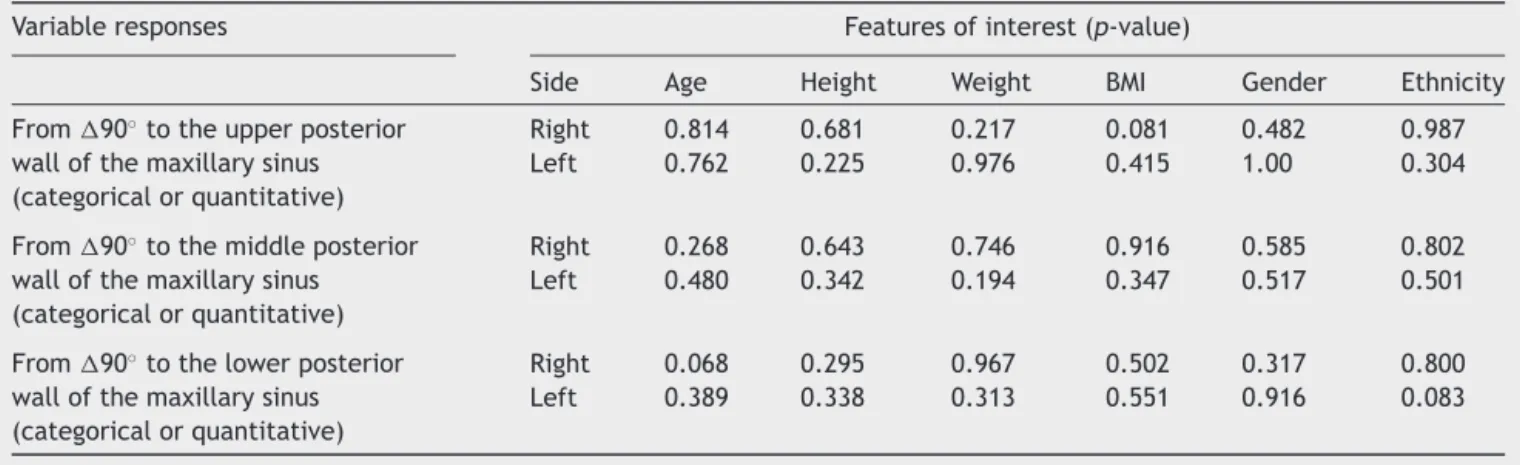
Table4 Summaryofcomparisonsamongthethreeevaluatedmeasuresandfeaturesofinterest.
Variableresponses Featuresofinterest(p-value)
Side Age Height Weight BMI Gender Ethnicity
From90◦totheupperposterior wallofthemaxillarysinus (categoricalorquantitative)
Right 0.814 0.681 0.217 0.081 0.482 0.987
Left 0.762 0.225 0.976 0.415 1.00 0.304
From90◦tothemiddleposterior wallofthemaxillarysinus (categoricalorquantitative)
Right 0.268 0.643 0.746 0.916 0.585 0.802
Left 0.480 0.342 0.194 0.347 0.517 0.501
From90◦tothelowerposterior wallofthemaxillarysinus (categoricalorquantitative)
Right 0.068 0.295 0.967 0.502 0.317 0.800
Left 0.389 0.338 0.313 0.551 0.916 0.083
Inten(16.7%)of the60studiedcadavers,themeasure from90◦totheupperposteriorwallofthemaxillarysinus was<2cmand>1.5cm.
Comparisonsbetweensides
Themeasurefrom90◦tothemiddleposteriorwallofthe maxillarysinus showeda variationbetween sides, witha lowervalueontheleftversusrightside,withadifference of0.2(1.9---1.7)cmforthisfeature,withastatistically sig-nificantdifference.Nodifferencewasobservedintheother twomeasures(Table3).
Comparisonsoffeatureswithvariableresponsesby side
Rightandleftsides---quantitative
The coefficient and p-values of Pearson’s correlation (r)
showednoassociationbetweenmeasuresfrom90◦ tothe
upper, middle, and lower posterior wall of right and left
maxillarysinusesandage,height,weight,BMI,gender,and
ethnicityofthecadavers(p>0.05)(Table4).
Rightandleftsides---categorical
The measure from 90◦ tothe upper, middle, andlower
posterior wall of right and left maxillarysinuses wasnot
associatedwithage,height,weight,BMI,race,andgender
ofthecadavers(p>0.05).
Discussion
This research wasdeveloped after an observation, during
approximatelytenyearsofnasalendoscopicsurgeries,that
the anatomical measures discussed were constant.
Meas-uresfrom90◦ totheposteriorwallofthemaxillarysinus
were similar,regardlessof gender, ethnicity, age,weight,
or height; but other measures variedwith such features.
Observations in surgical practice led the authors to
per-formtheseanatomicalmeasurementsoncadavers,seeking
evidence in favor or against these observations, because
themedicalliteraturedoes notprovidedefinitionsonthis
topic. The corroboration of the regularity of the
meas-ures would allow the attainment of a more precise and
constant anatomicalreference,probably implying greater
safetyintheapproachtoposteriorparanasalsinuses,chiefly
by the fact that this area shows a great anatomic
varia-tion.In caseswhere thereis a distortionof the anatomy,
asin reoperations,this measurebecomesevenmore
use-ful.
Othermeasurestakeninthenasalcavitiesof60
cadav-ers have shown the influence of personal characteristics.
However,therewas nochange in thedistance from 90◦
totheupperposteriorwallofthemaxillarysinus,providing
evidenceinfavorofwhatwasalreadyseenin thisclinical
practice. It wasobserved that 10% of the measures from
90◦totheupperposteriorwallofthemaxillarysinuswere
<2cmand>1.5cm;thus,thefixedmeasurewaschangedto
In the measurement of the distance from90◦ to the
lowerandmiddleposteriorwallofthemaxillarysinus,itwas
foundthatmeasures<1.5cmwereoutliers.Thesemeasures
havelittleaccuracy,andarenotsuitabletobeobtained
dur-ingsurgerybecauseoftheiranatomicalpositioninrelation
to90◦.Thus,theperformanceofsuchmeasuresisnot
fea-sibleduringsurgicalprocedures.Therefore,itwasdecided
tousethe1.5-cmmeasurewithrespecttotheupperpoint
oftheposteriorwallofthemaxillarysinusto90◦,thanks
toitsviabilityandalsoduetotheabsenceofoutliervalues.
In surgicalcases inwhicha maxillarysinusapproachis
notused,otheranatomicalstructuresshouldbeused.
Conclusion
Theanalysisofthedatapresentedinthisstudy allowsfor
theconclusionthatthereisafixedmeasurementbetween
theupperposteriorwallofthemaxillarysinusand90◦.The
valuefoundwasalwaysgreaterthan1.5cm,whichcan
facil-itateasafeopeningoftheposteriorparanasalsinusesduring
nasalendoscopicsurgerieswithamaxillarysinusapproach.
Themeasurementsoflowerandmiddlepointswithrespect
tothe posterior wallof the maxillarysinus shouldnot be
usedinsurgicalpractice,becauseofmeasurement
difficul-tiesduetotheiranatomicalposition.
Bothcategoricallyandquantitatively,therewasno
statis-ticalassociationwithrespecttothedifferencebetweenthe
measurementsfrom90◦ totheupper,middle,andlower
posterior walls ofthe maxillarysinus in anyof the
evalu-atedcharacteristics.Thus,therewasnoimpactfromage,
weight,height,ethnicity,orgenderonthesemeasures.
The definition of a fixed measure in paranasal sinus
anatomyinanareawherethereisagreaterchanceof
occur-rence of iatrogenicerror could impart a senseof greater
safetytothesurgeonandfewercomplicationsinnasal
endo-scopicsurgery.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.KarasenM,KantarciIRM,AlperF,OnbasO,OkurA,KaramanA. Remarkableanatomic variationsinparanasalsinusregionand theirclinicalimportance.EurJRadiol.2004;50:296---302.
2.LuongA,MarpleBF.Sinussurgery:indicationsandtechniques. ClinRevAllergImmu.2006;30:217---22.
3.TanHKK.Sphenoidsinus:ananatomicandendoscopicstudyin Asiancadavers.ClinAnat.2007;20:745---50.
4.ScutariuMD,BâldeaV.Neighbouringrelationsoftheposterior ethmoid studiedbyaxial computedtomography. Morphology. 2010;94:51---7.
5.TanBK,LaneAP.Endoscopicsinussurgeryinthemanagement ofnasalobstruction.OtolaryngClinNAm.2009;42:227---40.
6.BunzenDL,Campos A, LeãoFS, Morais A, SperandioF,Neto SC. Eficácia da operac¸ão endoscópicanasal nos sintomasda rinossinusitecrônicaassociadaounãoàpolipose.BrazJ Otorhi-nolaryngol.2006;72:242---6.
7.StammA.Operac¸ãomicroendoscópicadosseiosparanasais ---conceitosbásicos.BrazJOtorhinolaryngol.2002;68:299---302.
8.Stamm AC,Pignatari S, Sebusiani BB, Galati MC, Mitsuda S, Haetinger RG. Operac¸ão endoscópicanasossinusal eda base do crânio guiada por computador. Braz J Otorhinolaryngol. 2002;68:502---9.
9.HemmerdingerSA,JacobsJB,LebowitzRA.Accuracyandcost analysisofimage-guided sinussurgery. OtolaryngClinNAm. 2005;38:453---60.