REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
REVIEW
ARTICLE
Perioperative
gabapentin
and
pregabalin
in
cardiac
surgery:
a
systematic
review
and
meta-analysis
Souvik
Maitra,
Dalim
K.
Baidya,
Sulagna
Bhattacharjee,
Anirban
Som
∗AllIndiaInstituteofMedicalSciences,DepartmentofAnaesthesiology&IntensiveCare,NewDelhi,India
Received26October2015;accepted20July2016 Availableonline1October2016
KEYWORDS Cardiacsurgery; Gabapentin; Pregabalin; Post-operativepain
Abstract
Objectives:Sternotomy forcardiacsurgeriescausessignificantpostoperativepainandwhen not properlymanaged may causesignificant morbidity. As neuropathic pain isa significant componenthere,gabapentinandpregabalinmaybeeffectiveinthesepatientsandmayreduce postoperativeopioidconsumption.Thepurposeofthissystematicreviewwastofindoutefficacy ofgabapentinandpregabalininacutepostoperativepainaftercardiacsurgery.
Methods:Published prospective human randomized clinical trials, which compared pre-operative and/or postoperative gabapentin/pregabalin with placebo or no treatment for postoperativepainmanagementaftercardiacsurgeryhasbeenincludedinthisreview.
Results:FourRCTseachforgabapentinandpregabalinhavebeenincludedinthissystematic review.Threegabapentinandtwopregabalinstudiesreporteddecreaseinopioidconsumption incardiacsurgicalpatientswhileonegabapentinandtwopregabalinstudiesdidnot. Three RCTseachforgabapentinandpregabalinreportedlowerpainscoresbothduringactivityand rest.Thedrugsarenotassociatedwithanysignificantcomplications.
Conclusion:Despitelowerpainscoresinthepostoperativeperiod,thereisinsufficientevidence torecommendroutineuseofgabapentinandpregabalintoreduceopioidconsumptioninthe cardiacsurgicalpatients.
©2016SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE Cirurgiacardíaca; Gabapentina; Pregabalina;
Dornopós-operatório
Gabapentinaepregabalinanoperíodoperioperatórioemcirurgiacardíaca:uma revisãosistemáticaemetanálise
Resumo
Objetivos: A esternotomia para cirurgias cardíacas causa dor intensa no pós-operatório e quandonão tratada adequadamente pode causarmorbidade grave.Comonesse caso ador neuropática éuma componente importante, gabapentinae pregabalinapodem ser eficazes
∗Correspondingauthor.
E-mail:[email protected](A.Som).
http://dx.doi.org/10.1016/j.bjane.2016.07.014
nessespacientesepodemreduziroconsumodeopioidesnopós-operatório.Oobjetivodesta revisãosistemáticafoiavaliaraeficáciadegabapentinaepregabalinanadoragudaapóscirurgia cardíaca.
Métodos: Estudos clínicos prospectivose randômicoscom humanos,quecompararam ouso de gabapentina/pregabalinanosperíodos pré-e/oupós-operatório complaceboounenhum tratamentoparaocontroledadornopós-operatóriodecirurgiacardíacaforamincluídosnesta revisão.
Resultados: Quatro ECRs de gabapentina e pregabalina foram incluídos nesta revisão sis-temática.Trêsestudosdegabapentinaedoisdepregabalinarelataramdiminuic¸ãodoconsumo de opioides em pacientescirúrgicoscardíacos; um estudode gabapentina edoisde prega-balinanãorelataram.TrêsECTsdegabapentinaepregabalinarelataramescoresmenoresde dor,duranteaatividadeeorepouso.Osmedicamentosnãoestãoassociadosacomplicac¸ões significativas.
Conclusão::Emboraosescoresdedortenhamsidomenoresnopós-operatório,nãohá evidên-ciassuficientespararecomendarousorotineirodegabapentinaepregabalinaparareduziro consumodeopioidesempacientescirúrgicoscardíacos.
©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigo OpenAccess sobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Sternotomyforcardiacsurgerycausessignificant postopera-tivepain,1 which hasboth significant shorttermandlong
term consequences. Poorly managed acute postoperative painmaycomplicateimmediatepostoperativeperiod2,3and
mayalsocausechronicpain.4Thoughpatientsusuallyfeel
worstpaininthefirstpostoperativeday,significantpainmay continue uptosixth postoperativeday.5 Adequately
man-agedacutepainlowersthemyocardialoxygendemandand decreasestheincidenceofischemicepisodes.3,6Parenteral
opioids,though effective,maycausesedation,respiratory depression, nausea-vomiting and pruritus which may be troublesome.7Moreover,opioidsmayhavelimitedefficacy
whenpainisassociatedwithactivitysuchascoughingand deepbreathing.8Optionsof centralneuraxialanalgesiain
cardiacsurgicalpopulationisalsolimitedmostlybecauseof perioperativeanticoagulantuse,anditssuperioritytoPCA opioidisalsodebatable.9
Acute postoperative pain may also have a significant neuropathic component along with nociceptive pain due toperipheral mechanoreceptor stimulation andboth cen-tralandperipheralsensitizationbyseveralmechanisms.10,11
Duringsternotomy,intercostalnervesmaybedamagedby stretchingofthe intercostalnervesat thecosto-vertebral junction due to sternal retraction and damage may also occurduringdissectionofinternalmammaryarteryfromthe sternum;allofwhichultimatelycontributetoneuropathic pain.
Thegabapentinoidsgabapentinandpregabalinarenovel antiepileptic drugs, which also have significant efficacy in neuropathic pain12,13 and postoperative pain.14---16 They
exert anti-nociceptive effect by binding with the ␣2␦
subunitofvoltagesensitivecalciumchannel.14,17Aswellas
havingacentralanti-allodyniceffecttheyalsoinhibitpain transmission.17 The drugs are available only as oral
preparations, and differ mainly in bioavailability. Gabapentin is absorbed in the duodenum by a saturable
l-aminoacid transport mechanism, sothat bioavailability
varies inversely with dose.18 Bioavailability also varies
widely between individuals underliningthe need for dose individualization to achieve clinical goals.19 In contrast,
pregabalinisabsorbedthroughoutthesmallintestineswith linear uptake without transporter saturation.17 Both the
drugshaveverylowplasmaproteinbinding,nometabolism and is excreted unchanged in urine; dose modification is neededinrenalimpairment.17Withaneliminationhalf-life
of 4.8---8.7h, gabapentin requires thrice daily dosing.18
Alteredformulationshave been devisedtofacilitate once or twice daily regimens, e.g. Gralise (sustained release) andgabapentinenacarbil (aprodrug).20 Pregabalin hasan
eliminationhalf-lifeof5.5---6.3h,requiringtwicetothrice daily dosing.17 Bothare free from significant side effects
and drug interactions in the clinically useful dosage.17
Gabapentin may be useful for the prevention of chronic postsurgical pain also.21 Both have also been extensively
studiedinvarioussurgicalpopulationforpostoperativepain managementwithvaryingdegreesofsuccess.FewRCTs22---29
haveaddressedtheefficacyofperioperativeadministration ofgabapentinoidsonacutepostoperativepainaftercardiac surgery and they reported variable results. Hence, we conducted this systematic review to find out efficacy of gabapentin and pregabalin in acute postoperative pain aftercardiacsurgery.
Methods
Publishedprospectivehumanclinicaltrials,whichcompared preoperative and/or postoperative gabapentin/pregabalin withplaceboor notreatment forpostoperativepain man-agement after cardiac surgery has been included in this review.
Datesourceandsearchmethod
PRISMA 2009 Flow diagram
Records identified through database searching
(n=174)
Records screened (n=174)
Full-text articles assessed for eligibility
(n=10)
Studies included in qualitative synthesis
(n=8 )
Studies included in quantitative synthesis
(meta-analysis) (n=8)
Records excluded (n=164 )
n=2 of full-text articles excluded:
n=1 article compared gabapentin with diclofenac for chronic pain
n=1 article was non-RCT
Identification
Screening
Eligibility
Included
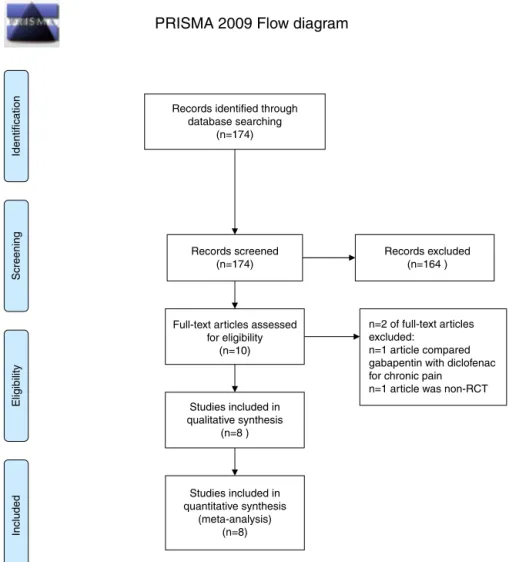
Figure1 PRISMAflowdiagramforstudyselection.
Keywords: ‘‘gabapentin’’; ‘‘pregabalin’’; ‘‘cardiac’’ and ‘‘sternotomy’’tofindouttheeligibleclinicaltrialson20th September2013. Another literaturesearch wasalso done on9th August; 2015 toupdate the result of the previous search. The search strategy in PubMed has been men-tionedinAppendix1.References fromtheprimarysearch resultswerealsomanuallysearchedforpotentiallyeligible trials.
Studyselection
Published prospective randomized human clinical tri-als, which compared preoperative and/or postoperative gabapentin/pregabalin with placebo or no treatment for postoperativepainmanagementaftercardiacsurgeryhave been included in this study. We did not impose any lan-guagerestrictioninthesearch strategy.Studies thathave beendoneoneitheradultorpediatricpopulationhavebeen includedinthisreview.Wedidnotsearchfor unpublished trials.Authorswerenotaskedfor unpublisheddatainthe includedtrials.APRISMAflowdiagram30 ofstudyselection
isdepictedinFig.1.
Exclusioncriteria
Clinicaltrialswhereoralgabapentinorpregabalinhasbeen comparedwithplacebooranyotherdruginsurgical popu-lationsotherthancardiacsurgerywerenotincludedinthis review.Studieswhichdidnotreporttheeffectsofthestudy drugonacute postoperativepainwere alsoexcluded. We alsoexcludedstudieswhereapostoperativeregional anal-gesiatechniquewasusedasapartofmultimodalregimen.
Datacollection
Potentiallyeligibletrialsweremanuallysearchedfromthe abstractstodeterminetheireligibilityinthisreview.We col-lectedtherequireddatafromthefull-textofthetrials.Two authorsindependently(DKB,SB)extractedalldatafromthe eligibletrials.InitiallyalldataweretabulatedinMicrosoft ExcelTMspreadsheet.
Dataitems
randomizationandblinding, study population, protocolof study drug administration, postoperative opioid consump-tion and pain scores, incidence of chronic pain following sternotomy andchronicpain scores,durationof mechani-calventilationandICUstay,andadversereactions.Allthe extracteddataweretabulatedinaMicrosoftExcel spread-sheet.
Primary outcome measure of this review was postop-erativepainscores(both atrest anddynamic).Secondary outcomemeasureswerepostoperativeopioidconsumption, effectsofthestudydrugsonopioidrelatedadverseeffects, durationofmechanicalventilationandICUstay.
Where a quantitativemeta-analysis wasnot possible a qualitativesystemicreview ofthe reporteddatawas per-formed.
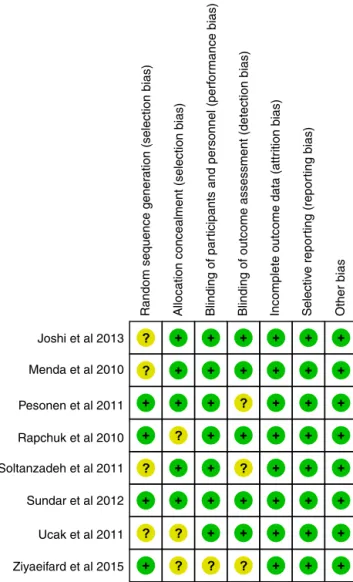
Riskofbiasinindividualstudies
The quality of eligible trials was assessed using the ‘risk of bias’ tool within Review Manager, version 5.2.3 soft-ware(ReviewManager[RevMan].Version5.2.Copenhagen: The Nordic Cochrane Centre, The Cochrane Collabora-tion,2012)bytwoauthorsworkingindependently(SMand AS).Randomsequencegeneration,allocationconcealment, blinding, incomplete data, and selective reporting were assessed;basedonthemethodofthetrials,eachwasgraded ‘‘yes’’,‘no’,or‘unclear’,whichreflectedahighriskofbias, low riskof bias,and uncertainbias, respectively. Risksof biassummaryintheindividualstudieshavebeenprovided inFig.2.
Results
Database searching revealed 174 articles. In six clinical studiesgabapentinwasusedasananalgesicincardiac sur-geries. However, in one31 of them it was compared with
diclofenac; hence it was excluded fromanalysis. Another RCT32 compareda gabapentin containing multimodal
reg-imen with opioid-based analgesic regimen. Finally, four RCTs23,25,26,28evaluatinggabapentinandanotherfour
study-ing pregabalin22,24,27,29 met our inclusion criteria for this
systematic review. Risk of bias in the individual studies hasbeen furnishedinFig.2.Studyprotocolofthe individ-ualstudies andpatientpopulationhavebeen describedin
Table1.The pooledresults have been summarized in the followingsection.
Postoperativepain
All the included studies reported painscores at different pointsoftime;henceapooledanalysishasnotbeen possi-ble.
Gabapentin
Ucak etal.28 reported alower painscorewiththe useof
gabapentinbothduringrestandcoughat6h,12h,18h,24h, 48hand72h.Soltanzadehetal.26reportedthatpainscores,
bothatrestandduringcoughingat2h,6h,and12hafter extubationweresignificantlylowerinpatientswhoreceived gabapentin. Menda et al.23 reported lower pain scores
Joshi et al 2013
Random sequence gener
ation (selection bias)
Allocation concealment (selection bias) Blinding of par ticipants and personnel (perf
or
mance bias)
Blinding of outcome assessment (detection bias) Incomplete outcome data (attr
ition bias)
Selectiv
e repor
ting (repor
ting bias)
Other bias
Menda et al 2010
Pesonen et al 2011
Rapchuk et al 2010
Soltanzadeh et al 2011
Sundar et al 2012
Ucak et al 2011
Ziyaeifard et al 2015
Figure2 Summaryof‘‘riskofbias’’atindividualstudylevel.
duringrestupto48hafterextubationbutonlyupto12hfor painduringcoughing.However,Rapchuketal.25reporteda
similarVASscorebothduringrest andcoughingupto72h postoperativeperiod.Rafiqetal.32evaluatedpainscoresby
11pointNRSandfoundthatpatientsinthegabapentin con-tainingmultimodalgroup,inallcategories,except‘‘worst pain’’onday4,hadlowermeanpainscores.Patientshad significantlyloweraverage painsensationfromday0(day ofsurgery)throughouttoday3.Theleastpainexperienced duringthedaywasalsolowerinthemultimodalgroupfrom day1today3.
Pregabalin
InthestudyofJoshietal.22pain-scoresatrestat6h,12h,
24hand36hfromextubationandpainscoresatdeepbreath at 4h, 6h, 12h, 24h and 36h fromextubation were less in pregabalintreated patients (p<0.05). They also found that peak inspiratory flow rates as assessed by incentive spirometry were higher in pregabalin group as compared to control group at 12h, 24h and 36h from extubation (p<0.05).Pesonenetal.24reportedsignificantlylower
Table1 Summaryofstudyprotocolandresultsofindividualstudies. Author&year Patients Studyprotocol Post-operative
analgesics
Analgesicoutcome Otheroutcome
Gabapentin
SoltanzadehM etal.,201126
60menaged 20---70years postedforCABG
Oralgabapentin 800mg2hbefore surgeryand 400mg2hafter extubation (n=30),vs. placebo(n=30)
Morphine Painscoresbothat restandduring coughingwere significantlylower inthegabapentin group(p=0.02). Hemodynamic changes(HR,SBP, DBP)andthe incidenceof nausea,vomiting andrespiratory depressionwithin 24hwere comparable betweenthetwo groups.
Postoperative
mechanicalventilation wassignificantly (p=0.03)longer (5.4±1.7h)in gabapentinthanin controlgroup (4.4±1.6h). Thenumberof over-sedatedpatients (asedationscore>2) washigherin gabapentingroup.
Mendaetal., 201023
60youngmen undergoingCABG
Oralgabapentin 600mg2hbefore surgery(n=30), vs.placebo (n=30)
MorphinePCA, paracetamol
Totalmorphine consumptionwas lowerintheGABA group(6.7±2.5) thantheplacebo (PLA)group (15.5±4.6mg, p<0.01)at24h. Painscoresatrest weresignificantly lowerintheGABA groupthroughout thestudyperiod (p<0.05).
Painscoresat2,6, and12hduring coughingwere significantlylower intheGABAgroup (p<0.05),whereas painscoresduring coughingwere similarat18,24, and48hbetween thegroups.
Thepostoperative mechanicalventilation periodwassignificantly prolongedintheGABA group(6.6±1.2h) comparedwiththePLA group(5.5±1h, p<0.01).
Thenumberofover sedatedpatients (patientswitha Ramsayscore>2)was higherinthe
GABAgroupat2,6, and12hofstudy. Therewaslower incidenceofnauseain theGABAgroup (p=0.02).
Rapchuk etal.,201025
60patients undergoing median sternotomy
Oralgabapentin 1200mg2hbefore surgicalincision and600mgtwice adayforthenext twopostoperative days(n=30),vs. placebo(n=30).
FentanylPCA, paracetamol, tramadol, pethidine, NSAIDs
TotalPCAfentanyl usageinthefirst 48hwassimilarin twogroups. VASscoresrecorded at12,24,48and 72hatrestand movementwerenot significantly different.
Sleepscores,number ofantiemeticdosesin first48h,adjunctive painmedicationsused andscoreachievedon thequalityofrecovery questionnairewere similarinthetwo groups.
Theincidenceof side-effects
Table1 (Continued)
Author&year Patients Studyprotocol Post-operative analgesics
Analgesicoutcome Otheroutcome
UcakAetal., 201128
40patientswith IHDundergoing CABG
Oralgabapentin 1.2g·dL−11h
beforesurgeryand for2daysafter surgery(n=20), vs.placebo (n=20)
Tramadol, paracetamol
Postoperativepain scoresat1,2,and3 dayswerelowerin thegabapentin group(p<0.05). Painscoresat1and 3months
postoperatively werealsolowerin thegabapentin group(p>0.05). Consumptionof rescueanalgesic (tramadol)within 24hafter extubationinthe gabapentingroup was99.0±53.8mg vs.149.4±72.5mg intheplacebo group(p<0.05).
Therewereno differencesinthe incidenceofside effectsandtimeto extubation.
Pregabalin Joshietal., 201322
40patientsaged 30---65years undergoing primaryoff-pump CABG
Oralpregabalin 150mg2hbefore inductionand 75mgevery12h for2
post-operative days(n=20),vs. placebo(n=20)
Tramadol, paracetamol, diclofenac
Pain-scoresatrest at6,12,24and36h fromextubationand painscoresatdeep breathat4,6,12, 24and36hfrom extubationwere lessinpregabalin treatedpatients (p<0.05).Rescue analgesic(tramadol) consumptionwas reducedby60%in pregabalingroup (p<0.001).Thepain severityscoreswere higherinthecontrol groupat12,24and 36h(p<0.05).Pain atrestanddeep breathingat1 monthand3months aftersurgerywere comparableamong thegroups.
Sedation(RASS), incidencesof
respiratorydepression andnauseawere comparable. Extubationtime, durationofICUand hospitalstaywerealso similar.Peak
inspiratoryflowrates asassessedby incentivespirometry werehigherin pregabalingroupas comparedtocontrol groupat12,24and 36hfromextubation (p<0.05)
Pesonen etal.,201124
70patientsaged 75yearsorolder, undergoing primaryelective CABGorsingle valverepairor replacementwith CPB
Oralpregabalin 150mg1hbefore surgeryand75mg twicedailyfor5 postoperativedays (n=35),vs. placebo(n=35)
Oxycodone Percentageof patientsrequiring analgesiawas significantlylower at2,10,and12h afterextubationin thepregabalin group(p<0.05).
Table1 (Continued)
Author&year Patients Studyprotocol Post-operative analgesics
Analgesicoutcome Otheroutcome
Pregabalinalso reduced consumptionof parenteral oxycodoneduring 16hafter extubationby43% andtotaloxycodone consumptionfrom extubationtothe endofthefifth postoperativeday by48%.The incidenceofpain duringmovement wassignificantly lowerinthe pregabalingroupat 3months
postoperatively,but painafter1month wassimilar.
Timetoextubationwas significantlylongerin thepregabalingroup (638±285vs. 500±233min;
p<0.05).Incidenceof nauseaandvomiting wascomparable.
Sundaretal., 201227
60adultpatients scheduledfor electiveoff-pump CABG
Oralpregabalin 150mg1hbefore surgery(n=30), vs.placebo (n=30)
Fentanyl VASmeasuredat6, 12,and24hafter surgeryandfentanyl consumptionupto 24haftersurgery wassimilarbetween thegroups.
Ramsaysedationscores at6,12,and24hafter surgeryweresimilar betweenthegroups. Durationofventilation andICUstayand incidencesofnausea, vomitinganddizziness werealsocomparable. Ziyaeifard
etal.,201529
60patientsolder than20years postedforelective CABG
Oralpregabalin 150mg2hbefore surgery(n=30), vs.placebo (n=30)
Morphine Painscoreswere significantlylower inthepregabalin groupat4,12,and 24hofsurgery (p<0.05);but morphine consumptionwas similarbetweenthe groups.
DurationofICUstay wassimilar.
CABG,CoronaryArteryBypassGrafting;HR,HeartRate;SBP,SystolicBloodPressure;DBP,DiastolicBloodPressure;PCA,PatientControlled Analgesia;IHD,IschemicHeartDisease;ICU,IntensiveCareUnit;VAS,VisualAnalogueScale;RASS,RichmondAgitation-SedationScale; MMSE,MiniMentalStateExamination;CAM-ICU,ConfusionAssessmentMethodfortheICU.
measuredat6h,12h,and24haftersurgery;while Ziyaei-fardetal.29foundpainscorestobesignificantlylowerinthe
pregabalingroupat4h,12h,and24hofsurgery(p<0.05).
Postoperativeopioidconsumption
Gabapentin
Threestudies23,26,28reportedpostoperativeopioid
consump-tionupto24hafterextubationandone25reportedfentanyl
consumption up to 48h. Two23,26 of them used morphine
and one28 used tramadol. Menda et al.23 found that
pre-operative gabapentinreduces morphineconsumption than placebo (6.7±2.5mg vs. 15.5±4.6mg, p<0.01). Soltan-zadehet al.26 reportedpre andpostoperative gabapentin
reduces opioid consumption than placebo (0.9±1.5mg vs. 1.5±4mg, p=0.01). Ucak et al.28 reported
intra-venous tramadol consumption and found that gabapentin reducestramadolconsumption thanplacebo (99±53.8mg vs. 149.4±72.5mg, p<0.05). Rapchuk et al.25 reported
Mean difference IV, Fixed, 95% Cl Mean difference
IV, Fixed, 95% Cl Placebo
Weight Total SD
SD Mean
Mean Study or subgroup
Menda et al 2010 6.6
9.6 4.1 27 9.2 3.9 27 30 20
–2 –1 0 1 2
0.8 1.6 4.4 30 1.7 1.4 7.9 5.4
20 7.65
3.2%
29.2% 20.9%
0.40 [–1.73, 2.53] 1.00 [0.16, 1,84] 0.25 [–0.46, 0.96] 1.2 30 5.5 1 30 46.7% 1.10 [0.54, 1.66] Rapchuk et al 2010
Soltanzadeh et al 2011 Ucak et al 2011
Heterogeneity: Chi2=3.79, df=3 (P=.29); l2=21%
Favours [Gabapentin] Favours [Placebo] Test for overall effect: Z=4.15 (P<.0001)
Total (95% Cl) 107 107 100.0% 0.81 [0.43, 1.19]
Total Gabapentin
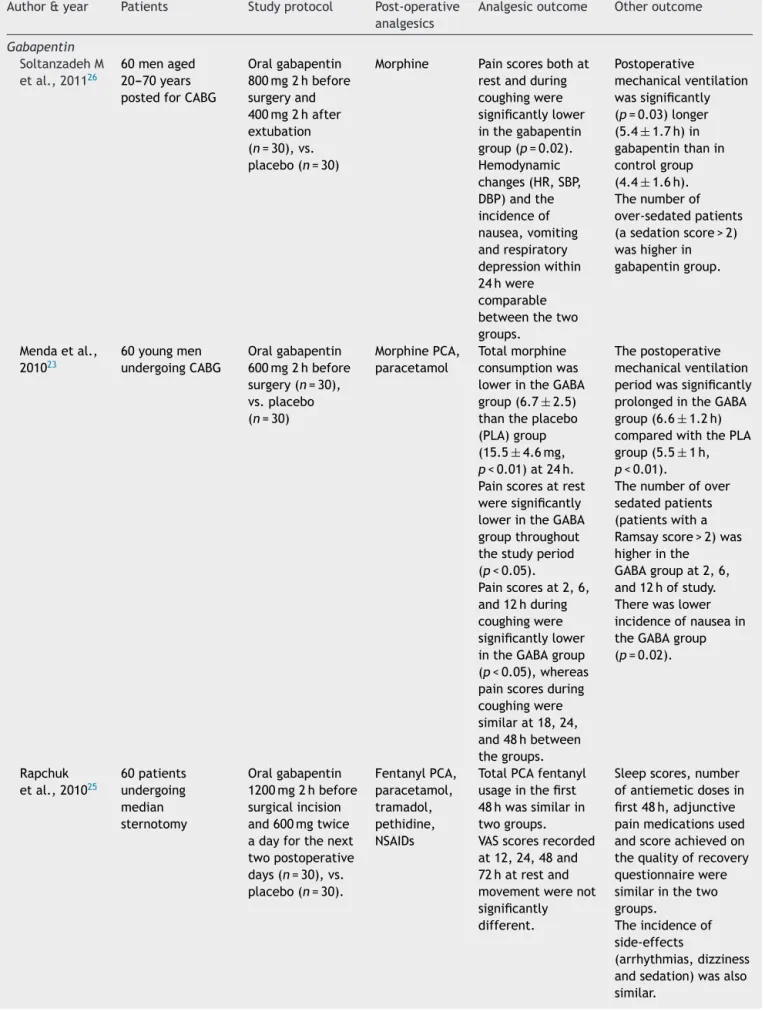
Figure3 Forestplotshowingpooledanalysisofmeandifferenceofdurationofmechanicalventilationforgabapentin.
Mean difference IV, Random, 95% Cl Mean difference
IV, Random, 95% Cl Control
Weight Total SD
SD Mean
Mean Study or subgroup
Joshi et al 2013 7.45
10.63 4.75 29 8.33 3.88 31 30
–100 –50 0 50 100
5.13 10.37 30 4.68 10.6
28.2% 24.4%
2.30 [0.10, 4.50] 0.23 [–2.25, 2.71] 1.95 20 7.68 1.98 20 47.4% –0.23 [–1.45, 0.99] Pesonen et al 2011
Sundar et al 2012
Heterogeneity: Tau2=0.91, Chi2=3.89, df=2 (P=.14); l2=49%
Favours [experimental] Favours [control] Test for overall effect: Z=0.76 (P=.45)
Total (95% Cl) 79 81 100.0% 0.60 [–0.94, 2.13]
Total Pregabalin
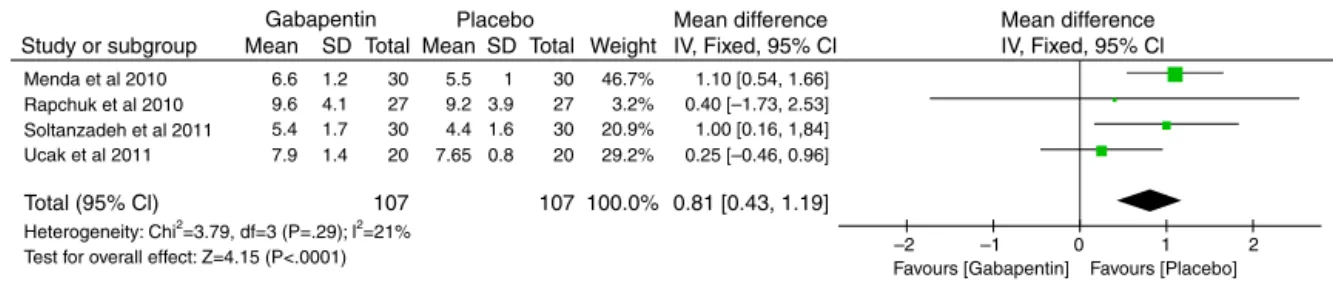
Figure4 Forestplotshowingpooledanalysisofmeandifferenceofdurationofmechanicalventilationforpregabalin.
Pregabalin
Joshietal.22foundthattramadolconsumptionwasreduced
by 60% in the pregabalin group compared to placebo (67.8±60.25mg vs. 167.1±52.1mg, p<0.001). Pesonen et al.24 reported that pregabalin reduced consumption
of parenteral oxycodone during 16h after extubation by 43% (8±5mg vs. 14±6mg, p<0.001) and total oxy-codone consumption from extubation to the end of the fifth postoperative dayby 48% (48±28mg vs.93±44mg,
p<0.001).However,Sundaretal.27 andZiyaeifardetal.29
found no difference in fentanyl (241.67±178.87mcg vs. 251.67±181.47mcg, p>0.05) and morphine (3±0.17mg vs. 3.1±0.15mg, p>0.05) consumption up to 24h after surgeryrespectively.Ofnote, pregabalinwascontinuedin thepostoperativeperiodinthefirsttwoRCTs(tilldays2and 5respectively),22,24 and wasusedasasinglepreoperative
doseinthelasttwo.27,29
Chronicpain
Gabapentin
Ucaketal.28foundthatpainscoresat1and3months
post-operatively were lower in the gabapentin group but the differencewasnotstatisticallysignificant(p>0.05).
Pregabalin
InthestudybyJoshietal.22painatrestanddeep
breath-ingat1monthand3monthsaftersurgerywerecomparable amongthegroups.Pesonenetal.24 reportedthatthe
inci-dence ofpainduring movement wassignificantlylowerin thepregabalingroupat3monthspostoperatively,butpain after1monthwassimilar.
Durationofmechanicalventilation
A pooledanalysis found that durationof mechanical ven-tilation is significantly increased withthe use gabapentin (MD=0.81h;95%CI0.43---1.19; p<0.0001;n=214)(Fig.3)
but not with pregabalin (MD=0.60h; 95% CI −0.94---2.13;
p=0.45;n=160)(Fig.4).
LengthofICUstay
Use of perioperative gabapentin (MD=1.06h; 95% CI
−0.67---2.79; p=0.23; n=120) or pregabalin (MD=0.63h; 95% CI −3.59---4.85; p=0.77; n=220) does not affect the durationofICUstaysignificantly.
Postoperativecomplications
Gabapentin
Commonlyreportedadverseeffectsofgabapentinare seda-tion, dizziness and somnolence.17 Ucak et al.28 reported
no increased incidence of any of the adverse effects of gabapentin. Menda et al.23 reported an increased
inci-dence of sedation (Ramsay sedation score>2) with the use of gabapentin at 2h, 6h and 12h after extubation. They also reported a significantly less incidence of nau-sea in gabapentin treated patients. Rapchuk et al.25 and
Soltanzadeh et al.26 also reported no increased adverse
effectwiththeuseofgabapentin.
Pregabalin
Pregabalin has a side effect profile similar to that of gabapentin.17 Sedation scores and incidence of
nau-sea/vomiting as reported by three RCTs22,24,27 were
comparablebetweengroups.Joshietal.22alsoreported
sim-ilarincidenceofrespiratorydepressionandSundaretal.27
Discussion
The principal findings of this review are that gabapentin didnotreducepostoperativeopioidconsumptionafter car-diac surgery; but mayreduce pain scores at the expense ofincreaseddurationof mechanicalventilation. However, gabapentinwassafeandfreeofseriousadverseeffectsanda singlestudy23reporteddecreasedincidenceofnauseaalso.
Pregabalin,ontheotherhand,decreasedpostoperativepain scores;reducedopioidconsumptionwhenitwascontinued inthepostoperativeperiod;anddidnotincreaseduration ofmechanicalventilation,sedationorothersideeffects.
Efficacyofperioperativegabapentininreducingpainis well established in other surgeries like spine surgeries,33
breastsurgeries,34 gynecologicsurgeries35 etc.However,it
maynothave efficacy inmanagement of post craniotomy pain.36 It is likely that gabapentin willbe more effective
whereneuropathiccomponentissignificant.Futilityof sin-gle preoperative dose of gabapentin has been found in varioussettings.37---39 Gabapentinmaybemoreeffectivein
postoperativepainmanagementat higherdosesandwhen administeredboth preandpostoperatively.17 Amongstthe
included studiesin ourreview, Ucaket al.28 and Rapchuk
et al.25 used gabapentin at a dose of 1200mg
·day−1 2h
beforesurgery andcontinued in the postoperative period also.However, Mendaet al.23 used only in the
preopera-tiveperiodand Soltanzadehetal.26 useda lowerdose of
gabapentin(800mg·day−1).Itisnotablethatdespite using
gabapentinatadoseof1200mcg·day−1bothpreand
post-operatively, Rapchuk et al.25 did not find any reduction
of pain scores and fentanyl consumption. Parlow et al.40
in2010 found that plasma concentrationof gabapentin is unaffected by cardio-pulmonary bypass and patients who receivedgabapentinconsumesimilaramount ofmorphine inthepostoperativeperiodasthosewhodidnot.In previ-ousstudies,41wheregabapentinwasfoundtobeineffective,
useofregionalanesthesiainthosestudieswasblamedand aspeculationwasmadethatregionalanesthesiacouldhave preventedcentralsensitization.However,noneofthe stud-iesincludedhere usedanyregionalanesthesiatechnique. Fromaclinicalpointofview,areducedopioidrequirement maybemore importantthan onlypainscores. Again pain scoresrecordedatspecifictimepointsonlydoesnotimply patients’analgesiaoveratimeperiod.Noneofthestudies reportedpatients’satisfactionlevelhere.
Data reporting chronic pain was inadequate for any conclusion.
Efficacyof pregabalinin reducingpost-operative acute painhasbeenreviewedinseveralmeta-analyses.15,42,43Eipe
etal.15 came tothe conclusionthat pregabalindecreases
analgesic consumption following various types of surger-ies, but had a small effect in improving pain control and this effect is primarily observed in surgeries asso-ciated with pronociceptivemechanisms, e.g. spine, joint arthroplasty,and amputations.As sternotomy and sternal retraction involves intercostal nerve damage and associ-ated central andperipheral sensitization,acute allodynia andhyperalgesiaoften occur.10 Thismayexplainthe
find-ing of reduced pain scores with pregabalin in three of the included RCTs.22,24,29 Two RCTs22,24 which had
contin-ued pregabalin 150mg·day−1 in the postoperative period,
demonstrated reduced opioid consumption, whereas the
other twoRCTs27,29 using single preoperative 150mg dose
of pregabalin did not find any reduction. In the case of Sundar et al.,27 their study was not adequately powered
to detect differences in pain scores or opioid consump-tion.Theabsenceofeffectintheotherone29corroborates
theconclusionofSchmidtetal.17 thatcontinuingthedrug
postoperativelyislikelytobemoreeffectivethanasingle preoperative dose, though it is in contrastto the finding byMishrikyetal.intheirmeta-analysis.42 Mishrikyetal.42
hadfoundnosignificantdifferencebetweensingleand mul-tiple dosing regimens, but their analysis hada significant componentofheterogeneitybecauseofpoolingofdifferent surgeriesandanesthesiatechniques.Thiscontradictioncalls forfurtherresearchinthisarea.However,itshouldbenoted thattheeffectofcardio-pulmonarybypassonpregabalinhas notbeenstudied.Inatleastonestudy,22 improved
analge-siatranslatedintoimproved peakinspiratoryflowratesas assessedbyincentivespirometry.
Increased duration of mechanical ventilation after gabapentin use may be due to a well-known side effect ofgabapentini.e.increasedsedation.However,the incre-mentisclinicallyinsignificant:meandifferenceisonly0.81h (48min).Itistobekeptinmindthatthestudiesused dif-ferentextubationandweaningprotocolandthisresultisto beinterpretedcautiously.Pregabalindidnotincrease dura-tionofmechanicalventilation.Bothdrugsdidnothaveany effectonthedurationofICUstay.
Despitepopularbelief,gabapentinwasshowntoincrease sedation in one RCT only. None of the studies reported any serious adverse effects of gabapentin. Moreover, one study23 found that gabapentin may reduce postoperative
nauseaalso.Itisnotsurprising,becauseitmayhavesimilar efficacyaftercraniotomyalso.36 Alowermorphine
require-mentingabapentintreatedpatientsmayberesponsiblefor this.Incidencesofsedation,respiratorydepressionand nau-sea/vomitingwerenotalteredwithpregabalinaswell.This lackofsignificantsideeffectsmaybeexplainedbytheuse ofalowerdose(150mg)ofthedrug.
The clinical relevanceof ourreview is that in spite of smallindividualstudiesreportingbenefitofusing perioper-ativegabapentinoidsincardiacsurgery,ouranalysisfailed to corroborate any unambiguous clinical efficacy, though nosignificant adverseeffectis associated.So,thereisno strong evidencetosupportusingperioperative gabapentin andpregabalinincardiacsurgicalpatientsatthistime.
Limitations
Themostimportantlimitationofourreviewistheinclusion of limited number of studies. Despite extensive database searching,only eightstudies couldbeincluded.Individual studies, though well designed, comprise small number of patients.AlargeRCTinthefuturemayalterourfinding.The dosageprotocolsofgabapentinandpregabalinarealso var-iedinthestudies.Dataonchronicpainisalsoverylimited.
Conclusion
consumption in the cardiacsurgical patients primarily for themanagementofacutepostoperativepain.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Appendix
1.
(‘‘gabapentin’’[SupplementaryConcept]OR‘‘gabapentin’’ [All Fields]) AND (‘‘heart’’[MeSH Terms] OR ‘‘heart’’ [All Fields]OR‘‘cardiac’’[AllFields])
(‘‘gabapentin’’ [Supplementary Concept] OR ‘‘gabapentin’’ [All Fields]) AND (‘‘sternotomy’’ [MeSH Terms]OR‘‘sternotomy’’[AllFields])
(‘‘pregabalin’’ [Supplementary Concept] OR ‘‘pregabalin’’[AllFields])AND(‘‘heart’’[MeSHTerms]OR ‘‘heart’’[AllFields]OR‘‘cardiac’’[AllFields])
(‘‘pregabalin’’ [Supplementary Concept] OR ‘‘pregabalin’’ [All Fields]) AND (‘‘sternotomy’’ [MeSH Terms]OR‘‘sternotomy’’[AllFields])
References
1.MeehanDA,McRaeME,RourkeDA,etal.Analgesic administra-tion,painintensity,andpatientsatisfactionincardiacsurgical patients.AmJCritCare.1995;4:435---42.
2.MilgromLB,BrooksJA,QiR,etal.Painlevelsexperiencedwith activitiesaftercardiacsurgery.AmJCritCare.2004;13:116---25. 3.ChaneyMA.Howimportantispostoperativepainaftercardiac
surgery?JCardiothoracVascAnesth.2005;19:705---7.
4.EisenbergE,PultorakY,PudD,etal.Prevalenceand character-isticsofpostcoronaryarterybypassgraftsurgerypain(PCP). Pain.2001;92:11---7.
5.MazzeffiM,KhelemskyY.Poststernotomypain:aclinicalreview. JCardiothoracVascAnesth.2011;25:1163---78.
6.ManganoDT, SilicianoD, Hollenberg M, et al. Postoperative myocardialischemia.Therapeutictrialsusingintensive analge-siafollowingsurgery.TheStudyofPerioperativeIschemia(SPI) ResearchGroup.Anesthesiology.1992;76:342---53.
7.Baltali S, Turkoz A, Bozdogan N, et al. The efficacy of intravenous patient-controlled remifentanil versus morphine anesthesiaaftercoronaryarterysurgery.JCardiothoracVasc Anesth.2009;23:170---4.
8.Tverskoy M, Oren M, Dashkovsky I, et al. Alfentanil dose---responserelationships for relief ofpostoperativepain. AnesthAnalg.1996;83:387---93.
9.Hansdottir V, Philip J, Olsen MF, et al. Thoracic epidural versusintravenous patient-controlled analgesiaaftercardiac surgery: a randomized controlledtrial on lengthof hospital stayandpatient-perceivedqualityofrecovery.Anesthesiology. 2006;104:142---51.
10.AlstonRP,PechonP.Dysaesthesiaassociatedwithsternotomy forheartsurgery.BrJAnaesth.2005;95:153---8.
11.DahlJB,MathiesenO,MoinicheS.’Protectivepremedication’: an option with gabapentin and related drugs? A review of gabapentinandpregabalininthetreatmentofpost-operative pain.ActaAnaesthesiolScand.2004;48:1130---6.
12.Moore RA, StraubeS, Wiffen PJ,et al. Pregabalin for acute and chronic pain in adults. Cochrane Database Syst Rev. 2009:CD007076.
13.MooreRA, Wiffen PJ,DerryS,et al.Gabapentinfor chronic neuropathicpainandfibromyalgiainadults.CochraneDatabase SystRev.2011:CD007938[Review].
14.Dauri M, FariaS, Gatti A, et al. Gabapentinand pregabalin fortheacutepost-operativepainmanagement.A systematic-narrative reviewof therecent clinicalevidences. Curr Drug Targets.2009;10:716---33.
15.EipeN,PenningJ,YazdiF,etal. Perioperativeuseof prega-balin for acute pain-asystematic review and meta-analysis. Pain.2015;156:1284---300.
16.StraubeS,DerryS,MooreRA,etal.Singledoseoralgabapentin for establishedacutepostoperativepain inadults.Cochrane DatabaseSystRev.2010:CD008183[Review,35refs].
17.Schmidt PC, Ruchelli G, Mackey SC, et al. Perioperative gabapentinoids:choiceofagent,dose,timing,andeffectson chronicpostsurgicalpain.Anesthesiology.2013;119:1215---21. 18.RoseMA,KamPC.Gabapentin:pharmacologyanditsuseinpain
management.Anaesthesia.2002;57:451---62.
19.GidalBE,RadulovicLL,KrugerS,etal.Inter-andintra-subject variabilityingabapentinabsorptionandabsolute bioavailabil-ity.EpilepsyRes.2000;40:123---7.
20.Moore RA, WiffenPJ,Derry S,et al.Gabapentinfor chronic neuropathicpainandfibromyalgiainadults.CochraneDatabase SystRev.2014;4.CD380079.
21.ClarkeH,BoninRP,OrserBA,etal.Thepreventionofchronic postsurgical pain using gabapentin and pregabalin: a com-bined systematic review and meta-analysis. Anesth Analg. 2012;115:428---42.
22.JoshiSS, JagadeeshAM. Efficacyofperioperative pregabalin inacuteandchronicpost-operativepainafteroff-pump coro-naryarterybypasssurgery:arandomized,double-blindplacebo controlledtrial.AnnCardAnaesth.2013;16:180---5.
23.Menda F, Koner O, Sayin M, et al. Effects of single-dose gabapentin on postoperative pain and morphine consump-tion after cardiac surgery. J Cardiothorac Vasc Anesth. 2010;24:808---13.
24.PesonenA,Suojaranta-YlinenR,HammarenE,etal.Pregabalin hasanopioid-sparingeffectinelderlypatientsaftercardiac surgery:arandomizedplacebo-controlledtrial.BrJAnaesth. 2011;106:873---81.
25.Rapchuk IL, O’Connell L, Liessmann CD, et al. Effect of gabapentin on pain after cardiac surgery: a randomised, double-blind,placebo-controlledtrial.AnaesthIntensiveCare. 2010;38:445---51.
26.SoltanzadehM,EbadA,PipelzadehM,etal.Gabapentinmay relievepost-coronaryarterybypassgraftpain:adoubleblind randomizedclinicaltrial.IranCardiovascResJ.2011;5:79---82. 27.SundarAS,KodaliR,SulaimanS,etal.Theeffectsofpreemptive pregabalinonattenuationofstressresponseto endotracheal intubation and opioid-sparing effect in patients undergoing off-pumpcoronaryarterybypassgrafting.Ann CardAnaesth. 2012;15:18---25.
28.UcakA,OnanB,SenH,etal.Theeffectsofgabapentinonacute and chronic postoperative pain aftercoronaryartery bypass graftsurgery.JCardiothoracVascAnesth.2011;25:824---9. 29.ZiyaeifardM,MehrabanianMJ,FaritusSZ,etal.Premedication
with oral pregabalin for the prevention of acute postsurgi-calpainincoronaryarterybypass surgery.Anesth PainMed. 2015;5:e24837.
30.MoherD,LiberatiA,TetzlaffJ,etal.Preferredreportingitems for systematicreviewsandmeta-analyses:thePRISMA state-ment.PLoSMed.2009;6:e1000097.
31.BiyikI,GulculerM,KarabigaM,etal.Efficacyofgabapentin ver-susdiclofenacinthetreatmentofchestpainandparesthesiain patientswithsternotomy.AnadoluKardiyolDerg.2009;9:390---6. 32.RafiqS,SteinbruchelDA,WanscherMJ,etal.Multimodal anal-gesia versus traditionalopiate basedanalgesia aftercardiac surgery, a randomized controlled trial. J Cardiothorac Surg. 2014;9:52.
asystematicreviewandmeta-analysis.Spine(PhilaPa1976). 2013;38:1947---52.
34.Bharti N,BalaI,NarayanV,et al.Effect ofgabapentin pre-treatmentonpropofolconsumption, hemodynamicvariables, and postoperative pain relief inbreast cancersurgery. Acta AnaesthesiolTaiwan.2013;51:10---3.
35.Frouzanfard F, Fazel MR, Abolhasani A, et al. Effects of gabapentinon painand opioid consumptionafter abdominal hysterectomy.PainResManag.2013;18:94---6.
36.MisraS,ParthasarathiG,VilanilamGC.Theeffectofgabapentin premedication on postoperative nausea, vomiting, and pain inpatientsonpreoperativedexamethasoneundergoing cran-iotomy for intracranial tumors. J Neurosurg Anesthesiol. 2013;25:386---91.
37.Paul JE, Nantha-Aree M, Buckley N, et al. Gabapentin does not improve multimodal analgesia outcomes for total knee arthroplasty: a randomized controlled trial. Can J Anaesth. 2013;60:423---31.
38.Short J,DowneyK, Bernstein P,et al. Asinglepreoperative doseofgabapentindoesnotimprovepostcesareandeliverypain
management:arandomized,double-blind,placebo-controlled dose-findingtrial.AnesthAnalg.2012;115:1336---42.
39.Siddiqui NT, Fischer H, Guerina L, et al. Effect of a pre-operative gabapentin on postoperativeanalgesia in patients with inflammatory bowel disease following major bowel surgery: a randomized, placebo-controlled trial. Pain Pract. 2014;14:132---9.
40.ParlowJ,GilronI,MilneB,etal.Cardiopulmonarybypassdoes notaffectplasmaconcentrationofpreoperativelyadministered gabapentin.CanJAnaesth.2010;57:337---42.
41.Kinney MA, Mantilla CB, Carns PE, et al. Preoperative gabapentinforacute post-thoracotomyanalgesia:a random-ized, double-blinded, active placebo-controlled study. Pain Pract.2012;12:175---83.
42.MishrikyBM,WaldronNH,HabibAS.Impactofpregabalinon acuteandpersistentpostoperativepain:asystematicreview andmeta-analysis.BrJAnaesth.2015;114:10---31.