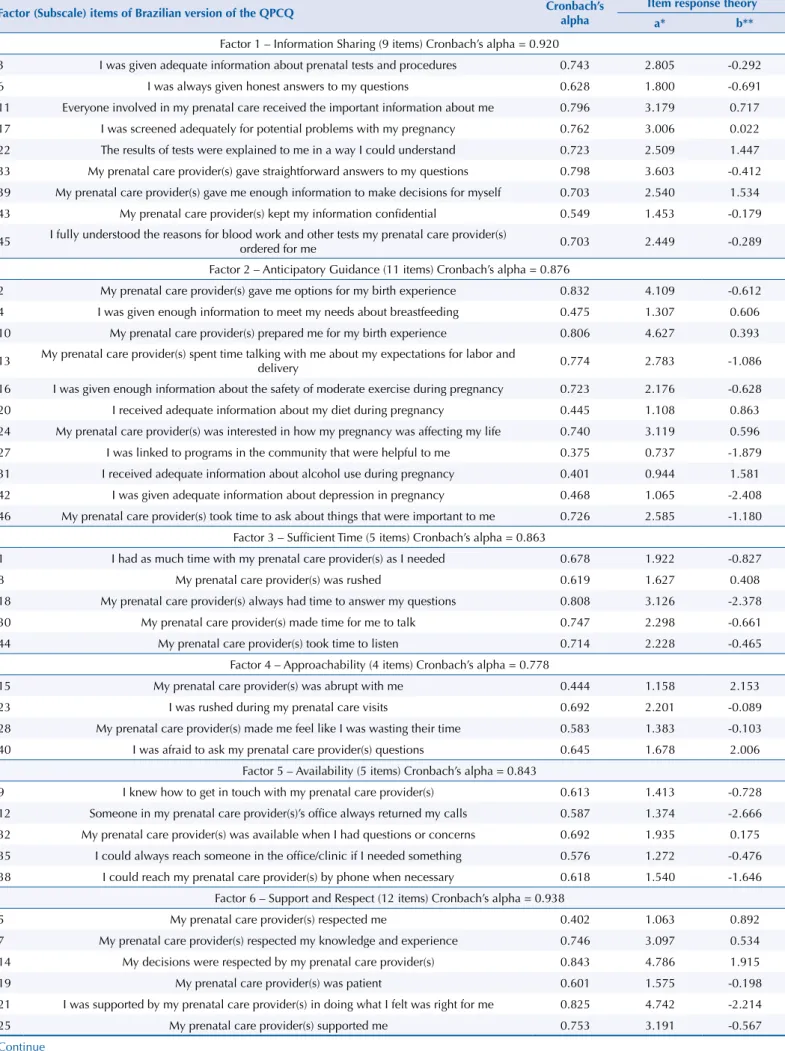
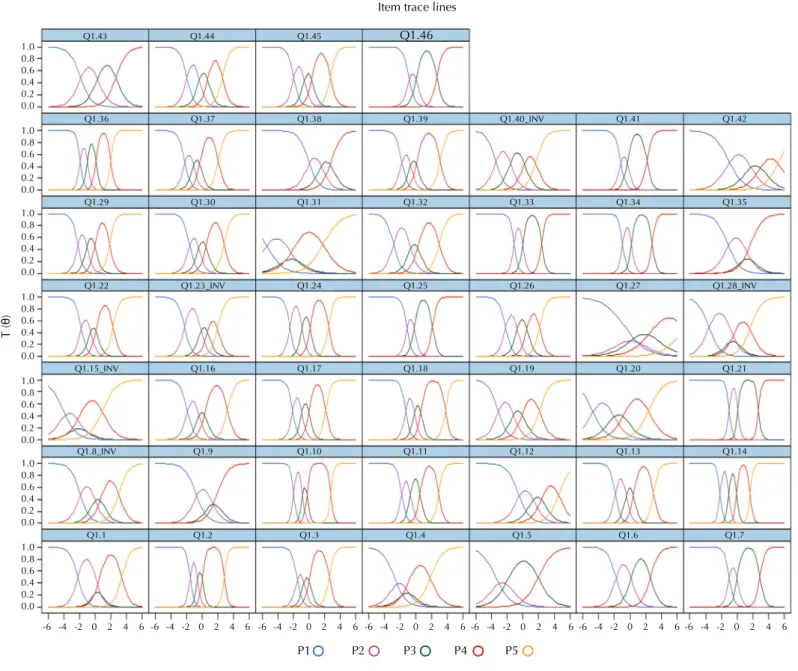
Cross-cultural adaptation and psychometric properties of the Brazilian-Portuguese version of the Quality of Prenatal Care Questionnaire (QPCQ)
Texto
Imagem


Documentos relacionados
E como eu tive, a seguir ao 25 de Abril, um investimento forte na militância política, militância política profissional, primeiro na clandestinidade e depois na luta política
To the best of our knowledge, this is the fi rst study designed to develop a Brazilian Portuguese version of the UCOPD questionnaire, which is a reliable questionnaire to
Objective: To assess the psychometric properties of the official Brazilian Portuguese-language version of the Paediatric Asthma Quality of Life Questionnaire
Massa seca de folha, caule, parte aérea, raiz, nódulo, massa unitária de nódulo, massa total, número de nódulos e atividade da nitrato redutase de plantas de feijoeiro,
Objective: To assess the psychometric properties of the official Brazilian Portuguese-language version of the Paediatric Asthma Quality of Life Questionnaire
The Portuguese version of the King’s Health Questionnaire has now all the psychometric properties assessed including validity, reliability and responsiveness, being the first Quality
Conclusions: The Brazilian version of EPIC is reliable and valid, and is a useful tool to evaluate the impact of retropubic radical prostatectomy on quality of life of Brazilian
Objective: The aim of this study was to examine the psychometric properties of the Brazilian version of the Multifactorial Memory Questionnaire (MMQ), which evaluates
