Artigo Original
Karlin Fabianne Klagenberg D’Andrea1 Bianca Simone Zeigelboim2 Paulo Breno Noronha Liberalesso3 Lucimary de Castro Sylvestre4 Ari Leon Jurkiewicz2 Jair Mendes Marques2
Keywords
Renal insuficiency Chronic Kidney transplantation Audiometry Acoustic impedance tests Auditory perception
Descritores
Insuiciência renal crônica Transplante de rim Audiometria Testes de impedância acústica Percepção auditiva
Correspondence address:
Karlin Fabianne Klagenberg D’Andrea Rua Acyr Guimarães, 436/1003, Água Verde, Curitiba (PR), Brazil, CEP: 80240-230.
E-mail: [email protected]
Received: 05/15/2012
Accepted: 10/05/2012
(1) Post-graduation (PhD) in Communication Disorders at the Biology and Medical School of Universidade Tuiuti do Paraná – UTP – Curitiba (PR), Brazil.
(2) Post-graduation in Communication Disorders at the Biology and Medical School of Universidade Tuiuti do Paraná – UTP – Curitiba (PR), Brazil.
(3) Post-graduation in Communication Disorders at the Biology and Medical School of Universidade Tuiuti do Paraná – UTP – Curitiba (PR), Brazil; Department of Neuropediatrics, Hospital Pequeno Príncipe – HPP – Curitiba (PR), Brazil.
(4) Department of Pediatric Nephrology, Hospital Pequeno Príncipe – HPP – Curitiba (PR), Brazil. This study was carried out at Universidade Tuiuti do Paraná – UTP – Curitiba (PR), Brazil.
Conlict of interest: nothing to declare.
kidney transplant
Achados audiológicos em pacientes submetidos ao
transplante renal
ABSTRACT
Purpose: To investigate the auditory behavior of patients with chronic renal failure (CRF) undergoing kidney transplantation. Methods: Thirty patients were evaluated, 10 (33.33%) females and 20 (66.67%) males, aging from 13 to 26 years (average, 16.97 years; standard deviation, 3.60 years). Patients underwent the following procedures: anamnesis, otolaryngological examination, audiological evaluation (pure tone and high frequency), acoustic impedance measurements and central auditory processing evaluation. A control group was used to compare the high-frequency audiometry results. Results: The following observations were made: absence of auditory complaints at the time of anamnesis; pure-tone audiometry was predominantly normal; patients presented lower hearing levels at the high-frequency audiometry, when compared to the control group, and as for the acoustic impedance measurements, curves of the type A were predominant; there was a change of the central auditory processing for 14 patients (46.67%) in the Staggered Spondaic Word Test (SSW); there was a signiicant difference between the age variable and the result of the pure-tone audiometry, that is, hearing sensitivity in thresholds from 250Hz to 8,000Hz decreased with advancing age; and the relation between the type of donor and the SSW test result was signiicant. Rates were higher when the patients had been transplanted from deceased donors compared to living donors. Conclusion: There were no changes in conventional audiological and high-frequency evaluation, or in the central auditory processing. Professionals involved in the care of kidney transplantation recipients must be better informed about the care, prevention, and early identiication of auditory disorders.
RESUMO
Objetivo: Investigar o comportamento auditivo de pacientes com insuiciência renal crônica submetidos ao transplante renal. Métodos: Foram avaliados 30 pacientes, 10 do gênero feminino e 20 do gênero masculino, na faixa etária de 13 a 26 anos (média de idade 16,97 anos). Os sujeitos foram submetidos a anamnese, avaliação otorrinolaringológica, avaliação audiológica convencional e de altas frequências, medidas de imitância acústica e avaliação do processamento auditivo central. Para os resultados da audiometria de altas frequências foi utilizado um grupo controle. Resultados: Os sujeitos não apresentaram queixas auditivas na anamnese. Os resultados da audiometria convencional demonstraram predomínio da normalidade; na audiometria de altas frequências, os pacientes apresentaram resultados piores do que os sujeitos do grupo controle. Na imitanciometria houve predomínio de curva tipo A bilateral. Na avaliação do processamento auditivo central, 14 sujeitos (46,67%) apresentaram resultados alterados no Staggered Spondaic Word Test (SSW). Houve diferença signiicativa entre a variável idade e o resultado da audiometria tonal limiar: quanto maior a idade, menor a sensibilidade auditiva nos limiares de 250 Hz a 8 kHz. Houve relação entre o tipo de doador (cadáver ou vivo) e o resultado do teste SSW: os índices de resultados alterados foram maiores quando o doador era cadáver, em comparação com casos de doador vivo. Conclusão:
INTRODUCTION
Chronic renal failure (CRF) is a silent disease that causes slow, progressive, and irreversible loss of the kidney func-tions(1). Nowadays, it is considered to be a public health
problem. The number of patients undergoing dialysis in Brazil has doubled in the past nine years, and the incidence of new cases increases by 8% per year(2). Data from the 2011
survey by the Brazilian Society of Nephrology (SBN) showed that 91.314 patients — out of 192,38 million inhabitants in Brazil — were under dialysis treatment(3). Early diagnosis is
important to delay the progression of the disease, to prevent complications and comorbidities, and to adequately prepare renal replacement therapy(2).
Hearing loss has been identiied in renal patients since the past century. Alport(1) suggested, in 1927, a classic genetic
syndrome connecting hearing impairment with renal failure. Later on, patients who developed renal failure and did not meet the genetic basis were shown to have hearing loss from unknown causes in different stages of the disease.
Some authors(4) have observed that large numbers of
hemodialysis(HD) sessions or repeated kidney transplants may result in electrolyte, biochemical, immunological, os-motic, and vascular changes that may disturb the function of the inner ear. These changes may cause hearing symptoms, such as loss of perception of treble frequencies, and vestibu-lar symptoms or even cause hearing loss over the course of the disease.
Ototoxic medications — the aminoglycoside antibiotics being the most common ones — are likely to cause irrevers-ible damage to the hair cells of the spiral organ(5). Cell
dam-age is related to complex substances formed in the reaction between the drug and the cell membrane phosphoinositides(6).
The kidney and the cochlear duct have microscopic anatomical similarities, as well as comparable physiologic, immunological, and pathological behaviors. The renal glom-erulus as much as the tubules are similar to the stria vascu-laris, an epithelial structure directly related to the vascular system; therefore, nephrotoxic drugs may also be ototoxic(6).
The cochlear duct has been shown to be vulnerable to such drugs by functional and morphological studies. Its basis is affected irst, which causes hearing loss starting from high frequencies. The monitoring of hearing function aimed at early detection of high-frequency hearing loss during oto-toxic treatment allows for the identiication of the otooto-toxicity progression since its onset(7).
Moreover, the professionals involved in the kidney trans-plant recipient’s care must be familiar with the handling, prevention, and early identiication of hearing impairment, as well as with the consequences of the ototoxic treatment, the secondary diseases and the exposure to noise, factors that can cause or worsen hearing loss. Audiological follow-up must be performed to ensure early identiication of any alteration.
The purpose of this paper is to analyze the hearing function behavior of CRF patients submitted to kidney transplantation.
METHODS
This study has been approved by the Ethics Committee of
Hospital Pequeno Príncipe, protocol number 0715-09, and
all participants or caregivers signed the informed consent. Thirty patients were assessed in the Research Group, RG (10 females, 33.33%, and 20 males, 66.67%, aging from 13 to 26 years — mean age= 16.97 years; SD= 3.6 years), all of them presenting CRF with different causes and having been submitted to kidney transplantation. They were all referred from
Hospital Pequeno Príncipe to the branch of Otoneurology at Universidade Tuiuti do Paraná, Curitiba (PR), Brazil.
Patients receiving kidney transplants were enrolled in the study regardless of CRF cause, time of disease, time or type of previous treatment, and type of organ donor. All of them had been transplanted for at least ive months and at most 13 years. Patients presenting psychological, visual, or muscu-loskeletal disturbances that could hinder the examinations, as well as those with ear diseases and under the age of 13, were excluded from the study.
The sample included patients whose length of dialysis treatment prior to transplant ranged from one to 13 years (mean=6.77 years; SD=3.80 years). Eight patients had been through peritoneal dialysis (PD), 17 to HD, and five to both modalities.
Twenty-one patients had received transplants from living donors and nine from deceased donors, but the time between the death of the donor and the transplantation was not indi-cated on the medical records.
The length of hospital stay ranged from ive to 120 days (mean=26.60 days; SD=27.41 days), and the time of trans-plant varied from six months to nine years (mean=4.87; SD=2.37 years).
All patients selected were then submitted to anamnesis, otolaryngological and audiological evaluation, acoustic im-mittance, and central auditory processing testing.
Anamnesis
A questionnaire comprising audiological signs and symp-toms and family and personal history — based on the anamnesis protocol used by the Otoneurology Service — was applied to all participants. Information was, therefore, obtained from the participants’ or caregivers’ responses and from medical reports.
Otolaryngological evaluation
This was performed by an otolaryngologist, aimed at ex-cluding alterations that could interfere in certain tests.
Audiological evaluation
acoustically treated rooms to prevent interference from outside noises. An Itera Madsen GN Otometrics® audiometer was used,
gauged according to ISO 8253 standards, equipped with TDH-39 earphones and set by dBNA threshold levels. Some criteria were used to characterize the degree and type of hearing loss(8).
Afterward, hearing thresholds were assessed at high fre-quencies (9–16 kHz) with the use of Koss® HV/PRO earphones.
For the purpose of comparison, we used a control group from a previous study(9) which held 25 patients — 11 females (44%)
and 14 males (56%), aging 10 to 28 years old (mean=14.40 years; SD=4.06 years).
Acoustic immittance testing
This was performed to evaluate the eardrum and the ossicu-lar chain by assessing the tympanometric curve and the acoustic relex. Otolex impedance meter with TDH 39P earphones was used, and some criteria were used to interpret the results(10).
Central auditory processing evaluation
Patients underwent the Staggered Spondaic Word Test (SSW) and the Random Gap Detection Test (RGDT).
SSW is composed of 40 items subdivided into four groups of 10 items each. The irst and the fourth groups are applied separately to each ear, that is, without conlict, while the second and third groups are applied to both ears simultane-ously. Therefore, the test has four conditions: competitive right (CR), competitive left (CL), non-competitive right (NCR), and non-competitive left (NCL). There is an interval between conditions which allows for the patient’s verbal response. SSW was applied according to criteria proposed by authors(11), and the stimulus used in conduction was at
50 dBNS, the tritone average. Normality standard was set at 90%.
The RGDT consists of pure-tone pairs at the frequencies of 500 Hz, 1, 2, and 4 kHz, with interval between tones ranging from 0 to 40 ms (0, 2, 5, 10, 15, 20, 25, 30, or 40 ms) and of 4.5 ms between stimuli for patient’s response. The intervals between sound stimuli are random, and the procedure is re-peated for each frequency.
In all subtests, patients were informed that they would hear two very similar sounds and should raise one of their inger upon hearing one sound stimulus and two ingers upon hear-ing two sound stimuli. The test was presented at 50 dBNS in the frequencies tested in binaural conditions. The result cor-responded to the shorter interval at which the patient started identifying two stimuli, being calculated for each frequency tested. The test was carried out in compliance with criteria proposed in previous studies(12).
Statistical analysis
The Fisher’s exact test was used to analyze the association between variables — gender, age, length and type of treat-ment before transplant, type of donor, length of hospital stay post-transplantation, and time elapsed since transplant — and
the results. The level for null hypothesis rejection was set at 0.05 or 5%.
Tests comprising quantitative variables (age, length of treatment time elapsed since transplant and length of hospital stay after transplantation) were given two response catego-ries in order to enable statistical analysis, as summarized in tables. Finally, the Mann–Whitney test was used to compare threshold values.
RESULTS
Nobody from the study group had hearing complaints at anamnesis.
Fourteen patients (46.67%) presented alterations at audiom-etry and SSW testing, out of which ive (16.67%) had unilateral changes and nine (30%) bilateral; 16 patients (53.33%) had normal results. The most common change found at audiom-etry was lowering in the perception of the 6–8 kHz frequency range. At RGDT, two patients (6.67%) presented alterations and 28 patients (93.33%) were normal. At immittance testing, 20 patients (66.67%) had type A tympanometric curve for both ears, nine (30%) had type As tympanometric curve for both ears, and one patient (3.33%) had type Ad tympanometric curve for both ears. No difference was observed between the variable gender and the pure-tone audiometry tests (p=0.0632 for unilateral changes and p=0.1557 for bilateral changes), the SSW testing (p=0.4499 for unilateral changes and p=0.2871 for bilateral changes), and RGDT (p=0.4368).
The relation between age and bilateral changes at pure tone audiometry was considered to be signiicant. Patients under the age of 17 presented fewer changes than those above this age (Table 1). We found no association of the length of dialysis treat-ment with audiological changes in transplant recipients (Table 2).
Regarding the length and type of treatment prior to trans-plantation, no signiicant differences were found, that is, regardless of the length and type of treatment, changes may occur in audiological exams at the same proportion (Table 3).
The Fisher’s exact test showed a relation between the type of donor and bilateral changes at SSW testing (Table 4).
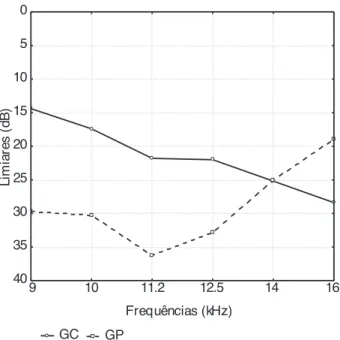
Descriptive results of hearing thresholds at high frequen-cies in both study and control groups are summarized in Table 5. Figures 1 and 2 show the comparison between mean high-frequency thresholds for both groups with regard to right and left ears, respectively. There was a signiicant difference between groups as to thresholds at 11.2 kHz (p=0.0456) and 16 kHz (p=0.0211) in the right ear and at 9 kHz (p=0.0074) and 11.2 kHz (p=0.0204) in the left ear.
When considering the gender, groups presented differ-ences at 16 kHz (p=0.0328) in right ears for males, at 10 kHz (p=0.0305) and 11.2 kHz (p=0.0403) in right ears for females, and at 9 kHz (p=0.0131) in left ears also for females.
DISCUSSION
Table 1. Association between age and threshold tonal audiometry results in Staggered Spondaic Word and Random Gap Detection tests for kidney transplant recipients
Test and age (years) Result p-value
Altered Normal Audiometry—unilateral
<17 2 12
0.1816
≥17 3 4
Audiometry—bilateral
<17 1 12
0.0033*
≥17 8 4
SSW—unilateral
<17 3 7
0.4502
≥17 2 9
SSW—bilateral
<17 5 7
0.4400
≥17 4 9
RGDT
<17 1 14
1.0000
≥17 1 14
*Significant values (p≤0.05)—Fisher’s exact test.
Legends: SSW = Staggered Spondaic Word Test; RGDT = Random Gap Detection Test; unilateral = unilateral changes; bilateral = bilateral changes
Table 2. Association between time of dialysis treatment and the results of threshold tonal audiometry results in Staggered Spondaic Word and Random Gap Detection tests for kidney transplant recipients
Test and time of treatment Results p-value Altered Normal
Audiometry—unilateral
<7 2 9
0.4502
≥7 3 7
Audiometry—bilateral
<7 3 9
0.2481
≥7 6 7
SSW—unilateral
<7 2 8
0.5498
≥7 3 8
SSW—bilateral
<7 4 8
0.5600
≥7 5 8
RGDT
<7 1 13
0.7241
≥7 1 15
Table 3. Association between type of dialysis treatment and threshold tonal audiometry results in Staggered Spondaic Word and Random Gap Detection tests for kidney transplant recipients
Test and type of treatment Result p-value Altered Normal
Audiometry—unilateral
Peritoneal dialysis 2 3
0.3298
Hemodialysis 2 10
Hemodialysis/peritoneal dialysis 1 3
Audiometry—bilateral
Peritoneal dialysis 3 3
0.4097
Hemodialysis 5 10
Hemodialysis/peritoneal dialysis 1 3
SSW—unilateral
Peritoneal dialysis – 5
0.2337
Hemodialysis 4 9
Hemodialysis/peritoneal dialysis 1 2
SSW—bilateral
Peritoneal dialysis 3 5
0.5573
Hemodialysis 4 9
Hemodialysis/peritoneal dialysis 2 2
RGDT
peritoneal dialysis 1 7
0.4444
hemodialysis – 17
hemodialysis / peritoneal dialysis 1 4
Table 4. Association between the type of donor and threshold tonal audiometry results in Staggered Spondaic Word and Random Gap Detection tests for kidney transplant recipients
Test and type of donor Results p-value
Altered Normal
Audiometry—unilateral
Living donors 2 13
0.1146
Deceased donors 3 3
Audiometry—bilateral
Living donors 6 13
0.5368
Deceased donors 3 3
SSW—unilateral
Living donors 4 14
0.5782
Deceased donors 1 2
SSW—bilateral
Living donors 3 14
0.0099*
Deceased donors 6 2
RGDT
Living donors 2 19
0.4828
Deceased donors – 9
Fisher’s exact test (p≤0.05). Only two treatment modalities were considered: peritoneal dialysis and hemodialysis (most common ones).
Legend: Unilateral = unilateral changes; Bilateral = bilateral changes Fisher’s exact test (p≤0.05).
Legend: Unilateral = unilateral changes; Bilateral = bilateral changes
*Significant values (p≤0.05)—Fisher’s exact test.
Legend: Unilateral = unilateral changes; Bilateral = bilateral changes
otologic symptoms such as tinnitus, dizziness, and hypoacusis. In the literature reviewed, the authors do not mention the patient’s length of hospital stay, so it was not possible to make a compari-son in this regard with the data obtained from the present study. Some papers(13–17) show that hearing loss is diagnosed in
loss in CRF patients is associated with extrinsic factors, such as ototoxic side-effects of uremia; ototoxic medications(14,17);
degree of hyponatremia(13); exposure to noises; presbycusis;
mumps; inherited dysacusis(14); exogenous and endogenous
factors(6); multifactors(18,19); Alport syndrome; age and exposure
to noise; vascular, electrolytic, and metabolic alterations; meta-bolic alterations secondary to renal failure and comprising hair cells; plasma viscosity; use of gentamicin in high-frequency hearing loss; endolymphatic hydrops in low frequency; and length of treatment(13–15).
A study(20) reported that hearing loss is neither related to
the use of ototoxic medications nor to inherited nephritis and that such loss cannot be reversed with improvement of uremia. Another study(17) stated that the cause is unknown; thus, so
it can be attributed to both CRF or HD. It is known that the kidney and the cochlear duct share some antigens; therefore, an autoimmune defect can occur. There are microscopic simi-larities in anatomy and in physiological, immunological, and pathological behavior of these organs, which suggests that a possible defect in electrolyte transport across cell membranes could be the cause of hearing loss(6,13).
In our study, we could not establish a relation between hear-ing loss and its possible causes in the group holdhear-ing 30 kidney transplant recipients. Although we have observed a higher frequency of hearing impairment in patients above the age of 17, it could be associated with many factors other than age.
The studied sample presented alterations at central auditory processing evaluation. The auditory processing disorder (APD) is known to be an alteration in the group of speciic auditory abilities on which individuals depend to discriminate what they hear. The auditory system integrity — peripheral or central — is a prerequisite for the acquirement and development of human communication regarding written and oral language abilities.
Table 5. Descriptive statistics of high frequency thresholds (dBNA) of both groups
Ear and frequency n Mean Minimum Maximum SD
Control group*
RE 9 kHz 25 14.40 0.00 25.00 5.27
RE 10 kHz 25 17.40 5.00 25.00 5.80
RE 11.2 kHz 25 21.80 10.00 40.00 7.48
RE 12.5 kHz 25 22.00 10.00 45.00 8.42
RE 14 kHz 25 25.20 15.00 45.00 7.14
RE 16 kHz 25 28.40 10.00 55.00 8.26
LE 9 kHz 25 15.20 10.00 25.00 4.67
LE 10 kHz 25 18.60 5.00 30.00 6.38
LE 11.2 kHz 25 19.20 10.00 30.00 5.53
LE 12.5 kHz 25 20.20 10.00 40.00 6.53
LE 14 kHz 25 21.20 10.00 50.00 8.69
LE 16 kHz 25 27.00 15.00 50.00 8.04
Study group
RE 9 kHz 30 29.67 0.00 95.00 28.19
RE 10 kHz 29 30.34 0.00 90.00 27.51
RE 11.2 kHz 29 36.21 10.00 85.00 25.20
RE 12.5 kHz 27 32.78 0.00 80.00 26.51
RE 14 kHz 23 25.00 0.00 60.00 21.95
RE 16 kHz 18 18.89 0.00 50.00 15.58
LE 9 kHz 30 33.17 10.00 90.00 26.80
LE 10 kHz 29 31.72 0.00 85.00 27.03
LE 11.2 kHz 29 37.76 0.00 85.00 26.58
LE 12.5 kHz 27 34.07 0.00 80.00 25.80
LE 14 kHz 23 27.17 0.00 60.00 21.15
LE 16 kHz 17 25.59 0.00 50.00 17.58
*Source: Bitencourt (2003)(9).
Legend: RE = right ear; LE = left ear; SD = standard deviation.
Legends: CG = control group; SG = study group
Figure 1. Comparison of high frequency thresholds between groups as to the right ear.
GC GP
9 10 11.2 12.5 14 16
Frequências (kHz) 0
5
10
15
20
25
30
35
40
L
im
ia
re
s
(d
B
)
Legends: CG = control group; SG = study group
Figure 2. Comparison of high frequency thresholds between groups as to the left ear.
GC GP
9 10 11.2 12.5 14 16
Frequências (kHz) 0
5
10
15
20
25
30
35
40
L
im
ia
re
s
(d
B
We found no published study about the abilities of the auditory processing. A study comprising the cognitive aspect concluded that that P300 was able to evaluate the cognitive function of CRF patients — even asymptomatic ones — and showed that PD can be a better treatment when it comes to prevention of cognitive impairments as compared to HD(21).
Some authors(22) showed a signiicant delay in the latency
of the I, III, and V waves and I–III and I–V interpeaks in the auditory steady state on the brainstem of CRF patients, which demonstrates central and peripheral involvement on the central nervous system (CNS).
The alteration found in SSW testing were related to dif-iculty in igure ability and binaural integration, that is, CRF patients struggled to receive and recognize information in both ears. This dificulty may onset in cases of pathologies involving the brainstem and connections. The CNS structures responsible for this ability are olivary complex, which is linked to both ears and compares sound characteristics between them, and the auditory brain cortex, which uses the differences in intensity and time of information reception to determine where the sound comes from(23).
In the present study, all participants with complaint of hearing impairment also presented changes in audiometry. Authors(24) have reported that hearing loss cannot be considered
determining to alterations in the hearing process, although it is a worsening factor. From this study, we can infer that central alterations could well be consequences of the hearing loss and of extrinsic and intrinsic factors.
The present study has reinforced the results of previous ones(13,22) that did not ind correlations between audiometric
indings and gender. The association of age with pure-tone audiometry, however, was signiicant: patients under 17 years were shown to have fewer alterations than those above 17 years. These data agree with the study by Yassin et al.(13) and disagree
with that by Jakic et al.(19). Other authors(7) have reported
sig-niicant differences in the hearing thresholds regarding age, where there is a gradual worsening in the hearing perception of high frequencies along with aging.
We did not ind a correlation between the type of treat-ment prior to transplant and audiological results, which agrees with data from other studies as to type(17) and
time(16,18,25) of treatment. Another study(26) reported a higher
prevalence of hearing loss among patients who received dialysis treatment for longer periods, even though it was not signiicant in comparison with other groups of patients. A study also reported an association between the time of renal disease and auditory threshold(27). According to Oda
et al.(4), 37.5% of their sample of patients who had
under-gone more than 264 HD sessions or had been transplanted presented auditory and vestibular symptoms; on the other hand, patients who had undergone less than 59 sessions had no hearing impairment.
A previous study(18) reported 75% of CRF patients without
any auditory changes along a 4-year follow-up. In another research(28) that considered the period of 6–26 months for the
normalization of blood chemical parameters, a regression of the hearing loss was found.
In the present study, the relation between time elapsed from the transplantation and the pure-tone audiometry, SSW, and RGDT was not signiicant. However, other studies(29) stated the
need for otologic follow-up for transplant recipients, for they use immunosuppressant medications (such as cyclosporine A and corticosteroids) that may cause changes in plasma viscosity and in the inner ear vascular system.
The effect of kidney transplant on the hearing function is controversial. It has been suggested that kidney transplant initially improves the hearing ability, but, in the long term, it worsens it(28). Some authors reported no improvement in
the hearing function after kidney transplantation(29), while
others stated that it resulted in improvement or stabilization of hearing loss(22).
According to Alves and Ribeiro(30), stabilization or even
slower progression of hearing loss is deemed understandable after kidney transplantation, since the hearing loss results from changes in basal membranes because of the damage caused to type IV collagen, their main constituent.
The association between the type of donor — living or de-ceased — and SSW, results was signiicant. The rate of changes in function was higher in cases of deceased donors, but there are no data in the literature to support this inding.
Moreover, the association between length of hospital stay after transplantation and pure-tone audiometry, SSW, and RGDT results was not signiicant. The literature reviewed could not support or confront this inding either.
At audiometry, we found a worsening of high-frequency thresholds in the study group when compared to the control group. The literature attests that high-frequency audiometry is an important resource for early diagnosis of hearing loss as much as for function monitoring. Some studies(7,16,29) reported
alterations in the examination of CRF patients and reinforce the importance of high-frequency audiometry for the early detection of ototoxicity.
A previous research(16) reported that all individuals
pre-senting hearing loss at pure-tone threshold audiometry also presented low thresholds at high-frequency audiometry. Our study corroborates these indings, although the results of high-frequency audiometry have been shown lower among patients with normal pure-tone audiometry results.
Histological studies have shown that hearing impairment starts from the basis of the cochlear duct and progresses to its apex; thus the hearing loss is initially identiied at higher fre-quencies. Therefore, auditory monitoring at high frequencies may detect ototoxicity before the frequencies of conventional audiometry are affected(15).
Finally, high-frequency audiometry is important for audi-tory monitoring in patients under ototoxic treatment (chemo-therapeutic or renal function conservation drugs) and aims to prevent permanent hearing impairment; many studies(6,7,29)
reinforce the clinical importance of this test for this purpose.
CONCLUSION
audiological evaluation at high frequencies and central auditory processing evaluation have shown evidence of changes; thus, there is a need to orient the professionals involved in the care of CRF patients who underwent kidney transplantation as to management, prevention, and early diagnosis of audiological changes.
*KFKDA was responsible for the data collection, bibliographical research, and writing; BSZ assisted in the data collection, bibliographical research, and inal review; PBNL assisted in the bibliographical research, writing, and inal review; LCS assisted in the writing and inal review; ALJ assisted in the writing and inal review; JMM assisted in the writing, statistical analysis (descriptive and analytical).
REFERENCES
1. Alport AC. Hereditary familial congenital haemorrhagic nefhritis. Br Med J. 1927;1(3454):504-6.
2. Romão Jr JE. Doença renal crônica: deinição, epidemiologia e classiicação. J Bras Nefrol. 2004;26(Supl.1)(3):1-3.
3. SBN – Sociedade Brasileira de Nefrologia. (2011) [Internet]. Censo dos centros de diálise no Brasil 2011. [cited 2011 out 5] Available from: http://www.sbn. org.br/pdf/censo_2011_publico.pdf
4. Oda M, Preeciado MC, Quick CA, Paparella MM. Labyrinthine pathology of chronic renal failure patients treated with hemodialysis and kidney transplantation. Laryngoscope. 1974;84(9):1489-506.
5. Matz GJ, Naunton RF. Ototoxic drugs and poor renal function. JAMA.1968;206(9): 2119.
6. Thomsen J, Bech P, Szpirt W. Otologic symptoms in chronic renal failure. The possible role of aminoglycoside – furosemide interaction. Arch. Otorhinolaryngol. 1976;214(1):71-9.
7. Zeigelboim BS, Mangabeira-Albernaz PL, Fukuda Y. High frequency audiometry and chronic renal failure. Acta Otolaryngol. 2001;121(2):245-8.
8. Davis H, Silverman RS. Hearing and deafness. 3ª ed. New York: Holt, Rinehart & Wilson; 1970. p. 253-79.
9 Bitencourt RF. Avaliação audiológica em indivíduos expostos a agentes quimioterápicos [dissertação]. Curitiba: Mestrado em Distúrbios da Comunicação, Universidade Tuiuti do Paraná; 2003.
10. Jerger J. Clinical experience with impedance audiometry. Arch Otolaryngol. 1970;92(4):311-24.
11. Borges ACLC. Dissílabos alternados – SSW. In: Pereira LD, Schochat E. Processamento auditivo central: manual de avaliação. São Paulo: Lovise, 1997. p. 169-78.
12. Keith RW. Random gap detection test.St. Missouri (USA): Auditec of Saint Louis, 2000.
13. Yassin A, Badry A, Fatt-Hi A. The relationship between electrolyte balance and cochlear disturbances in cases of renal failure. J Laryngol Otol. 1970;84(4):429-35.
14. Bergstrom L, Jenkins P, Sando I, English GM. Hearing loss in renal disease: clinical and pathological studies. Ann Otol Rhinol Laryngol. 1973;82(4):555-76.
15. Pérez Garrigues H, Clemente J M. Chronic renal insuficiency and auditory system. An Otorrinolaringol Ibero Am. 1987;14(6):635-44. 16. Morton LP, Reynolds L, Zent R, Rayner BL. Hearing thresholds in CAPD
patients. Adv Perit Dial. 1992;8:150-2.
17. Nikolopoulos TP, Kandiloros DC, Segas JV, Nomicos PN, Ferekidis EA, Michelis KE, et al. Auditory function in young patients with chronic renal failure. Clin Otolaryngol Allied Sci. 1997;22(3):222-5.
18. Henrich WL, Thompson P, Bergstrom LV, Lum GM. Effect of dialysis on hearing acuity. Nephron. 1977;18(6):348-51.
19. Jakic M, Mihaljevic D, Zibar L, Jakic M, Kotromanovic Z, Roguljic H. Sensorineural hearing loss in hemodialysis patients. Coll Antropol. 2010;34(1):165-71.
20. Alder D, Ritz E. Terminal renal failure and hearing loss. Arch Otorhinolaringol. 1982;235(2-3):587-90.
21. Tilki HE, Akpolat T, Tunali G, Kara A, Onar MK. Effects of haemodialysis and continous ambulatory peritoneal dialysis on P300 cognitive potentials in uraemic patients. Ups J Med Sci. 2004;109(1):43-8.
22. Bains KS, Chopra H, Sandhu JS, Aulakh BS. Cochlear function in chronic kidney disease and renal transplantation: a longitudinal study. Transplant Proc. 2007;39(5):1465-8.
23. Bonaldi LV, Angelis MAA, Smith RL. Hodologia do sistema auditivo. In: Pereira LD, Schochat E. Processamento auditivo central: manual de avaliação. São Paulo: Lovise, 1997. p. 19-25.
24. Diveyi PL, Haupt KM. Audiological correlates of speech understanding deicits in elderly listeners with mild to moderate hearing loss. Ear Hear. 1995;18:19-32.
25. Thodi C, Thodis E, Danielides V, Pasadakis P, Vargemezis V. Hearing in renal failure. Nephrol Dial Transplant. 2006;21(11):3023-30.
26. Bazzi C, Venturini C, Pagani C, Arrigo G, D’Amico G. Hearing loss in short and long-term haemodialyzed patients. Nephrol Dial Transplant. 1995;10(10):1865-8.
27. Lasisi AO, Salako BL, Kadiri S, Arije A, Oko-Jaja R, Ipadeola A, et. al. Sudden sensorineural hearing loss and hemodialysis. Ear Nose Throat J. 2006;85(12):819-21.
28. Mitschke H, Schmidt P, Kopsa H, Zazgornik J. Reversible uremic deafness after successful renal transplantation. N Eng J Med. 1975;292(20):1062-3.
29. Sefer S, Trotic R, Lacmanovic V, Degoricija V, Ratkovic-Gusic I, Kes, P. Effects of renal transplantation on hearing and ocular changes in a monozygotic twin with Alport´s syndrome: comparasion with other twin on hemodialysis. Croat Med J. 2000;41(2):203-6.