www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Positioning
of
earphones
and
variations
in
auditory
thresholds
夽
,
夽夽
Bettina
Poggi
Almeida
a,
Pedro
de
Lemos
Menezes
b,∗,
Kelly
Cristina
Lira
de
Andrade
c,
Cleide
Fernandes
Teixeira
daEspecializac¸ãoemFonoaudiologiadoTrabalho,UniversidadeEstadualdeCiênciasdaSaúdedeAlagoas(UNCISAL),
MarechalDeodoro,AL,Brazil
bFísicaAplicadaàMedicinaeBiologia,UniversidadeEstadualdeCiênciasdaSaúdedeAlagoas(UNCISAL),MarechalDeodoro,AL,
Brazil
cSaúdedaComunicac¸ãoHumana,UniversidadeFederaldePernambuco(UFPE),Recife,PE,Brazil dSaúdeColetiva,UniversidadeFederaldePernambuco(UFPE),Recife,PE,Brazil
Received19June2014;accepted4October2014
Availableonline8September2015
KEYWORDS
Pure-tone audiometry; Auditorythreshold;
Occupationalhealth
Abstract
Introduction:Oneoftheproblemsobservedinpure-toneaudiometrytonalhasbeenthe varia-tionintestresultsofasameindividual,particularlyatfrequenciesof4kHz,6kHzand/or8kHz. Improperplacementofheadphonesisoneofthefactorsthatcancausealterationsinresults. Objective:Tocomparedifferences inauditory thresholdsusingearphonespositioned bythe examinerandbytheworker.
Methods:Clinicalandexperimentalstudyconductedin2009,with324workersagedbetween 19and61years,withameanof33.29yearsandmeanexposuretimeof7.67years.Allsubjects werefamiliarwithaudiometryprocedures.Auditorythresholdswereobtainedatfrequencies of0.25---8kHz,with earphonespositioned bytheexaminers,andatfrequencies of4,6and 8kHz,withearphonesplacedbyworkersinacomfortableposition,followingtheexaminer’s instructions.Thethresholdsobtainedinthesetwosituationswerecompared.
Results:Thethreefrequenciesexhibitedbetterresponseswithearphonesplacedbythe work-ersthemselves(p<0.001).Atafrequencyof8kHzagreaterdifferencewasfound(p<0.001), withameanof13.89dBandstandarddeviationof6.07dB.
夽
Pleasecitethisarticleas:AlmeidaBP,MenezesPL,deAndradeKCL,TeixeiraCF.Positioningofearphonesandvariationsinauditory thresholds.BrazJOtorhinolaryngol.2015;81:642---6.
夽夽
Institution:UniversidadeFederaldePernambuco(UFPE),Recife,PE,Brasil.UniversidadeEstadualdeCiênciasdaSaúdedeAlagoas (UNCISAL),MarechalDeodoro,AL,Brasil.
∗Correspondingauthor.
E-mail:[email protected](P.d.L.Menezes).
http://dx.doi.org/10.1016/j.bjorl.2015.08.016
1808-8694/©2015Associac¸ãoBrasileiradeOtorrinolaringologia eCirurgiaCérvico-Facial. PublishedbyElsevierEditoraLtda.All rights
Conclusion: Earphoneplacementbytheworkersthemselvesundersupervisionoftheexaminer resultsinimprovedmean auditorythresholdsatfrequenciesof4,6and8kHz, thelastone significantlyhigherthantheothertwo.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Audiometriadetons
puros;
Limiarauditivo;
Saúdedotrabalhador
Oposicionamentodosfonesdeouvidoeasvariac¸õesdoslimiaresauditivos
Resumo
Introduc¸ão: Umdosproblemasobservadosnaaudiometriatonaléavariac¸ãonosresultados detestesdeummesmoindivíduo,sobretudonasfrequênciasde4,6e/ou8kHz.Acolocac¸ão indevidadosfoneséumdosfatoresquepodemcausaralterac¸õesnosresultados.
Objetivo: Compararasdiferenc¸asnoslimiaresauditivoscomosfonesposicionadospelo exam-inadorepelopaciente.
Método: Estudoclínicoeexperimentalrealizado,em2009,com324trabalhadores,comidade entre19e61anos,médiade29,33anosetempomédiodeexposic¸ãoaoruídode7,67anos;todos familiarizadoscomosprocedimentosdaaudiometria.Oslimiaresauditivosforamobtidosnas frequênciasde0,25a8kHz,comosfonescolocadospelosexaminadores;enasfrequênciasde 4,6e8kHzcomosfonescolocadospelostrabalhadoresemposic¸ãodeconforto,soborientac¸ão doexaminador.Oslimiaresobtidosnasduassituac¸õesforamcomparados.
Resultados: As três frequências apresentaram melhores respostas com os fones colocados pelosprópriosindivíduos(p<0,001).Nafrequênciade8kHzfoiencontradaamaiordiferenc¸a (p<0,001),commédiade13,89dBedesviopadrãode6,07dB.
Conclusão:Acolocac¸ãodosfonesdeouvidopelosprópriostrabalhadores,sobsupervisãodos examinadores,resultanamelhoradoslimiaresauditivosmédiosnasfrequênciasde4,6e8kHz, sendoestaúltimasignificativamentemaiorqueasdemais.
©2015Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Since pure-tone audiometry depends directly on the
responseofthe individual,a numberofvariablesmust be
controlledduringthe process.Itmust beconductedusing
standardizedcriteria,suchasthecabinandequipmentduly
calibrated according toRegulatoryGuideline No.7(NR7),
annex I,itemII, amended by Decree No. 19,of April 19,
1998,oftheDepartmentforWorkHealthandSafetyofthe
Ministry of Labor andEmployment.1 Thus, it is indispens-ablethattherebeanintervalbetweentonestopreventthe possibleeffectsofatemporarychangeinthresholdfrom fal-sifyingtheresultsofsequentialaudiograms,whichprovide dataonprogressivehearinglossovertime.2
Oneoftheproblemshasbeenthevariationinpure-tone auditorythresholdsobserved,relatedtothechangeintest resultsofasameindividual,particularlyatfrequenciesof 4kHz,6kHz,and/or8kHz.Itisimportanttounderscorethat since1965,anumberofauthorshaveshownthatinstability inhearingtestresultscanbeprovokednotonlybyfactors intrinsictotheindividual,butalsobythoserelatedtothe methodologyadopted.3---6
The inadequate placement of earphones may cause erroneous alterations in results, owing to discomfort and consequentlackofattentionpaidbytheworkersthemselves and/oreffectofthispoorpositioningonacutefrequencies
whenthesupra-auralphoneexertspressureontheauricular pavilion.7Additionalfactorsmayalsoaffectthevalidityand reliabilityoftheaudiogram,suchaslackofequipment cali-bration,inappropriatetest setting, positionoftheworker during the test, inadequateinstructions, false responses, andthelearningeffect.8
Studies that show the variability of audiometric test results between the exams of a same individual, mainly for frequencies between 4kHz and 8kHz, remain scarce. Somestudiescomparevariationsinaudiometricthresholds between genders, age, time of employment, and occu-pational function.9 When the test is aimedat monitoring occupationalhearing,itisimportantthatthisvariabilitybe minimizedbyobtainingaccurateresults,inordertoavoid inaccuratehearinglossmeasurement, therespective con-sequence for the worker, and the costs of work-related injuries.
comparison analysis defined by this Decree considers as suggestiveoftriggeringand/or worseningofnoise-induced hearing loss (NIHL) whenever comparison between the sequentialandreferencetestsshowsadifferencebetween meanauditory thresholds, at frequencies of 3kHz; 4kHz, and/or6kHzgreaterthanorequalto10dBHL,orworsening bymorethan15dBHL.1AccordingtotheDecree,thisisan indicator that adverse conditions in the environment are notcontrolledandthatpreventiveactionsmustbetaken.
Inthis context,differentsequential test results hinder comparativeanalysis,andmayindicatediscrepantfindings thatprecludeconclusiveanalysisortriggeringorworsening of hearing loss notcompatible withreality, and does not reflecttheefficacyofthehearingprotector.Itisimportant tohighlightthattheaudiometrictestisusedtopreservethe healthofexposedworkers,anditisadecisivedocumentin employeehiringorjudicialdisputesinvolvinghearing dam-age.
Since 1974,10 the Department of Labor of the United States (Occupational Safety and Health Assessment) has stressedtheimportanceofaudiometricretestsasamethod ofcontrollingpossibleerrorsindetecting auditory thresh-olds,suggestingimmediatereassessmenttoensurereliable resultsthatdonotcompromisetheefficacyofauditory mon-itoring,alsofavoringcompaniesthatuseasafetyandhealth managementsystembasedoninternationalstandardssuch asOHSAS18001.
Thus, the aim of the present study was to compare pure-tone auditory thresholds, obtained by workers who positioned the earphones themselves, as per instructions fromtheaudiologist,withthoseobtainedwhenearphones wereplaced solely by the health-careprofessional. Addi-tionally,thestudyaimedatobservingvariationsinauditory thresholdsobtainedafterasecondassessment.
Methods
This is a cross-sectional study conductedat twofacilities specializedinoccupationalaudiologyandconsultancyinthe fieldofworkerhealthinRecife,Brazil.Thesamplewas com-posedof324workers(bothsexes)fromawiderangeofjob areas (callcenters, printing, transport,food, steel, port, security,drivers,furniture,hydroelectric,amongothers).
To avoid selection bias, individuals whose audiograms showedconductiveormixedhearingalterationsand/or pre-sentedwithvisiblecollapseoftheexternalacousticmeatus (EAM)wereexcluded.Audiograms wereconsiderednormal whenauditorythresholdwaslessthanorequalto25dB(dB HL).1Furthermore,workersenrolledinahearingloss pre-ventionprogram,withmorethanoneaudiogramperformed, andwithacomparisonofresultsshowingresponsevariations wereselected.
Todeterminetheauditorythresholdsofthe experimen-talgroup,thedescendingtechniqueat10dBintervalswas useduntiltheindividualnolongerrespondedtothesound. Atthisintensity,theascending techniqueat 5dBintervals wasuseduntiltheindividual couldonceagaindetect the sound.Inthefirsttest,oneoftheparticipantswasassessed atfrequenciesbetween0.25kHzand8kHz,withaminimum restperiodof14h.The samecriteriawereadoptedinthe secondtest,butonlyfrequenciesbetween4kHzand8kHz
were assessed. Aduly calibrated GSI-64 audiometer, with TDH-50 earphones was used in the experiments, in addi-tiontopriorinspectionoftheexternal auditorycanaland tympanicmembrane,excludingcasesofearwaxblockage.
Earphoneswereplacedalternatelyintestsoneandtwo. Forthefirstworker,intestone,theearphoneswereplaced by the examiner, while in test two they were placed by theworker,underguidanceoftheexaminer.Theorderwas reversedfor thenextworker.Test andretestresultswere comparedforintensityindBHLandfrequency,beforeand afterearphonerepositioning.
Theorderoffrequencypresentation,choiceofear,and orderofretestwererandomforeachindividual,inorderto eliminateinterferencefromtirednessandlearning.
Dataanalysis wasconducted by absolute and percent-agedistributionofdescriptivestatisticsmeasures,usingthe pairedStudent’st-testwithunequalvariances.The hypoth-esisofequalvarianceswascarriedoutusingLevene’sF-test. Finally,ANOVAwasappliedtotestdifferencesbetween fre-quencies,andTukey’stestforpairwisecomparisonwasused inordertoobservepossiblesignificantdifferencesbetween thefrequenciesstudied.Asignificancelevelofp<0.05was establishedusingSPSSv.21.Thestudywasapprovedbythe EthicsCommittee,underregistrationNo.199/09.
Results
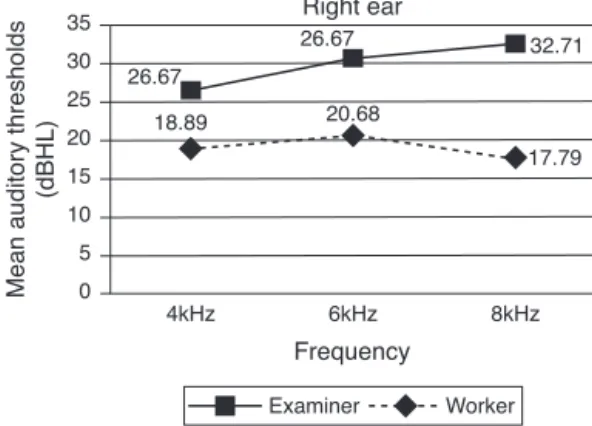
Participants were aged between 19 and 61 years, with a mean of 33.29 years and standard deviation of 10.41. Most (65.1%) had completed secondary school. Analysis ofaudiometric distribution,afterconfirmationof auditory thresholds,revealedthat75%exhibitedauditorythresholds within the normal range and 25% had an altered thresh-oldin at least oneof the frequencies. Auditorythreshold distribution by frequency,comparing the first andsecond exam,irrespectiveofwhoplacedtheearphones,showedno statisticallysignificantdifferences,withap-valueof0.456. The distribution of mean auditory thresholds in the experimental group between tests and retests, for both ears,wasbetterafterearphoneswererepositionedbythe workersthemselves, withagreater differenceinintensity levelforafrequencyof8kHz,asshowninFigs.1and2.
Student’s t-test for independent samples was applied to the results of both ears and showed no significant
35
26.67
26.67 32.71
17.79 20.68
18.89 30
25 20 15 10 5 0
4kHz 6kHz
Examiner Worker
Frequency Right ear
Mean auditory thresholds
(dBHL)
8kHz
Figure 1 Distribution of mean auditory thresholds in the
35 40
30.01 32.52 30.69
17.21 17.21
21.82 30 25 20 15 10 5 0
4kHz 6kHz
Examiner Worker
Frequency
Left ear
Mean auditory thresholds
(dBHL)
8kHz
Figure 2 Distribution of mean auditory thresholds in the
experimentalgroupbetweentestsandretestsintheleftear.
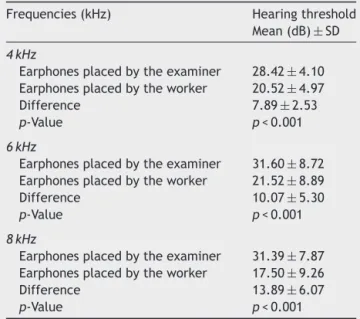
Table 1 Mean standard deviation of altered and nor-mal audiograms according to individual who placed the earphones.
Frequencies(kHz) Hearingthreshold Mean(dB)±SD
4kHz
Earphonesplacedbytheexaminer 28.42±4.10 Earphonesplacedbytheworker 20.52±4.97
Difference 7.89±2.53
p-Value p<0.001
6kHz
Earphonesplacedbytheexaminer 31.60±8.72 Earphonesplacedbytheworker 21.52±8.89
Difference 10.07±5.30
p-Value p<0.001
8kHz
Earphonesplacedbytheexaminer 31.39±7.87 Earphonesplacedbytheworker 17.50±9.26
Difference 13.89±6.07
p-Value p<0.001
differences (p>0.2). Thus, results were obtained for
frequency,irrespectiveofwhichearwastested.
Finally,theStudent’st-testforpairedsamples,appliedto theresultsobtainedwiththeearphonesplacedbythe
exam-iner,andthosewiththeearphonesplaced bytheworkers
themselvesaccordingtoexaminerinstructions,showed sta-tisticaldifferencesforthethreefrequenciesstudied,with p-value<0.001,asshowninTable1.
TheANOVAtestrevealedtheexistenceofstatistically sig-nificantdifferencesinfrequenciesdependingonwhoplaced the earphone (p<0.001). Tukey’spost hoc test, however, revealedsignificantlygreaterdifferencesfor8kHzthanfor thetwoothersunderstudy.
Discussion
Thefirstpointtodiscussisthechoiceoffrequencies ana-lyzed.Itwasdecidedtostudyonly4kHz,6kHz,and8kHz,
sincethey exhibit shorter wavelengths and are therefore more susceptible to interference because of earphone placement.Moreover, two of these,4kHz and 6kHz, are veryimportantin determining noise-inducedhearingloss, according to Brazilian labor law (INSS/DAF/DSS No. 608, of August 5, 1998), whose text states that hearing loss predominatesatfrequenciesof6000,4000,and/or3000Hz, progressingslowlyat8000,2000,1000,500,and250Hz.11
The fact that workers are familiar with the annual audiometrytest proceduresand have high education lev-elsmayhave minimized possible sample selection biases. Furthermore, the literature contains many studies that showno differences between auditory thresholds in tests andretests,when variablesarecontrolledbyfamiliarized workers, or when different earphones are placed by the examiner.12 Similarly, the results obtained in the present studyshowednostatisticallysignificantdifferencesbetween testsandretests,irrespectiveofwhoplacedtheearphones. However,thepresent study sought toensure earphone comfort when placed by the workers themselves, a key determinantfor better soundtransmission at short wave-lengths, enhanced attention, and consequently improved auditorythresholds.4---6
Inthisrespect,thefindingsofthepresentstudy corrob-oratethoseobtainedinaclinicalstudyshowingsignificant differencesinaudiologicaltestsandretestsalsoat frequen-ciesof6kHzand8kHz,10andinotherstudiesdemonstrating collapseofthe externalacousticmeatusduetopoor ear-phoneplacement.13---16
The differences found between the two forms of ear-phoneplacement,inthetwodifferenttests,variedbetween 7.89dBand13.89dB,corroboratingstudieswiththesame frequencies, which found differences between 15dB and 20dBforhigh-pitchedsounds.17,18
Finally,inrelationtotheothertwofrequenciesstudied, thedifferences in the 8kHz frequency,which reached an average of 13.89dB, may be related toits shorter wave-length,because the higher the frequency,the shorter its wavelengthand the greater theinterference, due to col-lapseorpoorearphoneplacement.8
AccordingtoMinistryofLaborDecree19,avariationof 10dBor15dBmustbeconsideredwhencomparingbetween reference and sequential tests, since it indicates a sig-nificant change in auditory threshold,either triggering or exacerbating the disease; i.e., it allows the physician to inferthattheindividualisbecomingill.Thus,afalseresult compromisesthepreventionprogramestablishedby compa-niestoreducethenumberofaccidents,especiallythoseput inpracticeinahealthandsafetymanagementsysteminthe workplacebasedoninternationalstandards,suchasOHSAS 18001.Theseinternationalstandardsusetoolsto systemat-icallycontrol andimprovehealth and safetyperformance levelsatwork.1
Thus,contradictoryresultsbetweensequentialand ref-erence tests must be avoided, since they may lead to incorrectinterpretationsof workerhealth,efficacy ofthe NIHL,andaccidents,withalltheconsequencesthatthese aspectsrepresenttoworkersandthecompany.
company.AccordingtotheBrazilianSocialSecurityInstitute (Instituto Nacional do Seguro Social [INSS]), work-related hearinglossrepresentsatechnicalepidemiologicallink, sug-gestingthatthedegreeofworkplacesafetyinacompanyis notsatisfactory,which couldincrease social security con-tributionsrelatedtoenvironmentalrisk.
Finally,giventhelimitationsofthepresentstudy,owing tothespecificgroupofworkers,theirfamiliarizationwith theexam,andhigheducationlevels,cautionmustbe exer-cisedwhengeneralizingtheresultstoothergroups.
Conclusion
Earphone placement by workers, under examiner super-vision, resulted in better mean auditory thresholds at frequenciesof 4kHz, 6,kHz,and 8kHz,the latter signifi-cantlyhigherthantheothertwo.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Brasil. Ministério do Trabalho e Emprego. Secretaria de
Seguranc¸a e Saúde no Trabalho. Portaria n◦ 19, de 09 de
abril de 1998. Brasília: Ministério do Trabalho e Emprego;
1998. Available from: http://portal.mte.gov.br/data/files/
FF8080812BE914E6012BEEB7F30751E6/p1998040919.pdf
[cited17.06.14].
2.OlivaFC,MorataTC, Lacerda ABM,SteinmetzL, BramattiL, VivanAG,et al. Mudanc¸a significativadolimiar auditivo em trabalhadores expostosa diferentesníveisde ruído.RevSoc BrasFonoaudiol.2011;16:260---5.
3.AmaralLKM,FerreiraFHV,DiasFAM.Utilizac¸ãodeumamanobra específica para evitar alterac¸ões dos limiaresauditivos cau-sadaspelocolabamentodomeatoacústicoexterno.RevCEFAC. 2008;10:409---15.
4.FletcherJL.Reliabilityofhigh-frequencythresholds.JAudRes. 1965;5:133---7.
5.Northern JL, Downs MP, Rudmose W, Glorig A, Fletcher JL.Recommendedhigh-frequencyaudiometrythreshold level (8000---18000Hz).JAcoustSocAm.1971;52:585---95.
6.SchechterMA,FaustiAS,RappaportBZ,FreyRH.Age catego-rizationofhigh-frequencyauditorythresholddata.JAcoustSoc Am.1986;79:767---71.
7.SteffaniJA,GergesSNY,JanuárioAC.AInfluênciadaposic¸ão decolocac¸ãodofonenaobtenc¸ãodoslimiaresauditivos.Acta AWHO.2002;21:3---4.
8.MenezesPL,CabralA,MoraisLS,RochaL,PassosV.Ressonância: umestudodaorelhaexterna.Pró-fono.2004;16:333---40.
9.SantosJD,FerreiraMIDC.Variac¸ãodoslimiaresaudiométricos emtrabalhadoressubmetidosaruídoocupacional.ArqInt Oto-rrinolaringol.2008;12:201---9.
10.Occupational Safety and Health Administration. Pro-posed requirements and procedures: OSHA, Fed Reg. 1974;39:37774---8.
11.Brasil.InstitutodeSeguridadeSocial.OrdemdeServic¸oNo608
INSS/DSSN◦ 329,de05/8/1998.Normatécnicasobreaperda
auditivaneurossensorialporexposic¸ãocontinuadaaníveis
ele-vadosdepressãosonoradeorigemocupacional.DiárioOficial
daUnião,19deagostode1998.
12.StuartA,StenstromR,TompkinsC,VandenhoffS.Test---retest variability in audiometric threshold with supraaural and insert earphones among children and adults. Audiology. 1991;30:82---90.
13.Campos CF, Cruz MS, Feniman MR. Colabamento do meato acústicoexterno: ocorrênciaem trabalhadoressubmetidos à avaliac¸ão audiológica e otorrinolaringológica no CEDAUVI -USP/Bauru.JBrasFonoaudiol.2004;18:1.
14.ChaiklinJB,McClellanME.Audiometrymanagementof collaps-ibleearcanals.ArchOtolaryngol.1971;93:397---407.
15.ToniossoS, RedondoMC, LopesFilho O. Alterac¸ões dos limi-aresauditivoscausadospelocolabamento demeatoacústico externo.RevBrasOtorrinolaringol.2000;66:652---8.
16.Yonesaki CA. Influência do posicionamento dos fones na audiometriatonal[Dissertation].SãoPaulo(SP):Pontifícia Uni-versidadeCatólicadeSãoPaulo;2000.
17.Almeida EOC, NishimoriAY. Influência do posicionamento do fonenaaudiometriadealtafrequência.RevBras Otorrinolarin-gol.2006;72:691---8.