w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Sensory
disturbance
and
polyneuropathy
in
rheumatoid
arthritis
patients
with
foot
deformity
Ebru
Karaca
Umay
∗,
Eda
Gurcay,
Pinar
Bora
Karsli,
Aytul
Cakci
PhysicalMedicineandRehabilitationClinic,AnkaraDiskapiYildirimBeyazitEducationandResearchHospital,Ankara,Turkey
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received8October2014 Accepted2March2015
Availableonline8September2015
Keywords:
Rheumatoidarthritis Foot
Polyneuropathy Functionality
a
b
s
t
r
a
c
t
Introduction:Ouraiminthisstudywastopresenttheresultsofsensoryevaluationtestsand electrophysiologicalevaluationsinrheumatoidarthritis(RA)patientswithfootdeformity andtodeterminetheirrelationwithgeneralhealthstatusandlowerextremityfunctionality.
Materialsandmethods:Fifty-onepatientswithRAdiagnosisandfootdeformitywereincluded inthestudy.Demographicanddiseasecharacteristicsofthepatientswererecorded,anda detailedneurologicalexaminationwasperformed.Superficialsensation,pain,heat, vibra-tion,andtwo-pointdiscriminationsensationwereevaluatedineachfoot,andtheirsumwas usedtodeterminethesensorydeficitsindex(SDI)of0–10.Thepresenceofpolyneuropathy wasevaluatedwithelectrophysiologicalmethods.TheHealthAssessmentQuestionnaire andmobilityandwalkingsubscalesoftheArthritisImpactMeasurementScales-2wereused toassessgeneralhealthstatusandlowerextremityfunctionality,respectively.Accordingto thesensoryexaminationandelectromyographyresults,patientswerecomparedinterms oftheirgeneralhealthstatusandlowerextremityfunctionalstatus.
Results:Sensorydisturbancewasdetectedin39patients(74%)duringtheexamination; how-ever,27patients(52.9%)hadpolyneuropathydeterminedelectrophysiologically.Inpatients withsensorydeficits,statisticallysignificantdeteriorationwasdetectedingeneralhealth andfootfunctionality,includingmobilityandwalking,whencomparedtopatientswitha normalsensoryevaluation.
Conclusions: Eveninthepresenceofnormalelectrophysiologicaltests,sensory dysfunc-tionaloneseemstobeassociatedwithseveredisabilityingeneralhealthstatusandfoot functionalitywhencomparedtopatientswithanormalsensoryexamination.
©2015ElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](E.KaracaUmay).
http://dx.doi.org/10.1016/j.rbre.2015.08.010
Perturbac¸ões
sensitivas
e
polineuropatia
em
pacientes
com
artrite
reumatoide
com
deformidade
do
pé
Palavras-chave:
Artritereumatoide Pé
Polineuropatia Aspectofuncional
r
e
s
u
m
o
Introduc¸ão: Oobjetivodesteestudofoiapresentarosresultados dostestesdeavaliac¸ão sensitivaeexameeletrofisiológicoempacientescomartritereumatoide(AR)com deformi-dadedopéedeterminarasuarelac¸ãocomoestadogeraldesaúdeeaspectofuncionaldos membrosinferiores.
Materiaise métodos: Foram incluídosno estudo51 pacientescom diagnósticode ARe deformidadedopé.Foramregistradasascaracterísticasdemográficasedadoenc¸adecada indivíduo,efoirealizadoum exameneurológicodetalhado.Foiavaliadaa sensibilidade superficial,sensibilidadedolorosa,sensibilidadetérmica,sensibilidadevibratóriaeaplicado otestedediscriminac¸ãodedoispontosemcadaumdospés,easomadosescoresfoiusada paradeterminaroíndicededéficitssensitivos(IDS)de0-10.Apresenc¸adepolineuropatia foiavaliadacommétodoseletrofisiológicos.FoiutilizadooHealthAssessment Question-naireeassubescalasmobilidadeedeambulac¸ãodaArthritisImpactMeasurementScales-2 paraavaliaroestadogeraldesaúdeeoaspectofuncionaldemembrosinferiores, respec-tivamente.Deacordocomosresultadosdosexamesdeeletromiografiaedesensibilidade, ospacientesforamcomparadosemrelac¸ãoaoseuestadogeraldesaúdeeestadofuncional demembrosinferiores.
Resultados: Foramdetectadosdistúrbiossensitivosem39pacientes(74%)duranteoexame; contudo,27deles(52,9%)tinhampolineuropatiadeterminadaeletrofisiologicamente.Em pacientescom déficitssensitivos,foi detectadadeteriorac¸ão estatisticamente significa-tiva noestado geraldesaúdeeno aspectofuncionaldopé, inclusivenamobilidadee deambulac¸ão,quandocomparadosaospacientescomumaavaliac¸ãosensitivanormal.
Conclusão: Mesmonapresenc¸adetesteseletrofisiológicosnormais,adisfunc¸ãosensitiva isoladapareceestarassociadaaincapacidadegravenoestadogeraldesaúdeenoaspecto funcionaldopéemcomparac¸ãoapacientescomumexamesensitivonormal.
©2015ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Rheumatoidarthritis(RA)isachronic,systemicand inflam-matory disease with involvement of the peripheral joints, and its etiology cannot be understood completely despite the many new developments. It causes joint destruction, decreasedlifequalityandshortenedlifeexpectancy.1
The joints of the hand are the most frequentand ini-tiallyaffectedinarthritis;thus,studiesintheliteraturehave focusedmostly on hand deformitiesand hand disabilities. Whilefootinvolvementattheonsetofthediseasehasbeen reported in 16–20% ofpatients, this ratio may increase to approximately95%overthecourseofthedisease.2,3
Synovialhypertrophyandcapsulartensiongeneratedby hyperplasia, ligamentous laxity, muscular imbalance, and ultimately joint subluxationand dislocation playa role in thedevelopmentoffootdeformitiesinRA.Further,withthe directeffectofinflammation,destructionoccursinthe carti-lageandpericapsularstructures.4Duetoallthesechanges,the
loadingonjointscausesdifferentdeformitiesandconstitutes a severe disability inthe patient’s mobility and functional independence.5,6
Nervous system involvement in RA is often in the formofperipheralinvolvement.7Entrapmentneuropathies,
mononeuropathies, and sensory and sensorimotor axonal
polyneuropathies areconsidered inthis context.In clinical practice, superficialtouch,pain, heat, and vibrationsenses withthetwo-pointdiscriminationtest,musclestrength mea-surement,deeptendonreflexestests,andelectrophysiological methodsareusedfortheassessmentoftheperipheral ner-voussystem.Studiesinvestigatingthepresenceofneuropathy in RA patients have frequently used electrophysiological methodsintheirevaluations.7–10
Although sensory evaluation tests are often subjective tests,inrecentyears,itisreportedthattheinvolvementof theothernervefiberscanbeshownwiththesetests.11
Whileinsomestudiestheywerereportedthata correla-tionbetweendeteriorationinqualityoflifeandfunctionality, andfootcomplaintsinRA,12,13thereisnostudycomparing
thesensoryexaminationandelectrophysiologicalassessment findingsorevaluatingtherelationshipbetweentheseandthe patient’sgeneralhealthstatusandlowerextremity function-ality.
Footdeformitiesinpatientsmaybeonlyvisiblepartofthe icebergandmuchmoreitsbelow.Evenifeffectivetreatment wasgivenforthepatient’sdeformity,functionalityandquality oflifemaynotbeenoughimprovementduetonervoussystem involvement.
functionalityand generalhealthstatusinRApatientswith footdeformity.
Material
and
methods
Studypopulation
ThisstudywasconductedbythePhysicalMedicineand Reha-bilitationclinicinAnkaraDiskapiYildirimBeyazitEducation andResearchHospitalinAnkara,Turkey.
Fifty-onepatients aged35–65 years withfoot deformity anddiagnosedas RAaccording totheAmerican Collegeof Rheumatology(ACR)1990classificationcriteriawereincluded inthisstudy.
Only housewives and female patients with no salaried employmentwereincludedbecauseoffootinvolvementinRA wasreportedas89–90%inalmostequalratesinbothgenders14
andtoensurehomogeneityintermsoffunctionalstatusof patients.
Exclusioncriteriaofthestudywereasfollows:ageunder 16 years and over 65 years,male gender, lower extremity traumaand/orhistoryofoperation,diabetesmellitus,acute and/or chronic liver and kidney disease, severe heart fail-ure,hypo/hyperthyroidism,amyloidosis,malignancy,vitamin B12deficiency,additionalconnectivetissuedisease,suchas Sjögren’ssyndrome,and/orvasculitissymptoms,previously diagnosedperipheralnervoussysteminvolvement,and posi-tivepathologicalreflexes.Alsoexcludedfromthestudywere patientsusingmorethan7.5mgcorticosteroidoverthelast sixmonthsorbiologictherapy.
Ourpatientsonbiologic therapyrepresentedlate-period diseaseandalsofitotherexclusioncriteria,suchasmostly high-dosecorticosteroiduseanddiabetesmellitus.
Atbaseline,patientswereinformedaboutthestudyand theirwritteninformedconsentwasobtained.Theapproval ofthehospital’slocalethicscommitteewasreceivedbefore thestudy.Thestudywasconductedinaccordancewiththe HelsinkiDeclaration.
Fortheevaluationofdemographicanddisease characteris-ticsofthepatients,age,education,maritalstatus,durationof thediseaseandofmorningstiffness,medicationsused, num-beroftenderand swollenjoints,qualityoflife(QOL) level, erythrocytesedimentation rate (ESR) (mm/h),and rheuma-toidfactor(RF)(IU/ml)wererecorded.Diseaseactivityscore-28 (DAS-28) wascalculated by using tenderand swollen joint counts, QOL level assessed on the visual analog scale of 0–100mm,andESR.
A detailed neurological examination of patients was performed. On the lower extremity sensory assessment, superficial sensation, pain, heat, vibration, and two-point discriminationsenseswereevaluatedineachfoot,andwith the sum of these, the sensory deficits index (SDI) of0–10 wasobtained.Forsuperficialsenses,5.07Semmes-Weinstein monofilament was applied perpendicular to the plantar surfaceof the distalphalanx ofthe foot thumb. Pain sen-sationwasevaluatedwithneedleinsertioninto theplantar surfaceofthedistalphalanxoffootthumb.Thepatientwas queriedregardingdistinction between bluntand sharp tip, andinthepresenceofcorrectanswersto8of10questions,
pain sensation was accepted as preserved. Ice cubeswere appliedfor 3s tothe plantarsurface ofthe distalphalanx offootthumbtodetermineheatsensation.Vibration sensa-tion wasevaluated onthe dorsalsurfaceofthe metatarsal joint of foot thumb with a 256Hz tuning fork. Two-point discriminationtestwasevaluatedasstatic.Distancebetween the two needles applied to the plantar side of the distal phalanxofthefootthumblessthan0.5cmwasevaluatedas normal.
Electrophysiologictests
PolyneuropathyinpatientswasevaluatedwithMedelec Syn-ergy10-channelelectroneuromyography(ENMG)(Oxford,U.K.) deviceandtheprotocoldescribedbyOhetal.15Accordingly,
bilateral sural sensory nerve conduction studies and bilat-eralperonealandtibialnervemotorconductionstudieswere carried out. For identification of the polyneuropathy, right median,ulnarmotorandsensory nerveconductionstudies were added. Bilateraltibial and common peroneal nerve F waveswere studied.Entrapmentneuropathywas ruledout byapplyingthelateralandmedialplantarnerveconduction studies inpatientswithoutpolyneuropathy. Toidentifythe presenceofpolyneuropathy,pathophysiologicalassessment was performed as axonalor demyelinatingat the affected motorandsensorynervefiber.
Clinictests
For theassessmentofthefunctional statusofpatients,the HealthAssessmentQuestionnaire(HAQ)wasused.16
MobilityandwalkingsubscalesoftheArthritisImpact Mea-surement Scales-2 (AIMS-2) were used for assessinglower extremity functionality.17 Scoring was from 0 to 10, with
0 indicating the best and 10 indicating the poorest health status.
Comparisons
PatientsweredividedintogroupsaccordingtoSDIscoresand electrophysiologicalevaluationasSDIscore0(group1a),SDI score ≥1(group1b),normalelectrophysiologicalevaluation (group2a),andpolyneuropathy(group2b).Groupswere com-paredwithHAQintermsoftheirgeneralhealthstatusand withthemobilityandgaitsubscalesofAIMS-2forthe assess-mentoftheirlowerextremityfunctionalstatus.
Statisticalanalysis
Mann–WhitneyU-test.Avalueofp<0.05wasconsidered sta-tisticallysignificant.
Results
Theaverageageofthe51patientsinthestudywas54.0years, diseaseduration was13years,andmorning stiffness dura-tionwas30min.Thedistributionofdemographicanddisease characteristicsofthepatientsareshowninTable1.
Themeannumberoffootdeformitieswas8.00(7.49±4.24). Therewere17patients(33.3%)withhammertoe,15(29.4%) withclawtoe,25(49%)withcock-updeformity,32(62.7%)with halluxvalgus,21(41.2%)withmetatarsophalangeal subluxa-tion,11(21.6%)withanklecontracturedeformity,29(56.9%) withpesplanus,and6(11.8%)withpescavusdeformity.
Theresultsofthesensory examinationarepresentedin
Table2.
Sensorydisturbancewasdetectedin39 patients(76.4%). TheaveragelevelofSDIwasfoundtobe4.00.Polyneuropathy was detectedin27 patients (52.9%)with electrophysiologi-calevaluation.Inallpatients,therewassensorimotoraxonal polyneuropathy withsensorial predominance. Atleast one sensoryevaluationtestwasimpairedinallpatients.
Table1–Thedistributionofdemographicanddisease characteristicsofthepatients.
n=51 mean ± SD,n(%)
Age(year) 54.72 ± 10.98
Educationlevel
Illiterate 10(19.6)
Onlyliterate 12(23.5)
Primaryschoolgraduate 24(47.1)
Secondaryschoolgraduate 3(5.9)
Highschoolgraduate 1(2.0)
Universitygraduate 1(2.0)
Maritalstatus
Married 42(82.4)
Single 3(5.9)
Divorced 6(11.8)
Diseaseduration(year) 14.91 ± 9.41 Morningstiffnessperiod(min) 74.01 ± 65.45
Drugsused
NSAID 51(100)
Sulfasalazine 39(76.5)
Methotrexate 42(82.4)
Leflunomide 12(23.5)
Hydroxychloroquine 14(27.5)
QOL(0–100mm) 59.21 ± 26.00 DAS-28score 5.50 ± 1.36 RF(IU/mL) 109.19 ± 184.69
HAQ(0–3) 1.53 ± 0.68
Mobilitylevel(AIMS-2)(0–10) 5.27 ± 2.25 Walkinglevel(AIMS-2)(0–10) 6.77 ± 2.61
SD,standarddeviation;min,minute;NSAID,nonsteroidal anti-inflammatorydrug;QOL,qualityoflife;DAS-28,diseaseactivity score-28;RF,rheumatoidfactor;HAQ,healthassessment question-naire;AIMS-2,arthritisimpactmeasurementScale-2.
Table2–Theresultsofthesensoryexamination.
Rightfoot(n=51) n(%)
Leftfoot(n=51) n(%)
Sensoryevaluation
Disturbanceofsuperficial sensation
29(56.9) 30(58.8)
Disturbanceofpain sensation
14(27.5) 14(27.5)
Disturbanceof temperaturesensation
13(25.5) 13(25.5)
Disturbanceofvibration sensation
34(66.7) 34(66.7)
Disturbanceoftwo-point discriminationsensation
16(31.4) 15(29.4)
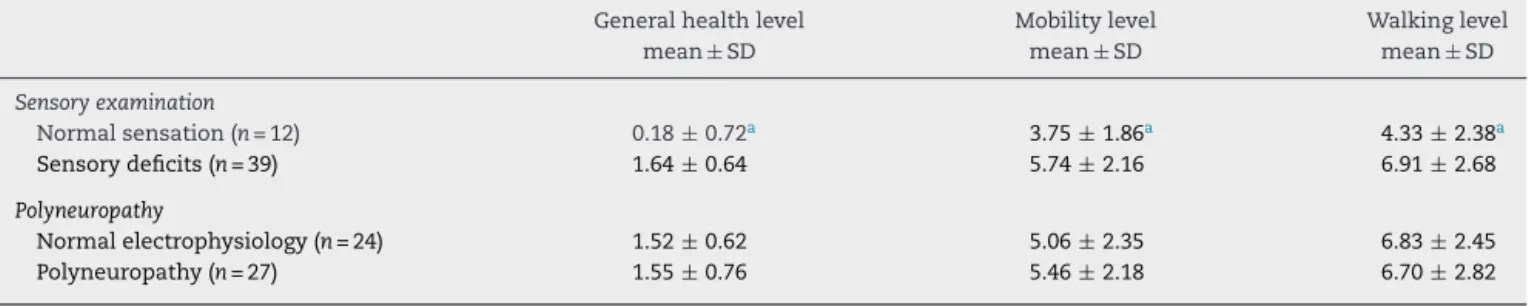
Thecomparisonsbetweengeneralhealthstatusandfoot functionalityevaluationsinpatientswithandwithoutsensory deficitandalsointhosewithandwithoutpolyneuropathyare showninTable3.
In patients with sensory deficits, a statistically signifi-cantdeteriorationwasdetectedingeneralhealthstatusand foot functionality,including mobilityandwalking(p=0.044,
p=0.005, p=0.006, respectively)whencomparedtopatients withanormalsensoryevaluation.
Therewasnostatisticallysignificantdifferenceintermsof generalhealthstatus,mobilityandwalkingfunctionswhen patients with polyneuropathy were compared to patients withnormalelectrophysiologicalfindings(p=0.871,p=0.532,
p=0.866,respectively).
Discussion
InpatientswithRA,severalextra-articularsystems, includ-ing thenervoussystem,areinvolved,and morecommonly, theperipheralnervoussystem,andthesecasesarereported asentrapmentneuropathies,mononeuropathies,andsensory andsensorimotoraxonalpolyneuropathy.7Theincidenceof
peripheralnervoussysteminvolvementinRAhasbeenshown instudiestorangewidely,from18%to75%.7–9,18–20Thiswide
range can be attributed to the fact that in patients with-outclinicalneuropathy,subclinicalperipheralnervoussystem involvementisdetectedduringelectrophysiologicstudiesand autopsies.Inthesepatients,themechanismofinvolvement oftheperipheralnervoussystemisexplainedbythe inflam-mationandimmunecomplex-mediatedinjuryofmyelinated nerve fibers as well as soft tissue swelling, bone deformi-ties,andmechanicalcompressionduetonodules.9Further,
comorbiditiesandthedrugsusedbythesepatientsmaycause secondaryinvolvementoftheperipheralnervoussystem.7
InRApatientswithfootdeformity,thereisaspecialfocus onentrapmentneuropathies.21 Inolderstudies,
polyneuro-pathywasoftenassociatedwiththepresenceofvasculitis.22
However, more recently, sensory-predominant polyneuro-pathyhasemergedasthemostfrequentlyreportedperipheral neuropathyinRApatientsindependentofvasculitis.21
Table3–Comparisonbetweengeneralhealthandfootfunctionevaluationinpatientswithandwithoutsensorydeficit andwithandwithoutpolyneuropathy.
Generalhealthlevel Mobilitylevel Walkinglevel
mean± SD mean± SD mean± SD
Sensoryexamination
Normalsensation(n=12) 0.18± 0.72a 3.75±1.86a 4.33±2.38a
Sensorydeficits(n=39) 1.64±0.64 5.74±2.16 6.91±2.68
Polyneuropathy
Normalelectrophysiology(n=24) 1.52±0.62 5.06±2.35 6.83±2.45
Polyneuropathy(n=27) 1.55±0.76 5.46±2.18 6.70±2.82
SD,standarddeviation. a p<0.05.
Somestudieshaveinvestigatedthepresenceof polyneu-ropathy in RA. Disease duration, disease activity and RF positivityhavebeen reported tobe associatedwith neuro-pathicinvolvement,buthaveshownnoassociationwithfoot deformitiesandjointdamage.7,10,23Theseresultsarein
con-flict with the studies reporting muchmore foot deformity developmentinpatientswithlong-termillnessandhigh dis-easeactivity.14Therefore,theprimarypurposeofthisstudy
was toexclude entrapmentneuropathies due to mechani-calcompression causedby foot deformity and to evaluate theperipheralnervous systeminvolvement,including pos-siblepolyneuropathy,usingsensoryexaminationaswell as electrophysiologicalmethods.Accordingtotheresultsofour study,therewas impairmentinatleastoneofthesensory examinationtestsin76.4%ofpatients.Onelectrophysiological studies,sensorimotoraxonalneuropathywasfoundin52.9% ofpatients.
In our study, the presence of polyneuropathy in RA patientswasconsistentwiththerateof18–90%reportedin the literature.18–20 In thesestudies,particularly inpatients
withover 2–5years’ diseaseduration, observed polyneuro-pathy was associated with disease duration, RF positivity anddiseaseactivity,irrelevantofjointdeformitiesand radio-graphic damage. In our study, in accordance with reports inthe literature,patientshad muchlongerduration of dis-ease(13years)and higherlevels ofdisease activityand RF levels.
In our study, disturbance in terms of polyneuropathy detectedbysensoryevaluationtestswasmuchgreaterthan thepolyneuropathy(76.4%)detectedbyelectrophysiological studies.Toourknowledge,thereisnostudyintheliterature evaluating sensory tests in RA patients specifically. How-ever,inRApatientswithpolyneuropathy,somestudiesused sensorytestsincludingsuperficialtouch,pain,heat,and vibra-tion sensesas wellas electrophysiologicalassessmentand reporteddisturbanceinthesensoryevaluationtests.20,22,25,26
One other study compared electrophysiological methods andsensoryevaluationtests.However,thestudyconducted Ajena et al.25 reported that 12% of patients who were
determined normal electrophysiologically had small fiber neuropathy.
Electrophysiological methods only examine the thick myelinated fibers, and do not show the dysfunction of unmyelinated and thinly myelinated fibers. In sensory
evaluation tests, superficial touch, pain and temperature senses are conducted with unmyelinated C and thinly myelinated A delta fibers, while vibration and two-point discrimination tests are conducted with thick myelinated A beta fibers.27 In two studies in patients with diabetes
mellitus,ahighcorrelationwasreportedbetweenthe vibra-tion sense and electrophysiological methods, but it does not reflect the involvement ofsmall fibers.28,29 In another
study comparing the electrophysiological methods and sensory evaluation tests, with the clinical examination of pain and heat senses, small fiber neuropathy can be detected in electrophysiologically normal patients.30 This
may explain why more disturbance was detected using sensoryexaminationteststhanwiththeelectrophysiological methods in ourstudy. Thus, wethink that alimitation of our study isnot verifying the possible existenceof small-fiber neuropathy with adiagnostic procedure such asskin biopsy.
However, another possible cause of this result may be changesinfootsensitivitytotwo-pointdiscrimination,touch, pain,andtemperaturesensesduetohyperkeratosisin abnor-mal regions due to foot deformities. Studies of the feet in RA patients have reported altered pressure zones and decreased sensory sensitivity when compared to healthy subjects.31Anotherlimitationisthatourstudydidnotinclude
aquantitativegaitanalysis.Largerstudiesareneededinthis regard.
Itwasalsofoundinthisstudythatgeneralhealthstatus andfootfunctionalityareworseinpatientswithsensory dis-turbancethaninpatientswithanormalsensoryexamination, buttherewasnostatisticallysignificantdifferencebetween thepatientswithandwithoutpolyneuropathyaccordingto ENMG.
Therearenostudiesintheliteratureevaluatingthe rela-tionshipbetweendisturbanceinsensorytestsinRApatients andgeneralhealthstatusandfootfunctionality.Furthermore, theresultsreportedinstudiesofRApatientswith polyneuro-pathyareconflicting.20,27
In the study of Bayrak et al.27 polyneuropathy in RA
patients was associated with the general health status as assessedbyHAQ,anddisabilitywasmuchgreaterinpatients with polyneuropathy than in patients without polyneuro-pathy. On the other hand,Agarwal et al.19 study with 108
general health status assessed by HAQ. Unlike our study, patients inthose studies had a shorterduration of illness (mean5.5years), andthe study wasperformedinpatients withoutfootdeformities.Webelievethatthereisnot neces-sarilyanelectrophysiologicalabnormalityinallpatientswith sensorydisturbances.Thestatisticallysignificantdifference between the patients with and without sensory disturb-anceintermsofgeneralhealthstatusandfootfunctionality supportsthisprediction.Asdiscussedabove,sensory disturb-anceoverlaps withthepossibility ofthepresenceofsmall fiberneuropathy;however,morecomprehensivestudiesare needed.
Conclusion
Finally, sensory disturbance was detected in 76% of RA patients with foot deformities with sensory evaluation tests. Although those patients had electrophysiologically detectedpolyneuropathy,thismethodshouldnotbeassessed alone especially in terms of general health status and footfunctionality.Further,evenif electrophysiologicaltests are normal, it should be taken into consideration that the presence of sensory dysfunction alone may lead to severedisabilityingeneralhealthstatusandfoot function-ality when compared to patients with a normal sensory examination.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. CalguneriM.Rheumatoidarthritis.In:YasavulU,editor. Textbookofinternalmedicine,HacettepeUniversity.1sted. Ankara:PrestijPress;2003.p.1477–95.
2. WilliamsAE,GrahamAS,DaviesS,BowenCJ.Guidelinesfor themanagementofpeoplewithfoothealthproblemsrelated torheumatoidarthritis:asurveyoftheiruseinpodiatry practice.JFootAnkleRes.2013;6(1):23.
3. KeskinD,BarcaN,KeskinG,BormanP,BodurH.Foot deformitiesinrheumatoidarthritis.JPMRS.2003;6(1):15–9.
4. AttarSM,Al-GhamdiA.Radiologicalchangesinrheumatoid arthritispatientsatateachinghospitalinSaudiArabia.East MediterrHealthJ.2010;16(9):953–7.
5. BalA,AydogE,AydogST,CakciA.Footdeformitiesin rheumatoidarthritisandrelevanceoffootfunctionindex. ClinRheumatol.2006;25(5):671–5.
6. GökselAK,GünaydinR,AdibelliZH,KayaT,DuruözE.Foot deformitiesinpatientswithrheumatoidarthritis:the relationshipwithfootfunctions.IntJRheumDis. 2010;13(2):158–63.
7. LanzilloB,PapponeN,CrisciC,DiGirolamoC,MassiniR, CarusoG.Subclinicalperipheralnerveinvolvementin patientswithrheumatoidarthritis.ArthritisRheum. 1998;41(7):1196–202.
8. NadkarMY,AgarwalR,SamantRS,ChhuganiSJ,IdgunjiSS, IyerS,etal.Neuropathyinrheumatoidarthritis.JAssoc PhysiciansIndia.2001;49:217–20.
9.BekkelundS,TorbergsenT,OmdalR,HusbyG,MellgrenSI. Nerveconductionstudiesinrheumatoidarthritis.ScandJ Rheumatol.1996;25:287–92.
10.SivriA,UysalGF.Theelectroneurophysiologicalfindingsin rheumatoidarthritispatients.ElectromyogrClin
Neurophysiol.1999;39:387–91.
11.BakkersM,FaberCG,PetersMJ,ReulenJP,FranssenH,Fischer TZ,etal.Temperaturethresholdtesting:asystematicreview. JPeripherNervSyst.2013;18(1):7–18.
12.WickmanAM,PinzurMS,KadanoffR,JuknelisD.
Health-relatedqualityoflifeforpatientswithrheumatoid arthritisfootinvolvement.FootAnkleInt.2004;25(1):19–26.
13.OtterSJ,LucasK,SpringettK,MooreA,DaviesK,YoungA, etal.Identifyingpatient-reportedoutcomesinrheumatoid arthritis:theimpactoffootsymptomsonself-perceived qualityoflife.MusculoskeletCare.2012;10(2):65–75.
14.OtterSJ,LucasK,SpringettK,MooreA,DaviesK,CheekL, etal.Footpaininrheumatoidarthritisprevalence,risk factorsandmanagement:anepidemiologicalstudy.Clin Rheumatol.2010;29(3):255–71.
15.OhS.In:OhS,editor.Principlesofclinicalelectromyography: normalvaluesforcommonnerveconductiontests.2nded. Baltimore:WilliamsandWilkinsCompany;1998.p.84–105.
16.FriesJF,SpitzP,KrainesRG,HolmanHR.Measurementof patientoutcomeinarthritis.ArthritisRheum.1980;23:137–45.
17.MeenanRF,MasonJH,AndersonJJ,GuccioneAA,KazisLE. Thecontentandpropertiesofarevisedandexpanded arthritisimpactmeasurementscaleshealthstatus questionnaire.ArthritisRheum.1992;35:1–10.
18.GoodAE,ChristopherRP,KoepkeGH,BenderLF,TarterME. Peripheralneuropathyassociatedwithrheumatoidarthritis. Aclinicalandelectrodiagnosticstudyof70consecutive rheumatoidarthritispatients.AnnInternMed.1965;63:87–99.
19.AgarwalV,SinghR,WiclafC,ChauhanS,TahlanA,AhujaCK, etal.Clinical,electrophysiological,andpathologicalstudyof neuropathyinrheumatoidarthritis.ClinRheumatol. 2008;27:841–4.
20.BiswasM,ChatterjeeA,GhoshSK,DasguptaS,GhoshK, GangulyPK.Prevalence,types,clinicalassociations,and determinantsofperipheralneuropathyinrheumatoid patients.AnnIndianAcadNeurol.2011;14(3):194–7.
21.KishnerS.Detectingperipheralnerveinvolvementin rheumatoidarthritispatients:commentonthearticleby Lanzilloetal.ArthritisRheum.1999;42(6):1304–5.
22.PallisCA,ScottJT.Peripheralneuropathyinrheumatoid arthritis.BrMedJ.1965;1(5443):1141–7.
23.AktekinLA,GözlükayaH,BodurH,BormanP,KözO. Romatoidartritlihastalardaperiferiknöropati:
elektronörofizyolojikc¸alıs¸ma.TurkJRheumatol.2009;24:62–6.
24.BekkelundSI,TorbergsenT,HusbyG,MellgrenSI.Myopathy andneuropathyinrheumatoidarthritis.Aquantitative controlledelectromyographicstudy.JRheumatol. 1999;26(11):2348–51.
25.AnejaR,SinghMB,ShankarS,DhirV,GroverR,GuptaR,etal. Prevalenceofperipheralneuropathyinpatientswithnewly diagnosedrheumatoidarthritis.IndianJRheum.
2007;2(2):47–50.
26.BayrakAO,DurmusD,DurmazY,DemirI,CanturkF,Onar MK.Electrophysiologicalassessmentofpolyneuropathic involvementinrheumatoidarthritis:relationshipsamong demographic,clinical,andlaboratoryfindings.NeurolRes. 2010;32(7):711–4.
27.HsiehST.Pathologyandfunctionaldiagnosisofsmall-fiber painfulneuropathy.ActaNeurolTaiwan.2010;19:82–9.
29.Vlckova-MoravcovaE,BednarikJ,BelobradkovaJ,SommerC. Small-fibreinvolvementindiabeticpatientswithneuropathic footpain.DiabetMed.2008;25(6):692–9.
30.LøsethS,LindalS,StålbergE,MellgrenSI.Intraepidermal nervefibredensity,quantitativesensorytestingandnerve conductionstudiesinapatientmaterialwithsymptomsand
signsofsensorypolyneuropathy.EurJNeurol. 2006;13(2):105–11.