www.jped.com.br
ORIGINAL
ARTICLE
Clinical
utility
of
early
amplitude
integrated
EEG
in
monitoring
term
newborns
at
risk
of
neurological
injury
夽
,
夽夽
Paulina
A.
Toso
a,∗,
Alvaro
J.
González
a,
María
E.
Pérez
b,
Javier
Kattan
a,
Jorge
G.
Fabres
a,
José
L.
Tapia
a,
Hernán
S.
González
aaDivisionofPediatrics,EscueladeMedicina,PontificiaUniversidadCatólicadeChile,Santiago,Chile bPontificiaUniversidadCatólicadeChile,Santiago,Chile
Received21March2013;accepted1July2013 Availableonline30October2013
KEYWORDS
Amplitudeintegrated
electroencephalogra-phy(aEEG);
Hypoxicischemic
encephalopathy (HIE);
Neonatalintensive
care; Seizures
Abstract
Objective: totesttheclinicalutilityofanearlyamplitude-integratedelectroencephalography (aEEG)topredictshort-termneurologicaloutcomeintermnewbornsatriskofneurologyinjury.
Methods: thiswasaprospective,descriptivestudy.Theinclusioncriteriawereneonatal ence-phalopathy, neurologic disturbances, and severe respiratory distress syndrome. Sensitivity, specificity,positiveandnegativepredictivevalues,andlikelihoodratio(LR)werecalculated. Clinicalanddemographicdatawereanalyzed.Neurologicaloutcomewasdefinedasthesumof clinical,electroimaging,andneuroimagingfindings.
Results: tenofthe21monitoredinfants(48%)presentedalteredshort-termneurologic out-come. TheaEEG had90%sensitivity,82%specificity,82%positive predictivevalue,and90% negativepredictivevalue.ThepositiveLRwas4.95,andthenegativeLRwas0.12.Inthreeof 12(25%)encephalopathicinfants,theaEEGallowedforabetterdefinitionoftheseverityof theircondition.Seizuresweredetectedineightinfants(38%),allsubclinicalatbaseline,and nonehadanormalaEEGbackgroundpattern.Thestatusofthreeinfants(43%) evolvedand requiredtwoormoredrugsfortreatment.
Conclusions: ininfantswithencephalopathyorothersevereillness,aEEGdisturbancesoccur frequently.aEEGprovidedabetterclassificationoftheseverityofencephalopathy,detected earlysubclinicalseizures,andallowedformonitoringoftheresponsetotreatment.aEEGwas ausefultool attheneonatalintensivecareunitforpredictingpoorshort-termneurological outcomesforallsicknewborn.
©2013SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:TosoPA,GonzálezAJ,PérezME,Kattan J,FabresJG,TapiaJL,etal.Clinicalutilityofearlyamplitude integratedEEGinmonitoringtermnewbornsatriskofneurologicalinjury.JPediatr(RioJ).2014;90:143---8.
夽夽NeonatalIntensiveCareUnit,HospitalClínico,PontificiaUniversidadCatólicadeChile,Santiago,Chile.
∗Correspondingauthor.
E-mail:[email protected](P.A.Toso).
PALAVRAS-CHAVE
Eletroencefalograma
deamplitude
integrada(aEEG);
Encefalopatia hipóxico-isquêmica (EHI);
Terapiaintensiva
neonatal; Convulsões
UtilidadeclínicadeummonitoramentoporEEGdeamplitudeintegradaprecoceem recém-nascidosatermocomriscodelesãoneurológica
Resumo
Objetivo: testarautilidadeclínicadoaEEGprecoceemrecém-nascidosatermocomriscode lesãoneurológica,parapreverresultadosneurológicosdecurtoprazo.
Métodos: estudoprospectivoedescritivo.Oscritériosdeinclusãoforamencefalopatia neona-tal, distúrbios neurológicos e bebês com SARA grave. Sensibilidade, especificidade, valor preditivo positivoe negativoerazãode verossimilhanc¸aforamcalculados.Dados clínicos e demográficosforamanalisados.Oresultadoneurológicofoidefinidocomoasomadeconclusões clínicas,deeletroedeneuroimagem.
Resultados: dentreos21neonatosmonitorados,dez(48%)apresentaramresultadoneurológico decurtoprazoalterado.OaEEGapresentousensibilidadede90%,especificidadede82%,valor preditivopositivode82%evalorpreditivonegativode90%.AVRpositivafoide4,95,eaRV negativade0,12.Emtrêsdos12(25%)neonatoscomencefalopatiafoipossíveldefinirmelhor agravidadedesuacondic¸ãopeloaEEG.Foramdetectadasconvulsõesemoitoneonatos(38%), todassubclínicasnoiníciodoestudo,enenhumapresentouumpadrãohistóriconormalnoaEEG. Oestadodetrêsneonatos(43%)evoluiueexigiudoisoumaismedicamentosparatratamento.
Conclusões: em neonatos com encefalopatia ououtra doenc¸a grave, osdistúrbios noaEEG ocorremcommaisfrequência.OaEEGforneceuumaclassificac¸ãomelhordagravidadeda ence-falopatia,detectouconvulsõessubclínicasprecocesepermitiuquefossefeitoomonitoramento darespostaaotratamento.OaEEGéumaferramentaútilparapreverresultadosneurológicos decurtoprazoemtodososbebêsdoentesnaUTIN.
©2013SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Modernneonatalpracticesinvolvemanagingincreasinglyill
andcomplexpatients.Theassessmentofneurological
func-tionofthesepatientsislimitedbytheseverityofthebase
illness and the use of sedatingmedications. It is difficult
todeterminewhichpatientsneed specializedneurological
follow-upafteraneonataldisease.
The introduction of continuous brain monitoring by
amplitude-integrated electroencephalography (aEEG)
allows for the evaluation of brain function in real time
andover long periods. The aEEG waveappears to bethe
result of the sum of the resting membrane potential,
whichis influenced primarily bythe metabolic statusand
secondarily by the blood flow to the brain, among other
factors.1---4
While the evolution of aEEGmonitoring after hypoxic-ischemiceventshasprovenprognosticvalue,5---10 itsutility forothercommonneonatalmorbiditieshasnotbeen well-studied. The main limitation of aEEG monitoring is that it provides limited information regarding electrical brain activity. The monitored areas correspond to the limit of irrigation of the three cerebral arteries that are more susceptible to hypoxic-ischemic insults.11 There is dis-agreement regarding its utility for detecting seizures.12 Another limitation is in distinguishing the true image of artifacts.13
The main objective of this study was to assess the clinicalutilityofanearly aEEGtopredictshort-term neu-rologicaloutcomesamongtermnewborns admittedtothe neonatalintensivecare unit(NICU)at risk ofneurological injury.
Materials
and
methods
Patients
Term newborns from the period of September of 2005 to
August of2006 wereselectedfor aEEGmonitoring ifthey
wereconsideredasevolvingwithaneurologicalrisk.Thus,
anybabieswithaneonatalencephalopathy,neurologic
dis-turbance,orwithsevererespiratorydistresssyndrome(RDS)
wereincluded.Diagnosesweremadebytheattending
physi-cians based onclinical andlaboratory criteria. In hypoxic
ischemic encephalopatic (HIE) neonates, the Sarnat
clas-sification I-III was used in order of increasing severity.9
Entrycriteriaforhypothermiaprotocolwereterminfants, less than 6hoursold,withacutefetal distress(prolonged resuscitation need, and/or cord pH < 7.0; and/or Apgar score at 5minutes < 5), evolvingencephalopathy, and an alteredaEEGrecordafterthefirsthouroflife.RDSpatients were monitored whentheyreached an oxygenationindex (OI) > 18. Extracorporeal membrane oxygenation (ECMO) treatmentcriteriawereOI>40aftermaximumrespiratory management,andreversiblelungdisease.Newbornswitha knownprenatalbrainlesionormalformationwereexcluded, aswellasanysimultaneouspatients,sinceonlyonebrain monitorwasavailable.Thestudywasapprovedbytheethics committeeofthisinstitution,andaninformedconsentwas obtainedfromtheparents.
Monitoring
Electrodes were installed onpatients’ shaved scalps, and
that provided information regarding both brain
hemi-spheres, in locations equivalentto C3-P3 and C4-P4 of a
standardEEG.Thisdeviceamplifiesthesignalobtainedafter
filtrationbetween 2to15Hz, integratesinformationfrom
theamplitudeofthewavesobtained,andthenscansto
dis-playpatternsonthescreen at6cm/handrawEEGinreal
time.Aphysician(notblinded),assistedbymedical
super-visors trainedin this technique, interpreted the tracings.
The information wasstored on a computerhard disk and
extracted forfurtheranalysisusingtwosoftware(Analyze
andChartAnalyzer).Thepatternsobtainedwereclassified
accordingtoHellström-Westasclassification,wheretype1
isnormal,andtypes 2,3,4,and5arealteredin
increas-ingorderofseverity.14 Monitoringwasinstalledassoonas
possibleandcontinueduntilpatientswerestable.EEGwas requestedforselectedepisodesasastandardclinicalneed. Thepresenceandmanagementofseizureswereregistered, aswell asadverse events related totheaEEG technique. Theuseofdrugsthataffectthecentralnervoussystemwas recorded.15---18
Datacollectionandoutcomemeasures
Demographicandclinicaldatawereprospectivelycollected.
The main outcomewasshorttermneurologicalevolution,
classifiedasnormalorabnormal.
The abnormal neurological outcome was defined by
standard clinical practices: the presence of an altered
physical exam (disturbances in consciousness, hyper- or
hypotonia, absentvisualfixation and/orabsent gag,suck,
andfeedingautonomy)documentedbytheattending
physi-cianaftertheacuteevolutionwasresolved,combinedwith
analteredbrainimaging(presenceofgrayorwhitematter
injury,basalgangliacompromise,andhemorrhagicand/or
stroke lesions) and/or altered pre-discharge EEG (altered
background pattern, persistentdepressedvoltage, and/or
seizures). Neuroimaging was requested based on clinical
need(headultrasound,transmissioncomputedtomography,
ormagneticresonanceimaging),andperformedbyan
inde-pendentneuroradiologistblinded totheclinical andaEEG
findings.
Analysis
Descriptive data were presented asmean±SD or median
(range),as appropriate.Two- sidedStudent’s t-test, with
95% of confidence interval, was used for parametric
variables, and the Mann-Whitney test was used for
non-parametricvariables.Categoricalvariableswerecompared
throughthemid-pexacttest.
Sensitivity, specificity, positiveand negativepredictive
values,andpositiveandnegativelikelihoodratios(LR)were
calculatedwith95%confidenceinterval,inordertoevaluate
whetheraEEGisapredictivetoolforshort-termneurological
evolutionforallpatients,regardlessofthediagnosis.
Results
During the study period; 2,196 patients were born at
this center and118 were transferredfrom other centers.
Of these, 225 term neonates were hospitalized in the
NICU.Twenty-one newborns weremonitored, of whom13
were outborns. The diagnoses of the patients included
were:neonatalencephalopathyin12newborns(fivebegan
hypothermiaprotocol),pulmonary hypertensionsecondary
toRDSineight(fourbeganECMO),andonewithsuspected
neonatalseizures.Thegestationalagewas38.6±1.4weeks
(mean±SD).Monitoringstartedat10(4-20)hours[median
(PC25-PC75)] of life, and the mean duration of
monitor-ingwas54 (27-120)hours;1,626hoursof monitoringwere
obtained.Noneofthepatientsdiedduringthestudyperiod.
Patients’ demographic and clinical characteristics are
describedonTable1.Of the21patientsstudied,ten
pre-sentedalteredshort-termneurologicaloutcomeasdefined throughclinical,EEG,and/oralteredneuroimagingcriteria. TheneurologicalabnormalbabieshadlowerApgarscoresat fiveminutesthanthenormal group,andweremorelikely todevelopseizuresduringevolution.Thegroupofabnormal neurologicaloutcomewasmostlyrepresentedby encepha-lopathy patients, but the difference was not statistically significant. The three patients who were not encephalo-pathicat this group, also hada complicated neurological course, but this did not appear to be attributable to an ischemic perinatal hypoxic event. aEEG was abnormal in nineofthesetennewborns(sensitivityof90%,95%CI: 59.6-98.2).Of the 11 neurologically normal patients, nine also hadacompletelynormalaEEG(specificityof82%,95%CI: 52.3-94.9).Thepositivepredictivevalue was82%(95%CI: 52.3-94.9)andthenegativepredictivevaluewas90%(95% CI:59.6-98.2).ThepositiveLRwas4.95(95%CI:1.81-13.51) andthenegativeLRwas0.12(95%CI:0.02-0.91).
48%ofthenewbornsstartedwithanormalaEEGpattern andprogressed normallyuntilthe end of thestudy. None ofthem had seizures. The recordings showedthat abnor-maltype2,3,4,and5aEEGpatternsweremorelikelyto continuetobealtered.
38% of the children had seizures during monitoring. Alldetectionswereinitiallyperformed throughmonitoring sincetherewereaboutthreehoursafterclinicalcorrelation (Fig.1).AllchildrenwhohadseizureshadanabnormalaEEG patternatthestartofmonitoring.75%ofthenewbornsthat evolvedtoaconvulsivestatusrequiredtwoormoredrugs forthetreatmentofseizures(Fig.2).
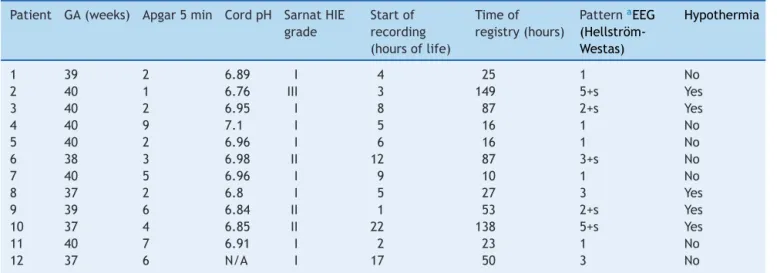
Of the 12 encephalopathic infants (Table 2), the nor-malrecordingsoffivehelpedclinicianstodecidethatthey didnotrequirehypothermiaprotocol.Twoencephalopathic newborns had altered aEEG patterns, but came late to hypothermia treatment (which is recommended to start before6hoursoflife).PatientsNo.3,8,and12had symp-tomsofHIEgradeIatthetimeofevaluation,buttheaEEG registrationshowed an abnormalpath; oneof the infants subsequentlydevelopedseizures,soallthreepatients actu-allyevolvedintoaHIEgradeIIinsteadofaHIEgradeI,as wasthefirstclinicalapproach.
Standard EEGs were performed in 11 of the newborns (57%), and the results were consistent with those of the aEEG.
Table1 Demographicandclinicalcharacteristicsofthestudygroup.
Neurologicshorttermoutcome
Abnormal(n=10) Normal(n=11) p-value
BirthWeight,kg 3,210±457 3,309±494 0.639
Gestationalage,weeks 38±1 38±1 0.999
Gender,n(%male) 6(60%) 6(55%) 0.37
Apgar5minutesa 5(1-9) 8(6-8) 0.045
Presenceofanygradeofencephalopathy,n(%) 7(70%) 5(46%) 0.068
PresenceofanabnormalaEEGpattern,n(%) 9(90%) 2(18%) <0.001
Presenceofseizures,n(%) 7(70%) 1(9%) <0.001
Datapresentedasmean±SD,exceptwherenoted(a).amedian(range).
aEEG,amplitude-integratedelectroencephalography;SD,standarddeviation.
EEG Waveform Left
EEG Waveform Right
aEEG Left
aEEG Right
Figure1 Patientwithseverepulmonaryhypertensionsecondarytoadilatedcardiomiopathywithheartfailure.Onthethirdday oflife,theaEEGshowed seizuresintherighthemisphere.Duetoclinicalsuspicion,aheadultrasoundwasperformed,showing intraventricularhemorrhageintherightsideofthebrain.aEEG,amplitude-integratedelectroencephalography.
EEG Waveform Left
EEG Waveform Right
aEEG Left
aEEG Right
67 8
8 67
Table2 ClinicalandaEEGcharacteristicsofencephalopathypatients.
Patient GA(weeks) Apgar5min CordpH SarnatHIE grade
Startof recording (hoursoflife)
Timeof registry(hours)
PatternaEEG (Hellström-Westas)
Hypothermia
1 39 2 6.89 I 4 25 1 No
2 40 1 6.76 III 3 149 5+s Yes
3 40 2 6.95 I 8 87 2+s Yes
4 40 9 7.1 I 5 16 1 No
5 40 2 6.96 I 6 16 1 No
6 38 3 6.98 II 12 87 3+s No
7 40 5 6.96 I 9 10 1 No
8 37 2 6.8 I 5 27 3 Yes
9 39 6 6.84 II 1 53 2+s Yes
10 37 4 6.85 II 22 138 5+s Yes
11 40 7 6.91 I 2 23 1 No
12 37 6 N/A I 17 50 3 No
a EEG,amplitude-integratedelectroencephalography;GA,gestationalage;HIE,hypoxicischemicencephalopathy;N/A,notavailable;
s,seizures).
(s,seizures,N/A,notavailable).
tosensorscomingunstuckandinthecaseofonenewborn,
duetohigh-frequencyventilatorinterference.
Discussion
Prior andMaynardcreated the aEEGin the1960sto
mon-itor adult cardiac patients.19 Since the late 1970s, it has
beenusedwithnewborns,butinitiallyonlyinEurope.20---23 The need toidentifyencephalopathic newborns withhigh neurological risk led to the development of this tech-niqueinparallelwithmulticenterstudiesofhypothermia,24 motivating its use in the rest of the world.25 There is nowincreasinglysophisticatedandlessinvasiveequipment. Thus,thisstudywasdesignedtotesttheemerging technol-ogyinordertobetterunderstandtheclinicalapproach.
Atthetimeofthestudy,approximately10%oftheterm infants were verysick and qualified for aEEGmonitoring. Withtheinclusivecriteriausedtomonitor patientsat this NICU, early aEEG performed asa gooddiagnostic test to predictpoorshort-termneurologicaloutcomes.Itwasless preciseinpredictingnormaloutcomes,wherethecommon diagnostictoolswerehelpful.
Among the most notable findings was that over half of the patients showed alterations in aEEG recordings. It was also found that patients with an altered aEEG pattern were more likely to develop seizures, and this was not only observed with encephalopathy patients. Seizures were initially all subclinical, asdescribed in the literature.26 However; there was also a notable latency period between the onset of the electrical disturbance andclinicalemergenceatthissetting.Instatusepilepticus infants,twoormoredrugswereneededtocontrolseizures, and the aEEG helped to manage the anticonvulsivant therapy.
A theme of discussion is whether aEEG is needed to decide if an encephalopathic newborn is a candidate for coolingtherapy.27aEEGhasbeenusedfortheinclusion crite-riainsomecoolingprotocols,25,28butnotinothers.Inthe presentstudy,itwasobservedthatearlyaEEGmonitoring,
especiallyininfantswithapparentgradeIHIE,24wasmore effectivethanclinicalassessmentaloneinidentifyingwhich encephalopathicpatientswoulddevelopserious neurologi-calconditions.This findingbecomesmoreimportantwhen considering that the time todecide whether a child is a candidatefor hypothermia therapy is limited,and that is importanttocorrectlyinitiatethiscrucialtherapy.
ThereisarecentprospectivestudyofuseofearlyaEEG(< 9hours)inmoderateandsevereencephalopathicpatients, which didn’t present any advantage compared with only stagingtopredict longterm neurologicaloutcome.29 That study differs inboth thepatients included andmain out-come; thus, a comparison with the present study is not feasible.
An unexpected finding wasthe inability of the clinical examinationtodistinguishpatientsevolvingwithasevere neurologicalconditioninreal-timeandhowtheuseofaEEG influencedtheadoptionof moreagiletherapies. This was moststrikinginRDSpatients.
The mainlimitations ofthe studywerethe small num-ber of patients, and the absence of a strict protocol for totalmonitoring timeorfor EEGor neuroimagingrequest. However,thisscenarioissimilartotheactualpracticewith infantsintheNICUs.
Thelong-termbenefitsoftheuseofaEEGhavenotbeen evaluated. Thereis one reportthat, amongpatients with seizuresin theneonatalperiod,thesubsequentincidence ofepilepsywasmuchlowerwiththeuseofthistechnique thanwithout(9.4%vs.56%).30Thus,aEEGappearstobean interestingcomplementarytool.
In conclusion, early aEEG at the NICU allowed for moreaccurate diagnoses, betterselection of patients for hypothermiatherapy,appropriatedetectionandearly treat-mentofseizures,andselectionofpatientsforneurological follow-up.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Victor S, Marson AG, Appleton RE,Beirne M, Weindling AM. Relationshipbetweenbloodpressure,cerebralelectrical activ-ity,cerebralfractionaloxygenextraction,andperipheralblood flow invery low birth weight newborn infants. Pediatr Res. 2006;59:314---9.
2.GreisenG,PrydsO, RosénI,LouH.PoorreversibilityofEEG abnormalityinhypotensive,pretermneonates.ActaPaediatr Scand.1988;77:785---90.
3.BendersMJ,MeineszJH,vanBelF,vandeBorM.Changesin electrocortical brainactivityduringexchange transfusionsin newborninfants.BiolNeonate.2000;78:17---21.
4.West CR, Groves AM, Williams CE, Harding JE, Skinner JR, KuschelCA,etal.Earlylowcardiacoutputisassociatedwith compromisedelectroencephalographicactivityinverypreterm infants.PediatrRes.2006;59:610---5.
5.ThornbergE,Ekström-JodalB.Cerebralfunctionmonitoring:a methodofpredictingoutcomeintermneonatesaftersevere perinatalasphyxia.ActaPaediatr.1994;83:596---601.
6.Hellström-WestasL,RosénI,SvenningsenNW.Predictivevalue ofearlycontinuousamplitudeintegratedEEGrecordingson out-comeafterseverebirthasphyxiainfullterminfants.ArchDis ChildFetalNeonatalEd.1995;72:F34---8.
7.vanRooij LG,Toet MC, OsredkarD, vanHuffelen AC, Groe-nendaal F, de Vries LS. Recovery of amplitude integrated electroencephalographicbackgroundpatternswithin 24hours of perinatal asphyxia. Arch Dis Child Fetal Neonatal Ed. 2005;90:F245---51.
8.ter Horst HJ, Sommer C, Bergman KA, Fock JM, van Weer-denTW,BosAF.Prognosticsignificanceofamplitude-integrated EEGduringthefirst72hoursafterbirthinseverelyasphyxiated neonates.PediatrRes.2004;55:1026---33.
9.SarnatHB,SarnatMS.Neonatalencephalopathyfollowingfetal distress. A clinical and electroencephalographic study. Arch Neurol.1976;33:696---705.
10.SpitzmillerRE,PhillipsT,Meinzen-DerrJ,HoathSB. Amplitude-integrated EEG is useful in predicting neurodevelopmental outcome infull-terminfantswithhypoxic-ischemic encepha-lopathy:ameta-analysis.JChildNeurol.2007;22:1069---78.
11.Hellström-WestasL,WestgrenU,RosénI,SvenningsenNW. Lido-cainefor treatmentof severeseizuresin newborninfants I. Clinicaleffectsandcerebralelectricalactivitymonitoring.Acta PaediatrScand.1988;77:79---84.
12.ShellhaasRA, SoaitaAI, ClancyRR. Sensitivityof amplitude-integratedelectroencephalographyforneonatalseizure detec-tion.Pediatrics.2007;120:770---7.
13.Hagmann CF, Robertson NJ, Azzopardi D. Artifacts on elec-troencephalograms may influence the amplitude-integrated EEGclassification:aqualitativeanalysisinneonatal encepha-lopathy.Pediatrics.2006;118:2552---4.
14.Hellström-WestasL,RosénI,deVriesLS,GreisenG. Amplitude-integratedEEGclassificationandinterpretationinpretermand terminfants.NeoReviews.2006;7:e76---87.
15.BellAH,GreisenG,PrydsO.Comparisonoftheeffectsof phe-nobarbitoneand morphineadministrationon EEG activity in pretermbabies.ActaPaediatr.1993;82:35---9.
16.vanLeuvenK,GroenendaalF,ToetMC,SchobbenAF,BosSA, deVriesLS,etal.Midazolamandamplitude-integratedEEGin asphyxiatedfull-termneonates.ActaPaediatr.2004;93:1221---7.
17.NguyenTheTichS,VecchieriniMF,DebillonT,PéréonY.Effects ofsufentanilonelectroencephalograminveryand extremely pretermneonates.Pediatrics.2003;111:123---8.
18.YoungGB,daSilvaOP.Effectsofmorphineonthe electroen-cephalogramsofneonates:aprospective,observationalstudy. ClinNeurophysiol.2000;111:1955---60.
19.Maynard D, Prior PF, Scott DF. Device for continuous moni-toringofcerebralactivityinresuscitatedpatients.BrMedJ. 1969;4:545---6.
20.VermaUL,ArchbaldF,TejaniNA,HandwerkerSM.Cerebral func-tionmonitorintheneonateI:Normalpatterns.DevMedChild Neurol.1984;26:154---61.
21.Hellström-WestasL,RosénI.Amplitude-integrated electroen-cephalogram in newborn infants for clinical and research purposes.ActaPaediatr.2002;91:1028---30.
22.ToetMC,vanderMeijW,deVriesLS,UiterwaalCS,vanHuffelen KC. Comparison between simultaneously recorded amplitude integratedelectroencephalogram(cerebral functionmonitor) and standard electroencephalogram in neonates. Pediatrics. 2002;109:772---9.
23.Hellström-Westas L. Comparison between tape-recordedand amplitude-integratedEEGmonitoringinsicknewborninfants. ActaPaediatr.1992;81:812---9.
24.Shalak LF, Laptook AR, Velaphi SC, Perlman JM. Amplitude-integrated electroencephalography coupled with an early neurologicexaminationenhancespredictionofterminfantsat riskforpersistentencephalopathy.Pediatrics.2003;111:351---7.
25.GluckmanPD,WyattJS,AzzopardiD,BallardR,EdwardsAD, FerrieroDM,etal.Selectiveheadcoolingwithmildsystemic hypothermiaafterneonatalencephalopathy:multicentre ran-domisedtrial.Lancet.2005;365:663---70.
26.Tekgul H, Bourgeois BF, Gauvreau K, Bergin AM. Electroen-cephalographyinneonatalseizures:comparisonofareduced andafull10/20montage.PediatrNeurol.2005;32:155---61.
27.ThoresenM.Hypothermiaafterperinatalasphyxia:selectionfor treatmentandcoolingprotocol.JPediatr.2011;158:e45---9.
28.Azzopardi DV, Strohm B, Edwards AD, Dyet L, Halliday HL, Juszczak E, et al. Moderate hypothermia to treat perinatal asphyxialencephalopathy.NEnglJMed.2009;361:1349---58.
29.Shankaran S, Pappas A, McDonald SA, Laptook AR, Bara R, EhrenkranzRA,et al.Predictivevalueofanearlyamplitude integratedelectroencephalogramandneurologicexamination. Pediatrics.2011;128:e112---20.