RevBrasAnestesiol.2014;64(2):140---144
REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
LETTERS
TO
THE
EDITOR
Change
Pain
Latin
America
---
new
initiative
established
to
enhance
management
of
patients
with
chronic
pain
in
Latin
America
DearEditor,
I wish to advise you of the formation of a new scien-tific advisory panel, committed to enhancing the quality of life of chronic pain patients in Latin America. The panelwasformedinresponsetotheencouragingoutcomes observed with the Change Pain Europe program, which aimed to identify the unmet needs of European chronic painpatientsandprovidebestpracticesolutionstoimprove patientoutcomes.The panelofregionalexpertsisdriving apan-LatinAmericaninitiative:ChangePainLatinAmerica (CPLA).
The CPLA Advisory Panel comprises 17 experts from Brazil,Chile,Colombia,CostaRica,Ecuador,Mexico,Peru, VenezuelaandSpain,whoworkacrossavarietyofclinical pain-related specialties (Table 1). Panel members are applyingtheirknowledge and experiencetohighlight and addresstheunmetmedicalneedsassociatedwithtreating patientswithchronicpaininLatin Americaand overcome obstacles to improve best practice and outcomes in this region.The inaugural meeting of the panel took placein Miami (June 28---29, 2012) where discussions focused on currenttreatmentparadigmsinLatinAmericaandbarriers to effective patient management. During this meeting, the objectives for CPLA were determined after robust discussions,andacceptedwithconsensualagreementfrom thepanelmembers(Table2).
Whilesuboptimalmanagementofpatientswithchronic painisaglobalissue,factorsthatcontributetothisproblem inLatinAmericaincludegapsinphysicians’understanding andassociatedpainmanagementmisconceptions.Patients in Latin America often misunderstand the risks associ-atedwithanalgesics,making patienteducationapriority. Consequently,healthcare professionals in theregion have inadequateknowledgeoftheadvantagesanddisadvantages of opioids, and the correct dosing of these medications, whichlimitsappropriateprescribing.Othersignificant bar-riersincludelimitedpatientaccesstomedicationsand/or painspecialistsand specialistfacilities,aswell as restric-tive government healthcare policies. All of these factors
contribute to the unmet medical needs of patients with chronicpaininLatinAmerica.
At the second CPLA meeting in Mexico City (Novem-ber9---10,2012),thepanelunveiledseveralkeyinitiatives designed to address these unmet needs.To help improve patient management, panel members are now reviewing international chronic pain guidelines to identify manage-ment strategies that are most relevant toLatin America. Thenextstepwillbetoprovidephysiciansthroughoutthe regionwithcleartreatmentrecommendationsbasedonthis researchtofacilitatetheadoptionofuniformbestpractice throughout the region. The first set of recommendations will focuson chronic low back pain.The unmetneed for educationamongphysicians isalsobeingaddressed viaan online ‘Meeting in a Box’ tool comprising an up-to-date slide library and meeting organization resources for the educationof groups ofphysicians onkeyissuesin chronic pain at local meetings. In addition, newsletters detailing keyregionalissuesinchronicpainmanagementand activ-ities planned by the CPLA panel to help address these issues,willbedistributedtothewiderhealthcare commu-nity.
Part of thepanel’s effortswill focusongaining a bet-ter understanding of the burden of chronic pain in the Latin American region. Panel members have conducted a meta-analysis of available epidemiological data, which established the prevalence of chronic lower back pain in theregionandhighlightedtheneed formorerobust stud-ies. To support this, the panel discussed a new burden of disease protocol that is designed to quantify health-careresourceconsumptionbychronicpainpatientsacross LatinAmerica.Thedatageneratedshouldprovideconsistent estimates of both the direct and indirect costs associ-ated with this burden in all member countries, which it is hoped will inform better resource management in the area. In addition, information onprescribing and diagno-sishabitsamongphysicians inMexico willbepublished in the near future. Ifthe survey is extended to include the entire regionandrepeatedona yearlybasis,it willallow changesinclinicalpracticeacrossLatinAmericatobe doc-umented.
The CPLA panel willestablish working groups tofocus onmeetingacceptedconsensusobjectives.Practical strate-giesarerequiredtobreakdownregional-specificbarriersto the effective management of patients with chronic pain. Improved training and ongoing education of healthcare
LETTERSTOTHEEDITOR 141
Table 1 Change Pain Latin America Advisory Panel members.
Argelia Lara-Solares
Mexico Anesthesiology,
painmanagement andpalliativecare JoséAlberto
FloresCantisani
Mexico Anesthesiology,
painmanagement andpalliativecare César
Amescua-García
Mexico Anesthesiology,
painmanagement andpalliativecare MaríadelRocío
GuillénNú˜nez
Mexico Anesthesiology,
painmanagement andpalliativecare AzizaJreige
Iskandar
Venezuela Physical rehabilitation PatriciaBonilla Venezuela Anesthesiology,
painmanagement andpalliativecare JoãoBatista
SantosGarcia
Brazil Anesthesiology,
painmanagement andpalliativecare
OsvandréLech Brazil Orthopedics
DurvalCampos Kraychete
Brazil Anesthesiology
andpain management MaríaAntonieta
Rico
Chile Anesthesiology,
painmanagement andpalliativecare JohnJairo
Hernández-Castro
Colombia Neurosurgery,pain managementand palliativecare FrantzColimon Colombia Anesthesiology
andpain management CarlosGuerrero Colombia Anesthesiology,
painmanagement andpalliativecare WilliamDelgado
Barrera
CostaRica Anesthesiology
Manuel Sempértegui Gallegos
Ecuador Anesthesiology
andpain management MaríaBerenguel
Cook
Peru Anesthesiology,
painmanagement andpalliativecare ConcepciónPérez
Hernández
Spain Anesthesiology
andpain management
professionalsandprovidersareneededtoimprove diagnos-ticandtreatmentdecisions.Thiswillincreaseappropriate prescribing of currently available analgesics and the acceptance of new analgesic technologies as they are approved across Latin America. A greater understand-ing of the burden of pain in Latin America is also critical moving forward. By generating robust epidemio-logic and pharmacoeconomic data for the region, CPLA will assist efforts to predict how the needs for anal-gesics will change in future. These new dataand current
Table2 ObjectivesoftheChangePainLatinAmerica Advi-soryPanel.
•Identifytherelevantfactorsinfluencingthetreatment ofpainandthedecisionmakersacrossLatinAmerica
•Understandtherelevantfactors/reasonsbehindthe currentpaintreatmentparadigm
•Identifytheleversthatcanbeusedtomodifythe situation
•Establishthelinkbetweenmedicalpracticeand theoryinthemanagementofchronicpain
•Establishtherealunmetneedsinthetreatmentof chronicpaininLatinAmerica
•Betterunderstandtherealityofchronicpainpatients today
•Findconsensusonthechallengesinmanagingchronic painfromaphysician’sperspective
•Evaluatetheneedtoeducatetoraisetheawareness onbestpracticeinthemanagementofchronicpain •Assesstheneedtoenhancecommunicationbetween physiciansandpatientsasawaytoimprovethe managementofpain
•Developsolutionsbasedonresearchdataandexperts’ opinionsupportingmoreeffectiveandefficientpain management
•Increaseknowledgeandprovideappropriatetoolsto improvepaindiagnosis
•Eliminateopiophobiathrougheducationofhealthcare professionalsandpatientsonopioidtreatment
evidence will also be vital in endeavors to facilitate greaterdialoguewithnationalgovernmentdecision-makers, and help reshape healthcare policy leading to the best possible care for patients with chronic pain in Latin America.
To help highlight the relevant issues in Latin America, CPLA is seeking topartner withestablished national pain organizationsacrosstheregion.Afamiliarapproachassisted Change Pain Europe, which is endorsed by the European FederationofIASP®Chapters(EFIC),inachievingitsaims.
The CPLA Advisory Panelis next scheduled to meet in May 2013, with a further meeting planned for later in 2013.Practicalmaterials arebeingdeveloped andwillbe disseminated at a national level. For further information about CPLA and the CPLA panel, please visitthe website
atwww.latamchangepain.com.
Conflicts
of
interest
ChangePainLatinAmerica issupported byan educational grantfromGrünenthal.
JoãoBatistaSantosGarciaa,b,c,1
aSociedadeBrasileiradeEstudodaDor,SãoPaulo,SP,
Brazil
bUniversidadeFederaldoMaranhão,SãoLuís,MA,Brazil
cInstitutoMaranhensedeOncologiaAldenoraBelo,São
Luís,MA,Brazil
142 LETTERSTOTHEEDITOR
1On behalf of The Change Pain Latin America Advisory
Panel: ArgeliaLara-Solares,José AlbertoFlores Cantisani, César Amescua-García, María del Rocío Guillén Nú˜nez, AzizaJreigeIskandar,PatriciaBonilla,OsvandréLech, Dur-val Campos Kraychete, María Antonieta Rico, John Jairo
Hernández-Castro,FrantzColimon,CarlosGuerrero,William Delgado Barrera, Manuel Sempértegui Gallegos, María Berenguel Cook, João Batista Santos Garcia, Concepción PérezHernández.
http://dx.doi.org/10.1016/j.bjane.2013.03.004
Contraction
versus
contracture
and
centronuclear
myopathy
versus
central
part
myopathy
in
malignant
hyperthermia
DearEditor,
We read with great interest the review article by Cor-reiaetal.‘‘Malignanthyperthermia:clinicalandmolecular aspects’’1 (Hipertermia maligna: aspectos moleculares e
clínicos)andwouldliketocommentonsomeaspects.
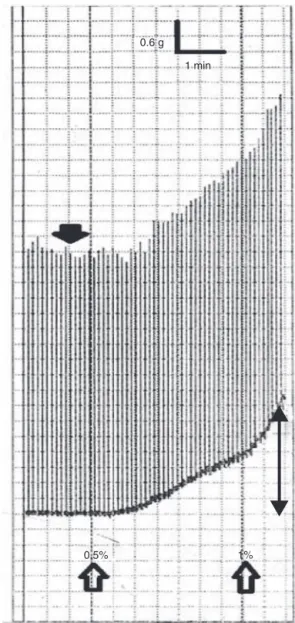
In the section ‘‘Malignant hyperthermia’’, item ‘‘Contraction to exposure to halothane-caffeine (TCHC) Test’’,Correia etal. use theterm ‘‘contraction’’instead oftheoriginalterm‘‘contracture’’.Thetest fordiagnosis of susceptibilityto malignanthyperthermia (MH) is based onanabnormalcontractureresponseafter administration ofcaffeine/halothane, andnotonthenormalresponseof muscle contraction after electrical stimulation, which is appliedthroughoutthetesttoproveviabilityofthemuscle fragment tested. Fig. 1 shows the difference between contractionandcontractureinthechartofapositivetestin apatientsusceptibletoMH.Thus,thenomenclatureshould be‘‘contracturetest’’ in Englishandteste decontratura
inPortuguese.2---4
Alsointhissubsection,weemphasizethatthecutoff lev-elsofTCHCcitedcorrespondtovaluesusedintheU.S.group ofHM (MHAUS --- www.mhaus.org)protocol. Moreover,the protocoloftheEuropeanMHGroup(EMHG---www.emhg.org) differs fromthe U.S. onein additional aspectsthat were notmentioned,suchasthenumberoffragmentstested(six intheU.S. andfourin theEuropean protocol),halothane administration(singledoseof3%intheU.S.andan increas-ingdosefrom0.5%to3%intheEuropeanprotocol)andfinally thecutoff, whichis 0.2gtoforhalothane2%and0.2gfor caffeine2mmintheEuropeanprotocol.5,6
UnlikethatnotedbyCorreiaetal.,inBraziltheCedhima (CenterfortheStudy,DiagnosisandResearchforMalignant Hyperthermia),Escola Paulista de Medicina, Universidade FederaldeSãoPaulo(UNIFESP)usestheEuropeanMHgroup protocolforinvitromusclecontracturetesting(IVCT).4
In the same section ‘‘Malignant hyperthermia’’, item ‘‘Treatment’’,Correiaetal.includeasanindicated mea-surethe‘‘Replacementofanesthesiacircuitbyothercircuit uncontaminated by anesthetic agent’’. It is important to emphasizeherethatthereisnoindicationforthismeasure duringthetreatmentofacrisis,butonlyinthepreparation oftheanestheticmachineforanesthesiainapatientwitha historyofHM.AtthetimeofaMHcrisiswemust‘‘disconnect thevaporizer,butwithnowasteoftimechangingthe cir-cuitor the anesthetic machine’’.7 In ‘‘Dantrolene’’ item,
although Correiaetal. state thatthe modernclinical use ofdantroleneisrestrictedtomalignanthyperthermia,this drugisstillemployedinthemanagementofspasticity.8
Furthermore,themaintenanceofdantrolenefor24---48h aftertheinitialtreatmentofHMcrisisisimportanttoavoid
1 min 0.6 g
0.5% 1%
Figure1 Invitromusclecontracturetest(IVCT)inresponse