REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
A
randomized,
double
blind
trial
of
prophylactic
fibrinogen
to
reduce
bleeding
in
cardiac
surgery
Mostafa
Sadeghi
a,
Reza
Atefyekta
a,
Omid
Azimaraghi
a,
Seyed
Mojtaba
Marashi
a,
Yasaman
Aghajani
a,
Fatemeh
Ghadimi
a,
Donat
R.
Spahn
b,
Ali
Movafegh
a,∗aTehranUniversityofMedicalSciences,Tehran,Iran
bManagementUniversityandUniversityHospitalZurich,Zurich,Switzerland
Received22July2013;accepted30October2013 Availableonline11December2013
KEYWORDS
Bloodtransfusion; Bleeding;
Cardiacsurgery; Cardiopulmonary bypass;
Hemostasis
Abstract
Backgroundandobjectives: Postoperativebleedinghasagreatclinicalimportanceandcan
con-tributetoincreasedmortalityandmorbidityinpatientsundergoingcoronaryarterybypassgraft
surgery.Inthisprospective,randomized,double-blindstudy,weevaluatedtheeffectof
pro-phylacticadministrationoffibrinogenconcentrateonpost-coronaryarterybypassgraftsurgery
bleeding.
Methods:A total of 60 patients undergoing coronaryartery bypass surgerywere randomly
dividedintotwogroups.Patientsinthefibrinogengroupreceived1goffibrinogenconcentrate
30min prior to the operation, whilepatients inthe control group received placebo.
Post-operativebleedingvolumes,prothrombintime,partialthromboplastintime,INR,hemoglobin
andtransfusedbloodproductsinbothgroupswererecorded.Astrictredbloodcelltransfusion
protocolwasusedinallpatients.
Results:Therewerenosignificantdifferencesbetweenintra-operativepackedredbloodcells
infusioninthestudiedgroups (1.0±1.4infibrinogengroup,and1.3±1.1incontrolgroup).
Lesspostoperativebleedingwasobservedinthefibrinogengroup(477±143versus703±179,
p=0.0001).Fifteenpatientsinthefibrinogengroupand21inthecontrolgrouprequired
post-oppackedredbloodcellsinfusion(p=0.094).Nothromboticeventwasobservedthrough72h
aftersurgery.
Conclusion: Prophylactic fibrinogen reduces post-operative bleeding in patients undergoing
coronaryarterybypassgraft.
© 2013SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights
reserved.
∗Correspondingauthor.
E-mail:[email protected],[email protected](A.Movafegh).
0104-0014/$–seefrontmatter©2013SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Transfusãodesangue; Sangramento; Cirurgiacardíaca; Circulac¸ão extracorpórea; Hemostasia
Estudorandômicoeduplo-cegodeprofilaxiacomfibrinogênioparareduziro sangramentoemcirurgiacardíaca
Resumo
Justificativaeobjetivo:A hemorragia no período pós-operatório é de grande importância
clínicaepodecontribuirparaoaumentodamorbidadeemortalidadeempacientessubmetidos
àcirurgiaderevascularizac¸ãocoronária.Nesseestudoprospectivo,randômicoeduplo-cego,
avaliamosoefeitodaadministrac¸ãoprofiláticadeconcentradodefibrinogêniosobreo
sangra-mentoapóscirurgiaderevascularizac¸ãocoronária.
Métodos: Nototal, 60pacientes submetidosà cirurgiade revascularizac¸ãocoronáriaforam
randomicamentedivididosemdoisgrupos.Ospacientesdogrupofibrinogênioreceberam1g
deconcentradodefibrinogênio30minutosantesdaoperac¸ão,enquantoosdoentesdogrupo
controlereceberamplacebo. Osvolumesdesangramentonopós-operatório, tempode
pro-trombina,tempodetromboplastinaparcial,INR,hemoglobinaehemoderivadostransfundidos
emambososgruposforamregistrados.Umprotocolodecondutarigorosoparatransfusãode
hemáciasfoiusadoemtodosospacientes.
Resultados: Nãohouvediferenc¸assignificantesentreasinfusõesdeconcentradosdehemácias
nosgruposestudados(1,0±1,4nogrupofibrinogênioe1,3±1,1nogrupocontrole).Ogrupo
fibrinogênio apresentou menos sangramento no pós-operatório (477±143 versus 703±179,
p=0,0001).Quinzepacientesdogrupofibrinogênioe21dogrupocontroleprecisaramdeinfusão
deconcentradodehemáciasnopós-operatório(p=0,094).Eventotrombóticonãofoiobservado
durante72hapósacirurgia.
Conclusão:Profilaxia com fibrinogênio reduz o sangramento no período pós-operatório de
pacientessubmetidosàrevascularizac¸ãocoronária.
©2013SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos
direitosreservados.
Introduction
Optimal prevention and management of intra- and
post-operativebleedinghasagreatclinicalimportanceinvarious types of surgeries, including coronaryartery bypass graft surgery(CABG).Suchmanagementcanefficientlydecrease theamount ofblood productstransfusionandasa result, mayleadtolesstransfusionrelatedcomplications.
Twoto6percentofCABGsurgerypatientswouldbe
re-exploreddue tointraorpost-operative hemorrhage, which
can lead to high morbidity and mortality rates. Further-more,complications such assternalwound infections are more frequent along with post-operative transfusion.1---2
Consequently, the importance of any approach or
inter-vention to decrease intra- or post-operative hemorrhage
isobvious.2 Coagulopathy is onepossiblereasonof
exces-sivebleedingduringandfollowingsurgery.Multiplefactors includingplateletdysfunction,fibrinolysisandcoagulation
factordeficienciesmayaffectpost-operativebleeding
fol-lowingcardiacsurgery.3
During CABG surgery, low fibrinogen plasma
concen-tration may directly be associated with blood loss.4 This
associationislikelysincefibrinogenisessentialinthe
cross-linkingof plateletsduring primaryhemostasisandplaysa
centralrolein the coagulationcascade,5 andit had been
shownthatfollowinghemorrhage,fibrinogenconcentration
decreasesmorethanothercoagulationfactors.6---9
The purpose of present study was to investigate the
effectofpre-operativeinfusionoffibrinogenconcentrateon
post-operativebleedingvolumein CABG surgerypatients.
The percentageand amount of transfused blood products
wereconsideredassecondaryoutcomeparameters.
Methods
Following the approvalof thestudy protocol by the
Insti-tutionalEthicsCommittee,thistrialwasregisteredbythe
IranianRegistryofClinicalTrial.Allparticipantsprovideda
written formofconsentaftertheywerefullyinformedof
natureanddesignofthestudy.
Sixty patients, scheduled for first time elective CABG,
wereenrolled inthis double-blindedrandomized
placebo-controlled clinical trial. The patients with the following
criteria were not considered eligible to take part in this
study: previouslydiagnosed hematologicor liverdiseases,
uncontrolled or insulin dependent diabetes, pregnancy,
unstable angina, serumcreatinine more than130mol/L,
leftventricularejectionfractionless than35%,serum
fib-rinogenlevelsmorethan3.5g/L.Thepatientsalsoneeded
tobementallycapableofgivingawritteninformedconsent.
Usingacomputergeneratedrandomizationlist,patients
were assigned to fibrinogen and control groups. All the
requiredstudydrugswerepreparedbyananesthetistwho
wasnot involved in the surveillance of thepatients.
Fur-thermore,all thefluidplasticcontainerswerecoveredby
textile,socontentofplasticcontainerswasinvisible.
Anticoagulanttherapy withaspirin,warfarinand
clopi-dogrelwasdiscontinued48hpriortosurgery.Onarrivalto
theoperatingroom,allthepatientsreceivedoxygenviaa
facemaskatarateof4L/min,andan18-gaugeintravenous
catheterwasplacedinaperipheralveintoallowfor
hydra-tionofthepatientsusinglactatedringer’ssolution(7mL/kg)
and administration of medications. Standard monitoring
whichconsistedofinvasiveandnon-invasivearterialblood
and capnometery wasinitiated and continued throughout anesthesia.
Anesthesiawasinducedby1mgofIVmidazolam,8g/kg
of IV fentanyl and 3mg/kg of IV sodium thiopental, and
0.1mg/kg of IV pancuronium bromide. Prior to the start
ofsurgeryapercutaneouscentralvenous linewasplaced.
Isoflurane was used for maintaining general anesthesia.
Beforebeginningofcardiopulmonarybypass,abaseline
acti-vated clotting time (ACT) was measured and an IV bolus
doseofheparin(400U/kg)wasadministeredtoallpatients.
Next heparindosing wastargetedto maintainACT values
more than 480seconds. Myocardial protection techniques
wereidenticalinbothgroups,andprimingoftheblood
car-dioplegialinewasperformedonCPBwithautologousblood.
Identicalfluidtherapywasusedinbothgroups.
Inthefibrinogen groupthepatients received1gramof
fibrinogendissolvedin50mLofnormalsalineovera15min
period30minbeforeinductionofanesthesia.Inthecontrol
groupthepatientswereadministeredthesamevolumeof
normalsalineduringthesameperiodoftimeasaplacebo.
Allthedrugswerepreparedandadministeredbyan
anes-thetistwhowasnotanyhowinvolvedinthestudy.
Hemoglobin concentration, platelet count, partial
thromboplastin time (PTT), prothrombin time (PT) and
plasma fibrinogen concentrations were measured before
induction of general anesthesia and were repeated again
24hfollowingsurgery.Plasmaconcentrationsoffibrinogen
were adjusted to a standard hematocrit of 40%
accord-ing to the formula: corrected concentration=measured
concentration×(standard hematocrit/measured
hemat-ocrit).Hematocritlevelsweremeasuredevery30minuntil
termination of bypass.Red blood cells were transfused if
the intraoperative hematocrit was less than 20%. In the
intensive care unit,hematocrit valuesless than25% were
consideredastransfusiontrigger.Plasmawasadministered
in patients with ongoing bleeding and abnormal PT or
PTT. Platelets weretransfused withongoing bleeding and
plateletscountlessthan7×109perliter.
Post-operative bleeding was described as the overall
chesttubedrainageduringthefirst12post-operativehours
and was recorded by a trained intensive care nurse. The
amountof transfusedpackedredbloodcells, freshfrozen
plasma,andplateletsduringthefirst24hpost-surgerywere alsodocumented.Foraperiodof72hfollowingsurgery
clin-icalsignsandsymptomsofthromboticadverseeffectswere
followedandrecorded.Ifanyoftheseeventsoccurred,the
patientwasconsidered acandidatefor furtherevaluation
suchasDopplerultrasound.
Statistics
Itwasdeterminedthatasamplesizeof18patientsineach
groupwould besufficienttodetect a minimumof 200mL
bleedingdifferencesin 12h followingsurgerywitha
stan-dard deviation of 150mL, power of 90% and a significant
levelof0.01.
StatisticalanalysisofthedatawasperformedusingSPSS
forwindowsversion17(SPSS,Chicago,IL).Thedistribution
of data waschecked by Kolmogorov---Simonov test, which
consistedofanormaldistribution.Groupcomparisonswere
performedwithtwo-samplet-testsforcontinuousdata.Sex
wascomparedby2test.Statisticalsignificancewasdefined asap-value<0.05.
Results
Atotalof60patients(70%male,30%female)wereenrolled
in this study. There was no protocol violation and all of
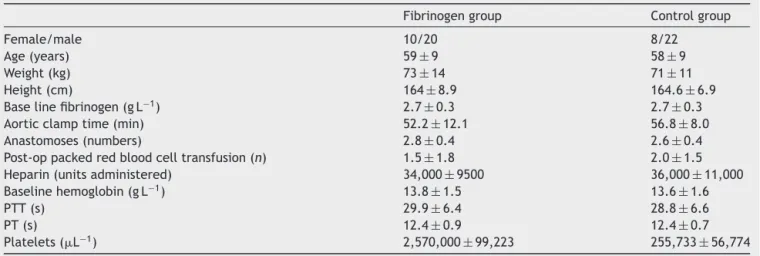
theparticipantswereincludedintheanalysis.Basic
char-acteristicsoftheparticipantssuchasage,weight,height,
aorticclamptimeandnumberofanastomosesweresimilar
betweenbothgroups(Table1).Baselineandpost-operative
laboratoryvariablesincludingPTT,PT,hemoglobin
concen-tration and platelet count in both fibrinogen and control
groupsweresimilar(Table2).
Post-operatively,alowerbloodlosswasobservedinthe
fibrinogen group (477±143) in comparison with the
con-trol group (703±179) (p<0.0001) (Fig. 1). Fifteen (50%)
patients in the fibrinogen group and 21 (70%) patients in
the control group received packed red blood cells
post-operatively, and there were no significant differences in
groups (p=0.094).Yet, totalamount of packedred blood
cellsinfusioningroupsdidnotdiffersignificantly(p=0.096).
Table1 Basiccharacteristicsofthepatientsandbaselinecoagulationvalues.
Fibrinogengroup Controlgroup
Female/male 10/20 8/22
Age(years) 59±9 58±9
Weight(kg) 73±14 71±11
Height(cm) 164±8.9 164.6±6.9
Baselinefibrinogen(gL−1) 2.7±0.3 2.7±0.3
Aorticclamptime(min) 52.2±12.1 56.8±8.0
Anastomoses(numbers) 2.8±0.4 2.6±0.4
Post-oppackedredbloodcelltransfusion(n) 1.5±1.8 2.0±1.5
Heparin(unitsadministered) 34,000±9500 36,000±11,000
Baselinehemoglobin(gL−1) 13.8±1.5 13.6±1.6
PTT(s) 29.9±6.4 28.8±6.6
PT(s) 12.4±0.9 12.4±0.7
Platelets(L−1) 2,570,000±99,223 255,733±56,774
aDatawerepresentedmean±SD.
Table2 Coagulationatpostoperativeday1.
Post-operativevalue Fibrinogengroup Controlgroup
Hemoglobin(gdL−1) 9.7±1.39 8±1.2
PTT(s) 40.5±25.2 44.7±18.1
PT(s) 15.6±8.5 14.6±2.1
Platelets(L−1) 1,670,000±55,000 1,680,000±54,000
Fibrinogen(gdL−1) 2.9±0.4 2.9±0.4
aDatawerepresentedasmean±SD. bThereisnosignificantdifferenceingroups.
1200
1000
800
600
400
200
0 0
1 2
P
ost-oper
ativ
e b
leeding (mL)
Figure 1 Post-operative bleeding (the overall chest tube
drainage duringthe first 12 post-operative hours) inthe
fib-rinogengroup(1)comparedtothecontrolgroup(2).
There were no significantly differences in the number of packedredblood cells infusionin groups(1.5±1.8 inthe fibrinogengroup,and2.0±1.5inthecontrolgroup).Four patientsinthefibrinogengroupreceivedfreshfrozenplasma toincomparisonto2inthecontrolgroup(ns).Onlyoneof patientsinthefibrinogengroupreceivedaplatelet transfu-sion.
Inneither ofgroups anyclinically apparentthrombotic
eventswerefound.
Discussion
Thisstudyshowedthattheimmediatepreoperative adminis-trationoffibrinogenconcentratestoCABGsurgerypatients
candecreasepost-operativehemorrhage.
Surgicalbleedingisamajorconcernincardiacsurgery.10
Preventingbloodproducttransfusionanddecreasing
hem-orrhagedependent re-exploration rates improvepatients’
outcomesandcouldlowertheoverallburdenonhealthcare
costs.11
Relatively low fibrinogen concentrations may play an
important role in bleeding following cardiac surgery.12,13
Low preoperative fibrinogen level has been found to be
an independent predictor of post-operative bleeding and
transfusion,13 lowfibrinogen levelsduring andafter CABG
surgery were found to be associated with bleeding14,15
andfibrinogenadministrationaftercardiopulmonarybypass
reducedthebleedingsignificantly.16 Andlastbutnotleast, inthesofaronlysmallprospectiverandomizedstudy,
Karls-son et al. showed in 20 patients that the preoperative
administrationof2goffibrinogendecreasedpostoperative
blood lossand minimizedthe decreaseof thehemoglobin
concentration postoperatively.13 Our study confirms these
resultsandexpandstheknowledgeinalargergroupof60
patientsinthatalreadytheadministrationof1gof fibrino-geniscapableofreducingpostoperativebleedinginpatients
undergoingfirsttimeCABGsurgery.
Karlssonetal.alsolookedat thromboticcomplications
andconcludedthatthe administrationof 2goffibrinogen
wassafe in thisregard.12 We confirm this conclusion in a
largergroupofpatientsalthough weonlyassessedclinical
thrombotic events. We thus concluded that
prophylac-tic fibrinogen infusion significantlyreduces post-operative
bleedingwithoutclinicaladverseevents.Yet,the investiga-tionofKarlsonetal.wasapilotstudyandonly10patients participatedinit.So,thepowerofstudyisnotsufficientto makeastrongconclusion.Inourstudy,prophylactic adminis-trationoftheloweramountoffibrinogen(1g)couldreduce
thepost-operativebloodlossby32%;however,thedecrease
in ablood transfusionwasnotsignificant but therewasa
trend.
In our study, the packed red blood cells infusion was
notdifferentstatisticallyingroups;however,basedon
cal-culated p value (p=0.096), it is possible that the power
of the study was not sufficient to show such a
differ-ence.Asthepresentsamplesizewasestimatedconsidering
post-operativehemorrhageasaprimaryoutcome,ahigher
poweredstudyisnecessarytoassesstheeffectoffibrinogen
concentrateadministrationonpost-CABGpackedredblood
cellsinfusion.
Therearelimitationsofthisstudysuchasthelackofany
form of thromboelastometric monitoring (TEG or ROTEM)
perioperativelyandthefixeddose(1g)offibrinogen.Future
studies with individualized and more precise coagulation
monitoring are needed to define the optimal dose of
fib-rinogen.Therationaleforchoosingthepresentdosagewas
based on a previous study conducted by Karlsson et al.13
and due tothe fact that the plasma fibrinogen level was
notevaluatedfrequentlyinourstudyaimingatdecreasing
thepostoperativebloodlossalongwithminimalthrombotic
adverseeffects.
In conclusion, administration of 1g of intravenous
fib-rinogenconcentratebeforeinductionofgeneralanesthesia
inCABGsurgerycanreducepost-operativebleeding.
Conflicts
of
interest
References
1.ZachariasA, HabibRH.Factors predisposingto median ster-notomy complications. Deep vs superficial infection. Chest. 1996;110:1173---8.
2.Unsworth-WhiteMJ,HerriotA,ValenciaO,etal.Resternotomy forbleeding aftercardiacoperation:a markerfor increased morbidityandmortality.AnnThoracSurg.1995;59:664---7.
3.PaparellaD, BristerSJ, Buchanan MR. Coagulation disorders of cardiopulmonary bypass: a review. Intensive Care Med. 2004;30:1873---81.
4.WahbaA,RotheG,LodesH,etal.Predictorsofbloodlossafter coronaryarterybypassgrafting. JCardiothorac VascAnesth. 1997;11:824---7.
5.FurieB,FurieBC.Mechanismsofthrombusformation.NEnglJ Med.2008;28:938---49.
6.MosessonMW.Fibrinogenandfibrinstructureandfunctions.J ThrombHaemost.2005;3:1894---904.
7.Standeven KF, Ariens RA, Grant PJ. The molecular physiol-ogy and pathology of fibrin structure/function. Blood Rev. 2005;19:275---88.
8.AljassimO,KarlssonM,WiklundL,etal.Inflammatoryresponse andplateletactivationafteroff-pumpcoronaryarterybypass surgery.ScandCardiovascJ.2006;40:43---8.
9.HiippalaST, Myllyla GJ,Vahtera EM. Hemostaticfactors and replacementofmajorbloodlosswithplasma-poorredcell con-centrates.AnesthAnalg.1995;81:360---5.
10.Pavie A, Szefner J, Leger P, et al. Preventing, minimiz-ing, and managingpostoperativebleeding. Ann ThoracSurg. 1999;68:705---10.
11.DespotisGJ,SkubasNJ,GoodnoughLT.Optimalmanagementof bleedingandtransfusioninpatientsundergoingcardiacsurgery. SeminThoracCardiovascSurg.1999;11:84---104.
12.Karlsson M, Ternström L, Hyllner M, Baghaei F, Nilsson S, Jeppsson A. Plasma fibrinogen level, bleeding, and transfu-sionsafteron-pump coronaryarterybypassgrafting surgery: aprospectiveobservationalstudy.Transfusion(Paris).2008;48: 2152---8.
13.Karlsson M, Ternström L, Hyllner M, et al. Prophylactic fibrinogen infusion reduces bleeding after coronary artery bypasssurgery.Aprospectiverandomizedpilotstudy.Thromb Haemost.2009;102:137---44.
14.BlomeM,IsgroF,KiesslingA,etal.Relationshipbetweenfactor XIIIactivity,fibrinogen,haemostasisscreeningtestsand post-operativebleedingincardiopulmonarybypasssurgery.Thromb Haemost.2005;93:1101---7.
15.Rahe-Mayer N, Pichlmaier M, Haverich A, et al. Bleeding management with fibrinogen concentrate targeting a high-normal plasmafibrinogen level: a pilotstudy. Br JAnaesth. 2009;102:785---92.