RESUMO
Objei vou-se invesi gar por meio de uma equipe muli disciplinar o estado neurológi-co e o desempenho neurológi-cognii vo de pacientes pós-AVC mediante um estudo transversal com 45 pacientes em processo de reabi-litação após um AVC agudo. Ui lizaram-se como instrumentos de coleta de dados uma fi cha de avaliação, o Mini Mental--MEEM e o Nai onal Internai onal Health Stroke Scale-NIHSS. Amostra predominan-temente feminina (55,6%), AVC Isquêmico (86,7%), Hemisfério cerebral direito (60%) e Escolarizados (68,8%). A média do MEEM para escolarizados e analfabetos foi de 19,3 ± 5,0 e 15,92 ± 3,7 respeci vamente. A média geral do estado neurológico en-contrado foi 13,0±4,8. Houve diferença signi fi cai va entre as médias cognii vas dos pacientes quanto à escolaridade (p valor = 0,017) e relação signifi cai va entre o estado
neurológico e o desempenho cognii vo (r = -0,44 p valor = 0,002). O estado neurológi-co e o nível neurológi-cognii vo de pacientes pós-AVC agudo parecem estar diretamente relacio-nados, o que evidencia a necessidade de maior atenção à questão cognii va envol-vida no início do processo de reabilitação.
DESCRITORES Acidente cerebral vascular Cognição
Avaliação Reabilitação
The neurological state and cognition
of patients after a stoke
*O
RIGINAL
A
R
TICLE
ABSTRACT
The objeci ve of this study was to have a muli disciplinary team invesi gate the neurological state and cognii ve perfor-mance of pai ents at er a stroke, through a cross-seci onal study with 45 pai ents in rehabilitai on at er having an acute stroke. The data colleci on instruments used were an assessment sheet, the Mini Mental-ME-EM, and the Nai onal Internai onal Health Stroke Scale-NIHSS. The sample consisted mostly of women (55.6%), Ischemic Stroke (86.7%), right hemisphere of the brain (60%) and Educated (68.8%). The mean MEEM for educated and illiterate pai ents was 19.3 ± 5.0 and 15.92 ± 3.7, respeci -vely. The overall mean of the neurological state was 13.0±4.8. A signifi cant diff erence
was found between the cognii ve means of pai ents in terms of educai on (p value = 0.017), and there was a signifi cant
rela-i onship between the neurological state and cognii ve performance (r = -0.44 p va-lue = 0.002). It appears to be a direct re-lai onship between the neurological state and cognii on performance of pai ents af-ter an acute stroke, which evinces the need for greater at eni on to the cognii ve issue involved early in rehabilitai on.
DESCRIPTORS Stroke
Cognii on Evaluai on Rehabilitai on
RESUMEN
Se objei vó invesi gar mediante equipo muli disciplinario el estado neurológico y el desempeño cognii vo de pacientes post-ACV. Estudio transversal con 45 pa-cientes post-ACV agudo en proceso de re-habilitación. Se ui lizaron para recolección de datos una fi cha de evaluación; el Mini
Mental-MEEM y el Nai onal Internai onal Health Stroke Scale-NIHSS. Muestra pre-dominantemente femenina (55,6%), ACV Isquémico (86,7%), Hemisferio cerebral derecho (60%) y Escolarizados (68,8%). La media de MEEM para escolarizados y analfabetos fue 19,3±5,0 y 15,92±3,7 res-peci vamente. La media general del estado neurológico encontrado fue 13,0±4,8. Exis-i ó diferencia signifi cai va entre las medias
cognii vas de pacientes respecto de esco-laridad (pvalor=0,017), y relación signifi ca-i va entre el estado neurológico y el des-empeño cognii vo (r=0,44 pvalor=0,002). El estado neurológico y el nivel cognii vo de pacientes post-ACV agudo parecen es-tar directamente relacionados, lo que evi-dencia la necesidad de mayor atención a la cuesi ón cognii va involucrada en el inicio del proceso de rehabilitación.
DESCRIPTORES Accidente cerebrovascular Cognición
Evaluación Rehabilitación
Fabrícia Azevêdo da Costa1, Diana Lidice Araujo da Silva2, Vera Maria da Rocha3
ESTADO NEUROLÓGICO E COGNIÇÃO DE PACIENTES PÓS-ACIDENTE VASCULAR CEREBRAL
ESTADO NEUROLÓGICO Y COGNICIÓN DE PACIENTES POST ACCIDENTE CEREBRO-VASCULAR
The ability of patients to succeed in rehabilitation depends
on their motivation, social-family support, and, most importantly,
their cognitive condition. INTRODUCTION
Cerebrovascular Accident (CVA) is defi ned by the World Health Organizai on (WHO) as an acute neurologi-cal dysfunci on of vascular origin followed by the sudden or rapid occurrence of signs and symptoms related to compromised focal areas in the brain(1).
The incidence of CVA has grown due to increased life expectancy, causing changes in the populai on’s lifestyle(2).
CVA is the cause of 9% of deaths around the world, rank-ing second at er ischemic heart diseases(3).
The propori on of deaths from CVA is 10-12% in West-ern countries, while 12% of these deaths occur in people younger than 65 years old(3). In Brazil, the distribui on of
deaths caused by diseases in the circulatory system have increased in signifi cance among young adults older than 20 years of age and has become the main cause of death among those in the 40 years old age range, and predomi-nai ng in the subsequent age groups(4-5).
CVA is a common disease having a great impact on world public health because it is the main
cause of neurological impairment and im-portant motor and cognii ve dysfunci ons(2).
Those surviving a CVA generally face residu-al impairment such as parresidu-alysis of muscles, siff ness of the aff ected body parts, loss of joint mobility, diff use pain, memory prob-lems, diffi culi es in oral and writ en commu-nicai on, and sensory disabilii es(2,4).
The growth of the elderly populai on has increased the risk for the onset of cognii ve impairment since the risk for CVA occurrence also increases(6). Cognii ve dysfunci ons are
the main causes of impairment in people older than 65 years of age in industrialized countries. Taking into account that Brazil is considered a developing country whose clas-sifi cai on for elderly individuals includes those around 60 years of age, such informai on is even more relevant(1,6).
Reports in the literature indicate that 5% to 10% of the elderly populai on presents some cognii ve decline. Since CVA is one of the main causes of this type of impairment, the incidence of cognii ve disorders in the populai on sur-viving a CVA varies from 12% to 56%(6-7). CVA can be
con-sidered the main cause of cognii ve impairment in elderly individuals, aff eci ng about 50% of pai ents, both in the acute and chronic phases(7-8).
Cognii ve impairment is very common at er a CVA and can aff ect at eni on, memory and the associai on of these two skills. Such a fact reduces the organizai on of thoughts, leading to a disorganized language process, including problems related to speech and the sequeni al produci on of words, compromising one’s ability to under-stand writ en and spoken informai on(9).
Individuals with sequelae resuli ng from a CVA fre-quently need to take part in a rehabilitai on program. Rehabilitai on is a set of aci ons aimed to reestablish and maintain one’s physical funci ons; educate the pai ent and family; and reinsert the pai ent into the family’s and social circle(1,5). The ability of pai ents to succeed in
rehabilita-i on depends on their moi vai on, social-family support, and, most importantly, their cognii ve condii on(10).
The presence of cognii ve disorders is an important predictor of recovery, directly aff eci ng the pai ents’ reha-bilitai on and recovery process(11). Many studies suggest
that a pai ent’s cognii ve state can infl uence the results of treatment, given the fact that the techniques used in the process require some cognii ve skills such as the
evoca-i on and execui on of instruci ons(10).
These pai ents are required to learn new skills to per-form exercises and recall instruci ons during the rehabili-tai on process. Thus, an individual’s compromised memo-ry, for instance, can aff ect the success of a rehabilitai on program(12).
In this context, an early diagnosis, jointly with the prognosis of the pai ent’s cognii ve
poten-i al, can be very important to determining the best strategy to implement for these pai ents, since interveni ons designed to recover from and/or compensate for
cogni-i ve impairment can be inii ated during the acute phase of CVA, which is an important factor in treatment eff eci veness(8).
However, even though there is meni on in the literature of cognii ve impairment af-ter a brain damage, most studies addressing cognii ve funci oning at er a CVA have fo-cused on the development of demeni a(13).
Data concerning the relai onship between the pai ents’ neurological states at the i me they begin physical therapy and their cognii ve performance is limited.
Therefore, therapeui c procedures are limited since there are few studies guiding the implementai on of a therapeui c program focused on pai ents’ cognii ve needs.
This study reports the neurological state and cognii ve performance of post-CVA pai ents that are part of a physi-cal therapeui c rehabilitai on program, invesi gated by a muli -disciplinary team (Physical Therapists, Occupai onal therapists and speech and hearing therapists).
METHOD
This is a cross-seci onal analyi cal study. The
Cen-ter, and Adult Rehabilitai on Center) between May 2007 and May 2008.
The coni ngency sample was composed of 45 indi-viduals selected according to the following inclusion cri-teria: (a) having a CVA diagnosis confi rmed by comple-mentary exam (CT or MRI); (b) having been cared for by the physical therapy service in one of the chosen insi
tu-i ons in the research period; (c) being 40 to 90 years old; (d) i me of CVA less than three months prior at the i me of assessment; and (e) CVA had to be unilateral and non-recurrent.
Exclusion criterion was the presence of associated pathologies that could cause cognii ve sequelae beside those caused by CVA, such as Parkinson and Alzheimer’s disease. Pai ents with severe aphasia and visual impair-ments were also avoided.
Data colleci on instrument
A physical therapy form was used to collect general informai on about pai ents, such as idenifi cai on, clini-cal condii on, history of current disease, pathological and family antecedents, lifestyle, medicai on and physical assessment (palpai on and inspeci on) according to the model used by the Physical Therapy Service at the Onofre Lopes University Hospital (HUOL-UFRN).
The Mini Mental State Examinai on (MMSE) was used to evaluate the cognii ve condii on of pai ents. This instrument idenifi es evidence of cognii ve impairment in pai ents(14) and is divided into seven dimensions
in-cluding: i me and spai al orientai on, immediate mem-ory, at eni on and calculus, evocai on, language and visual construci on. Its total score varies from 0 to 30. This instrument was validated for Brazil and takes into account the age and educai onal level of the interviewed individuals(15).
The Stroke Scale by the Nai onal Insi tute of Health (NIHSS), the validity and reliability of which is well doc-umented both in Brazilian and internai onal literature, was used to quani tai vely assess the neurological state of pai ents(16-18). This scale is composed of 11 items that
include: level of consciousness, eye movements, visual fi elds, facial palsy, motor funci on and limb ataxia, sen-sory, language, dysarthria, and spai al neglect(18). In this
scale, the higher the pai ent’s score, the more severe is his/her neurological state. Scores below 5 at the i me of admit ance suggest mild clinical severity; scores between 6 and 13 indicates moderate severity; and scores equal to or greater than 14 indicate a more advanced level of clini-cal severity(16).
Data colleci on procedures
The research project was inii ally submit ed to the Research Ethics Commit ee guiding research with human
subjects at the Federal University of Rio Grande do Norte (UFRN). At er its approval, in accordance with resolui on 196/96 protocol No. 12/2007 CEP/UFRN, the researchers were trained to collect data in order to standardize the procedures. Before the applicai on of the protocol, each pari cipant was informed of the study’s objeci ves and limitai ons and signed a free and informed consent form confi rming their voluntary pari cipai on. The instruments were applied only once at the beginning of the physical therapy.
The data obtained were tabulated and stai si cally analyzed through SPSS version 13.0. According to the Kolmogorov-Smirnov normality test and a level of signifi -cance fi xed at 5%, a normal distribui on of data was as-sumed in this study.
Descripi ve stai si cs (frequency, averages and stan-dard deviai on) are presented to characterize the
inves-i gated sample. Infereni al stai si cs was applied to the remaining analyses. To verify the existence of signifi cant diff erences between the cognii ve averages concerning educai on, the Student t test was inii ally used in
inde-pendent samples and Pearson’s correlai on test was applied to check for the existence of a correlai on be-tween cognii ve performance and the neurological state of pai ents.
RESULTS
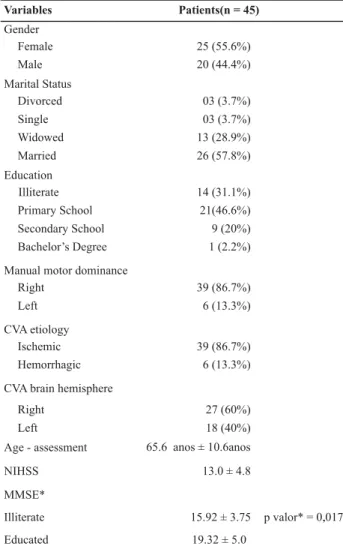
The studied sample was characterized in terms of per-sonal aspects (gender, marital status, age and schooling) and clinical aspects (ei ology of CVA, aff ected brain hemi-sphere, manual motor dominance). The results indicated a sample of 45 predominantly female (55.6%) and mar-ried pai ents (57.8%). The average age of the individuals was 65.6 years old (±10.6). The majority had at ended pri-mary school (n=21, 46.6%), followed by illiterate individu-als (n=14, 31.1%).
In relai on to clinical characterisi cs, the most preva-lent CVA ei ology was Ischemic CVA (86.7%) and the right brain hemisphere was the most aff ected (60%). In relai on to laterality, 86.7% of the pai ents were right-handed.
Source: study’s data.
*CVA – Cerebrovascular accident; NIHSS – NIH Stroke Scale; MMSE – Mini Mental State Examination.
Finally, when analyzing the existence of a relation-ship between the patients’ neurological state and cognitive performance, we verified the presence of a negative and significant relationship (r= -0.34 p-value =0.002), which shows that the greater the neurologi-cal severity, the worse the cognitive performance of pa-tients (Figure 1).
DISCUSSION
Current rehabilitai on programs directed to post-CVA pai ents neglect the cognii ve dimension of these
pa-i ents, which seems to hinder the success of their treat-ment. Appropriate treatment may favor recovery in
pa-i ents who are cognii vely compromised when admit ed into a rehabilitai on unit in the inii al phase of CVA(6). With
this in mind, this study was conducted to invesi gate, us-ing a muli -disciplinary team, the neurological state and cognii ve performance of post-CVA pai ents with up to three months of brain damage at the i me they were
ad-mit ed into the public physical therapy services in the city of Natal, RN, Brazil.
Table 1 – Characterization of patients in relation to personal and clinical aspects – Natal, RN, Brazil 2008
r = -0.44 p value = 0.002 Source: study’s data.
*NIHSS - National Institute of Health Stroke Scale; MMSE – Mini Mental State Examination.
Figure 1 – Correlation between the post-CVA patients’ neurologi-cal condition and cognitive performance - Natal, RN, Brazil - 2008
The results revealed a sample of pai ents with an av-erage age of 65 years old, a fact consistent with the lit-erature that reveals a greater concentrai on of individuals older than 60 years of age with cardiovascular diseases(1,4).
Addii onally, the inii al assessment showed a moderate neurological state (average of NIHSS 13 ± 4.8), which indi-cates the need to understand the cognii ve level of these pai ents to implement a more eff eci ve treatment.
Some authors report that the fi nal score obtained by pai ents in the NIHSS at the i me of their admit ance into the therapy service can help plan the recovery of
pa-i ents by predici ng the care required in the long term(16).
According to these authors, more than 80% of pai ents scoring less than 5 points at the i me of admit ance are discharged quickly without major intercurrences. Those scoring between 6 and 13, however, usually require a more elaborate rehabilitai on program. Finally, those scoring 14 or more, frequently require more intensive re-habilitai on care and for a more prolonged period(16).
The cognii ve dimension is evident in the case of
pa-i ents with severe levels of neurological impairment be-cause the severity of CVA seems to be related to a tenden-cy for individuals to present cognii ve dysfunci on. Such a dimension stands out when one acknowledges the need for cognii ve integrity to experience therapeui c success.
The eff ect of the pai ents’ cognii ve condii on in the CVA rehabilitai on process presents a diff erent context(10).
Variables Patients(n = 45)
Gender
25 (55.6%) 20 (44.4%)
Marital Status
03 (3.7%) 03 (3.7%) 13 (28.9%)
26 (57.8%)
Education
14 (31.1%) 21(46.6%)
9 (20%) 1 (2.2%)
Manual motor dominance
39 (86.7%)
6 (13.3%)
CVA etiology
39 (86.7%)
6 (13.3%)
CVA brain hemisphere
27 (60%) 18 (40%)
Age - assessment 65.6 anos ± 10.6anos
NIHSS 13.0 ± 4.8
MMSE*
Illiterate
Educated
15.92 ± 3.75 p valor* = 0,017.
19.32 ± 5.0 Female
Male
Divorced Single Widowed
Married
Illiterate Primary School
Secondary School Bachelor’s Degree
Right
Left
Ischemic
Hemorrhagic
Right Left
5,00 10,00 15,00 20,00 25,00 30,00
5,00 10,00 15,00 20,00 25,00 30,00
MMSE
0,00 5,00 10,00 15,00 20,00 25,00
0,00 5,00 10,00 15,00 20,00 25,00 30,00
It occurs because the eff ect of cognii on on the
rehabilita-i on process is a mat er of great controversy and has led the scienifi c community to much debate(11-12).
Research-ers have reported that pai ents with cognii ve impairment can improve their funci oning when at ending a rehabili-tai on program(10).
In this context, various studies have tried to ideni fy the relai on between the success of rehabilitai on and the degree of cognii ve impairment, leading researchers to suggest that a cognii ve assessment should be part of the rehabilitai on process(10-12). Studies with post-CVA
pa-i ents have shown that individuals with some cognii ve defi cit present unsai sfactory results in the rehabilitai on process. This may occur in pai ents with sensory or at
en-i on defi cit, or compromised learning and comprehension skills(11-12).
In agreement with this rai onale, some researchers suggest that an individual’s cognii ve state can infl uence the results of treatment because the techniques used in this process require certain cognii ve skills, such as
evoca-i on and performance of instruci ons, and these skills are generally compromised in these pai ents(10).
In this study, the cognii ve assessment of pai ents was performed using the MMSE. The results indicated that the averages obtained by pai ents in this instrument were be-low the cutoff points proposed for the Brazilian
popula-i on in the MMSE validai on(15), both for educated and
illit-erate pai ents, suggesi ng this populai on presented some level of cognii ve impairment.
A study using the MMSE and addressing the diagno-sis of demeni a in Brazil proposed cutoff points of 23 and 24 for educated elderly individuals and 19 and 20 for il-literate individuals, highlighi ng the infl uence of pai ents’ educai onal level on their cognii ve performance(15). Such
fi ndings are corroborated by those obtained in this study in which educated pai ents presented cognii ve averages greater than that of illiterate pai ents; the diff erence was stai si cally signifi cant (p value=0.017).
Finally, we invesi gated whether the neurological state of pai ents at the i me they were admit ed into the physical therapy service was related to their cognii ve performance. A negai ve and very signifi cant relai on
was found, which was evidence that the more severe the neurological state of pai ents, the worse was their
cogni-i ve performance.
Such a fact is highly relevant for the implementai on of a rehabilitai on program. The cognii ve-motor infl u-ence is of considerable clinical importance, since the per-formance of exercises requires simultaneous motor and cognii ve skills(19). Therefore, cognii ve domains aff ected
by neurological impairment should be idenifi ed so that more coherent treatment planning is devised and, conse-quently, pai ents achieve improved recovery from neuro-logical and cognii ve damage(19-20).
An early diagnosis jointly with the prognosis of
poten-i al cognii ve recovery can be very important in the de-terminai on of bet er interveni ons to be implemented for these pai ents, since interveni ons intended to recover from and/or compensate for cognii ve impairment could be inii ated in the CVA acute phase, which is important for treatment eff eci veness(8).
CONCLUSION
According to the fi ndings of this study, we conclude that the level of neurological severity found in the inii al assessment of pai ents at the i me they were admit ed in-to the physical therapy service was moderate and the cog-nii ve performance was below the Brazilian cutoff points. Addii onally, the study indicated that these two variables seem to be directly related, which shows the need to pay more at eni on to the cognii ve dimension involved at the beginning of the rehabilitai on process of these pai ents.
Despite the relevance of the fi ndings, this study pres-ents a certain limitai on since poteni al infl uences of how extensive the damage was and the topography of dam-age on the cognii ve state of the studied pai ents were not considered. However, since the NIHSS was applied and this instrument evaluated the severity of an individual’s neurological condii on, we believe this limitai on has lit le signifi cance for this study. Hence, we expect that its fi nd-ings will contribute to future studies addressing the
cogni-i ve level of post-CVA pai ents, aiming to develop thera-peui c interveni ons consistent with this clinical situai on.
REFERENCES
1. World Health Organizai on (WHO). Cerebrovascular disorders. Geneva: WHO; 1978.
2. Andrade LM, Costa MFM, Caetano JA, Soares E, Beserra EP. A problemái ca do cuidador familiar do portador de acidente vascular cerebral. Rev Esc Enferm USP. 2009;43(1):37-43.
3. Donnan GA, Fisher M, Macleod M, Davis SM. Stroke. Lancet. 2008;371(9624):1612-23.
4. Falcão IV, Carvalho EMF, Barreto KML, Lessa FJD, LeiteVMM. Acidente vascular cerebral precoce: implicações para adultos em idade produi va atendidos pelo Sistema Único de Saúde. Rev Bras Saúde Mater Infant. 2004;4(1):95-102.
6. Rabadi MH, Rabadi FM, Edelstein L, Peterson M. Cognii vely im-paired stroke pai ents do benefi t from admission to an acute rehabilitai on unit. Arch Phys Med Rehabil. 2008;89(3):441-8.
7. Glymour MM, Weuve J, Fay ME, Glass T, Berkman LF. Social i es and cognii ve recovery at er stroke: does social inte-grai on promote cognii ve resilience? Neuroepidemiology. 2008;31(1):10-20.
8. Nys GM, Van Zandvoort MJ, De Kort PL, Jansen BP, Van Der Worp HB, Kappelle LJ, et al. Domain-specifi c cognii ve recov-ery at er fi rst-ever stroke: a follow-up study of 111 cases. J Int Neuropsychol Soc. 2005;11(7):795-806.
9. Vukovic M, Vuksanovic J, Vukovic I. Comparison of the recov-ery pat erns of language and cognii ve funci ons in pai ents with post-traumai c language processing defi cits and in pa-i ents with aphasia following a stroke. J Commun Disord. 2008;41(6):531-52.
10. Hershkovitz A, Brill S. The associai on between pai ents´cognii ve status and rehabilitai on outcome in geriatric day hospital. Dis-abil RehDis-abil. 2007;29(4):333-7.
11. Zinn S, Dudley TK, Bosworth HB, Hoening HM, Duncan PW, Horner RD. The eff ect of poststroke cognii ve impairment on rehabilitai on process and funci onal outcome. Arch Phys Med Rehabil. 2004;85(7):1084-90.
12. Luk JK, Chin PK, Chu LW. Rehabilitai on of older Chinese pa-i ents with diff erent cognii ve funci ons: how did they diff er in outcome? Arch Phys Med Reahabil. 2008;89(9):1714-9.
13. Rasquin SM, Verhey FR, Lousberg R, Lodder J. Cognii ve per-formance at er the fi rst ever stroke related to progression of vascular brain damage: a 2 year follow up CT scan study. J Neurol Neurosurg Psychiatry. 2005;76(8):1075-9.
14. Folstein MF, Folstein SE, McHugh PR. Mini-Mental State: a praci cal method for grading the cognii ve state of pai ents for the clinician. J Psychiatr Res. 1975;12(3):189-98.
15. Almeida OP. Mini Exame do Estado Mental e o diagnósi co de demência no Brasil. Arq Neuropsiquiatr. 1998;56(3B):605-12.
16. Schlegel D, Kolb SJ, Luciano JM, Tovar JM, Cucchiara BL, Li-ebeskind DS, et al. Ui lity of the NIH Stroke Scale as a predic-tor of hospital disposii on. Stroke. 2003;34(1):134-7.
17. Cincura C, Pontes-Neto O, Neville L, Mendes H, Menezes D, Mariano D, et al. Validai on of the Nai onal Insi tutes of Health Stroke Scale, modifi ed Rankin Scale and Barthel In-dex in Brazil: the role of cultural adaptai on and structured interviewing. Cerebrovasc Dis. 2009; 27(2):119-22.
18. Caneda M, Fernandes J, Almeida A, Mugnol F. Confi abilidade de Escalas de Compromeni mento Neurológico em paci-entes com acidente vascular cerebral. Arq Neuropsiquiatr. 2006;64(3-A):690-7.
19. Haggard P, Cockburn J, Cock J, Fordham C, Wade D. Inter-ference between gait and cognii ve tasks in a rehabilitat-ing neurological populai on. J Neurol Neurosurg Psychiatry. 2000;69(4):479-86.