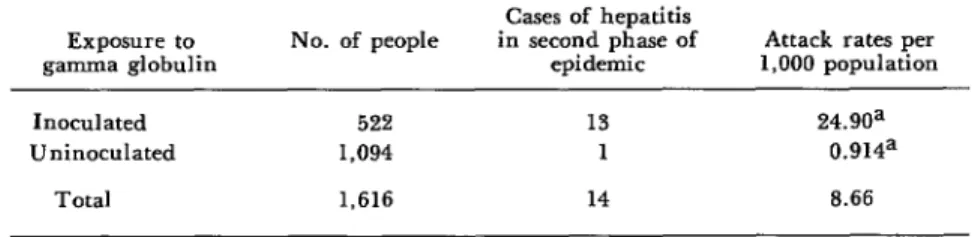
An outbreak of hepatitis attributable to inoculation with contaminated gamma globulin
Texto
Imagem
Documentos relacionados
Accidents at work and living conditions among solid waste segregators in the open dump of Distrito Federal = Acidentes de trabalho e condições de vida de catadores de resíduos
Nessas reticências os intentos de emancipação convergem com pautas de resignação, numa permanente ten- são entre o que se faz contrafeito e o que um dia se desejaria fazer
Entretanto, para alguns idosos a sexualidade não é um componente que faz parte de sua vivência atual, seja por não possuírem companheiro(a), seja por não terem interesse. A
Também, foi considerada a quantidade de pectina utilizada de acordo com o experimentos bem sucedidos na formação dos biofilmes, e somente as pectinas com alto grau
A fundamentação desta investigação no tema do design comprometido orientado para a conceção de um projeto de design no âmbito dos acessórios de moda, direcionou
Salienta-se que os estudantes, globalmente, apresentam níveis reduzidos de autoconfiança quanto às suas capacidades empreendedoras, já que apenas dois em cada cinco
a) O uso de tela de malha preta com 50 % de sombreamento associado a período de 9 semanas de aclimatação foi o que propiciou melhores condições para o segundo estágio da
No entanto, na amostra verificamos que existe uma repetição de notícia para notícia nos dois jornais de informações como o fato da pandemia ter surgido na China, os seus sintomas
